
Ambulances Deployment Problems: Categorization, Evolution and Dynamic Problems Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
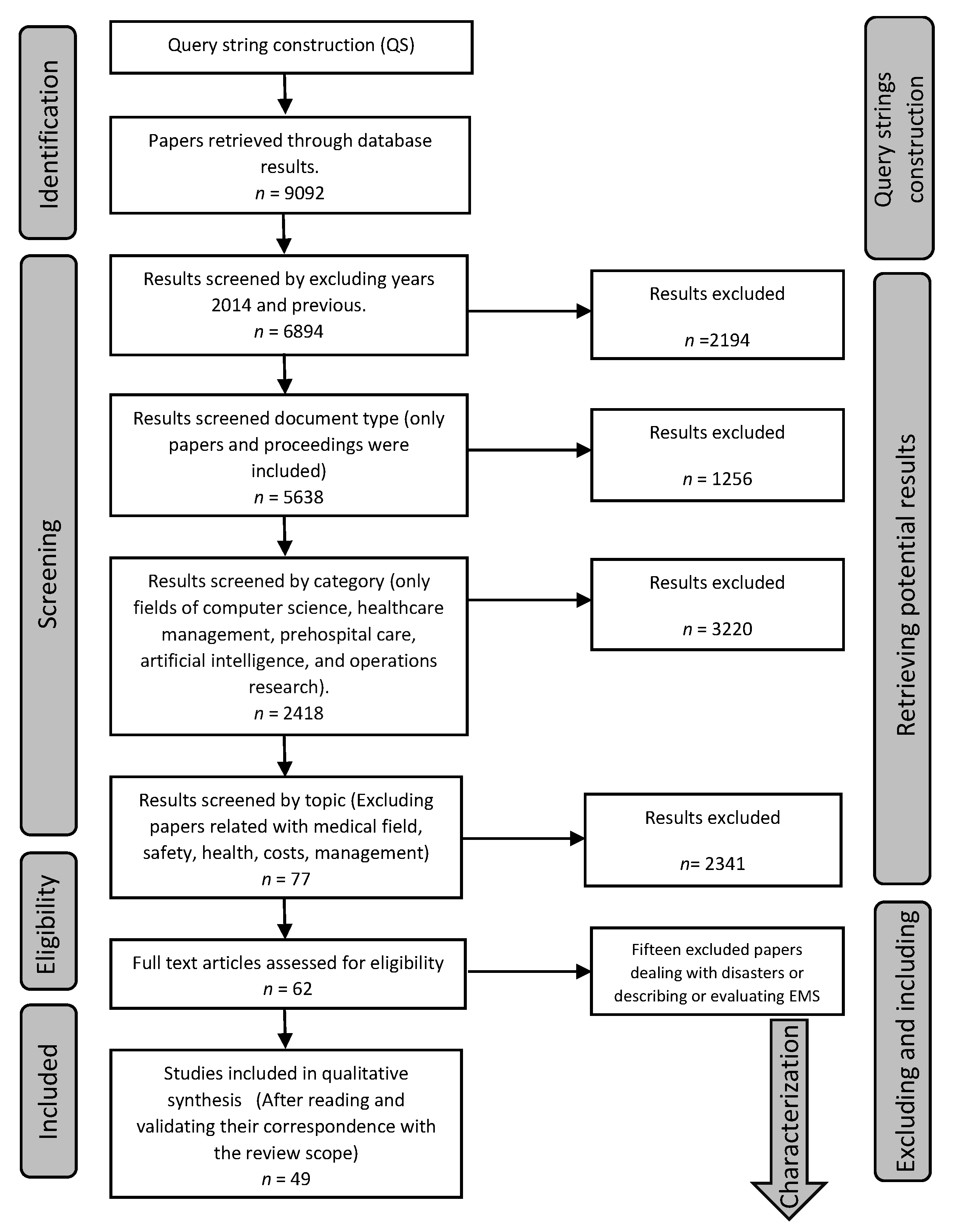
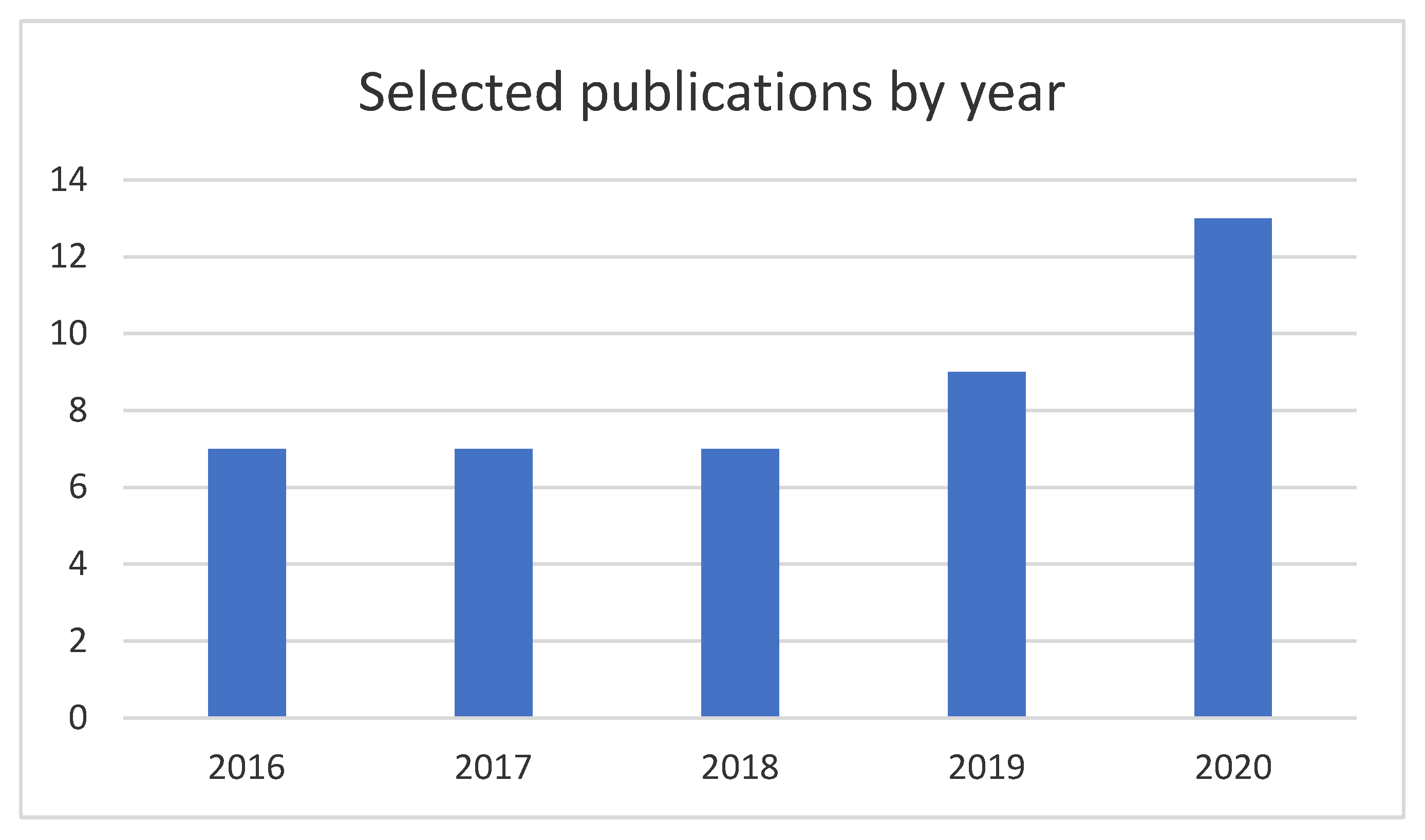
2. Review Methodology
- Tackled problem;
- Model used;
- Optimization objective;
- Optimization tools;
- Results.
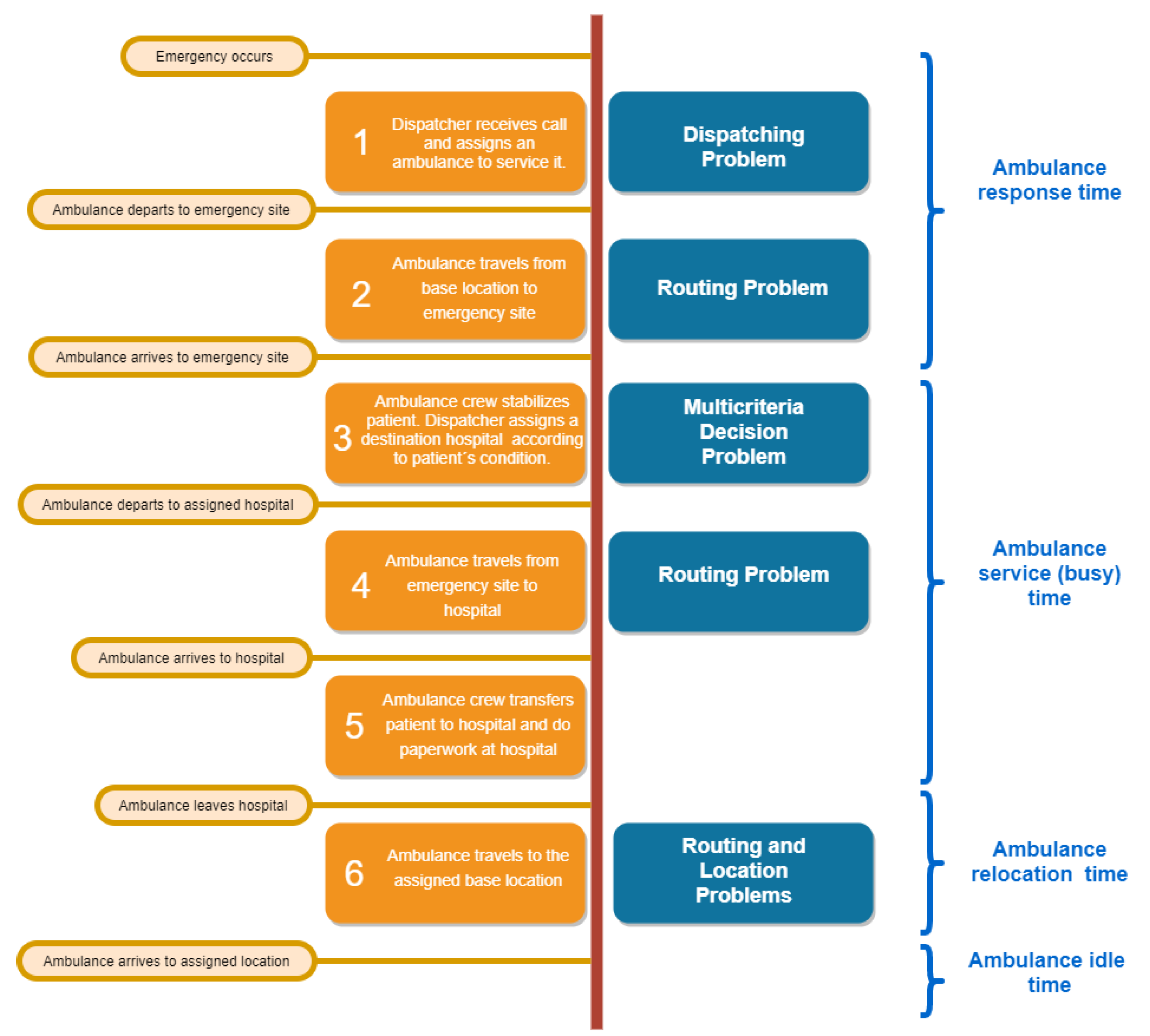
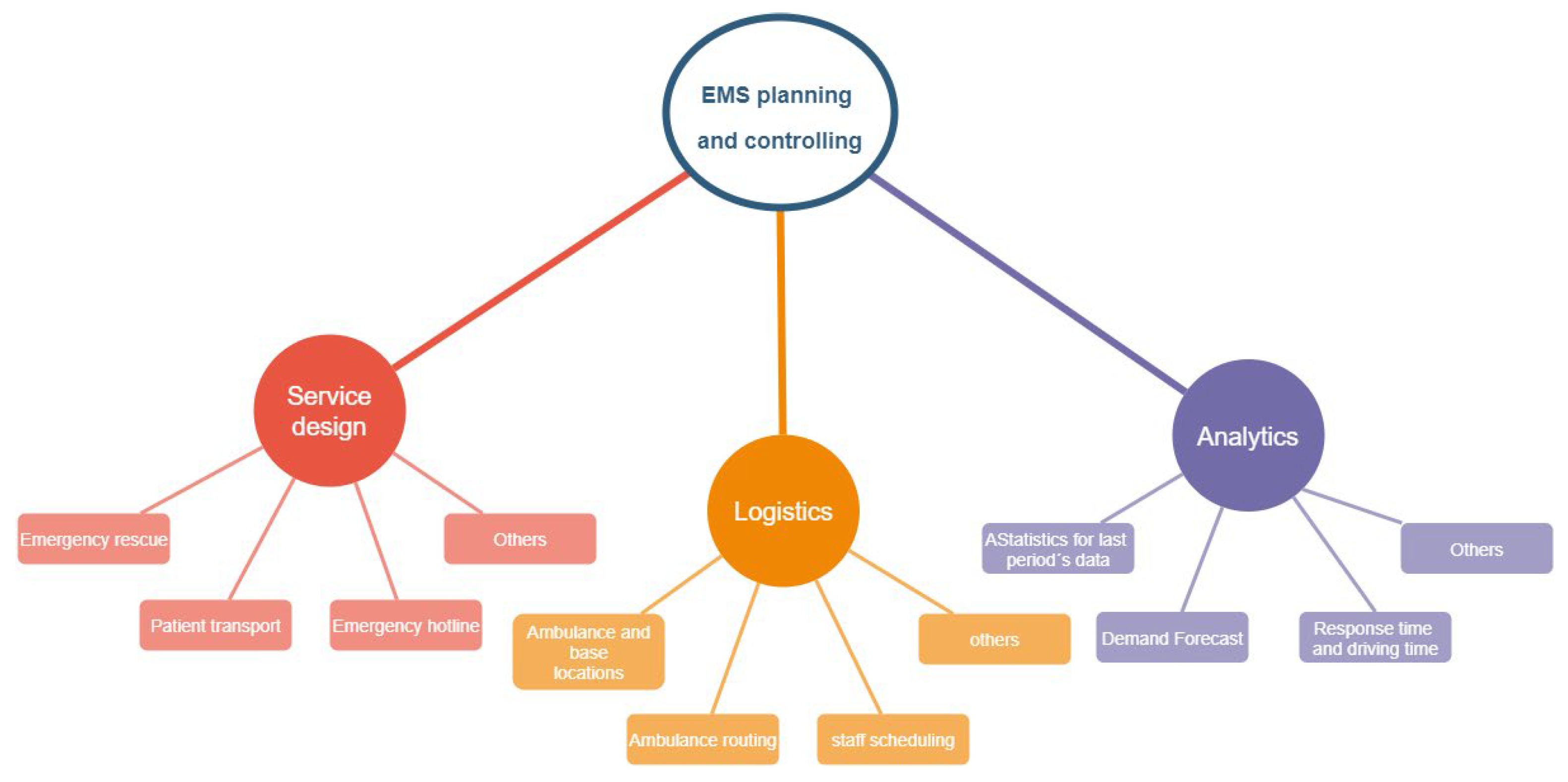
3. The Ambulance Service Process
4. Ambulance Location and Routing Problems Classification
- SL—for static location or deployment problems. This fact means that ambulances have a fixed location or base point through time.
- DL—for dynamic location problems. This fact refers to situations in which the ambulances change their position over time.
- BER—for routing problems considering base to emergency site routing.
- EHR—for routing problems considering an emergency site to hospital routing.
- HLR—for routing problems considering hospital to location routing.
- FR—for complete routing problems, i.e., includes the three routing problems.
- VF—for problems considering vehicle failures.
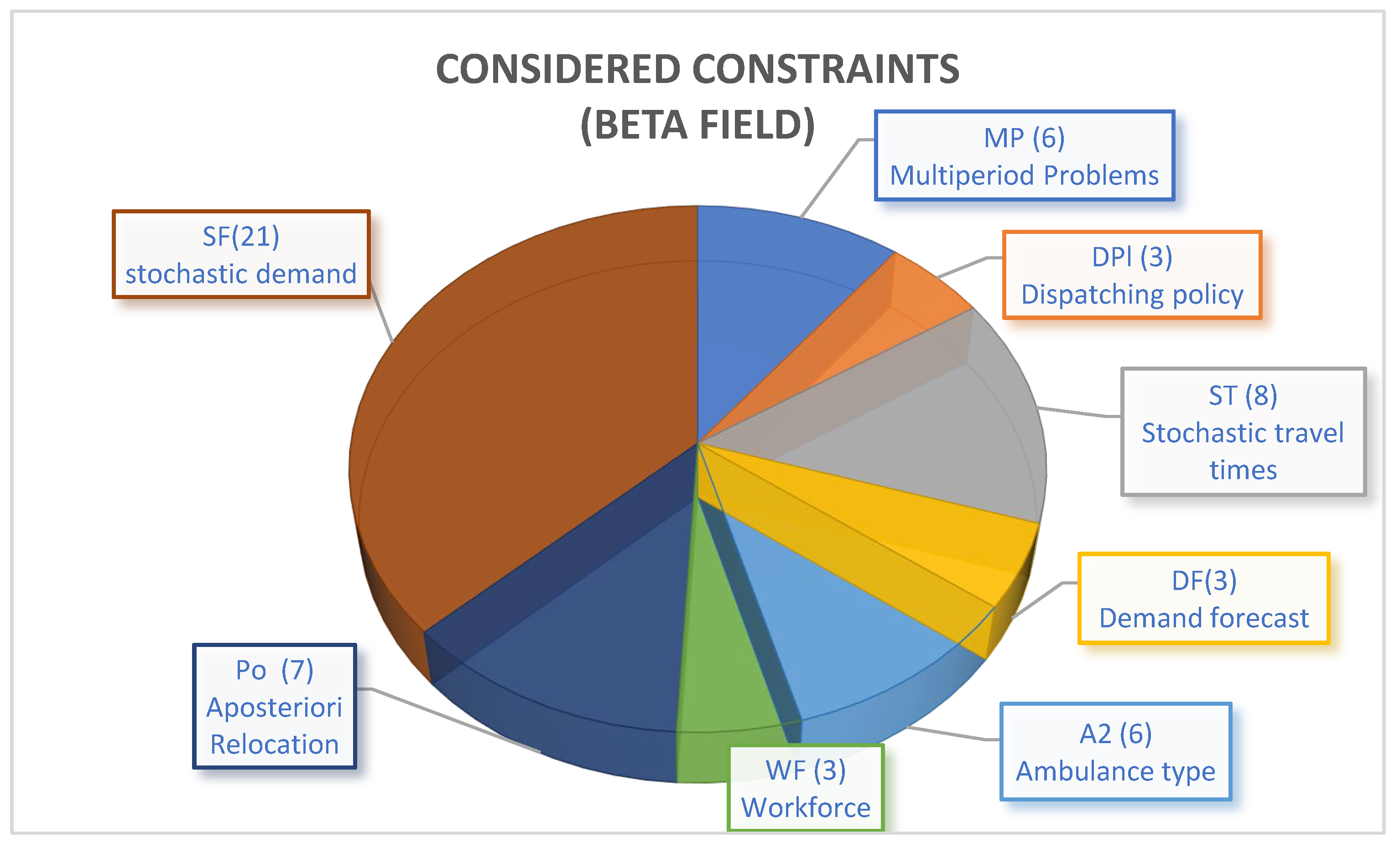
- MP—for multiperiod problems.
- Po—for problems considering relocation as a consequence of emergency events.
- DPl—for problems involving issues related to the dispatching policy.
- WF—for problems considering workforce shifts and workdays.
- SF—for problems addressing scenarios with stochastic demand.
- DF—for problems considering the demand forecast.
- ST—for problems considering stochastic routing times.
- RS—for problems considering the resilience of the system.
- At—for problems considering the ambulance type. For example, if the problem is A1—all the ambulances considered in the model are equal, i.e., there is one type of ambulance in the model. If the model is A2, there are two types of ambulances (ALS and BLS).
- BU—for problems considering Back-Up ambulances, such as double standard problems.
- FI—for problems considering financial issues.
- PS—probability of survival (maximization).
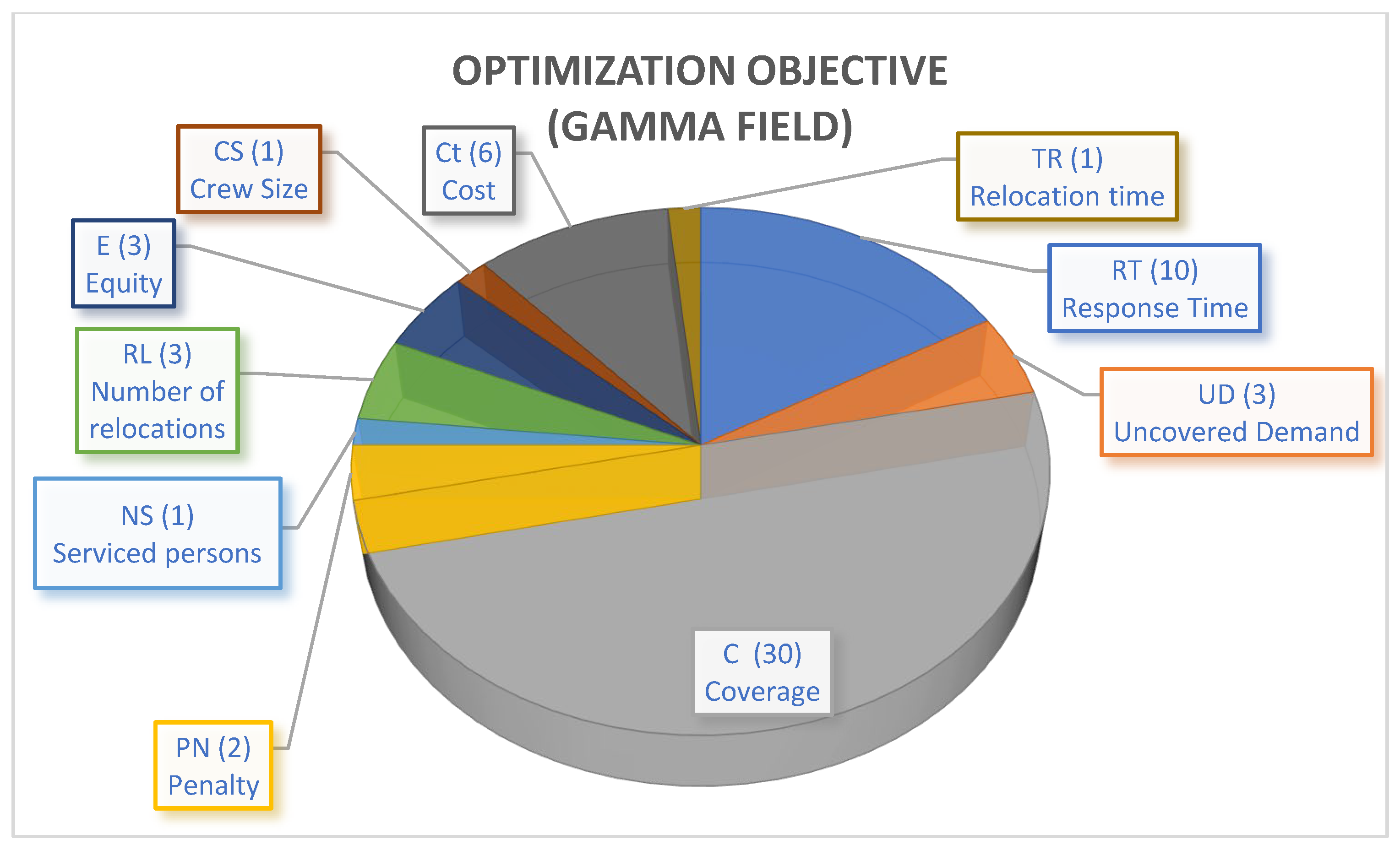
- E—equity (maximization).
- NS—number of serviced persons (maximization).
- RT—response time (minimization).
- D—distance (minimization).
- C—coverage (maximization).
- PN—penalty (minimization).
- UD—uncovered demand (minimization).
- S—survivors (maximization).
- RL—number of relocations (minimization).
- CS—crew size (minimization).
- Ct—cost (minimization).
- TR—relocation time (minimization).
5. Ambulance Location Problems
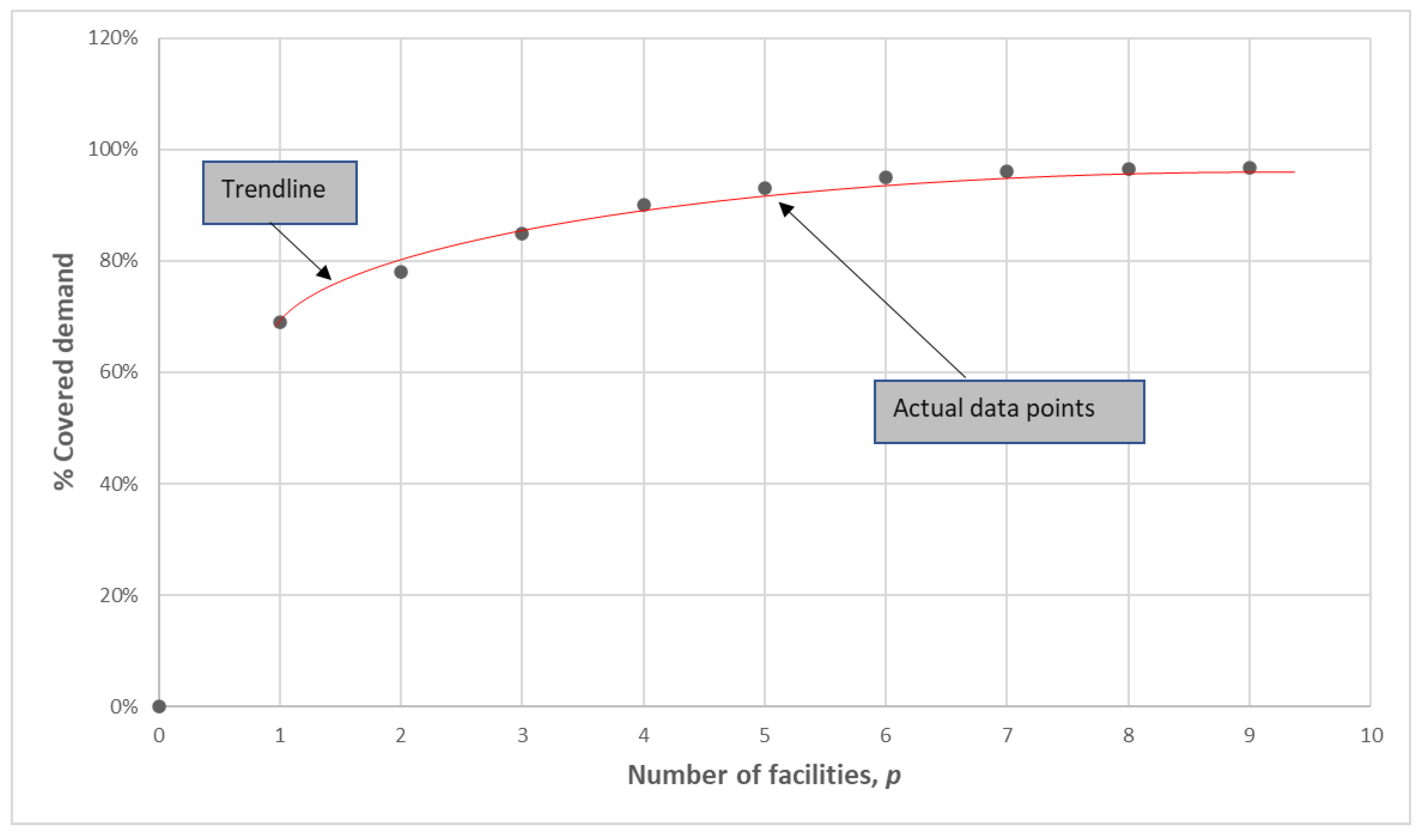
5.1. Basic Static Problems
5.2. Probabilistic Static Approaches
5.3. Gradual Coverage in Static Approaches
5.4. Dynamic Approaches
5.4.1. Dispatching Policies
5.4.2. Modeling Issues
5.4.3. Optimization Objectives
5.4.4. Fleet Type
5.4.5. Location Capacity
5.4.6. Solution Approaches
6. Concluding Remarks and Future Directions
6.1. Holistic Models
6.2. Algorithms for More Extensive and Realistic Models
6.3. Absence of Open Datasets
6.4. Artificial Intelligence and Machine Learning
6.5. Resilience
6.6. Models for Rural Areas
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A. Main Contributions to Ambulance Dynamic Location Problems
| Authors | Additional Considerations | Objective (s) | Solution Approach | Triplet Notation | ||
| α | β | γ | ||||
| Van Barneveld [106] | Compliance tables, relocalization | Expected penalty relocation | MILP/CPLEX | DL | MP | PN |
| Jagtenberg et al. [85] | NA | Fraction of arrival later than the target time | Markov decision process | DL | DPl | UD |
| Jagtenberg et al. [65] | NA | Fraction of late arrivals | Heuristic approach | DL | UD | |
| Van Barneveld et al. [68] | Compliance tables, relocalization | Covered demand | MILP/CPLEX | DL | MP-DPl | C |
| Van Barneveld et al [73] | Compliance tables, relocalization | Response time | Heuristic based different metrics | DL | MP-DPl | RT |
| Van Barneveld et al [109] | Linear bottleneck assignment problem | Response time | Heuristic-based different metrics | DL | DPl | RT |
| Degel et al. [103] | Time-dependent data | Coverage | MILP/Fico Xpress | DL | ST | C |
| Andrade and Cunha [104] | Time-dependent variations in travel time | Double coverage and minimization of relocation cost | MILP/artificial bee colony algorithm | DL | A2-ST | C-Ct |
| Lam et al. [105] | GIS data | Double coverage | MILP/CPLEX and geographical analysis | DL | DF | Ct |
| Van den Berg et al. [90] | Time dependency demand, availability. multiperiod | Expected coverage, minimization of the number of locations, and relocation cost | MILP/CPLEX | SL | MP-DF | C-RL |
| McCormack and Coates [94] | Survival function, travel times, vehicle availability | Survival probability | Nonlinear problem/genetic algorithm | DL | A2 | S |
| Enayati et al. [110] | Stochastic demand | Coverage and total relocation time | MILP/genetic algorithm | DL | SF | C-RL |
| Yoon and Albert [136] | Realtime | Expected coverage and suitability of sent ambulance | Markov decision process | DL | A2 | C |
| Andersson et al. [141] | NA | Coverage, survival | MILP/Xpress | DL | A2 | |
| Boujemaa et al. [126] | Uncertainty of demand | Costs, penalty for unsatisfied demand | MILP/CPLEX | DL | SF-MP-A2 | Ct-UD |
| Tsai et al. [89] | Stochasticity of demand | Coverage, relocation cost, equity | Nonlinear/PSO | DL | SF | Ct-C-E |
| Peng et al. [114] | Stochasticity of demand | Cost | MILP/chance constrained programming heuristic | DL | SF | Ct |
| Carvalho et al. [76] | NA | Coverage, preparedness | Heuristic approach | DL | C-RT | |
| Belanger et al. [142] | NA | Response time | MILP/PLEX and simulation | DL | RT | |
| Enayati et al. [88] | Stochasticity of demand | Gini, response time, coverage, workload, probability of loss | Nonlinear model/NSGA | DL | SF | E-RT-C-CS |
| Lee [77] | NA | Gini index, welfare | Heuristic approach | DL | RT-E | |
| van Barneveld et al. [82] | Redeployment, busy ambulances in system status, crew workload | Percentage on time, response time, relocation time, coverage | Heuristic approach | DL | WF-Po | RT-C-NS-RL |
| Peyravi et al. [112] | Temporary locations | Response time | Heuristic approach | DL | Po | RT |
| Dolejs et al. [130] | Stochastic travel times | Coverage | Random forest | ST | C | |
| Ji et al. [116] | Stochastic demand, stochastic travel times | Coverage | Optimal matching algorithm, based on different metrics | DL | ST-SF | C |
| Boutilier and Chan [117] | Stochastic demand and travel times, dispatching rules | Response time | MILP/Gurobi, two-stage robust optimization | DL | SF-DF-ST | RT |
| Roa et al. [75] | Realtime information | Coverage, relocation time | MILP/CPLEX, Matheuristic approach | DL | SF-Po | C-TR |
| Sun et al. [137] | Realtime information | Response time | Heuristic approach | DL | Po | RT |
| Yuangyai et al. [138] | Realtime, social networks | Coverage | Nonlinear optimization | DL | Po-SF | C |
| Mohri et al. [153] | NA | Coverage | Data envelope analysis/MILP | DL | C | |
| Abensur et al. [95] | Stochastic demand, competition between providers | Penalty function, considering financial issues, and customer loss function | Game theory, simulation. | DL | FI-SF-WF | PN |
| Asim et al. [113] | Stochastic demand | Coverage | Spatial analysis with GIS | DL | SF | C |
| Park and Lee [86] | Stochastic demand | Survival | Approximate dynamic programming/Markov decision process | DL | SF | S |
| Bertsimas et al. [118] | Stochasticity of demand | Coverage | MILP/Gurobi robust optimization, column generation, row generation | DL | SF | C |
| Nilsang et al. [139] | Realtime information, social networks (twitter) | Coverage | MILP | DL | SF-Po | C |
| Janosikova et al. [81] | Stochasticity of demand | Coverage | MILP/Xpress, simulation | DL | SF- A2 | C |
| Grekousis and Liu [119] | Stochasticity of demand | Coverage | Random forest | |||
| El Itani et al. [120] | Stochasticity of demand | Coverage, cost | MILP | DL | SF | C-Ct |
| Firooze and Rafiee et al. [146] | Unavailability time, relocation | Coverage | MILP/CPLEX | DL | C | |
| van Buuren et al. [140] | Realtime | Coverage | Heuristic approach | DL | Po | C |
| Enayati at al. [121] | Stochastic demand, workforce workload | Coverage | MILP/Lagrangian branch and bound | DL | SF-WF | C |
| Coelho et al. [154] | NA | Coverage | MILP/CPLEX | DL | C | |
| Lam et al. [122] | Stochastic demand, stochastic travel times | Coverage | Approximate dynamic programming | DL | SF-ST | C |
| Calderin et al. [148] | NA | Coverage | MILP/simulated annealing | DL | MP | C |
| Ansari et al. [123] | Stochastic demand and travel times | Coverage | MILP/Gurobi, hypercube model | DL | SF-ST | C |
| Drezner et al. [124] | Stochastic demand and travel times | Coverage | MILP/CPLEX | DL | ST-SF | C |
| Moeini et al. [125] | Stochastic demand | Coverage | MILP/CPLEX | DL | SF | C |
| Sudtachat et al. [67] | Stochastic demand | Coverage | MILP/CPLEX | DL | SF | C |
References
- Ortiz-Barrios, M.; Neira-Rodado, D.; Jiménez-Delgado, G.; McClean, S.; Lara, O. Definition of Strategies for the Reduction of Operational Inefficiencies in a Stroke Unit; Lecture Notes in Computer Science, Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics; Springer: Berlin/Heidelberg, Germany, 2018; Volume 1, pp. 488–500. [Google Scholar] [CrossRef]
- Schwarz, A.M.; Arias, O.S.; Zviniene, A.; Rudolph, H.P.; Eckardt, S.; Koettl, J.; Immervoll, H.; Abels, M. The Inverting Pyramid: Pension Systems Facing Demographic Challenges in Europe and Central Asia; World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Tamblyn, R.; McMahon, M.; Nadigel, J.; Dunning, B.; Drake, E. Health System Transformation through Research Innovation. HealthcarePapers 2016, 16, 8–20. [Google Scholar]
- Schmid, V.; Doerner, K.F. Ambulance location and relocation problems with time-dependent travel times. Eur. J. Oper. Res. 2010, 207, 1293–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez, A.K.; Osorno, G.M.; Maya, P.A. Relocalización de vehículos en servicios de emergencias médicas: A revisión. Ing. Cienc. 2016, 12, 163–202. [Google Scholar] [CrossRef] [Green Version]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef] [Green Version]
- Schmid, V. Solving the dynamic ambulance relocation and dispatching problem using approximate dynamic programming. Eur. J. Oper. Res. 2012, 219, 611–621. [Google Scholar] [CrossRef] [Green Version]
- Sundberg, G.; Bagust, A.; Terént, A. A model for costs of stroke services. Health Policy 2003, 63, 81–94. [Google Scholar] [CrossRef]
- McClean, S.; Gillespie, J.; Garg, L.; Barton, M.; Scotney, B.; Kullerton, K. Using phase-type models to cost stroke patient care across health, social and community services. Eur. J. Oper. Res. 2014, 236, 190–199. [Google Scholar] [CrossRef]
- World Health Organization. Cardiovascular Diseases (CVDs). 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 5 November 2019).
- Hernandez, B.; Benjumea, P.; Tuso, L. Physical Therapy clinical performance indicators in the early hospital management cerebrovascular attack (CVA). Rev. Cienc. Salud 2013, 11, 7–34. [Google Scholar]
- Sackley, C.; Pound, K. Setting priorities for a discharge plan for stroke patients entering nursing home care. Clin. Rehabil. 2002, 16, 859–866. [Google Scholar] [CrossRef]
- Bürger, A.; Wnent, J.; Bohn, A.; Jantzen, T.; Brenner, S.; Lefering, R.; Seewald, S.; Gräsner, J.-T.; Fischer, M. Effect of Ambulance Response Time on Survival Following Out-of-Hospital Cardiac Arrest an Analysis from the German Resuscitation Registry. Dtsch. Arztebl. Int. 2018, 115, 541–550. [Google Scholar] [CrossRef]
- Ingolfsson, A.; Budge, S.; Erkut, E. Optimal ambulance location with random delays and travel times. Health Care Manag. Sci. 2008, 11, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Budge, S.; Ingolfsson, A.; Zerom, D. Empirical Analysis of Ambulance Travel Times: The Case of Calgary Emergency Medical Services. Manag. Sci. 2010, 56, 716–723. [Google Scholar] [CrossRef]
- Church, R.L.; Murray, A. Location Covering Models: History, Applications and Advancements; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Bowling, A. Mode of questionnaire administration can have serious effects on data quality. J. Public Health 2005, 27, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Comas, A.; Synnes, K.; Hallberg, J. Hardware for Recognition of Human Activities: A Review of Smart Home and AAL Related Technologies. Sensors 2020, 20, 4227. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Waltman, L. Large-scale analysis of the accuracy of the journal classification systems of Web of Science and Scopus. J. Inf. 2016, 10, 347–364. [Google Scholar] [CrossRef] [Green Version]
- Zaric, G. Operations Research and Health Care Policy; Springer: Berlin/Heidelberg, Germany, 2013; Volume 190. [Google Scholar]
- Reuter-Oppermann, M.; Berg, P.V.D.; Vile, J.L. Logistics for Emergency Medical Service systems. Health Syst. 2017, 6, 187–208. [Google Scholar] [CrossRef] [Green Version]
- Hakimi, S.L. Optimum Locations of Switching Centers and the Absolute Centers and Medians of a Graph. Oper. Res. 1964, 12, 450–459. [Google Scholar] [CrossRef]
- Toregas, C.; Swain, R.; Revelle, C.; Bergman, L. The Location of Emergency Service Facilities. Oper. Res. 1971, 19, 1363–1373. [Google Scholar] [CrossRef]
- Toregas, C.; ReVelle, C. Optimal location under time or distance constraints. Pap. Reg. Sci. 1972, 28, 131–143. [Google Scholar] [CrossRef]
- Church, R.; Revelle, C. The maximal covering location problem. Pap. Reg. Sci. 1974, 32, 101–118. [Google Scholar] [CrossRef]
- Daskin, M.S.; Stern, E.H. A Hierarchical Objective Set Covering Model for Emergency Medical Service Vehicle Deployment. Transp. Sci. 1981, 15, 137–152. [Google Scholar] [CrossRef]
- Hogan, K.; ReVelle, C. Concepts and Applications of Backup Coverage. Manag. Sci. 1986, 32, 1434–1444. [Google Scholar] [CrossRef]
- Moon, I.D.; Chaudhry, S. An Analysis of Network Location Problems with Distance Constraints. Manag. Sci. 1984, 30, 290–307. [Google Scholar] [CrossRef]
- Revelle, C.; Schweitzer, J.; Snyder, S. The Maximal Conditional Covering Problem. INFOR Inf. Syst. Oper. Res. 1996, 34, 77–91. [Google Scholar] [CrossRef]
- Gendreau, M.; Laporte, G.; Semet, F. Solving an ambulance location model by tabu search. Locat. Sci. 1997, 5, 75–88. [Google Scholar] [CrossRef]
- Laporte, G.; Louveaux, F.V.; Semet, F.; Thirion, A. Applications of the double standard model for ambulance location. In Innovations in Distribution Logistics; Springer: Berlin/Heidelberg, Germany, 2009; pp. 235–249. [Google Scholar] [CrossRef]
- Zarandi, M.H.F.; Davari, S.; Sisakht, S.A.H. The large-scale dynamic maximal covering location problem. Math. Comput. Model. 2013, 57, 710–719. [Google Scholar] [CrossRef]
- Chapman, S.; White, J. Probabilistic Formulation of the Emergency Service Facilities Location Problems; Springer: Berlin/Heidelberg, Germany, 1974. [Google Scholar]
- Daskin, M. A Maximum Expected Covering Location Model: Formulation, Properties and Heuristic Solution. Transp. Sci. 1983, 17, 48–70. [Google Scholar] [CrossRef] [Green Version]
- Larson, R.C. A hypercube queuing model for facility location and redistricting in urban emergency services. Comput. Oper. Res. 1974, 1, 67–95. [Google Scholar] [CrossRef]
- Mandell, M.B. Covering models for two-tiered emergency medical services systems. Locat. Sci. 1998, 6, 355–368. [Google Scholar] [CrossRef]
- Batta, R.; Dolan, J.M.; Krishnamurthy, N.N. The Maximal Expected Covering Location Problem: Revisited. Transp. Sci. 1989, 23, 277–287. [Google Scholar] [CrossRef]
- Goldberg, J.; Dietrich, R.; Chen, J.M.; Mitwasi, M.; Valenzuela, T.; Criss, E. Validating and applying a model for locating emergency medical vehicles in Tuczon, AZ. Eur. J. Oper. Res. 1990, 49, 308–324. [Google Scholar] [CrossRef]
- Marianov, V.; ReVelle, C. The Queueing Maximal availability location problem: A model for the siting of emergency vehicles. Eur. J. Oper. Res. 1996, 93, 110–120. [Google Scholar] [CrossRef]
- Baron, O.; Berman, O.; Kim, S.; Krass, D. Ensuring feasibility in location problems with stochastic demands and congestion. IIE Trans. 2009, 41, 467–481. [Google Scholar] [CrossRef]
- Marianov, V.; Serra, D. Probabilistic, Maximal Covering Location—Allocation Models for Congested Systems. J. Reg. Sci. 1998, 38, 401–424. [Google Scholar] [CrossRef]
- Revelle, C.; Hogan, K. The Maximum Availability Location Problem. Transp. Sci. 1989, 23, 192–200. [Google Scholar] [CrossRef]
- Aytug, H.; Saydam, C. Solving large-scale maximum expected covering location problems by genetic algorithms: A comparative study. Eur. J. Oper. Res. 2002, 141, 480–494. [Google Scholar] [CrossRef]
- Daskin, M.; Hogan, K.; Revelle, C. Integration of Multiple, Excess, Backup, and Expected Covering Models. Environ. Plan. B Plan. Des. 1988, 15, 15–35. [Google Scholar] [CrossRef]
- Saydam, C.; Rajagopalan, H.K.; Sharer, E.; Lawrimore-Belanger, K. The dynamic redeployment coverage location model. Health Syst. 2013, 2, 103–119. [Google Scholar] [CrossRef]
- Sorensen, P.; Church, R. Integrating expected coverage and local reliability for emergency medical services location problems. Socio-Econ. Plan. Sci. 2010, 44, 8–18. [Google Scholar] [CrossRef]
- Erkut, E.; Ingolfsson, A.; Sim, T.; Erdoğan, G. Computational Comparison of Five Maximal Covering Models for Locating Ambulances. Geogr. Anal. 2009, 41, 43–65. [Google Scholar] [CrossRef]
- Lightner, C.; Graham, J.M.; Lightner, C.A. A Heuristic Approach for Locating EMS Facilities and Vehicle. In Proceedings of the PDPTA, Las Vegas, NV, USA, 26–29 June 2006; pp. 334–339. [Google Scholar]
- Erkut, E.; Ingolfsson, A.; Erdoğan, G. Ambulance location for maximum survival. Nav. Res. Logist. (NRL) 2008, 55, 42–58. [Google Scholar] [CrossRef]
- Church, R.L.; Roberts, K.L. Generalized coverage models and public facility location. Pap. Reg. Sci. 1983, 53, 117–135. [Google Scholar] [CrossRef]
- Schilling, D.; Elzinga, J.; Cohon, J.; Church, R.; Revelle, C. The Team/Fleet Models for Simultaneous Facility and Equipment Siting. Transp. Sci. 1979, 13, 163–175. [Google Scholar] [CrossRef]
- Murray, A.T. Geography in Coverage Modeling: Exploiting Spatial Structure to Address Complementary Partial Service of Areas. Ann. Assoc. Am. Geogr. 2005, 95, 761–772. [Google Scholar] [CrossRef]
- Drezner, T.; Drezner, Z.; Goldstein, Z. A stochastic gradual cover location problem. Nav. Res. Logist. 2010, 57, 367–372. [Google Scholar] [CrossRef]
- Berman, O.; Drezner, Z.; Krass, D.; Wesolowsky, G.O. The variable radius covering problem. Eur. J. Oper. Res. 2009, 196, 516–525. [Google Scholar] [CrossRef]
- Berman, O.; Krass, D.; Drezner, Z. The gradual covering decay location problem on a network. Eur. J. Oper. Res. 2003, 151, 474–480. [Google Scholar] [CrossRef]
- Peker, M.; Kara, B.Y. The P-Hub maximal covering problem and extensions for gradual decay functions. Omega 2015, 54, 158–172. [Google Scholar] [CrossRef] [Green Version]
- Restrepo, M.; Henderson, S.; Topaloglu, H. Erlang loss models for the static deployment of ambulances. Health Care Manag. Sci. 2009, 12, 67–79. [Google Scholar] [CrossRef]
- Davari, S.; Zarandi, M.H.F.; Hemmati, A. Maximal covering location problem (MCLP) with fuzzy travel times. Expert Syst. Appl. 2011, 38, 14535–14541. [Google Scholar] [CrossRef]
- Yin, P.; Mu, L. Modular capacitated maximal covering location problem for the optimal siting of emergency vehicles. Appl. Geogr. 2012, 34, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Gendreau, M.; Laporte, G.; Semet, F. The maximal expected coverage relocation problem for emergency vehicles. J. Oper. Res. Soc. 2006, 57, 22–28. [Google Scholar] [CrossRef]
- Brotcorne, L.; Laporte, G.; Semet, F. Ambulance location and relocation models. Eur. J. Oper. Res. 2003, 147, 451–463. [Google Scholar] [CrossRef]
- Wu, C.-H.; Hwang, K.P. Using a Discrete-event Simulation to Balance Ambulance Availability and Demand in Static Deployment Systems. Acad. Emerg. Med. 2009, 16, 1359–1366. [Google Scholar] [CrossRef]
- Maxwell, M.S.; Restrepo, M.; Henderson, S.; Topaloglu, H. Approximate Dynamic Programming for Ambulance Redeployment. INFORMS J. Comput. 2010, 22, 266–281. [Google Scholar] [CrossRef] [Green Version]
- Gendreau, M.; Laporte, G.; Semet, F. A dynamic model and parallel tabu search heuristic for real-time ambulance relocation. Parallel Comput. 2001, 27, 1641–1653. [Google Scholar] [CrossRef] [Green Version]
- Jagtenberg, C.; Bhulai, S.; van der Mei, R. An efficient heuristic for real-time ambulance redeployment. Oper. Res. Health Care 2015, 4, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Alanis, R.; Ingolfsson, A.; Kolfal, B. A Markov Chain Model for an EMS System with Repositioning. Prod. Oper. Manag. 2013, 22, 216–231. [Google Scholar] [CrossRef]
- Sudtachat, K.; Mayorga, M.E.; Mclay, L.A. A nested-compliance table policy for emergency medical service systems under relocation. Omega 2016, 58, 154–168. [Google Scholar] [CrossRef]
- van Barneveld, T.; van der Mei, R.; Bhulai, S. Compliance tables for an EMS system with two types of medical response units. Comput. Oper. Res. 2017, 80, 68–81. [Google Scholar] [CrossRef] [Green Version]
- Lim, C.S.; Mamat, R.; Braunl, T. Impact of Ambulance Dispatch Policies on Performance of Emergency Medical Services. IEEE Trans. Intell. Transp. Syst. 2011, 12, 624–632. [Google Scholar] [CrossRef]
- Sudtachat, K.; Mayorga, M.E.; McLay, L.A. Recommendations for dispatching emergency vehicles under multitiered response via simulation. Int. Trans. Oper. Res. 2014, 21, 581–617. [Google Scholar] [CrossRef]
- Nair, R.; Miller-Hooks, E. Evaluation of Relocation Strategies for Emergency Medical Service Vehicles. Transp. Res. Rec. J. Transp. Res. Board 2009, 2137, 63–73. [Google Scholar] [CrossRef]
- Bélanger, V.; Kergosien, Y.; Ruiz, A.; Soriano, P. An empirical comparison of relocation strategies in real-time ambulance fleet management. Comput. Ind. Eng. 2016, 94, 216–229. [Google Scholar] [CrossRef]
- Van Barneveld, T.C.; Bhulai, S.; Van Der Mei, R.D. A dynamic ambulance management model for rural areas: Computing redeployment actions for relevant performance measures. Health Care Manag. Sci. 2015, 20, 165–186. [Google Scholar] [CrossRef]
- Maxwell, M.S.; Ni, E.C.; Tong, C.; Henderson, S.G.; Topaloglu, H.; Hunter, S.R. A Bound on the Performance of an Optimal Ambulance Redeployment Policy. Oper. Res. 2014, 62, 1014–1027. [Google Scholar] [CrossRef] [Green Version]
- Van Barneveld, T. The Minimum Expected Penalty Relocation Problem for the Computation of Compliance Tables for Ambulance Vehicles. INFORMS J. Comput. 2016, 28, 370–384. [Google Scholar] [CrossRef] [Green Version]
- Jagtenberg, C.J.; Bhulai, S.; Van Der Mei, R.D. Dynamic ambulance dispatching: Is the closest-idle policy always optimal? Health Care Manag. Sci. 2016, 20, 517–531. [Google Scholar] [CrossRef] [Green Version]
- van Barneveld, T.; Bhulai, S.; van der Mei, R. The effect of ambulance relocations on the performance of ambulance service providers. Eur. J. Oper. Res. 2016, 252, 257–269. [Google Scholar] [CrossRef]
- Degel, D.; Wiesche, L.; Rachuba, S.; Werners, B. Time-dependent ambulance allocation considering data-driven empirically required coverage. Health Care Manag. Sci. 2014, 18, 444–458. [Google Scholar] [CrossRef]
- Andrade, L.A.C.G.; Cunha, C.B. An ABC heuristic for optimizing moveable ambulance station location and vehicle repositioning for the city of São Paulo. Int. Trans. Oper. Res. 2015, 22, 473–501. [Google Scholar] [CrossRef]
- Lam, S.S.W.; Zhang, J.; Zhang, Z.C.; Oh, H.C.; Overton, J.; Ng, Y.Y.; Ong, M.E.H. Dynamic ambulance reallocation for the reduction of ambulance response times using system status management. Am. J. Emerg. Med. 2015, 33, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Berg, P.L.V.D.; Aardal, K. Time-dependent MEXCLP with start-up and relocation cost. Eur. J. Oper. Res. 2015, 242, 383–389. [Google Scholar] [CrossRef]
- McCormack, R.; Coates, G. A simulation model to enable the optimization of ambulance fleet allocation and base station location for increased patient survival. Eur. J. Oper. Res. 2015, 247, 294–309. [Google Scholar] [CrossRef] [Green Version]
- Enayati, S.; Mayorga, M.E.; Rajagopalan, H.; Saydam, C. Real-time ambulance redeployment approach to improve service coverage with fair and restricted workload for EMS providers. Omega 2018, 79, 67–80. [Google Scholar] [CrossRef]
- Yoon, S.; Albert, L.A. Dynamic dispatch policies for emergency response with multiple types of vehicles. Transp. Res. Part E Logist. Transp. Rev. 2021, 152, 102405. [Google Scholar] [CrossRef]
- Andersson, H.; Granberg, T.A.; Christiansen, M.; Aartun, E.S.; Leknes, H. Using optimization to provide decision support for strategic emergency medical service planning—Three case studies. Int. J. Med. Inform. 2020, 133, 103975. [Google Scholar] [CrossRef] [PubMed]
- Boujemaa, R.; Jebali, A.; Hammami, S.; Ruiz, A. Multi-period stochastic programming models for two-tiered emergency medical service system. Comput. Oper. Res. 2020, 123, 104974. [Google Scholar] [CrossRef]
- Tsai, Y.; Chang, K.-W.; Yiang, G.-T.; Lin, H.-J. Demand Forecast and Multi-Objective Ambulance Allocation. Int. J. Pattern Recognit. Artif. Intell. 2018, 32, 1859011. [Google Scholar] [CrossRef]
- Peng, C.; Delage, E.; Li, J. Probabilistic Envelope Constrained Multiperiod Stochastic Emergency Medical Services Location Model and Decomposition Scheme. Transp. Sci. 2020, 54, 1471–1494. [Google Scholar] [CrossRef]
- Carvalho, A.; Captivo, M.E.; Marques, I. Integrating the ambulance dispatching and relocation problems to maximize system’s preparedness. Eur. J. Oper. Res. 2020, 283, 1064–1080. [Google Scholar] [CrossRef]
- Bélanger, V.; Lanzarone, E.; Nicoletta, V.; Ruiz, A.; Soriano, P. A recursive simulation-optimization framework for the ambulance location and dispatching problem. Eur. J. Oper. Res. 2020, 286, 713–725. [Google Scholar] [CrossRef]
- Enayati, S.; Mayorga, M.E.; Toro-Díaz, H.; Albert, L.A. Identifying trade-offs in equity and efficiency for simultaneously optimizing location and multipriority dispatch of ambulances. Int. Trans. Oper. Res. 2018, 26, 415–438. [Google Scholar] [CrossRef]
- Lee, S. The role of preparedness in ambulance dispatching. J. Oper. Res. Soc. 2011, 62, 1888–1897. [Google Scholar] [CrossRef]
- van Barneveld, T.; Jagtenberg, C.; Bhulai, S.; van der Mei, R. Real-time ambulance relocation: Assessing real-time redeployment strategies for ambulance relocation. Socio-Econ. Plan. Sci. 2018, 62, 129–142. [Google Scholar] [CrossRef] [Green Version]
- Peyravi, M.; Khodakarim, S.; Örtenwall, P.; Khorram-Manesh, A. Does temporary location of ambulances (“fluid deployment”) affect response times and patient outcome? Int. J. Emerg. Med. 2015, 8, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolejš, M.; Purchard, J.; Javorčák, A. Generating a spatial coverage plan for the emergency medical service on a regional scale: Empirical versus random forest modelling approach. J. Transp. Geogr. 2020, 89, 102889. [Google Scholar] [CrossRef]
- Ji, S.; Zheng, Y.; Wang, W.; Li, T. Real-Time Ambulance Redeployment: A Data-Driven Approach. IEEE Trans. Knowl. Data Eng. 2019, 32, 2213–2226. [Google Scholar] [CrossRef]
- Boutilier, J.J.; Chan, T.C.Y. Ambulance Emergency Response Optimization in Developing Countries. Oper. Res. 2020, 68, 1315–1334. [Google Scholar] [CrossRef]
- Roa, J.C.P.; Escobar, J.W.; Moreno, C.A.M. An online real-time matheuristic algorithm for dispatch and relocation of ambulances. Int. J. Ind. Eng. Comput. 2020, 11, 443–468. [Google Scholar] [CrossRef]
- Sun, C.-H.; Cheng, C.-Y.; Wang, C.-H.; Hsiao, P.-H. Dynamic Floating Stations Model for Emergency Medical Services with a Consideration of Traffic Data. ISPRS Int. J. Geo-Inf. 2020, 9, 336. [Google Scholar] [CrossRef]
- Yuangyai, C.; Nilsang, S.; Cheng, C.-Y. Robust ambulance base allocation strategy with social media and traffic congestion information. J. Ambient. Intell. Humaniz. Comput. 2020, 1–14. [Google Scholar] [CrossRef]
- Mohri, S.S.; Akbarzadeh, M.; Matin, S.H.S. A Hybrid model for locating new emergency facilities to improve the coverage of the road crashes. Socio-Econ. Plan. Sci. 2019, 69, 100683. [Google Scholar] [CrossRef]
- Abensur, E.O.; Paes, A.D.S.; Yamada, E.R.K.; Ruggieri, V.; de Aquino, W.A. Stochastic facility location problem in a competitive situation: A game theory model for emergency financial services. Cogent Eng. 2020, 7, 1837411. [Google Scholar] [CrossRef]
- Azim, M.A.; Jianwu, D.; Yangping, W.; Aziz, T.; Fengwen, Z. RTA Analysis & Existing Modelling for Emergency Medical Service. Teh. Vjesn.-Tech. Gaz. 2020, 27, 251–261. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, Y.H. Two-Tiered Ambulance Dispatch and Redeployment considering Patient Severity Classification Errors. J. Health Eng. 2019, 2019, 6031789. [Google Scholar] [CrossRef] [PubMed]
- Bertsimas, D.; Ng, Y. Robust and stochastic formulations for ambulance deployment and dispatch. Eur. J. Oper. Res. 2019, 279, 557–571. [Google Scholar] [CrossRef]
- Nilsang, S.; Yuangyai, C.; Cheng, C.-Y.; Janjarassuk, U. Locating an ambulance base by using social media: A case study in Bangkok. Ann. Oper. Res. 2019, 283, 497–516. [Google Scholar] [CrossRef]
- Jánošíková, Ľ; Kvet, M.; Jankovič, P.; Gábrišová, L. An optimization and simulation approach to emergency stations relocation. Cent. Eur. J. Oper. Res. 2019, 27, 737–758. [Google Scholar] [CrossRef]
- Grekousis, G.; Liu, Y. Where will the next emergency event occur? Predicting ambulance demand in emergency medical services using artificial intelligence. Comput. Environ. Urban Syst. 2019, 76, 110–122. [Google Scholar] [CrossRef]
- El Itani, B.; Ben Abdelaziz, F.; Masri, H. A Bi-objective Covering Location Problem: Case of ambulance location in the Beirut area, Lebanon. Manag. Decis. 2019, 57, 432–444. [Google Scholar] [CrossRef]
- Firooze, S.; Rafiee, M.; Zenouzzadeh, S.M. An Optimization Model for Emergency Vehicle Location and Relocation with Consideration of Unavailability Time. Sci. Iran. 2017, 25, 3685–3699. [Google Scholar] [CrossRef] [Green Version]
- van Buuren, M.; van der Mei, R.; Bhulai, S. Demand-point constrained EMS vehicle allocation problems for regions with both urban and rural areas. Oper. Res. Health Care 2018, 18, 65–83. [Google Scholar] [CrossRef] [Green Version]
- Enayati, S.; Özaltın, O.Y.; Mayorga, M.E.; Saydam, C. Ambulance redeployment and dispatching under uncertainty with personnel workload limitations. IISE Trans. 2018, 50, 777–788. [Google Scholar] [CrossRef]
- Coelho, O.; Alexandrino, F.; Barreto, B. SAMU ambulance positioning using MALP model. Braz. J. Oper. Prod. Manag. 2017, 14, 508. [Google Scholar] [CrossRef] [Green Version]
- Lam, S.S.W.; Ng, C.B.L.; Nguyen, F.N.H.L.; Ng, Y.Y.; Ong, M.E.H. Simulation-based decision support framework for dynamic ambulance redeployment in Singapore. Int. J. Med. Inform. 2017, 106, 37–47. [Google Scholar] [CrossRef]
- Calderín, J.F.; Masegosa, A.D.; Pelta, D.A. An algorithm portfolio for the dynamic maximal covering location problem. Memetic Comput. 2016, 9, 141–151. [Google Scholar] [CrossRef]
- Ansari, S.; McLay, L.A.; Mayorga, M.E. A Maximum Expected Covering Problem for District Design. Transp. Sci. 2017, 51, 376–390. [Google Scholar] [CrossRef]
- Drezner, Z.; Marianov, V.; Wesolowsky, G.O. Maximizing the minimum cover probability by emergency facilities. Ann. Oper. Res. 2014, 246, 349–362. [Google Scholar] [CrossRef]
- Moeini, M.; Jemai, Z.; Sahin, E. Location and relocation problems in the context of the emergency medical service systems: A case study. Cent. Eur. J. Oper. Res. 2014, 23, 641–658. [Google Scholar] [CrossRef]
- Andersson, T.; Värbrand, P. Decision support tools for ambulance dispatch and relocation. J. Oper. Res. Soc. 2007, 58, 195–201. [Google Scholar] [CrossRef] [Green Version]
- Mayorga, M.E.; Bandara, D.; McLay, L.A. Districting and dispatching policies for emergency medical service systems to improve patient survival. IIE Trans. Healthc. Syst. Eng. 2013, 3, 39–56. [Google Scholar] [CrossRef]
- Zhen, L.; Sheng, S.; Xie, Z.; Wang, K. Decision rules for ambulance scheduling decision support systems. Appl. Soft Comput. 2014, 26, 350–356. [Google Scholar] [CrossRef]
- Mason, A.J. Simulation and real-time optimised relocation for improving ambulance operations. In Handbook of Healthcare Operations Management; Springer LLC: New York, NY, USA, 2013; Volume 184, pp. 289–317. [Google Scholar]
- Liu, Y.; Yuan, Y.; Li, Y.-H.; Pang, H. A Chance Constrained Programming Model for Reliable Emergency Vehicles Relocation Problem. Procedia-Soc. Behav. Sci. 2013, 96, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Chanta, S.; Mayorga, M.E.; McLay, L.A. The minimum p-envy location problem with requirement on minimum survival rate. Comput. Ind. Eng. 2014, 74, 228–239. [Google Scholar] [CrossRef]
- Janosikova, L.; Jankovic, P.; Marton, P. Models for Relocation of Emergency Medical Stations. In The Rise of Big Spatial Data; Springer: Cham, Switzerland, 2017; pp. 225–239. [Google Scholar] [CrossRef]
- Ball, M.O.; Lin, F.L. A Reliability Model Applied to Emergency Service Vehicle Location. Oper. Res. 1993, 41, 18–36. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, M.S.; Henderson, S.G.; Topaloglu, H. Tuning Approximate Dynamic Programming Policies for Ambulance Redeployment via Direct Search. Stoch. Syst. 2013, 3, 322–361. [Google Scholar] [CrossRef]
- Knight, V.; Harper, P.; Smith, L. Ambulance allocation for maximal survival with heterogeneous outcome measures. Omega 2012, 40, 918–926. [Google Scholar] [CrossRef]
- Shariat-Mohaymany, A.; Babaei, M.; Moadi, S.; Amiripour, S.M. Linear upper-bound unavailability set covering models for locating ambulances: Application to Tehran rural roads. Eur. J. Oper. Res. 2012, 221, 263–272. [Google Scholar] [CrossRef]
- Maleki, M.; Majlesinasab, N.; Sepehri, M.M. Two new models for redeployment of ambulances. Comput. Ind. Eng. 2014, 78, 271–284. [Google Scholar] [CrossRef]
- Naoum-Sawaya, J.; Elhedhli, S. A stochastic optimization model for real-time ambulance redeployment. Comput. Oper. Res. 2013, 40, 1972–1978. [Google Scholar] [CrossRef]
- Toro-Díaz, H.; Mayorga, M.E.; Chanta, S.; McLay, L.A. Joint location and dispatching decisions for Emergency Medical Services. Comput. Ind. Eng. 2013, 64, 917–928. [Google Scholar] [CrossRef]
- Billhardt, H.; Lujak, M.; Sánchez-Brunete, V.; Fernández, A.; Ossowski, S. Dynamic coordination of ambulances for emergency medical assistance services. Knowl.-Based Syst. 2014, 70, 268–280. [Google Scholar] [CrossRef]
- Bertsekas, D.P. The auction algorithm: A distributed relaxation method for the assignment problem. Ann. Oper. Res. 1988, 14, 105–123. [Google Scholar] [CrossRef] [Green Version]
- Nickel, S.; Reuter-Oppermann, M.; Saldanha-Da-Gama, F. Ambulance location under stochastic demand: A sampling approach. Oper. Res. Health Care 2016, 8, 24–32. [Google Scholar] [CrossRef]
- Jarvis, J.P. Approximating the Equilibrium Behavior of Multi-Server Loss Systems. Manag. Sci. 1985, 31, 235–239. [Google Scholar] [CrossRef]
- Vile, J.; Gillard, J.; Harper, P.; Knight, V. Time-dependent stochastic methods for managing and scheduling Emergency Medical Services. Oper. Res. Health Care 2016, 8, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Jin, R.; Xia, T.; Liu, X.; Murata, T.; Kim, K.-S. Predicting Emergency Medical Service Demand with Bipartite Graph Convolutional Networks. IEEE Access 2021, 9, 9903–9915. [Google Scholar] [CrossRef]
- Yu, G.; Liu, A.; Sun, H. Risk-averse flexible policy on ambulance allocation in humanitarian operations under uncertainty. Int. J. Prod. Res. 2021, 59, 2588–2610. [Google Scholar] [CrossRef]
- Sudtachat, K.; Mayorga, M.E.; Chanta, S.; Albert, L.A. Joint relocation and districting using a nested compliance model for EMS systems. Comput. Ind. Eng. 2020, 142, 106327. [Google Scholar] [CrossRef]
- Yang, W.; Su, Q.; Zhou, M.; Qin, X. Ambulance allocation considering the spatial randomness of demand. Comput. Ind. Eng. 2020, 139, 106202. [Google Scholar] [CrossRef]
- Olave-Rojas, D.; Nickel, S. Modeling a pre-hospital emergency medical service using hybrid simulation and a machine learning approach. Simul. Model. Pract. Theory 2021, 109, 102302. [Google Scholar] [CrossRef]
- Sugishita, Y.; Sugawara, T.; Ohkusa, Y.; Ishikawa, T.; Yoshida, M.; Endo, H. Syndromic surveillance using ambulance transfer data in Tokyo, Japan. J. Infect. Chemother. 2020, 26, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Todkill, D.; Loveridge, P.; Elliot, A.J.; Morbey, R.A.; Edeghere, O.; Rayment-Bishop, T.; Rayment-Bishop, C.; Thornes, J.E.; Smith, G. Utility of Ambulance Data for Real-Time Syndromic Surveillance: A Pilot in the West Midlands Region, United Kingdom. Prehosp. Disaster Med. 2017, 32, 667–672. [Google Scholar] [CrossRef]
- Yue, Y.; Marla, L.; Krishnan, R.; Heinz, H.J. An Efficient Simulation-Based Approach to Ambulance Fleet Allocation and Dynamic Redeployment. In Proceedings of the AAAI Conference on Artificial Intelligence, Toronto, ON, Canada, 22–26 July 2012; Volume 26. [Google Scholar]
- Majzoubi, F.; Bai, L.; Heragu, S.S. An optimization approach for dispatching and relocating EMS vehicles. IIE Trans. Healthc. Syst. Eng. 2012, 2, 211–223. [Google Scholar] [CrossRef]
- Akıncılar, A.; Akıncılar, E.; Knoflacher, H.; Ocalir-Akunal, E.V. A specific issue on sustainability of transportation planning in an urban region: Ambulance location problem. In Engineering Tools and Solutions for Sustainable Transportation Planning; IGI Global: Hershey, PA, USA, 2017; pp. 303–316. [Google Scholar] [CrossRef] [Green Version]
- Schneeberger, K.; Doerner, K.; Kurz, A.; Schilde, M. Ambulance location and relocation models in a crisis. Cent. Eur. J. Oper. Res. 2014, 24, 1–27. [Google Scholar] [CrossRef]
- Berg, P.L.V.D.; Fiskerstrand, P.; Aardal, K.; Einerkjær, J.; Thoresen, T.; Røislien, J. Improving ambulance coverage in a mixed urban-rural region in Norway using mathematical modeling. PLoS ONE 2019, 14, e0215385. [Google Scholar] [CrossRef] [Green Version]
- Tozan, H.; Donmez, S. A Genetic Algorithm Based Approach to Provide Solutions for Emergency Aid Stations Location Problem and a Case Study for Pendik/İstanbul. J. Homel. Secur. Emerg. Manag. 2015, 12, 915–940. [Google Scholar] [CrossRef]
- Aringhieri, R.; Bruni, M.; Khodaparasti, S.; van Essen, T. Emergency medical services and beyond: Addressing new challenges through a wide literature review. Comput. Oper. Res. 2017, 78, 349–368. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Z.; Zhu, X.; Wyatt, T. Covering models and optimization techniques for emergency response facility location and planning: A review. Math. Methods Oper. Res. (ZOR) 2011, 74, 281–310. [Google Scholar] [CrossRef]
- Jagtenberg, C.; Berg, P.V.D.; van der Mei, R. Benchmarking online dispatch algorithms for Emergency Medical Services. Eur. J. Oper. Res. 2017, 258, 715–725. [Google Scholar] [CrossRef] [Green Version]
- Lateef, F.; Lim, S.H.; Tan, E.H. New Paradigm for Protection: The Emergency Ambulance Services in the Time of Severe Acute Respiratory Syndrome. Prehosp. Emerg. Care 2004, 8, 304–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neira-Rodado, D.; Escobar-Velasquez, J.W.; McClean, S. Ambulances Deployment Problems: Categorization, Evolution and Dynamic Problems Review. ISPRS Int. J. Geo-Inf. 2022, 11, 109. https://doi.org/10.3390/ijgi11020109
Neira-Rodado D, Escobar-Velasquez JW, McClean S. Ambulances Deployment Problems: Categorization, Evolution and Dynamic Problems Review. ISPRS International Journal of Geo-Information. 2022; 11(2):109. https://doi.org/10.3390/ijgi11020109
Chicago/Turabian StyleNeira-Rodado, Dionicio, John Wilmer Escobar-Velasquez, and Sally McClean. 2022. "Ambulances Deployment Problems: Categorization, Evolution and Dynamic Problems Review" ISPRS International Journal of Geo-Information 11, no. 2: 109. https://doi.org/10.3390/ijgi11020109