
Hemophagocytosis of the Hilar Pulmonary Lymph Nodes Is a More Sensitive Indicator of the Severity of COVID-19 Disease than Bone Marrow Hemophagocytosis

Abstract
:Simple Summary
Abstract
1. Background
2. Materials and Methods
2.1. Autoptic Tissues
2.2. Processing of Lymph Nodes and Bone Marrow
2.3. Identification and Counting of Phagocytes
2.4. Medical Records
2.5. HLH Score Calculation
2.6. Statistical Analysis
3. Results
3.1. Clinical Patient Characteristics
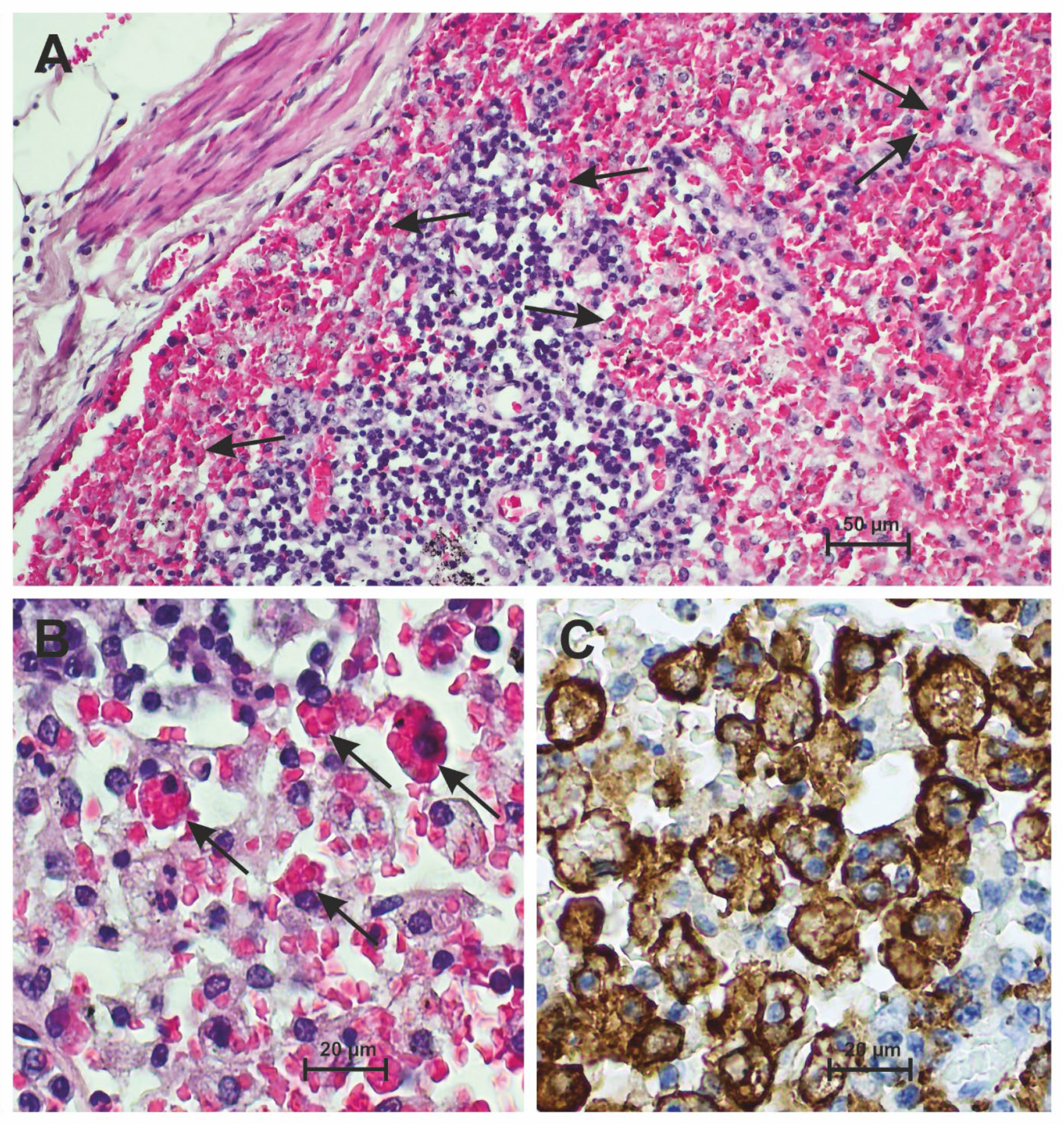
3.2. Hemophagocytosis Is Found in the Lymph Nodes of Patients Who Have Died from Severe COVID-19
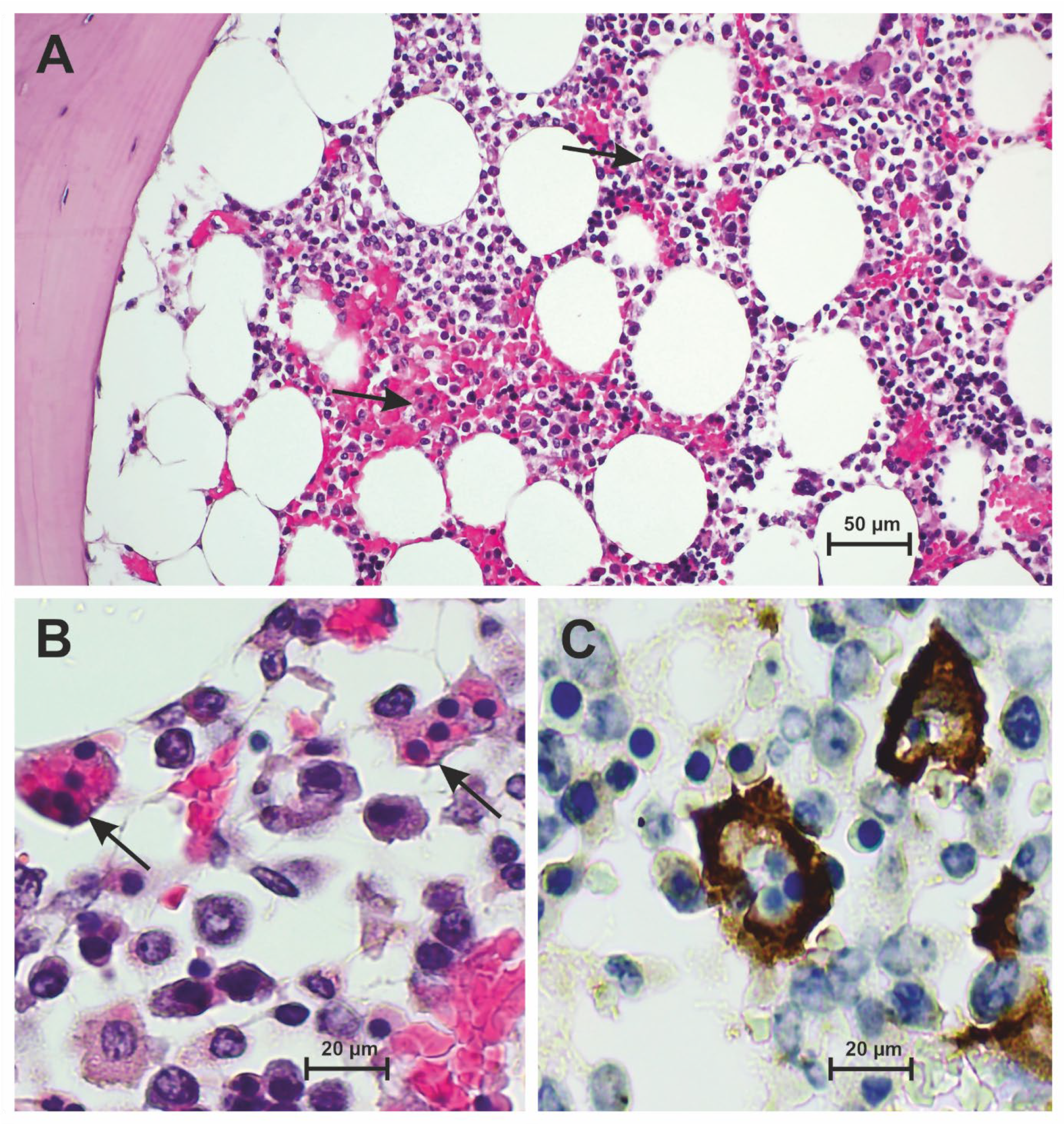
3.3. Hemophagocytosis Is Found in the Bone Marrow of Patients Who Have Died from Severe COVID-19
3.4. Frequency of Hemophagocytosis in Hilar Lymph Nodes Is Higher than in the Bone Marrow of Patients Who Have Died from Severe COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Long, Y.; Zheng, Y.; Li, C.; Guo, Z.; Li, P.; Zhang, F.; Liu, W.; Wang, Y. Respiratory pathogenic microbial infections: A narrative review. Int. J. Med. Sci. 2024, 21, 826–836. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The role of cytokines including interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Harris, C.K.; Hung, Y.P.; Nielsen, G.P.; Stone, J.R.; Ferry, J.A. Bone Marrow and Peripheral Blood Findings in Patients Infected by SARS-CoV-2. Am. J. Clin. Pathol. 2021, 155, 627–637. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fadlallah, M.M.; Salman, S.M.; Fadlallah, M.M.; Rahal, H. Hemophagocytic Syndrome and COVID-19: A Comprehensive Review. Cureus 2023, 15, e36140. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karakike, E.; Giamarellos-Bourboulis, E.J. Macrophage Activation-Like Syndrome: A Distinct Entity Leading to Early Death in Sepsis. Front. Immunol. 2019, 10, 55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wilcox, R.A. Janus Family kinase (JAK) inhibitors in HLH and severe COVID-19. Am. J. Hematol. 2020, 95, 1448–1451. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Zhou, C.; Deng, J.; Zhou, J. JAK inhibition as a new treatment strategy for patients with COVID-19. Biochem. Pharmacol. 2022, 202, 115162. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Z.; Wang, J.; Ji, B.; von Bahr Greenwood, T.; Zhang, Y.; Wang, Y.; Kong, D.; Li, A.; Jiang, Y.; Guo, Y.; et al. Clinical presentation of hemophagocytic lymphohistiocytosis in adults is less typical than in children. Clinics 2016, 71, 205–209. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nguyen, T.T.T.; Kim, Y.T.; Jeong, G.; Jin, M. Immunopathology of and potential therapeutics for secondary hemophagocytic lymphohistiocytosis/macrophage activation syndrome: A translational perspective. Exp. Mol. Med. 2024, 56, 559–569. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Swoboda, J.; Wittschieber, D.; Sanft, J.; Kleemann, S.; Elschner, S.; Ihle, H.; Hubig, M.; Pletz, M.W.; Mall, G.; Gassler, N. Bone marrow haemophagocytosis indicates severe infection with severe acute respiratory syndrome coronavirus 2. Histopathology 2021, 78, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Toeback, J.; Depoortere, S.D.; Vermassen, J.; Vereecke, E.L.; Van Driessche, V.; Hemelsoet, D.M. Microbleed patterns in critical illness and COVID-19. Clin. Neurol. Neurosurg. 2021, 203, 106594. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gars, E.; Purington, N.; Scott, G.; Chisholm, K.; Gratzinger, D.; Martin, B.A.; Ohgami, R.S. Bone marrow histomorphological criteria can accurately diagnose hemophagocytic lymphohistiocytosis. Haematologica 2018, 103, 1635–1641. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Allen, J.; McCambridge, M.M.; Kincaid, H.; Kalter, J.A. Incidence of Secondary Hemophagocytic Lymphohistiocytosis in Critically-Ill COVID-19 Patients. Cureus 2021, 13, e16735. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trougakos, I.P.; Stamatelopoulos, K.; Terpos, E.; Tsitsilonis, O.E.; Aivalioti, E.; Paraskevis, D.; Kastritis, E.; Pavlakis, G.N.; Dimopoulos, M.A. Insights to SARS-CoV-2 life cycle, pathophysiology, and rationalized treatments that target COVID-19 clinical complications. J. Biomed. Sci. 2021, 28, 9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Park, J.; Foox, J.; Hether, T.; Danko, D.; Warren, S.; Kim, Y.; Reeves, J.; Butler, D.J.; Mozsary, C.; Rosiene, J.; et al. Systemic Tissue and Cellular Disruption from SARS-CoV-2 Infection revealed in COVID-19 Autopsies and Spatial Omics Tissue Maps. bioRxiv 2021, arXiv:2021.03.08.434433. [Google Scholar]
- Schnaubelt, S.; Tihanyi, D.; Strassl, R.; Schmidt, R.; Anders, S.; Laggner, A.N.; Agis, H.; Domanovits, H. Hemophagocytic lymphohistiocytosis in COVID-19: Case reports of a stepwise approach. Medicine 2021, 100, e25170. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Haslbauer, J.D.; Zinner, C.; Stalder, A.K.; Schneeberger, J.; Menter, T.; Bassetti, S.; Mertz, K.D.; Went, P.; Matter, M.S.; Tzankov, A. Vascular Damage, Thromboinflammation, Plasmablast Activation, T-Cell Dysregulation and Pathological Histiocytic Response in Pulmonary Draining Lymph Nodes of COVID-19. Front. Immunol. 2021, 12, 763098. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xiang, Q.; Feng, Z.; Diao, B.; Tu, C.; Qiao, Q.; Yang, H.; Zhang, Y.; Wang, G.; Wang, H.; Wang, C.; et al. SARS-CoV-2 Induces Lymphocytopenia by Promoting Inflammation and Decimates Secondary Lymphoid Organs. Front. Immunol. 2021, 12, 661052. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cui, J.; Li, F.; Shi, Z.L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Goel, S.; Polski, J.M.; Imran, H. Sensitivity and specificity of bone marrow hemophagocytosis in hemophagocytic lymphohistiocytosis. Ann. Clin. Lab. Sci. 2012, 42, 21–25. [Google Scholar] [PubMed]
- Prieto-Perez, L.; Fortes, J.; Soto, C.; Vidal-González, Á.; Alonso-Riaño, M.; Lafarga, M.; Cortti, M.J.; Lazaro-Garcia, A.; Pérez-Tanoira, R.; Trascasa, Á.; et al. Histiocytic hyperplasia with hemophagocytosis and acute alveolar damage in COVID-19 infection. Mod. Pathol. 2020, 33, 2139–2146. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kyriazopoulou, E.; Leventogiannis, K.; Norrby-Teglund, A.; Dimopoulos, G.; Pantazi, A.; Orfanos, S.E.; Rovina, N.; Tsangaris, I.; Gkavogianni, T.; Botsa, E.; et al. Macrophage activation-like syndrome: An immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017, 15, 172. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Debliquis, A.; Harzallah, I.; Mootien, J.Y.; Poidevin, A.; Labro, G.; Mejri, A.; Lamarque, M.; Kuteifan, K.; Drénou, B. Haemophagocytosis in bone marrow aspirates in patients with COVID-19. Br. J. Haematol. 2020, 190, e70–e73. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Núñez-Torrón, C.; Ferrer-Gómez, A.; Moreno Moreno, E.; Pérez-Mies, B.; Villarrubia, J.; Chamorro, S.; López-Jiménez, J.; Palacios, J.; Piris-Villaespesa, M.; García-Cosío, M. Secondary haemophagocytic lymphohistiocytosis in COVID-19: Correlation of the autopsy findings of bone marrow haemophagocytosis with HScore. J. Clin. Pathol. 2022, 75, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Purohit, A.; Vaswani, S.; Vishwajeet, V.; Kumar, D.; Vijayvergiya, P.; Tripathi, S.; Kanchan, T.; Kothari, N.; Dutt, N.; Elhence, P.; et al. Evaluation of Bone Marrow Findings of COVID-19 by Minimally Invasive Autopsies: A Single Tertiary Care Centre Experience from India. Indian J. Hematol. Blood Transfus. 2022, 38, 416–421. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- AlJabban, A.; Evans, M.G.; Fell, G.G.; Guccione, J.P.; Edwards, R.A.; Pinkus, G.S.; Padera, R.F.; Pozdnyakova, O.; Kim, A.S. Autopsy findings from patients diagnosed with COVID-19 demonstrate unique morphological patterns in bone marrow and lymph node. J. Clin. Pathol. 2023, 77, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Prilutskiy, A.; Kritselis, M.; Shevtsov, A.; Yambayev, I.; Vadlamudi, C.; Zhao, Q.; Kataria, Y.; Sarosiek, S.R.; Lerner, A.; Sloan, J.M.; et al. SARS-CoV-2 Infection-Associated Hemophagocytic Lymphohistiocytosis. Am. J. Clin. Pathol. 2020, 154, 466–474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dandu, H.; Yadav, G.; Malhotra, H.S.; Pandey, S.; Sachu, R.; Dubey, K. Hemophagocytic histiocytosis in severe SARS-CoV-2 infection: A bone marrow study. Int. J. Lab. Hematol. 2021, 43, 1291–1301. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kikuchi, A.; Singh, K.; Gars, E.; Ohgami, R.S. Pathology updates and diagnostic approaches to haemophagocytic lymphohistiocytosis. Histopathology 2022, 80, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Stehen, E.A.; Nichols, K.E.; Meyer, L.K. Insights into the cellular pathophysiology of familial hemophagocytic lymphohistiocytosis. Front. Immunol. 2023, 14, 1147603. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wilson, C.; Lee, W.I.; Cook, M.C.; Smyth, L.; Talaulikar, D. Correlation of haemophagocytosis with clinical criteria of haemophagocytic lymphohistiocytosis and recommendations for bone marrow reporting. Pathology 2022, 54, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Deinhardt-Emmer, S.; Wittschieber, D.; Sanft, J.; Kleemann, S.; Elschner, S.; Haupt, K.F.; Vau, V.; Häring, C.; Rödel, J.; Henke, A.; et al. Early postmortem mapping of SARS-CoV-2 RNA in patients with COVID-19 and the correlation with tissue damage. eLife 2021, 10, e60361. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stein, S.R.; Ramelli, S.C.; Grazioli, A.; Chung, J.Y.; Singh, M.; Yinda, C.K.; Winkler, C.W.; Sun, J.; Dickey, J.M.; Ylaya, K.; et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022, 612, 758–763. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Birndt, S.; Schenk, T.; Heinevetter, B.; Brunkhorst, F.M.; Maschmeyer, G.; Rothmann, F.; Weber, T.; Müller, M.; Panse, J.; Penack, O.; et al. Hemophagocytic lymphohistiocytosis in adults: Collaborative analysis of 137 cases of a nationwide German registry. J. Cancer Res. Clin. Oncol. 2020, 146, 1065–1077. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Pat.No. | Age [Years] | Sex | BMI [kg/m2] | Hospitalization [Days] | Ventilation/ECMO [Days] | Key Comorbidity |
|---|---|---|---|---|---|---|
| 1 | 82 | m | 26.1 | 8 | 8/0 | Diabetes type 2 |
| 2 | 66 | m | 31.6 | 6 | 5/0 | Hypertension |
| 3 | 77 | m | 25.2 | 37 | 8/0 | Diabetes type 2 |
| 4 | 54 | m | 26.6 | 11 | 6/2 | Chronic lymphatic leukemia |
| 5 | 80 | m | 44.2 | 7 | 7/0 | Diabetes type 2 |
| 6 | 87 | w | 25.1 | 13 | 0/0 | Diabetes type 2 |
| 7 | 82 | w | 26.3 | 1 | 0/0 | Liver cirrhosis |
| 8 | 83 | w | 25.1 | 7 | 0/0 | Diabetes type 2 |
| 9 | 85 | w | 23.7 | 10 | 0/0 | Esophageal squamous carcinoma |
| 10 | 52 | w | 25.8 | 5 | 0/0 | Adenocarcinoma of the colon |
| 11 | 64 | m | 34.6 | 20 | 16/0 | Chronic obstructive lung disease |
| 12 | 64 | m | 33.2 | 15 | 20/9 | - |
| 13 | 81 | m | 32.2 | 31 | 0/0 | Prostatic carcinoma |
| 14 | 80 | m | 24.1 | 4 | 4/0 | Diabetes type 2 |
| 15 | 61 | m | 28.5 | 56 | 16/40 | - |
| 16 | 86 | m | 26.9 | 6 | 0/0 | Prostatic carcinoma |
| 17 | 84 | w | 21.5 | 3 | 0/0 | Adenocarcinoma of the rectum |
| 18 | 80 | m | 27.1 | 27 | 26/0 | Hypertension |
| 19 | 85 | w | 43.1 | 9 | 0/0 | Amyloidosis |
| 20 | 78 | m | 32.1 | 16 | 11/0 | Prostatic carcinoma |
| 21 | 79 | m | 29.4 | 22 | 19/0 | Hypertension |
| 22 | 83 | m | 25.7 | 1 | 0/0 | Diabetes type 2 |
| 23 | 66 | m | 25.7 | 11 | 7/0 | Liposarcoma |
| 24 | 83 | w | 35.2 | 9 | 8/0 | Hypertension |
| 25 | 58 | m | 38.7 | 9 | 8/0 | Adenocarcinoma of the rectum |
| 26 | 80 | m | 36.1 | 19 | 16/0 | Hypertension |
| 27 | 62 | w | 29.7 | 15 | 0/0 | Hepatocellular carcinoma |
| 28 | 58 | m | 32.5 | 8 | 0/0 | - |
| Pat.No. | HLH Score | Number of Hemophagocytes in | |||||
|---|---|---|---|---|---|---|---|
| Bone Marrow | All Lymph Nodes | Hilar Lymph Nodes | Cervical Lymph Nodes | Para-aortic Lymph Nodes | Inguinal/Mesenterial Lymph Nodes | ||
| 1 | 146 | 1 | 3 | 3 | 0 | N/A | 0 |
| 2 | 191 | 4 | 35 | 13 | 22 | N/A | 0 |
| 3 | 127 | 2 | 26 | 2 | 16 | N/A | 8 |
| 4 | 160 | 1 | 11 | 7 | 4 | 0 | 0 |
| 5 | 54 | 0 | 38 | 20 | 7 | 11 | 0 |
| 6 | 68 | 5 | 6 | 1 | 2 | 3 | 0 |
| 7 | 47 | 0 | 21 | 0 | 5 | 6 | 10 |
| 8 | 35 | 38 | 7 | 1 | 1 | 5 | 0 |
| 9 | 35 | 7 | 9 | 5 | 3 | 0 | 1 |
| 10 | 54 | 7 | 9 | 4 | 1 | 2 | 2 |
| 11 | 95 | 0 | 27 | 8 | 3 | 6 | 10 |
| 12 | 19 | 0 | 11 | 4 | 2 | 1 | 4 |
| 13 | 42 | 0 | 31 | 25 | 3 | 0 | 3 |
| 14 | 112 | 9 | 38 | 13 | 10 | 15 | 0 |
| 15 | 84 | 19 | 68 | 32 | 13 | 3 | 20 |
| 16 | 91 | 0 | 5 | 2 | 3 | 0 | 0 |
| 17 | 56 | 0 | 2 | 0 | 0 | 1 | 1 |
| 18 | 106 | 26 | 71 | 52 | 19 | 0 | N/A |
| 19 | 68 | 3 | 25 | 9 | 10 | 0 | 6 |
| 20 | 106 | 4 | 21 | 3 | 10 | 8 | 0 |
| 21 | 107 | 35 | 105 | 49 | 33 | 13 | 10 |
| 22 | 58 | 0 | 17 | 10 | 0 | 5 | 2 |
| 23 | 35 | 13 | 72 | 35 | 19 | 18 | N/A |
| 24 | 91 | 0 | 5 | 0 | 5 | 0 | 0 |
| 25 | 107 | 7 | 56 | 41 | 3 | 10 | 2 |
| 26 | 35 | 0 | 11 | 11 | 0 | 0 | 0 |
| 27 | 126 | 7 | 39 | 17 | 9 | 13 | N/A |
| 28 | 58 | 3 | 11 | 3 | 3 | 5 | 0 |
| Total | 191 | 780 | 370 | 206 | 125 | 79 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jusovic-Stocanin, A.; Kaemmerer, E.; Ihle, H.; Autsch, A.; Kleemann, S.; Sanft, J.; Hubig, M.; Mall, G.; Gassler, N. Hemophagocytosis of the Hilar Pulmonary Lymph Nodes Is a More Sensitive Indicator of the Severity of COVID-19 Disease than Bone Marrow Hemophagocytosis. Diseases 2024, 12, 241. https://doi.org/10.3390/diseases12100241
Jusovic-Stocanin A, Kaemmerer E, Ihle H, Autsch A, Kleemann S, Sanft J, Hubig M, Mall G, Gassler N. Hemophagocytosis of the Hilar Pulmonary Lymph Nodes Is a More Sensitive Indicator of the Severity of COVID-19 Disease than Bone Marrow Hemophagocytosis. Diseases. 2024; 12(10):241. https://doi.org/10.3390/diseases12100241
Chicago/Turabian StyleJusovic-Stocanin, Amira, Elke Kaemmerer, Hannah Ihle, Angelina Autsch, Sandra Kleemann, Juliane Sanft, Michael Hubig, Gita Mall, and Nikolaus Gassler. 2024. "Hemophagocytosis of the Hilar Pulmonary Lymph Nodes Is a More Sensitive Indicator of the Severity of COVID-19 Disease than Bone Marrow Hemophagocytosis" Diseases 12, no. 10: 241. https://doi.org/10.3390/diseases12100241