Abstract
The aim of this study was to develop a method to minimize the risk of cancellation of planned surgery in hospital orthopedic departments. The paper proposes a method that combines multi-criteria and multi-faceted risk assessment. Two data sources are used: a fuzzy FTOPSIS method, combined with FMEA assessment. The FMEA method presented in this paper uses the technique of prioritizing preferences according to FTOPSIS similarity to the ideal solution and belief structure, in order to overcome the shortcomings of traditional FMEA indicators. Finally, a numerical case study of process optimization for elective surgery in a Polish clinic is presented. The focus was on planned hip replacements. The effectiveness of the method in assessing the main factors influencing cancellation of elective surgery is demonstrated. A high accuracy of the results and wide adaptability of the method to other areas are features of the combination of the abovementioned methods. The problem addressed in this publication is the high rate of cancellation of elective surgery. The selection of relevant criteria, their importance, and the preferences of the patients were studied. The results of the method provide a viable action plan for the proposed research problem. The proposed method is multifaceted and can be part of an information system to support reorganization, restructuring, and modification of an operational process.
1. Introduction
The cancellation of surgery has various consequences for employees, employers, patients, the hospital, and people in the surrounding local community. An aging population, urbanization, and the prevalence of unhealthy lifestyles worldwide increasingly shape the sustainability of healthcare systems. This paper focuses on orthopedic surgery. This is one of the most common types of hospital treatment. This type of surgery accounts for 40 percent of hospital expenditure and generates about two-thirds of hospital revenue [1]. It consumes most resources, such as staff, operating rooms, and equipment [2].
Hospitals face a number of challenges regarding planned surgical processes, of which some of the most important instances are high healthcare expenditure [3] and rising healthcare cost ratios [4], combined with increasing demand for surgical procedures due to aging and growing patient populations. In addition, technological advances have expanded the scope of surgical interventions [5]. Against this backdrop, hospital management is under increasing pressure to control the costs of surgical procedures, while providing quality health care to surgical patients. An effective cost containment strategy must integrate decision-making at all levels: strategic, tactical, and operational. One of the main issues at the operational level is surgical case scheduling (SCS) [5]. A continued and disproportionate emphasis on specialized and specific healthcare models undermines the ability of these systems to provide equitable and economically sustainable healthcare. There is a lack of tailored solutions for optimizing operational planning processes in the domestic market. In the vast majority of cases, hospitals rely on the expertise of hospital staff [6]. This method is weak, because of human error and sensitivity to external factors. An automated IT system based on appropriately selected methods could positively influence the quality of the surgery planning process and reduce the number of canceled surgeries. The literature lacks solutions that are adapted to the specific conditions of the Polish Healthcare System. The following article presents a method that could provide a good input for an automated IT system for optimizing orthopedic surgery planning processes [7].
2. Related Works
Over the past two decades, multi-criteria decision-making (MCDM) methods have increased the effectiveness of risk assessment of failure modes [8]. Risk assessment is applied using appropriate techniques, to prevent unexpected failure scenarios. Several publications have already appeared in the literature and a number of problems of hospital reorganization, cost reduction, and the hospital care of patients have been solved [9]. The objective of one paper was to conduct a systemic analysis of the resources and performance of public hospitals. A multi-objective optimization (MOO) approach was proposed by [10]. This approach identified the theoretical capacity of the entire hospital and facilitated a sensitivity analysis, such as patient case mix (PCM). The combination of the uncertainty criteria, limited resources, and the competing interests of the decision-makers was used in a multi-criteria model for more efficient planning of surgeries, as described in [11]. Yet a significant problem persists in reliable estimation of hospital capacity—there is a lack of effective automated systems based on modern methods that could support hospitals in preparing schedules for elective surgery.
Modern scientific methods are increasingly effective at estimating risk in different areas [12,13]. As an example, the implementation of risk management tools based on a combination of decision-making methods that extract expert knowledge to improve the accuracy of making the best decision was discussed in a paper about implementation in photovoltaic facilities [14]. In fact, expert knowledge and experience play a key role in risk assessment. A fuzzy preference relation is an effective tool for expressing information about experts’ preferences when comparing alternatives in pairs [15]. One of the most well-known risk assessment methods is FMEA (failure mode and effects analysis) [16]. FMEA is a method used in the healthcare sector since the 1990s to determine the risk of drug production and control of medicines in hospitals [17]. As the application of FMEA in healthcare has been very successful, it has been called healthcare failure modes and effects analysis (H-FMEA) [18]. Recently, several studies have been published using FMEA together with fuzzy sets, to overcome the weaknesses of the traditional RPN (risk priority number) ranking system [19]. A general FMEA method based on fuzzy logic has been proposed. This simulates the traditional FMEA methodology by reducing the number of rules in the fuzzy RPN modeling process [20].
Numerous studies [8,21,22] have shown that the challenges of inappropriate financial allocation, healthcare efficiency, and patient safety make a compelling case for changes to medical systems. New and innovative approaches to healthcare are needed in financing, delivering, and managing health services. At the same time, these approaches should improve the quality of care, ensure financial sustainability, and meet the needs and demands of individuals and communities. Patient-centered approaches that engage people and enable self-care are gaining popularity in response to these challenges. Healthcare delivery is a unique process, involving real-time decision-making and complex human activities. An integrated, automated care-delivery model could effectively coordinate services based on patient and hospital needs.
Contribution
This study aimed to develop a hybrid method considering factors contributing to surgery cancellation in classified hip osteoarthritis patients. By accurately identifying the hospital’s risks (e.g., surgery cancellation), it is possible to select an appropriate solution to reduce surgery-related expenses (i.e., by eliminating unnecessary costs) and increase quality, efficiency, and patient safety and comfort. This study combines the multi-criteria method and FMEA to introduce a structure of belief and describe expert knowledge, by integrating the FMEA with FTOPSIS, while calculating the criterion weights from the expert questionnaires. FTOPSIS calculates the level of performance, and FMEA calculates the risks of hospital operations in a comprehensive and ranked manner based on potential criteria through their integration. This paper also presents a detailed scheme for combining FMEA and FTOPSIS methods.
3. General Scheme of the Method
A risk-based approach and decision-support methods were used to develop the model. The method considers factors that influence the quality of hospital services and the appropriate care for a patient scheduled for surgery for hip osteoarthritis (Figure 1). The TOPSIS fuzzy method was chosen because
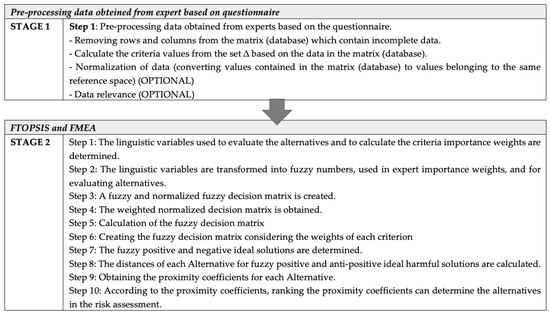
Figure 1.
Scheme of a risk assessment method for determining the coefficient of resignation from surgery.
- The group evaluation method (fuzzy TOPSIS method) with structure of beliefs includes fuzzy evaluations and degrees of belief. In the fuzzy approach, degrees of belief allow the expert to assign a more significant value to the factors under consideration;
- The FTOPSIS method is used to find high-risk options (determining the preference of the entire structure-of-belief problem of experts);
- The relevant calculation procedures can be carried out using fuzzy values;
- The ability to quickly identify the best alternative;
- The relative weightings of S—effect, O—probability, and D—detectability (FMEA method) of an undesirable scenario can “diverge”. The assigning of a weight to each of the mentioned factors is flexible, which gives greater consistency with the actual decision-making situation;
- Input factors (S—effect, O—probability, D—detectability (FMEA method) are combined according to their weights so that they match the research problem (cancellation of planned operations) [3,23,24].
Figure 1 shows the successive stages of the work methodology. The following section describes the exact calculations according to the steps in the figure above.
The following sections present the different steps of the risk assessment method in determining the discontinuation rate in Figure 1. Stage one presents data processing from the acquired database and the procedure for data reduction based on the questionnaire. Stage two presents a mathematical model combining the risk assessment methods and the MCDA fuzzy decision-making method. The proposed method calculation process is presented in the case study of the chapters ’Empirical Verification of The Proposed Method’ and ’Result of The Study’.
4. Risk Assessment Based on FTOPSIS and FMEA
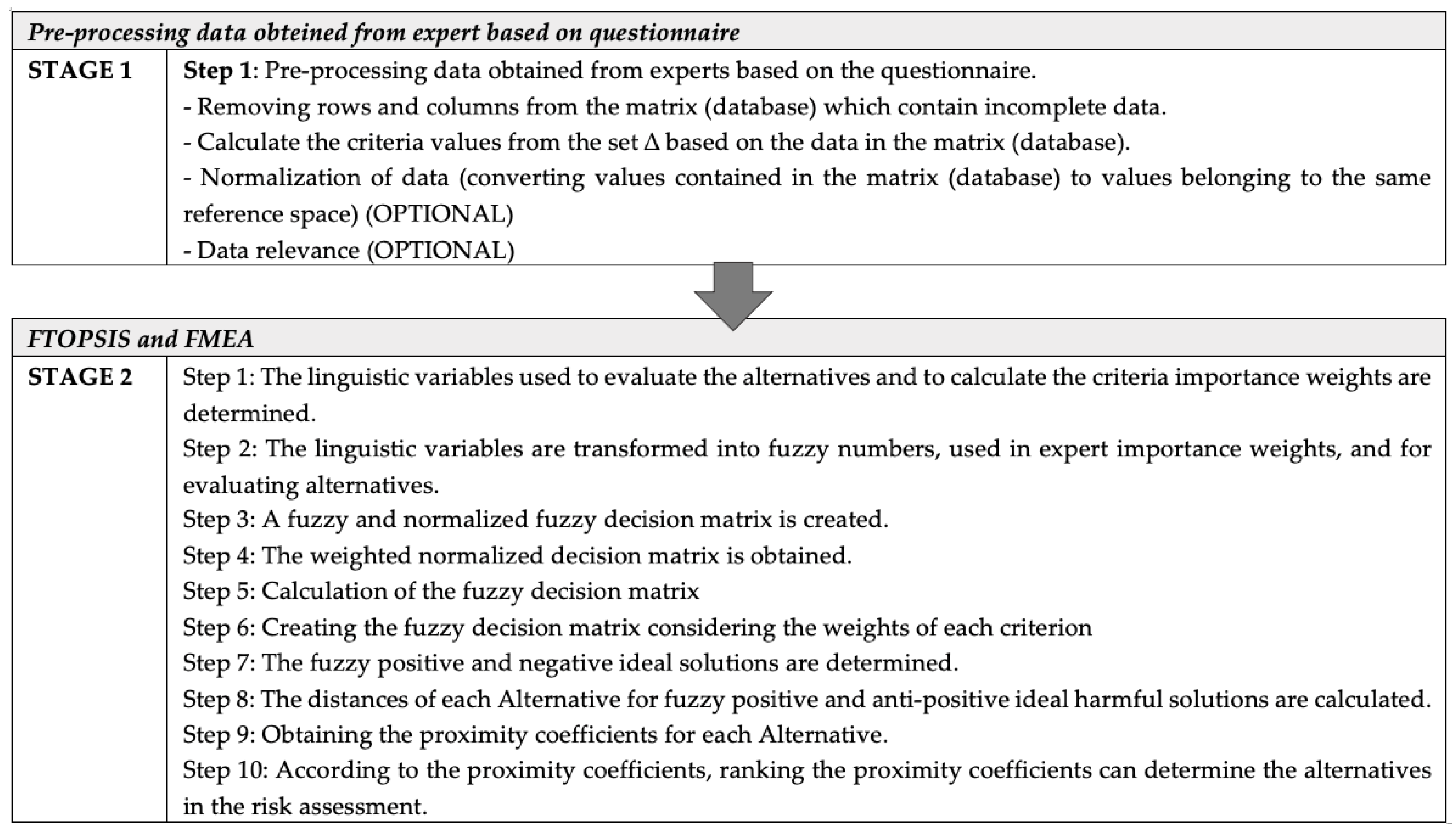
Based on Figure 1, which illustrates the risk assessment scheme, the following section of the paper introduces the solutions for all stages.
Stage one of the proposed risk assessment method, determining the abandonment rate, is to preprocess the data obtained from the experts based on the questionnaire. This step includes
- Removing rows and columns from a matrix (database) that contains incomplete data;
- Calculating the criteria values from the set based on the data in the matrix (database);
- Data normalization (replacing the values in the matrix (database) with values belonging to the same reference space).
Preprocess the data from the set , where the elements of the set are the expert measures (where denotes the element number in the set ; d—the number of elements in the set ; —the i-th element of the set ).
In further considerations, it is assumed that matrix is of dimensions N x p, where N represents the number of rows in the matrix and p represents the number of columns (the number of attributes from the set). Some of the attributes (measures) and opinions of the evaluators (elements of the set ) may be relatively interdependent and relevant or not for determining the availability of surgical rooms. Calculations may be required, such as determining the adequacy of medication or the availability of the necessary tools and materials. Additionally, information may be subject to what is known as “information noise”, which is the result of various errors that may occur in the data derived from the information obtained. To ensure a reduction in information noise, it is essential to use an appropriate cleaning, ordering, and validation method for the data contained within a matrix . This crucial step, known as data preprocessing, guarantees data accuracy and improves the overall data quality. To ensure a reliable risk assessment, a filtered subset of criteria must be prepared, regardless of data preprocessing. These criteria play a crucial role in determining the measured dropout rate, and the approach to this subset is known as reduction of criteria. Step one determines the language variables for evaluating the alternatives and calculating the weight of the criteria importance. A formalized multi-criteria information table helps combine the selected FTOPSIS method with the risk assessment method.
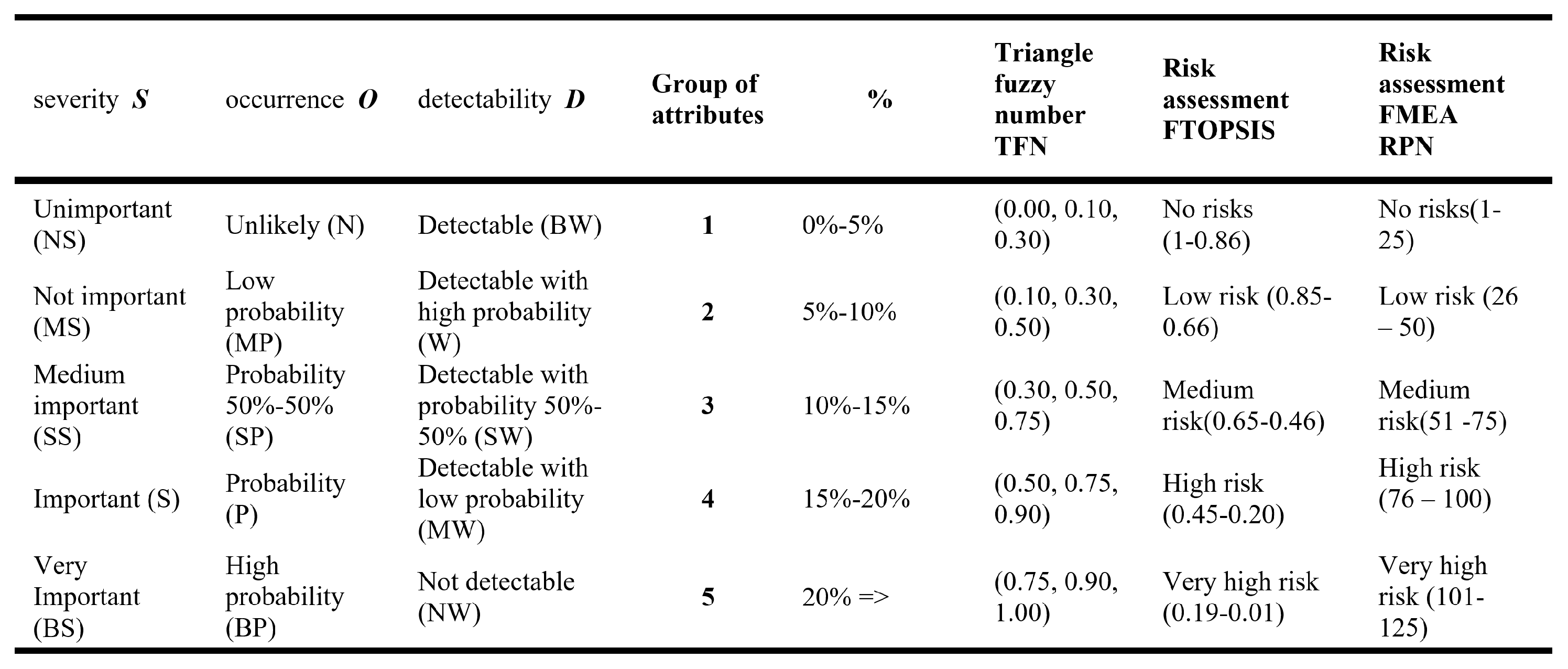
The next stage of the method (Figure 1) is the risk assessment based on FTOPSIS and FMEA. In traditional FMEA, an indicator known the as risk priority number (RPN) was used in qualifying the failure method by multiplying three parameters: occurrence (O), detectability (D), and severity (S). In FMEA, a value within is assigned to each parameter O, D, S. After calculating the RPN for the article, the higher the value assigned for a parameter, the more undesirable the effect of that parameter on the evaluation. Figure 2 shows the linguistic terms and triangular values for evaluating the alternatives, where the linguistic variables have been transformed into fuzzy numbers. Linguistic variables were used for assigning expert importance weights and evaluating alternatives. It contains both fuzzy ratings and degrees of belief. Using linguistic terms allows the decision maker (expert) to assign a more meaningful value to the factors under consideration.
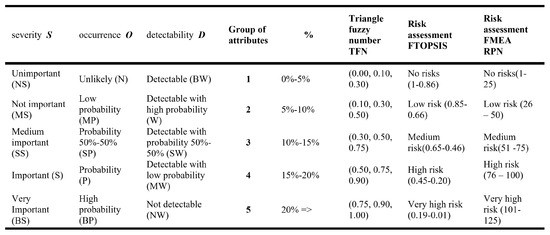
Figure 2.
Language terms and triangular values of alternative assessments.
In Step two, the linguistic variables were transformed into fuzzy numbers, which were used for the expert importance weights to evaluate alternatives. Each parameter’s fuzzy function can turned into a triangle fuzzy number, as a graphical representation of the fuzzy set. To consider the inaccurate data determining the values of alternatives, based on the data contained in the determined information matrix with criteria from the set (Equation (2)), the FTOPSIS method has been used, so that its corresponding calculation procedures can be carried out using fuzzy values.
The quality values of the alternatives A with weights defined for each criterion after the reduction (step one) C from the information matrix are aggregated. It is assumed that denote the alternatives among which the experts will choose the winning solution. are the criteria against which the performance of each alternative is calculated. The value is a triangular fuzzy number and denotes the performance of the alternatives against the criterion . From an analytical perspective, denotes the weight of the criterion and is a normalized triangular fuzzy number.
As well as the fuzzy weight vector W of the form:
Next, step three is computing the fuzzy decision matrix and the normalized fuzzy decision matrix. For each triangular fuzzy value, the set of —sections of the form calculate
Thus, each fuzzy value can be transformed into an interval value. Then, the following procedures are used to perform normalization of the interval values (step four):
As a result, the interval is the normalized equivalent of the interval . It is then possible to transform the normalized interval back into a triangular fuzzy number of the form in such a way that the value of at will be
Similarly, establishing the coefficient , we obtain the remaining values of a triangular fuzzy number:
then
The value is the normalized equivalent of the triangular fuzzy number .
Next, step five creates a fuzzy decision matrix considering the weights of each criterion. Step six creates a normalized fuzzy decision matrix considering the weights of each criterion:
These are normalized returns, each in the interval .
Step seven determines the ideal with fuzzy nature, both positive and negative. Determining the ideal solution and the inverse of the ideal solution (anti-ideal solution):
In step eight, the distances of each alternative for the fuzzy positive and anti-positive ideal negative solutions are calculated.
Calculating the distance of each considered alternative from the ideal solution and the inverse of the ideal solution between two fuzzy numbers of form and can be carried out as follows:
The distance of the alternatives from the ideal solution can be calculated as follows:
Similarly, the distance from the inverse of the ideal solution (anti-ideal solution) is calculated as follows:
Step nine obtains proximity coefficients for each alternative.
The relative closeness of alternative to the ideal solution is defined as
In step 10, depending on the result of the proximity coefficients, a ranking of these coefficients is created to determine the alternatives in the risk assessment. The result ranks the alternatives in order, from the largest to the smallest relative closeness value to the ideal solution .
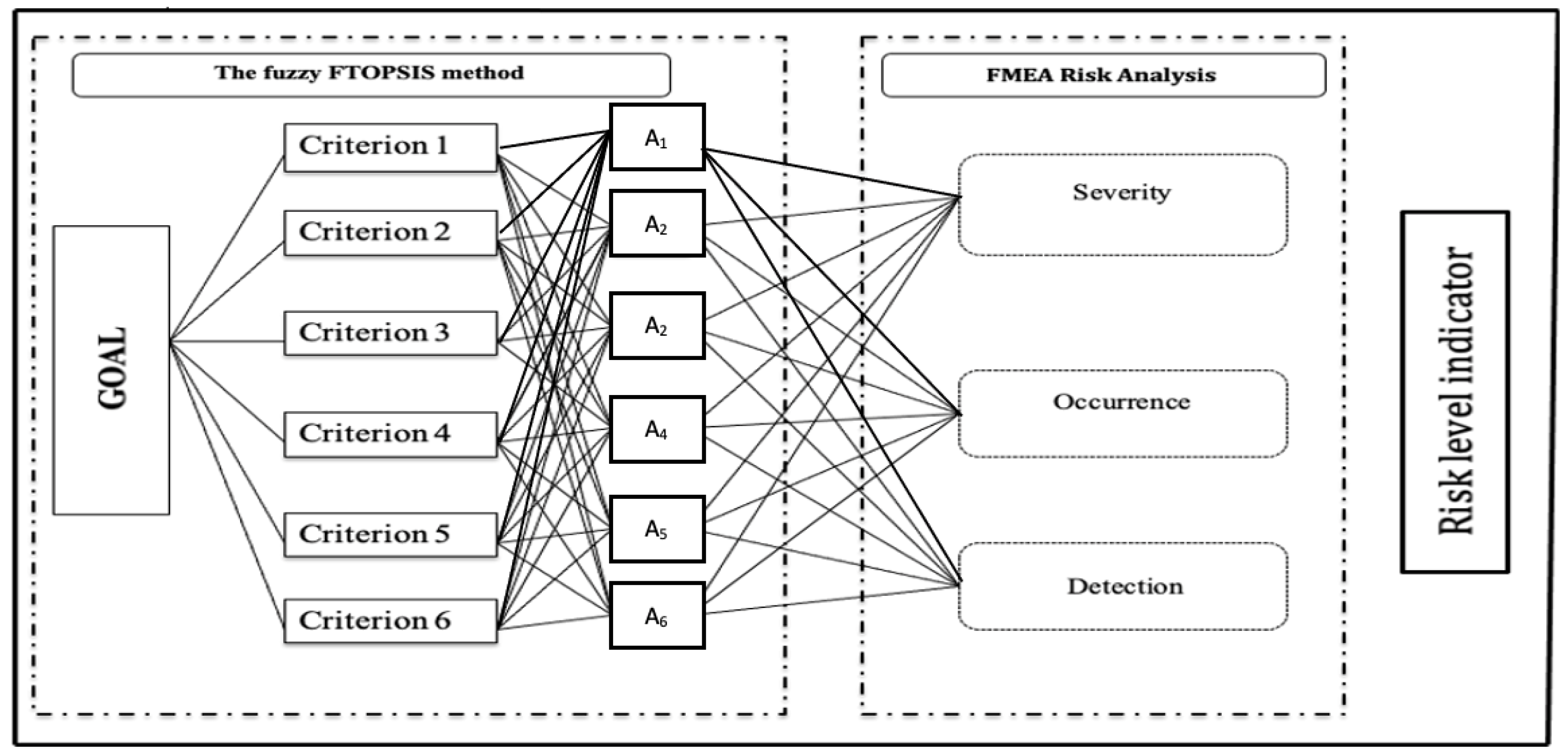
Figure 3 shows the graphical solution of the combination of the two methods, TOPSIS and FMEA.
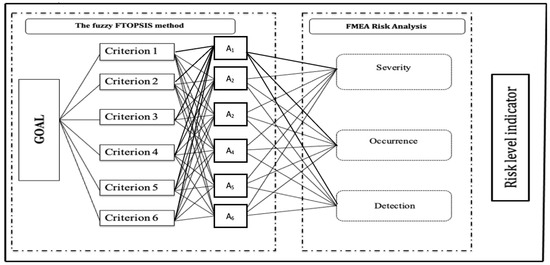
Figure 3.
Combining the fuzzy method with FMEA.
Conclusions of the analysis:
- The proposed risk assessment approach incorporates fuzzy judgments and belief degrees (expert preferences);
- The flexibility of assigning weights to each factor in the proposed approach is consistent with the actual decision situation;
- The input factors (S, O, D) are combined according to their weights, enabling a more comprehensive application approach.
5. Results
Surgical scheduling involves allocating hospital resources to individual cases and deciding when to perform surgeries. This task is critical to the efficient use of hospital resources, while providing quality patient care. The following are the results of the study of the treatment process based on actual data. Research at The Department of The Orthopedics and Traumatology at The Pomeranian Medical University in Szczecin usually consists of three stages: patient classification, therapeutic care, and elective surgery.
- Patients arriving at the orthopedic unit are first classified according to their level of urgency using appropriate indicators;
- A hip replacement (endoprosthesis) appointment is scheduled if the patient is eligible for elective surgery;
- A patient referred to the surgical service receives a medical consultation from nurses, registrars, surgeons, orthopedic surgeons, and anesthetists;
- After a screening, an essential examination is carried out. The patient is operated on the next day.
To confirm the validity of the risk assessment model, three experts (a nurse, an anesthetist, and a physician, referred to as “operator”—who performs the surgery) participated in this research. The assessment was made the day before the elective surgery [25]. The study considered the indicators that influence the cancellation of hip replacement surgery (six variants of the cancellation process). Finally, the scores obtained were compared with those of experts from the Department of Orthopedics and Traumatology of Pomeranian Medical University in Szczecin.
General hospital characteristics:
- Three operating rooms;
- Inpatient surgery room;
- Operating room for patients with infections;
- Operating room for trauma patients;
- One post-operative room,
- 42 patient beds.
Additional factors:
- Hip replacement surgery is performed on Mondays, Wednesdays, or Fridays (optional);
- There are three or four scheduled surgeries per day.
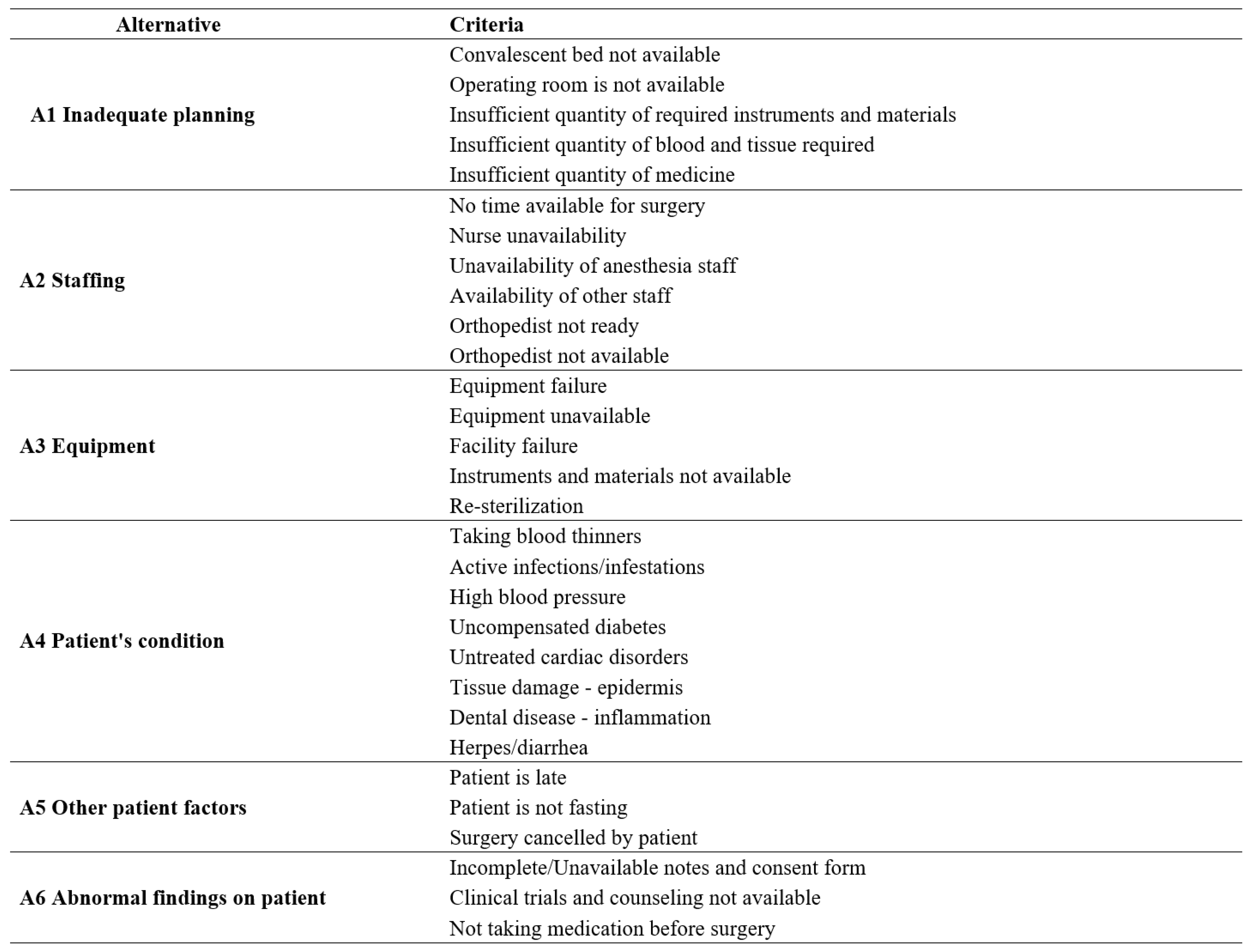
The questionnaire, evaluated by experts, obtained six alternatives based on 30 criteria. Figure 4 shows the obtained alternatives from the decision matrix for risk assessment based on the questionnaire.
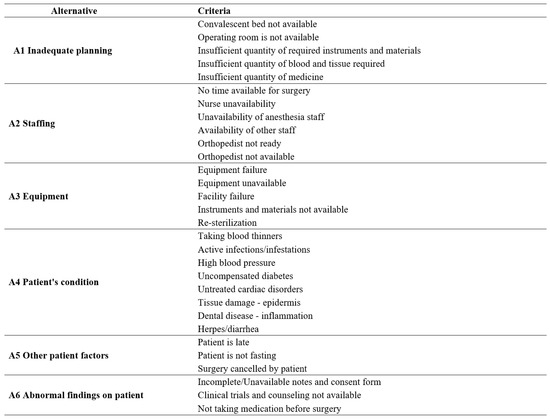
Figure 4.
Designated alternatives from the decision matrix for risk assessment.
The following research presents the results of the steps based on the previous method. To fit the data from the questionnaires into the information matrix, the following factors were determined to give the evaluation attributes with the determination of alternatives from the decision matrix for risk assessment. These are A1—Inadequate planning; A2—Staffing; A3—Equipment; A4—Patient condition; A5—Other patient factors; A6—Abnormal findings in a patient. After obtaining the results from stage one and stage two, the belief distance measurement is obtained along (Figure 5) with a graphical representation of the fuzzy function of each parameter (Figure 6, Figure 7 and Figure 8).
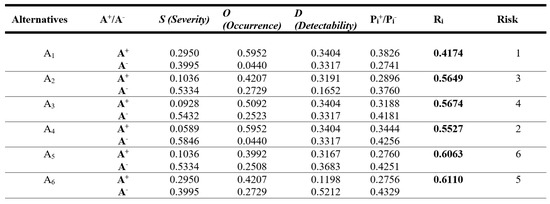
Figure 5.
Belief distance measurement.
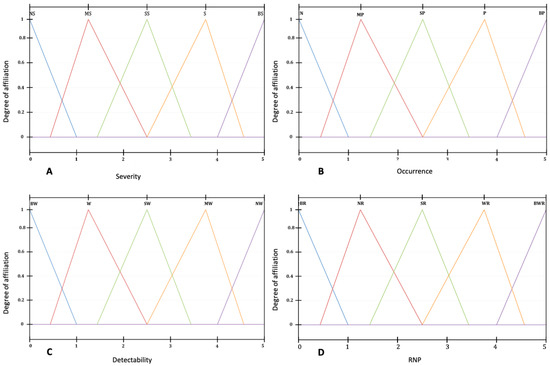
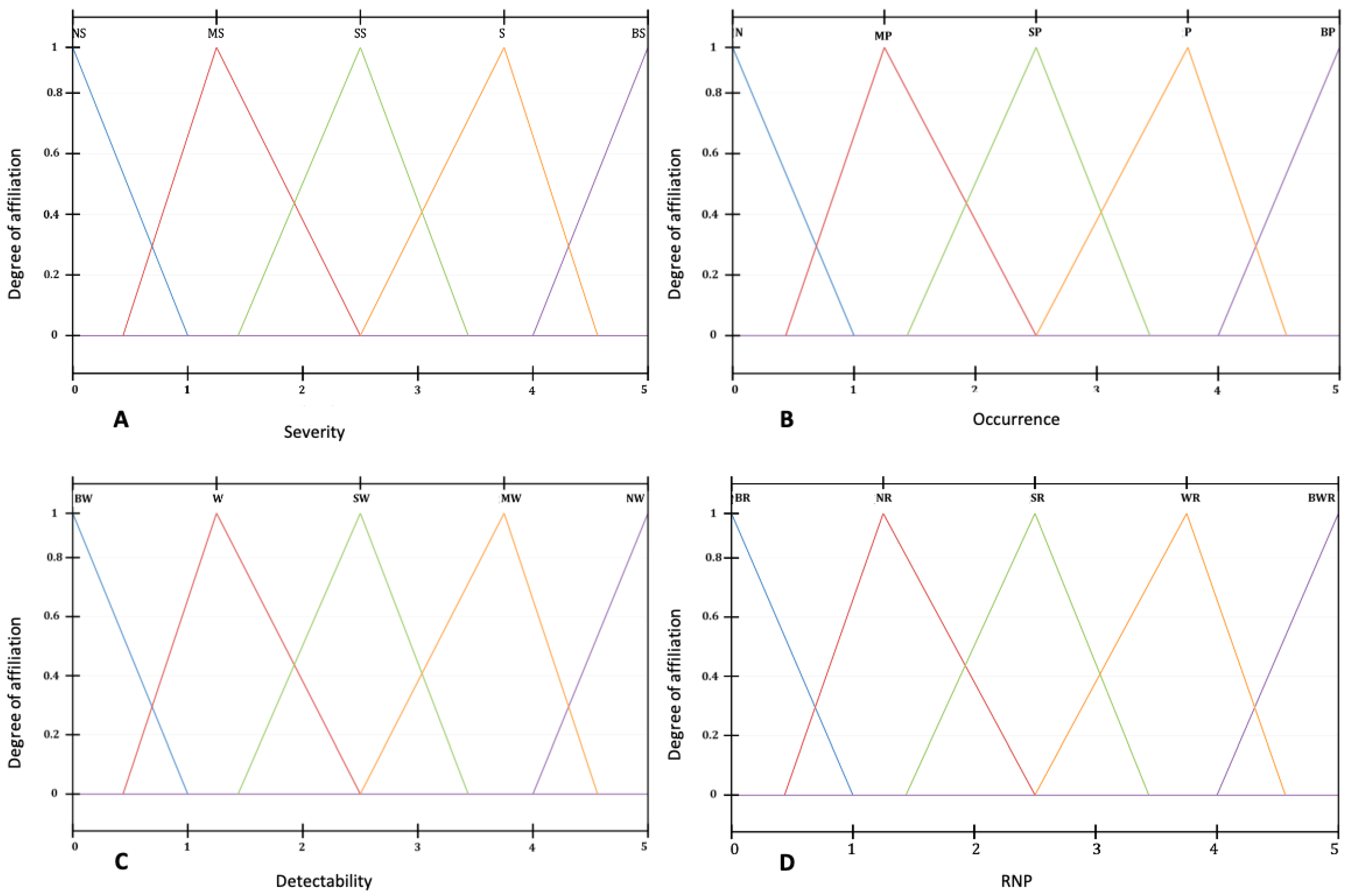
Figure 6.
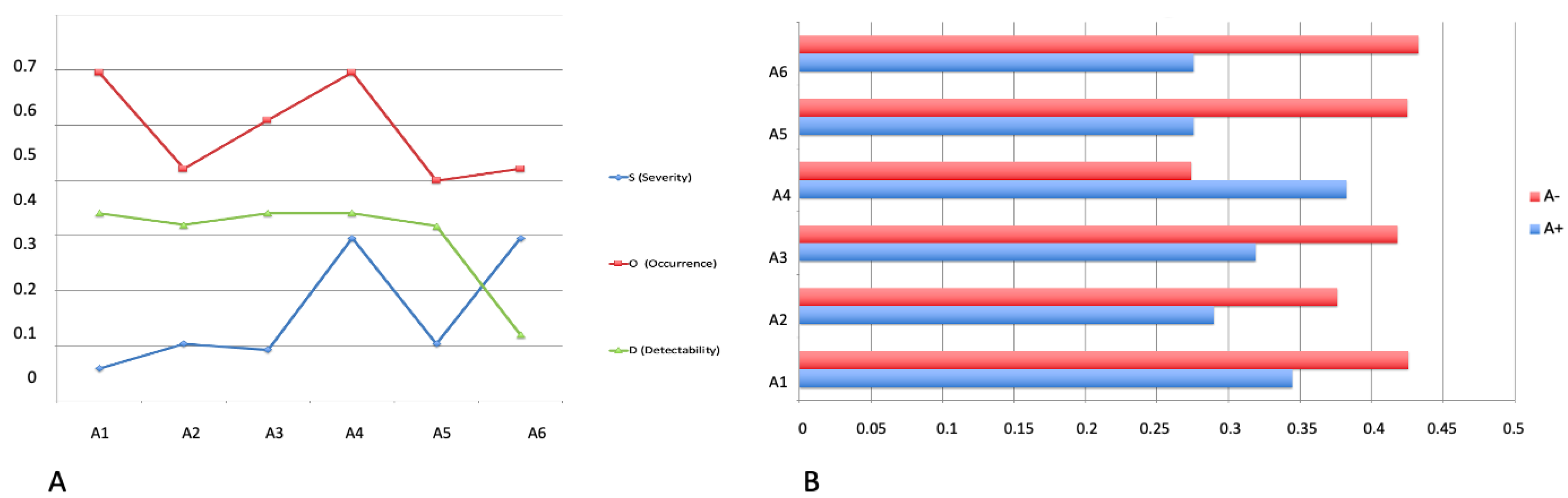
Fuzzy functions of each parameter. (A) Fuzzy function of parameter S–Severity; (B) fuzzy function of parameter O–Occurrence; (C) fuzzy function of parameter D–Detecability; (D) fuzzy function in risk assessment (RFN).
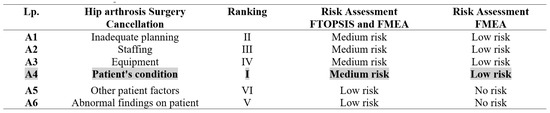
Figure 7.
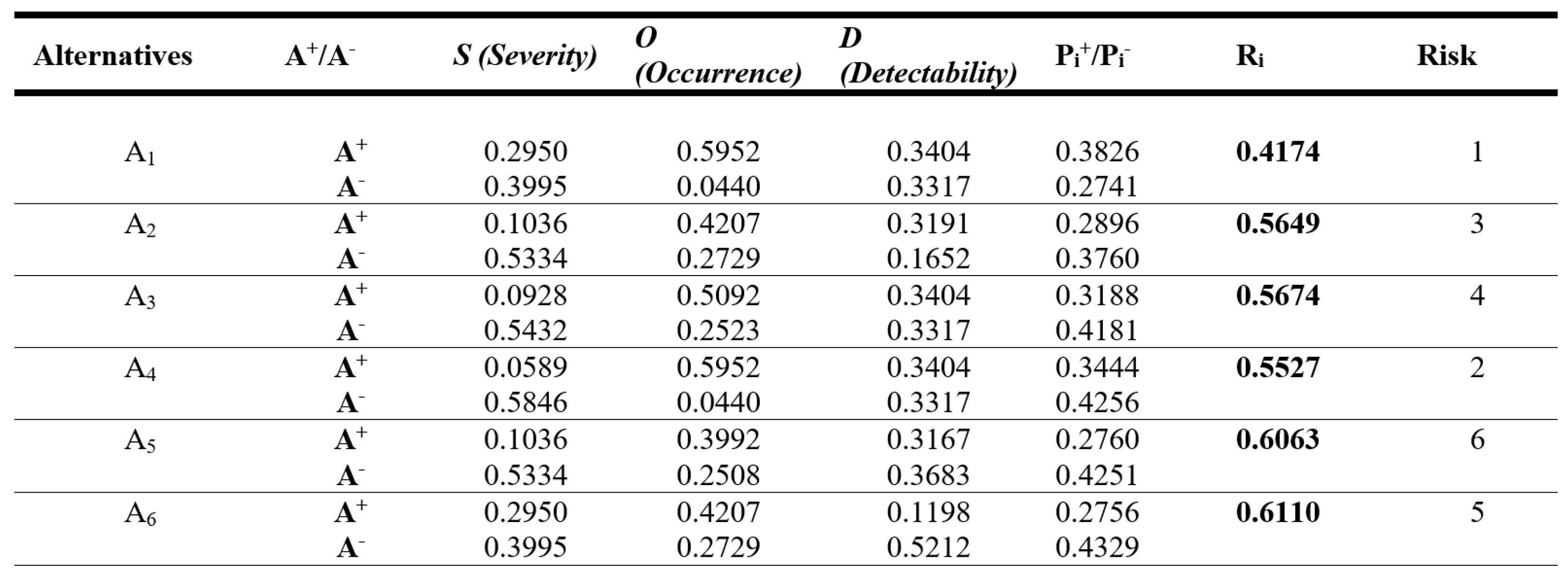
Risk assessment of the designated alternatives from the decision matrix.
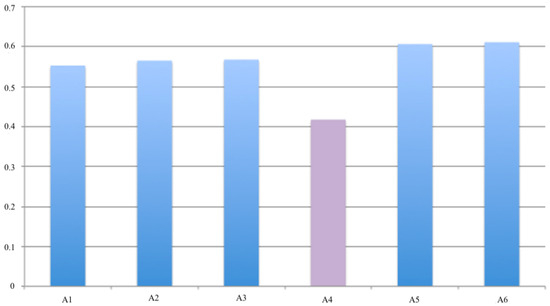
Figure 8.
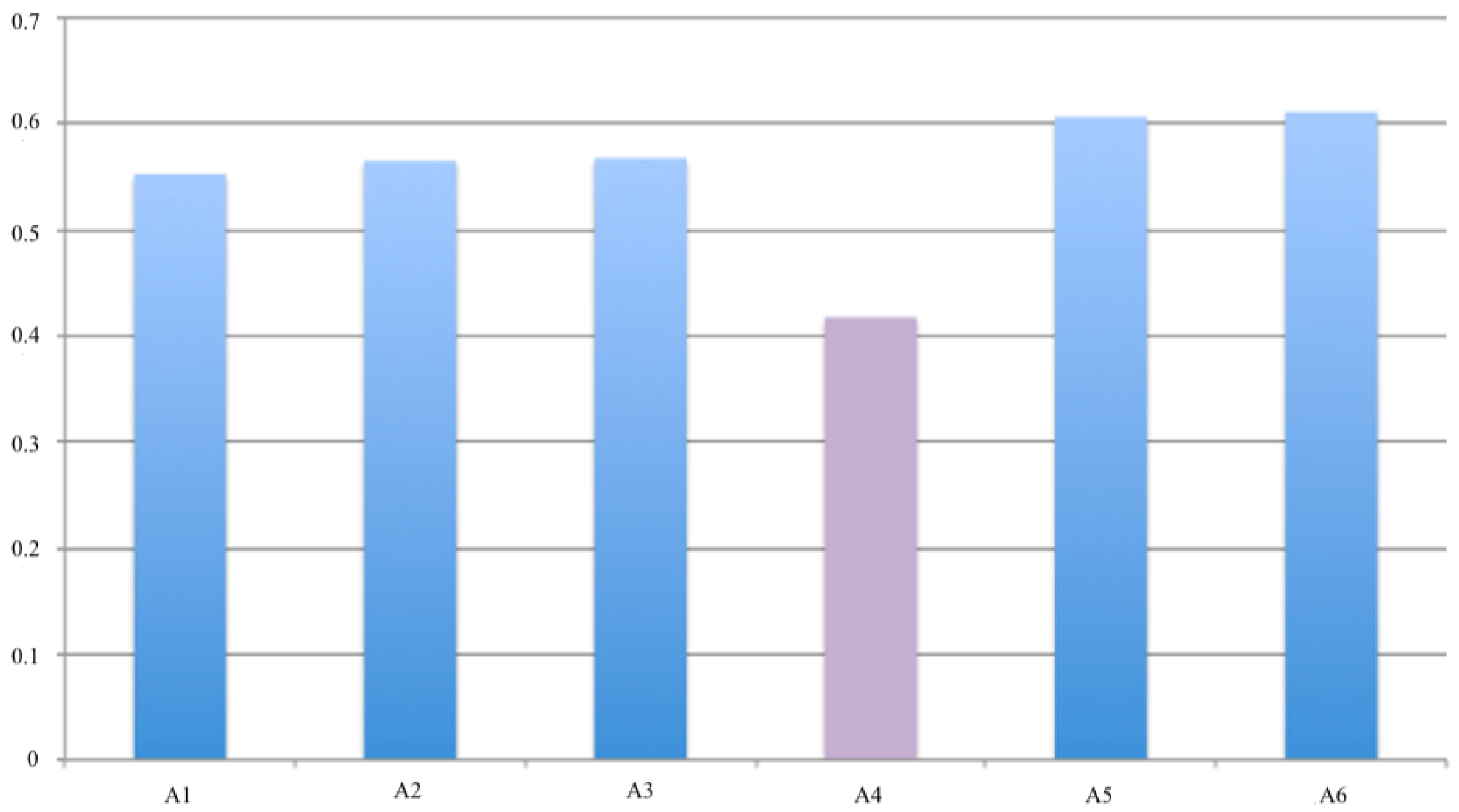
Relative proximity for each alternative in the risk assessment.
The results from the presented method using the measurement of belief distance are presented below, along with a graphical representation of the fuzzy function of each parameter.
Based on the proposed method, the results show that the expert opinion compared with the results of FMEA and FTOPSIS showed the potential of the framework for correctly prioritizing failure rates. Figure 6 shows the ideal solution for the designated alternatives in the risk assessment. Figure 9 shows the distance of each alternative to the ideal solution in the risk assessment.
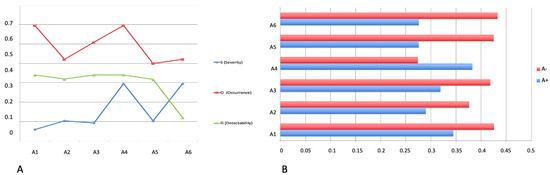
Figure 9.
(A) The ideal solution for the alternatives in the risk assessment; (B) Distance of each of the considered alternatives to the ideal solution in the risk assessment.
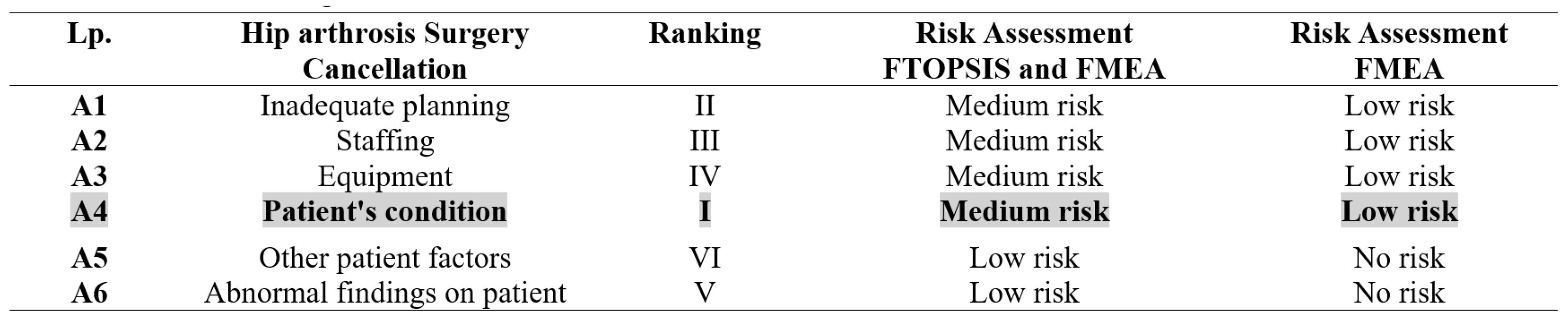
Of the six factors, three—patient condition, inadequate scheduling, and staffing—were identified as having the most significant impact on surgical cancellation of elective surgery, as shown in Figure 7 and Figure 8.
In considering the study results, it is worth looking at the three main indicators identified by the method. The first, and most important, is the patient’s condition. There is a high risk that tests performed just before a planned operation will exclude the patient from the procedure. Incorrect planning is the second most important indicator. This factor is quite common and offers many opportunities for the implementation of modern methods in this area. Finally, the third ranked indicator, staffing, is a complex and well-known problem in Polish healthcare. A shortage of staff often leads to delays or cancellations of elective surgery.
The results show that the patient’s condition is the main risk for cancellation. Of course, the financial risk can be reduced by examining the patient before admission to the ward, but only in the case of a planned operation. The patient can then have the necessary tests carried out using health insurance funds. In the case of urgent surgery, the risk increases and so do the costs to the hospital. There is a strong need for a strategy for hospitals to develop a system that reduces excessive costs due to canceled operations. The research presented in the case study combined the two methods and showed which problems in hospitals should be focused on when planning operations. The method confirmed the validity of the process used and its relevance to the quality of hospital performance.
6. Conclusions
This paper presents a method that combines a multi-criteria optimization approach with FMEA for the evaluation of aspects affecting the cancellation of planned orthopedic surgery. The case study includes a description of the organization of planned hip replacement surgeries in a clinic in Poland. It was shown that the combination of the above methods was characterized by a high accuracy of results and wide adaptability of the method to other fields.
The results of the method used are promising. The conclusions of the hybrid method were similar to those of the experts. This suggests that the applicability of the proposed hybrid method should be confirmed in larger scale research. It will be interesting to see how much the results vary depending on the environment. This raises the question of whether it is possible to develop a systematic approach to the operational planning process that could be applied on a larger scale. Taking this a step further, it is possible to consider how an information system based on the proposed method could be calibrated and improved.
The main characteristics of the risk assessment method for determining surgical dropout rates are
- The method is procedural in nature, a planned and reusable activity;
- The method takes into account the broad aspect of variability of expert preferences and is adaptive rather than rigid (once implemented). Adaptation here is the ability to adjust for changes in those factors where the criteria defined by the expert have the greatest impact on surgical attrition;
- The method can be used for any operation performed and in any hospital;
- The use of fuzziness through the application of the decision support method FTOPSIS allows for better (more accurate) risk assessment;
- Confirmation of the method’s applicability to risk analysis using a decision support method.
The novelty of this publication is the multi-criteria and multi-faceted risk assessment. This method combines two data sources, the FTOPSIS fuzzy method with the FMEA risk assessment. With this solution, it will be possible to automate the process of reorganization and redevelopment of the system in hospitals and other organizations and enterprises. The multi-faceted nature improves this method, and it can be applied to various problems. It is possible to achieve such automation by implementing the method presented in this paper, as shown in Figure 1.
The method developed in this paper can form part of an automated information system supporting the reorganization, restructuring, and modification of the operational process in a hospital. The process of renewal, modernization, and reconstruction of a given system can be understood, to allow reconstruction promoting flexibility and accuracy.The presented methodology belongs to the class of CASE systems. It enables automation in the so-called software system re-engineering. The method is also applicable in other areas where such benchmarking is required for complicated processes and quality service delivery. It is also a tool for improving an organization’s activities in so-called outsourcing aimed at increasing the effectiveness and efficiency of the organization in providing services related to health, industry, and learning.
Funding
This research received no external funding.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The author declares no conflict of interest.
References
- Wong, J.; Khu, K.J.; Kaderali, Z.; Bernstein, M. Delays in the operating room: Signs of an imperfect system. Can. J. Surg. 2010, 53, 189. [Google Scholar]
- Bennell, K.L.; Hinman, R.S. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J. Sci. Med. Sport 2011, 14, 4–9. [Google Scholar] [CrossRef]
- Liu, H.C.; You, J.X.; Chen, S.; Chen, Y.Z. An integrated failure mode and effect analysis approach for accurate risk assessment under uncertainty. Iie Trans. 2016, 48, 1027–1042. [Google Scholar] [CrossRef]
- Kai, X.; Tang, L.C.; Xie, M.; Ho, S.L.; Zhu, M. Fuzzy assessment of FMEA for engine systems. Reliab. Eng. Syst. Saf. 2002, 75, 17–29. [Google Scholar]
- Cihoda, J.H.; Alves, J.R.; Fernandes, L.A.; de Souza Neto, E.P. The analysis for the causes of surgical cancellations in a Brazilian university hospital. Care Manag. J. 2015, 16, 41–47. [Google Scholar] [CrossRef]
- Uzialko, J.; Radosinski, E. Metody zarządzania zasobami na przykładzie służby zdrowai. Badania Oper. Decyzyjne 2009, 1, 121–142. [Google Scholar]
- Denton, B.T.; Rahman, A.S.; Nelson, H.; Bailey, A.C. Simulation of a multiple operating room surgical suite. In Proceedings of the Winter Simulation Conference, Monterey, CA, USA, 3–6 December 2006; pp. 414–424. [Google Scholar]
- Liu, H.C.; Chen, X.Q.; Duan, C.Y.; Wang, Y.M. Failure mode and effect analysis using multi-criteria decision making methods: A systematic literature review. Comput. Ind. Eng. 2019, 135, 881–897. [Google Scholar] [CrossRef]
- Burdett, R.L.; Corry, P.; Yarlagadda, P.; Cook, D.; Birgan, S.; McPhail, S.M. A mathematical framework for regional hospital case mix planning and capacity appraisal. Oper. Res. Perspect. 2023, 10, 100261. [Google Scholar] [CrossRef]
- Burdett, R.; Kozan, E. A multi-criteria approach for hospital capacity analysis. Eur. J. Oper. Res. 2016, 255, 505–521. [Google Scholar] [CrossRef]
- Rachuba, S.; Werners, B. A fuzzy multi-criteria approach for robust operating room schedules. Ann. Oper. Res. 2017, 251, 325–350. [Google Scholar] [CrossRef]
- Carbone, T.A.; Tippett, D.D. Project risk management using the project risk FMEA. Eng. Manag. J. 2004, 16, 28–35. [Google Scholar] [CrossRef]
- Toljaga-Nikolić, D.; Todorović, M.; Bjelica, D. Appliction of the FMEA technique in a project risk analysis. Eur. Proj. Manag. J. 2018, 8, 36–42. [Google Scholar] [CrossRef]
- Rahimi, A.; Hejazi, S.M.; Zandieh, M.; Mirmozaffari, M. A Novel Hybrid Simulated Annealing for No-Wait Open-Shop Surgical Case Scheduling Problems. Appl. Syst. Innov. 2023, 17, 15. [Google Scholar] [CrossRef]
- Tang, M.; Liao, H.; Li, Z.; Xu, Z. Nature disaster risk evaluation with a group decision-making method based on incomplete hesitant fuzzy linguistic preference relations. Sustainability 2018, 15, 751. [Google Scholar] [CrossRef] [PubMed]
- Mahdi Bahrami, D.; Sajjadi, S.M. Innovation and Improvements In Project Implementation and Management; Using FMEA Technique. Procedia-Soc. Behav. Sci. 2012, 41, 418–425. [Google Scholar] [CrossRef]
- Duwe, B.; Fuchs, B.D.; Hansen-Flaschen, J. Failure mode and effects analysis application to critical care medicine. Crit. Care Clin. 2005, 21, 21–30. [Google Scholar] [CrossRef] [PubMed]
- DeRosier, J.; Stalhandske, E.; Bagian, J.P.; Nudell, T. Using health care failure mode and effect analysis™: The VA National Center for Patient Safety’s prospective risk analysis system. Jt. Comm. J. Qual. Improv. 2002, 28, 248–267. [Google Scholar] [CrossRef]
- Zhang, Z.; Chu, X. Risk prioritization in failure mode and effects analysis under uncertainty. Expert Syst. Appl. 2011, 38, 206–214. [Google Scholar] [CrossRef]
- Tay, K.M.; Lim, C.P. A guided rule reduction system for prioritization of failures in fuzzy FMEA. In Proceedings of the Applications of Soft Computing: Recent Trends; Springer: Berlin/Heidelberg, Germany, 2006; pp. 301–310. [Google Scholar]
- Valentijn, P.P.; Schepman, S.M.; Opheij, W.; Bruijnzeels, M.A. Understanding integrated care: A comprehensive conceptual framework based on the integrative functions of primary care. Int. J. Integr. Care 2013, 13, e010. [Google Scholar] [CrossRef]
- Goodwin, N.; Stein, V.; Amelung, V. What is integrated care? In Handbook Integrated Care; Springer: Berlin/Heidelberg, Germany, 2021; pp. 3–25. [Google Scholar]
- Guerrero, H.H.; Bradley, J.R. Failure Modes and Effects Analysis: An Evaluation of Group versus Individual Performance. Prod. Oper. Manag. 2013, 22, 1524–1539. [Google Scholar] [CrossRef]
- Huang, J.; Li, Z.; Liu, H.C. New approach for failure mode and effect analysis using linguistic distribution assessments and TODIM method. Reliab. Eng. Syst. Saf. 2017, 167, 302–309. [Google Scholar] [CrossRef]
- Walash, N.; Mitchell, H.; Reeves, B.; Hurley, M. Integrated exercise, and self-management programmers in steoarthritis of the hip and knee A systematic review of effectiveness. Rehabil. Med. 2006, 10, 57–65. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).