
Spatiotemporal Data-Driven Multiperiod Relocation Optimization of Emergency Medical Services: Maximum Equality Objective

Abstract
:1. Background
- (1)
- Simulated urban data. In EMS location and relocation studies, simplifying assumptions are used in the modeling phase to assess the models analytically [7]. Limited by the availability of data and the effectiveness of data processing methods, city managers mainly employ population data based on statistical surveys or Euclidean distance traffic data based on GIS software simulations when compiling EMS planning and dispatch strategies. To some extent, the generalized data representation of urban space loses the actual activity features of urban residents. It is crucial to conduct a quantitative evaluation of the realistic urban environment based on big geospatial data.
- (2)
- Static urban environment. Traditional research on the spatial accessibility of EMSs lacks consideration of spatiotemporal dynamics and spatiotemporal heterogeneity, which may lead to a problem regarding uncertain geographic context [8]. In the early stages, EMS location studies assumed that the urban population distribution was static and the urban traffic commuting state was consistent. Scholars first researched a series of stationary models for EMV locations, met the requirements for maximum coverage under limited EMV resources, and decreased the allocation and operating costs [9]. Dynamically estimating potential emergency demands based on big spatiotemporal data is a critical prerequisite for rationally dispatching EMVs at each station and shortening the response time.
- (3)
- Equilibrium between equality and efficiency is challenging. The objective of EMSs is to obtain emergency resources in the shortest time [6]. If the response time of EMSs can be shortened, the survival rate of patients will be improved. Inequitable solutions can be generated by classic shortest-time models due to imbalances in economic level between cities and densely populated and low-populated areas [10]. Efficiency disparities exist, especially in medical facilities in developing countries [11]. One important concept for people is equity and fairness, the “equalization of basic public services”, which is mutually affected by and is related to the degree of satisfaction regarding how people’s needs are met based on available resources [12].
- (1)
- Realistic urban spatiotemporal data. We adopted a novel approach for utilizing route planner data from web maps and city-wide fine-grained urban population distributions over multiple periods to address the issues of EMS accessibility evaluation and relocation. The EMS model was implemented in the megacity of Nanjing as a case study, and spatiotemporal patterns were discussed.
- (2)
- Dynamic time-dependent urban environment. EMS demand varies over space and time. Demand patterns change, and contingencies occur occasionally, which is why healthcare emergency operations can be delayed [16]. The MRO-EMS method can combine the demand status of the urban population with the traffic environment over various periods, redeploy and relocate idle EMVs between stations, transfer EMVs from potentially low-demand stations to high-demand stations, and realize scheduling changes such that EMVs are not fixed to a specific station in a dynamic environment, ensuring that the call demand near high-demand stations can be promptly responded to.
- (3)
- Toward maximum equality objective. An improved equality model considering dynamic time dependence is proposed based on the model to analyze spatiotemporal data. The dynamic relocation algorithm of EMVs between EMS stations is a viable, practical, and relatively straightforward operation that is anticipated to provide considerable effects given the fundamental fact of the lack of service.
2. Related Work
3. Methods
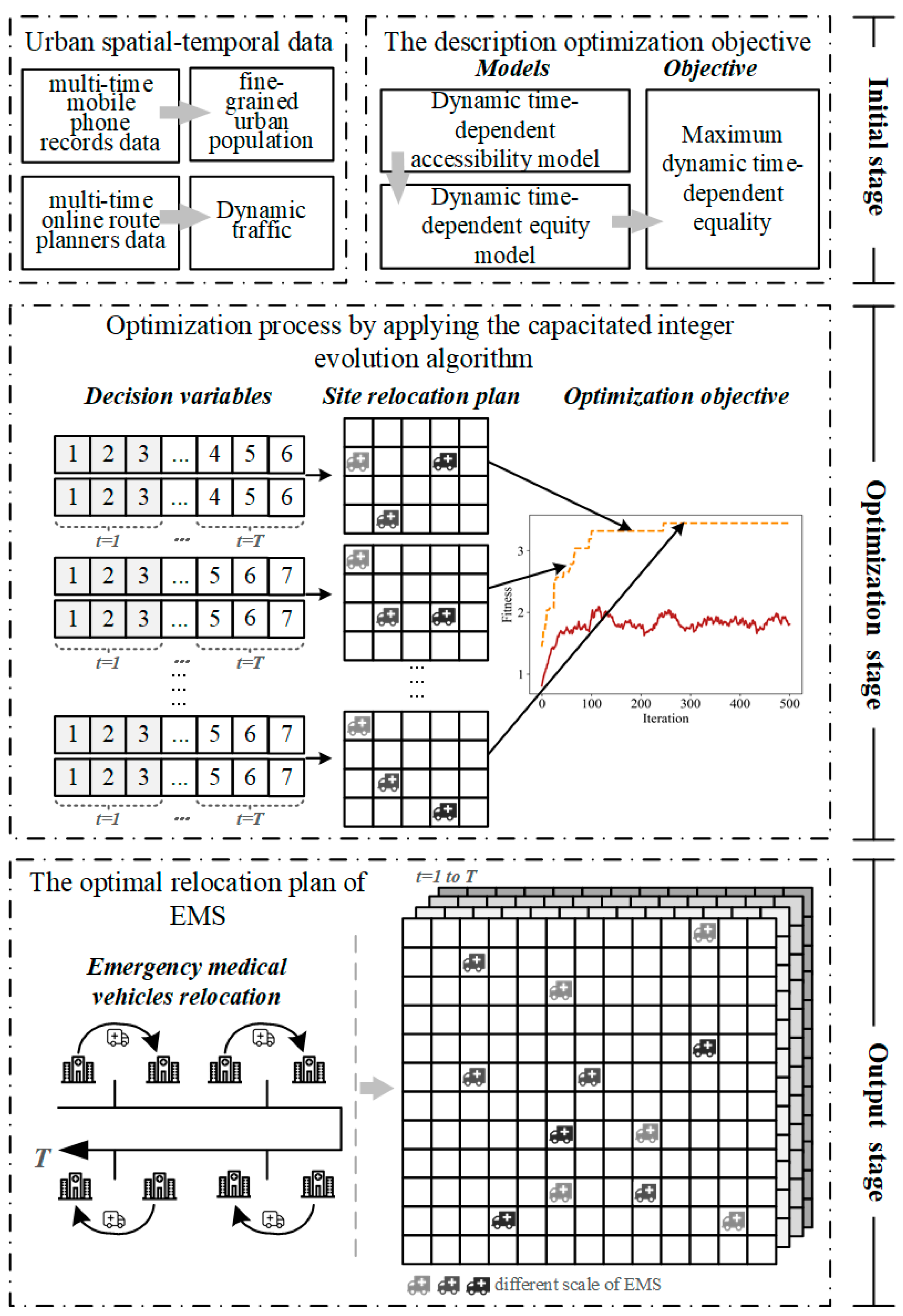
3.1. Outline of the Proposed Approach
3.2. Dynamic Time-Dependent Accessibility Model
- —the index of demand point;
- —the index of supply point;
- —the spatial accessibility of demand point ;
- —the number of pediatricians indicating the service resource supply capacity of provider point ;
- —the supply–demand ratio of service facility ;
- —the demand amount of demand point , such as population number (unit: 10,000 people, consistent with the dimensions in the previous data description);
- —generalized distance decay function;
- —the traffic impedance between demand point and supply point ;
- —the total number of demand points;
- —the total number of supply points;
- —the travel time threshold; that is, the search radius;
- —the coefficient of travel friction, set to 1, with reference to Yao, et al. [39].
- —represents different time slot, ;
- —the spatial accessibility of demand at time slot ;
- —the number of pediatricians indicating the service resource supply capacity of provider at time slot ;
- —the supply–demand ratio of service facility at time slot ;
- —the demand amount of demand at time slot ;
- —the traffic impedance between demand point and supply point at time slot .
3.3. Dynamic Time-Dependent Equality Model
- —the global average value of accessibility;
- —the inequality value of demand that has a positive and negative difference. The higher the positive value is, the higher the level of accessibility beyond the global average and the richer the accessibility.
- —the total service (provider) supply capacity;
- —the total demand amount.
- —a constant that is set to 500 in this research (Through visualization experiments, this value can scale the dimensionless equality value to the visualized value interval);
- —the lower (bottom) limit at provider ;
- —the upper (top) limit at provider ;
- —the total demand amount at time slot ;
- —the total service (provider) resource capacity at time slot ;
- —the original initial moment, representing the status quo before optimization;
- —the accessibility value of demand at initial moment ;
- —the global average value of accessibility at time slot ;
- —the global average value of accessibility at initial moment ;
- —the variation of the inequality value after the after optimization at time slot .
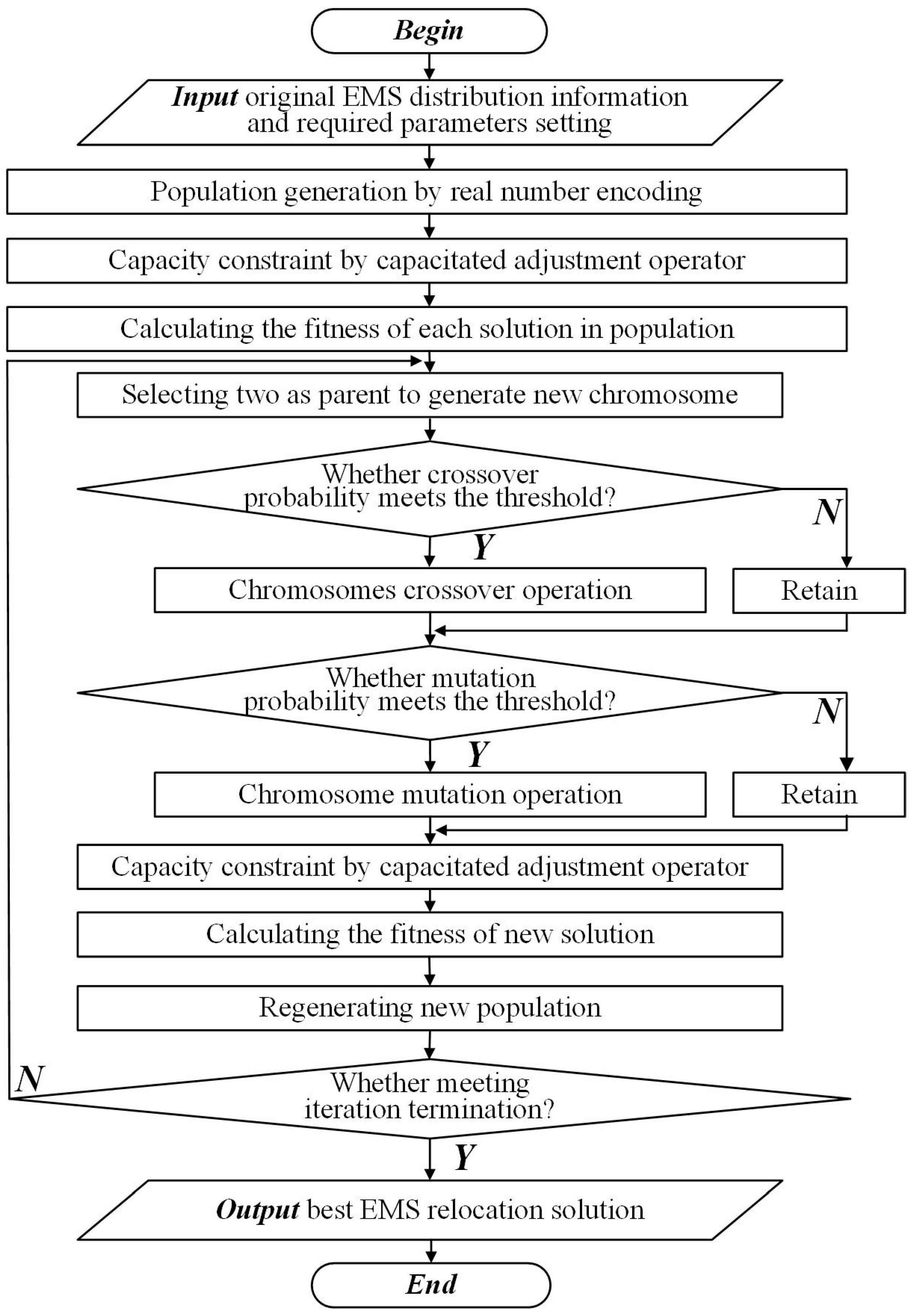
3.4. Capacitated Integer Evolution Algorithm (CIEA)
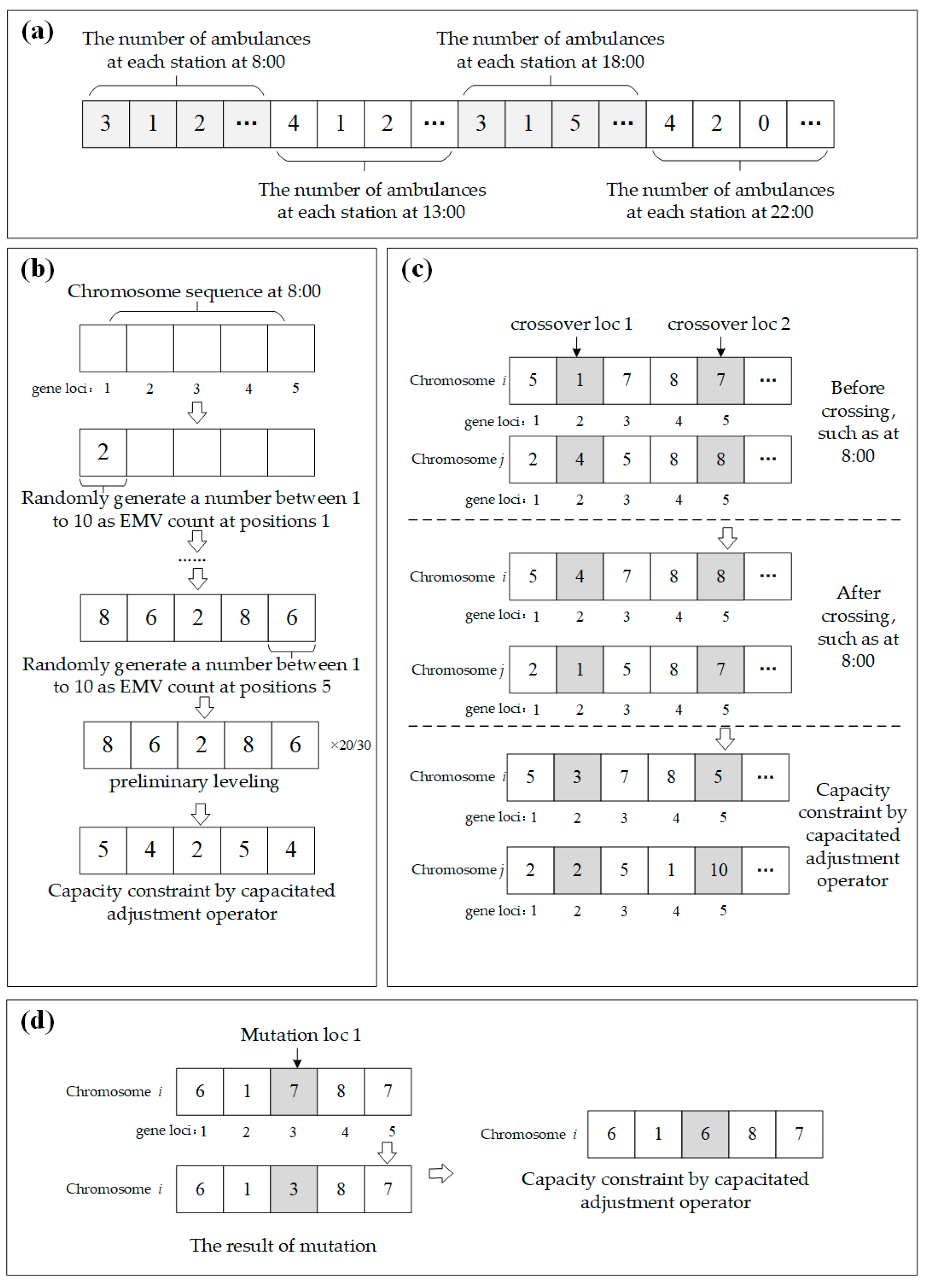
3.4.1. Real Number Encoding Mechanism
3.4.2. Population Generation
- Step 1: Select station j represented by each gene, and obtain the upper (top) and lower (bottom) limit on the number of EMVs that can be relocated at time t;
- Step 2: Determine whether station j is the last station at the current time slot. If so, terminate the CIEA operation and locate the generation of the chromosome at the next time slot; otherwise, the number of EMVs refers to a random number yi between and until the chromosome at time t is generated;
- Step 3: The chromosome generated by the above two steps may exceed the total capacity. Therefore, the value of the chromosome at time t must be preliminarily adjusted. Assuming that the number of EMVs available at time t is y and the number of EMVs is ysum, the number of EMVs after adjustment at each position is yi′ = yi × y/ysum;
- Step 4: Check whether the value of each gene locus is within the and limits;
- Step 5: Use the capacitated integer adjustment operator for further leveling such that the number of individual EMVs satisfies the capacity constraint;
- Step 6: Continue to generate the values of gene loci at the next time slot and go to Step 1.
3.4.3. Crossover Operation
- Step 1: Two chromosomes (i and j) are randomly selected from the population following the roulette method.
- Step 2: At each time slot, the number of positions where the chromosome crossover operation occurs is n. Therefore, the number of crossover gene loci for each chromosome is n × T. A cross gene loci sequence is randomly generated, denoted as {X1, X2 … XnT}, that points to the {X1, X2 …, XnT} locations of i and j, respectively. Assuming that the numbers of EMVs at the intersection of the two chromosomes are {i1, i2 … inT} and {j1, j2 …, jnT}, the numbers of EMVs after crossing are {i1′, i2′ …, inT’} and {j1′, j2′…, jnT’}.
- Step 3: Chromosome i crosses at gene loci nT, and the number of EMVs at that gene locus is inT’ = (i1 + i2 + … + inT) × jnT/(j1 + j2 + … + jnT), jnT’ = (j1 + j2 + … + jnT) × inT/(i1 + i2 + … + inT);
- Step 4: Repeat the crossing operation until the number of crossings reaches w/2.
3.4.4. Mutation Operation
- Step 1: One chromosome of i is randomly selected from the population following the roulette method;
- Step 2: The number of chromosome mutation locations at each time slot is n. Therefore, the number of individual mutation locations is n × T. A sequence of variant positions is randomly generated. Assuming that the number of EMVs at individual mutation locations is {i1, i2…, inT}, and that of the randomly generated mutation sequences is {m1, m2…, mnT}, the numbers of EMVs after mutation are {i1′, i2′…, inT’}, inT’ = (i1 + i2 + … + inT) × mnT/(m1 + m2 + … + mnT);
- Step 3: Repeat steps 1 and 2 until the sum of the gene values at the mutation position is equal to i1 + i2 + … + inT.
3.4.5. Capacitated Adjustment Operator
| Algorithm 1. The structure of the capacitated adjustment operator. |
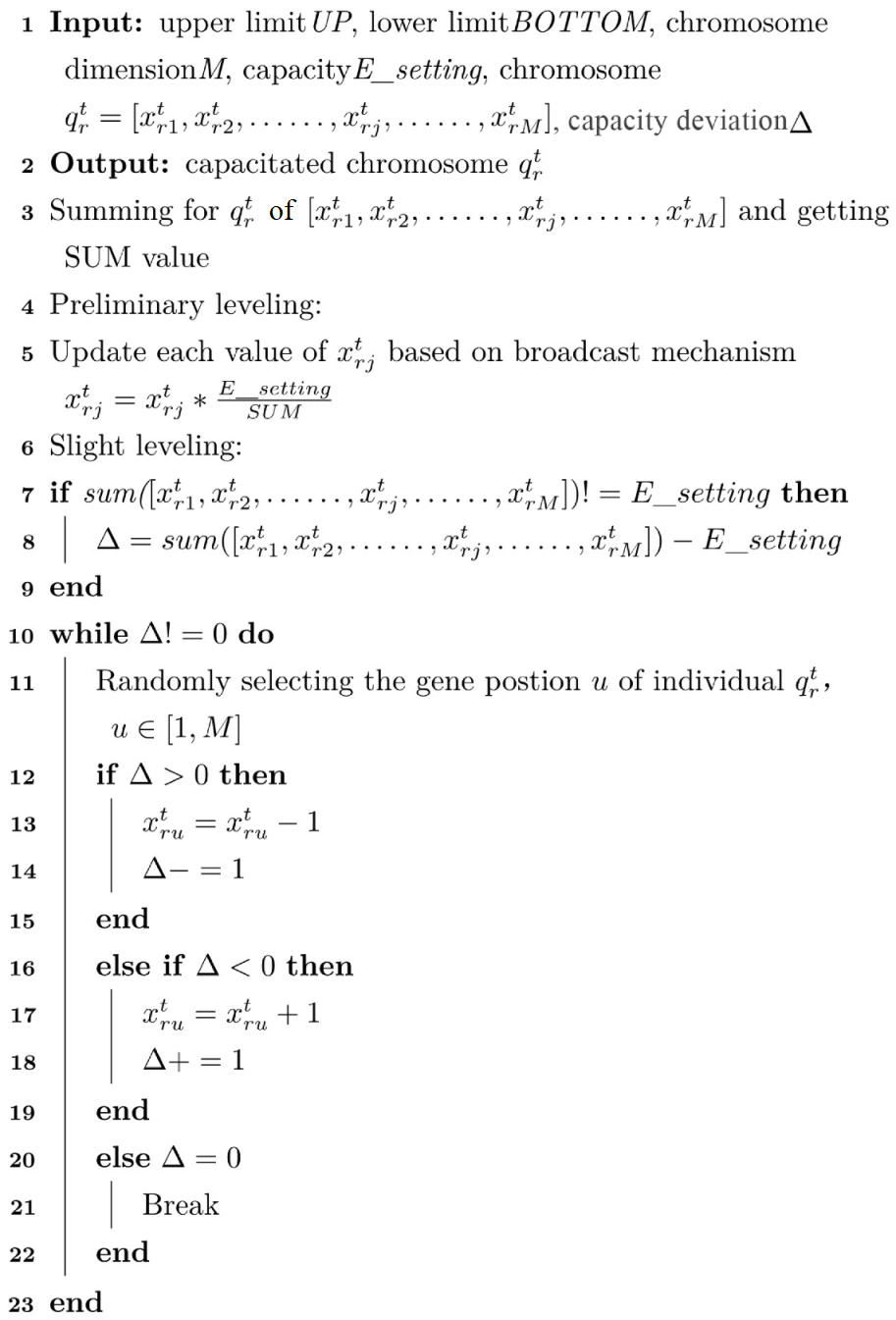 |
4. Study Area and Data
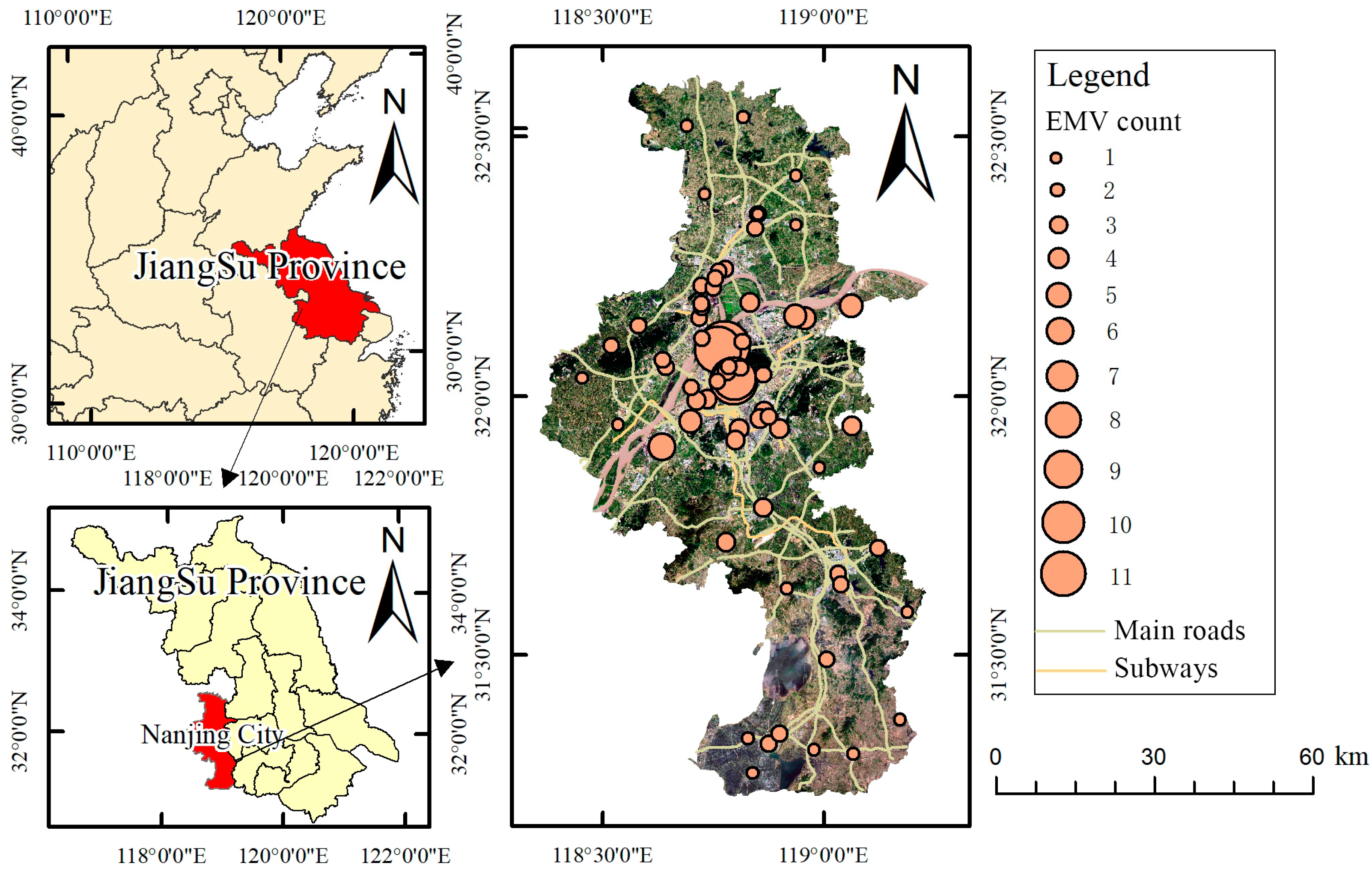
4.1. Study Area
4.2. Data
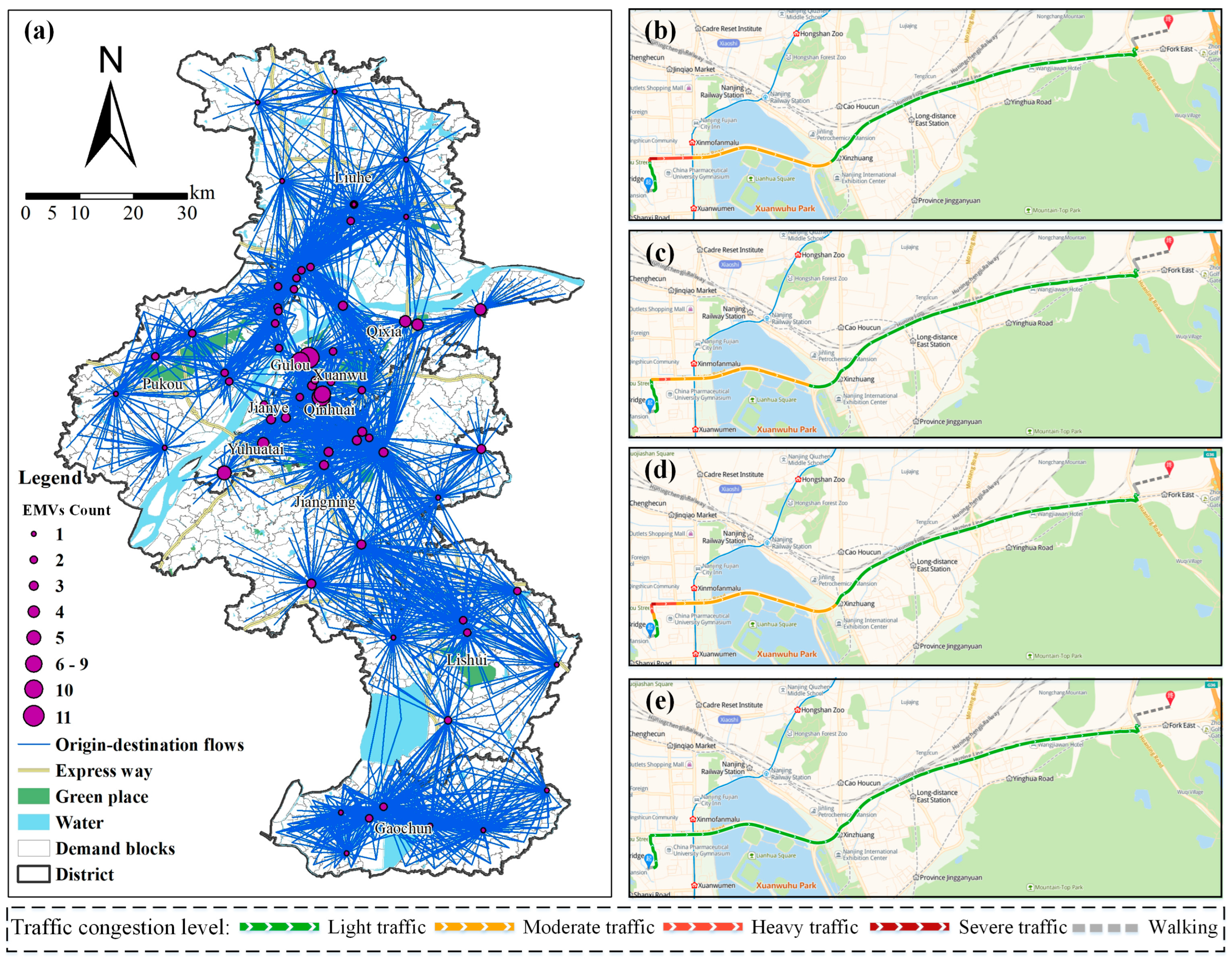
4.2.1. Multiperiod Online Route Planner (M-ORP) Data
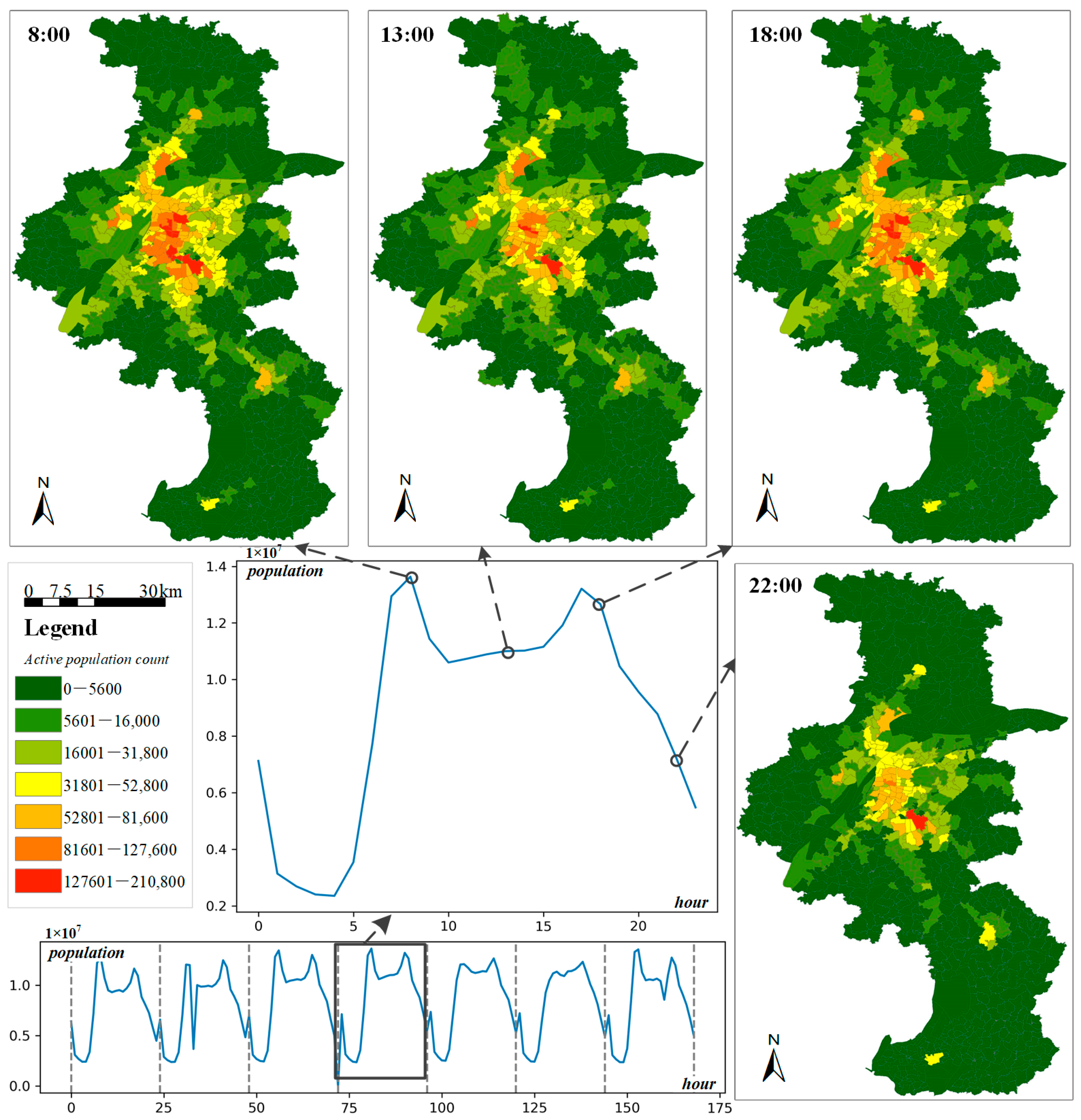
4.2.2. Multiperiod Mobile Phone Records (M-MPR) Data
5. Results
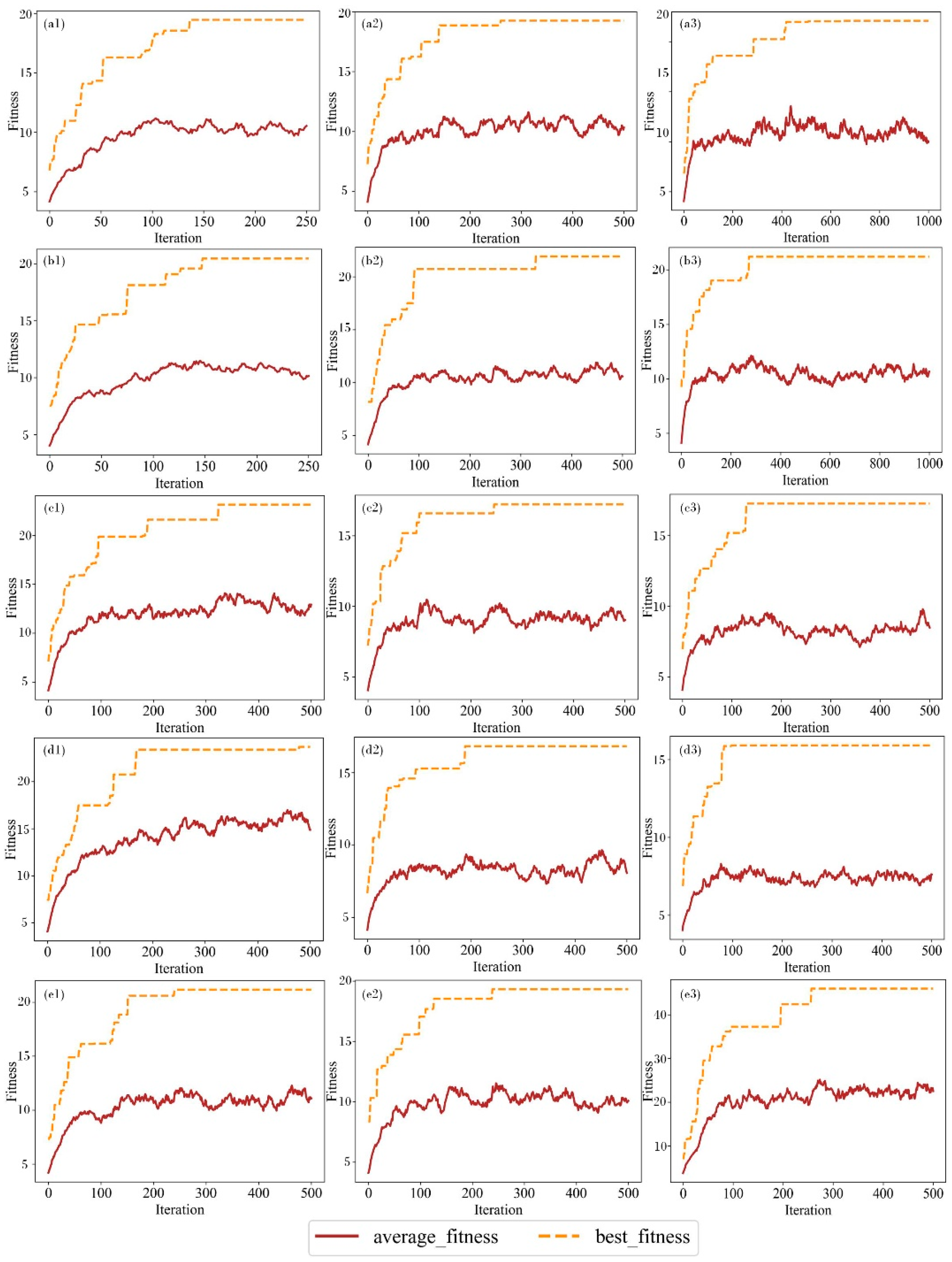
5.1. Relocation Experiment
5.2. Spatial Distribution Results of EMS after Optimization
- (1)
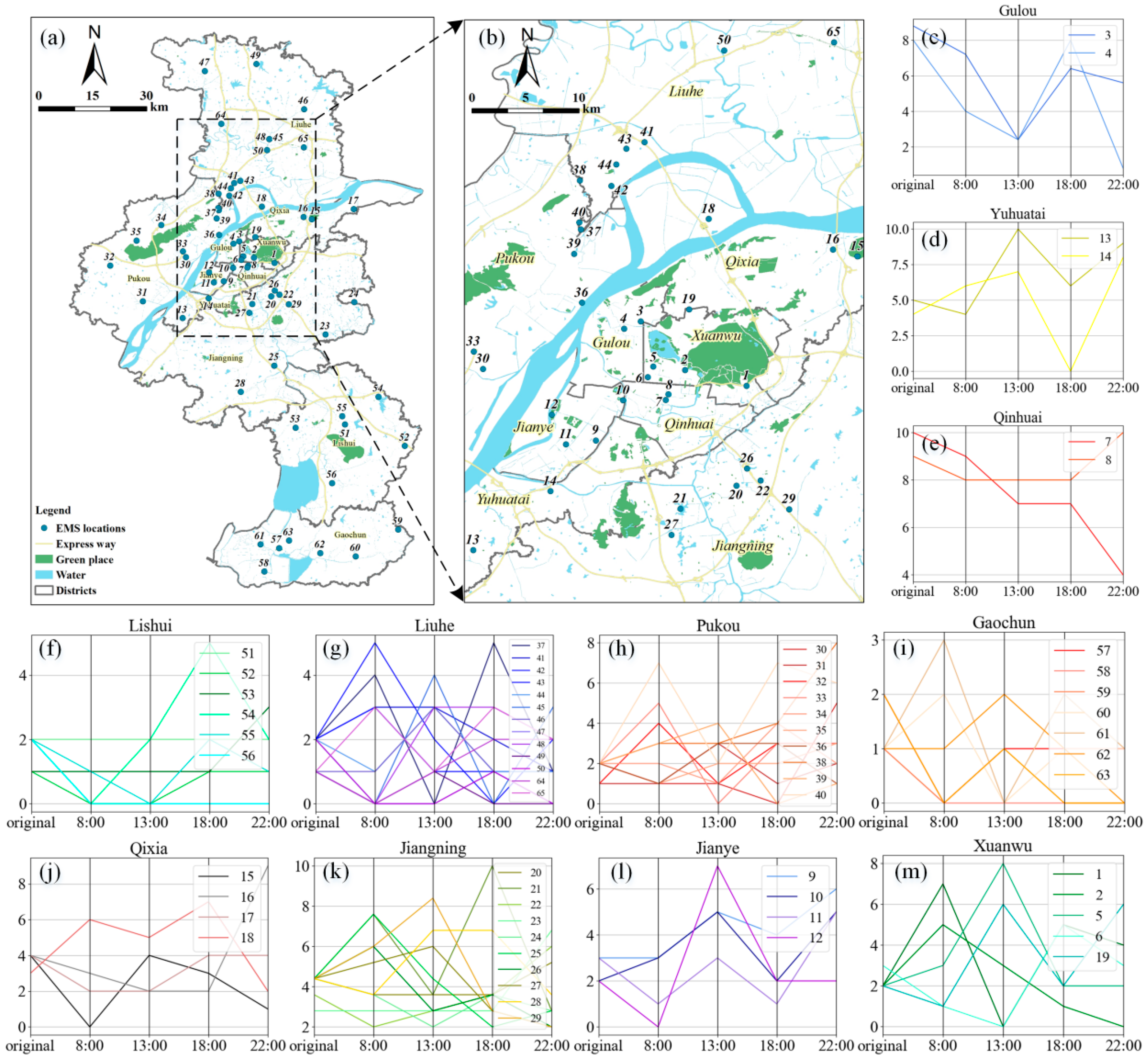
- An increasing pattern means that the number of EMVs at each time slot increases significantly after optimization of the EMS station, indicating that the original resources of the EMS stations were insufficient. Only a few stations, such as Lishui and Qixia, fit this growth pattern perfectly. Moreover, the districts showing a significant increase at night include Pukou, Liuhe, and Jiangning, a trend that was directly related to the districts’ large area, suburban location, and dense population.
- (2)
- A fluctuating pattern refers to the number of EMVs fluctuating during each time slot with the dynamic changes in population and traffic conditions, indicating that the original resources of EMS stations roughly satisfied the demand. Furthermore, the dynamics after time-dependent optimization effects are reflected. Figure 8 shows that most of the sites, including Jianye, Pukou, Liuhe, and Xuanwu, fully conform to the fluctuation pattern.
- (3)
- A descent pattern refers to the fact that the number of EMVs at each moment shows a significant decline after optimization of the EMS station, indicating that the original resource allocation of the EMS station easily satisfies the region’s demand. Some stations in the central urban area, such as Qinhuai and Gulou, perfectly correspond to the descending pattern (Figure 8).
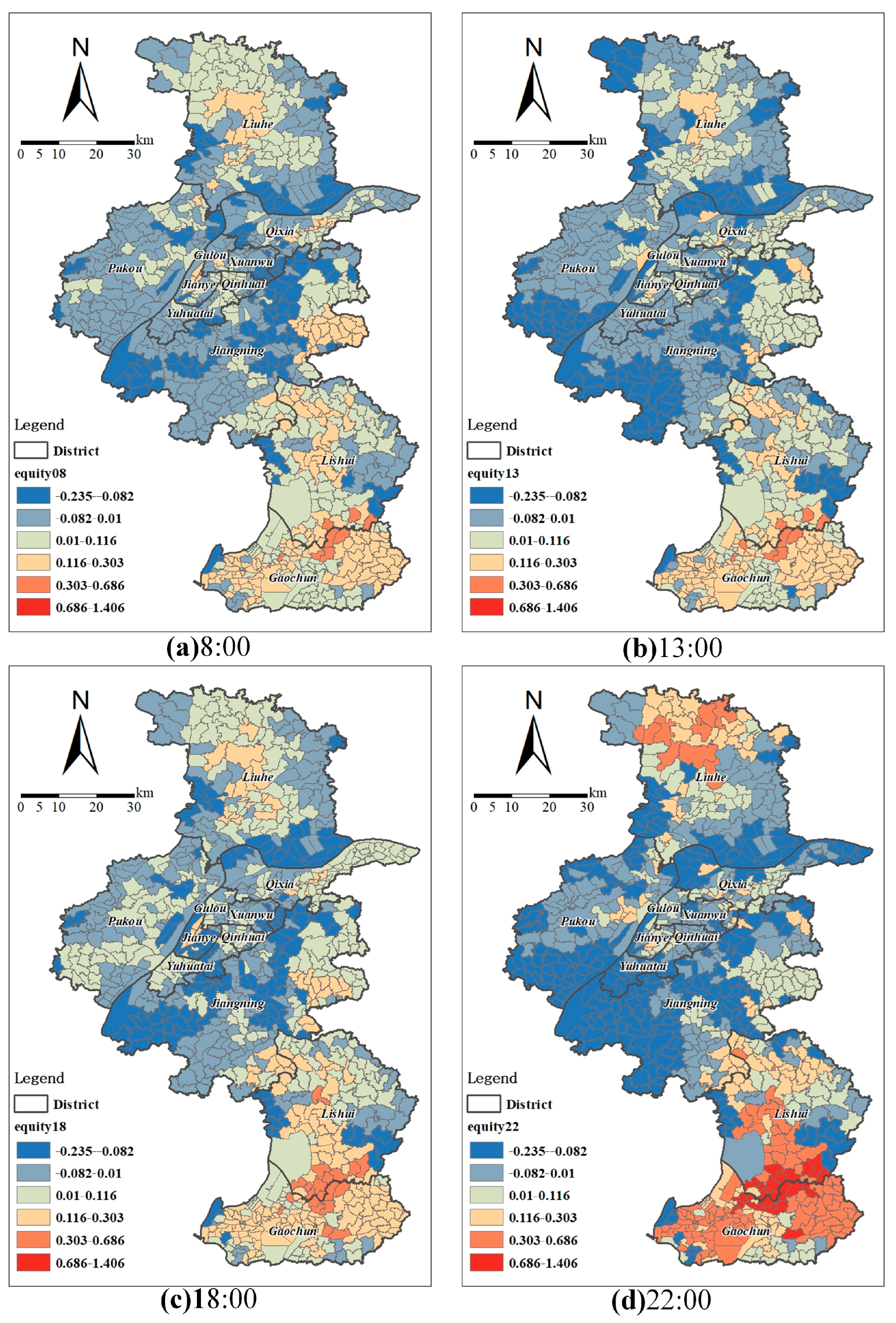
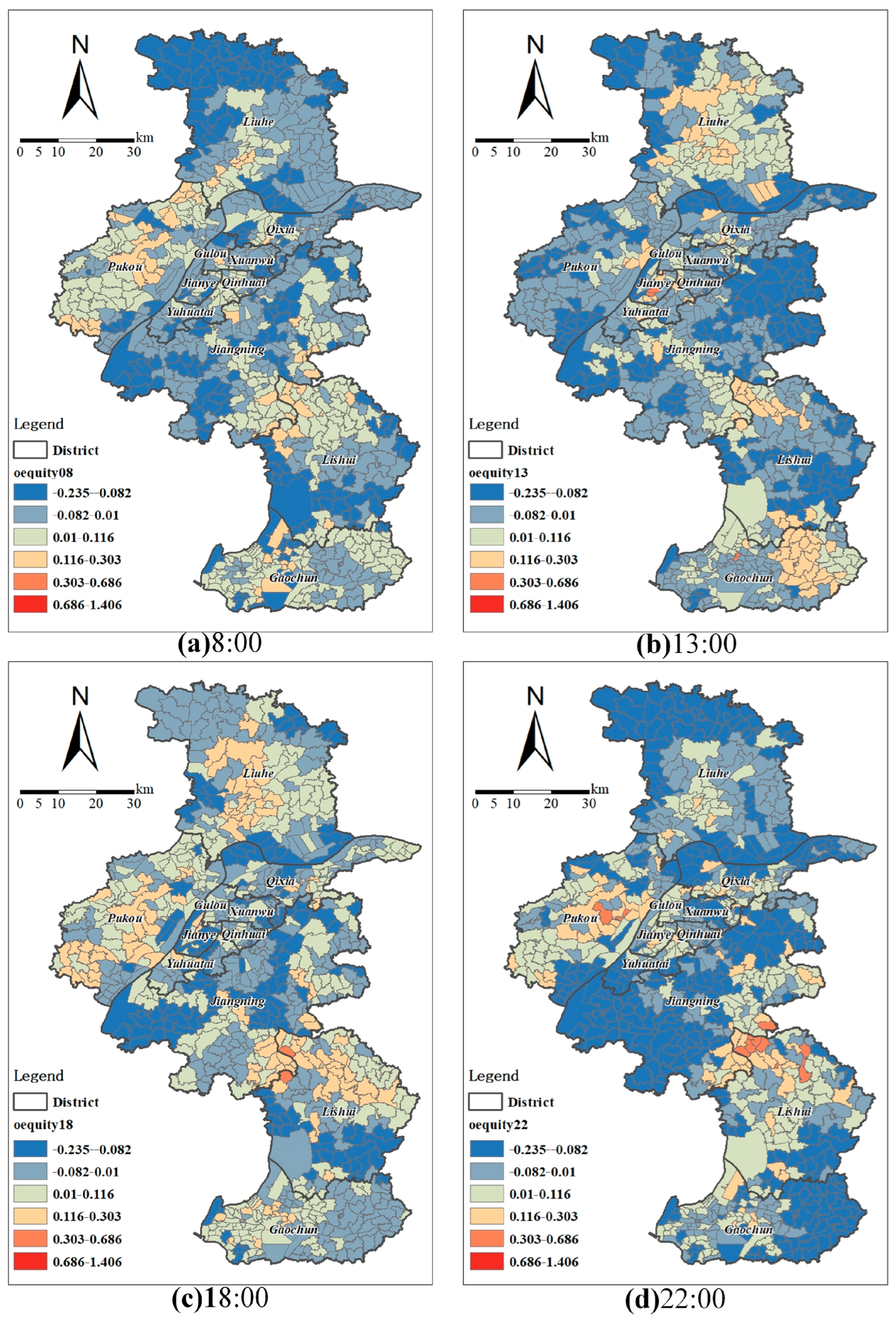
5.3. Equality Comparison before and after Optimization
6. Discussion and Conclusions
6.1. Discussion
- (1)
- EMSs in Nanjing show an aggregate developmental effect; that is, the Matthew effect [57]. However, the distribution of the central city is also uneven. Currently, the EMSs in the major city are concentrated, and the number of EMVs is considerable. Some social groups are concentrated in specific areas in the inner city and form localized contexts in which access to medical facilities and socio-institutional factors intersect and combine to create unequal accessibility. When a strong demand for rescue services close to these EMS stations exists, it is simple to create a shortage that can only be filled by stations located farther away, leading to a longer response time that has a detrimental effect on the overall average response time. As a result, we should monitor how these EMS stations operate from the perspective of the EMV dispatching center, construct more intense auxiliary stations to dispatch more vehicles on time, and increase the emergency network’s resiliency.
- (2)
- Echoing the triple jeopardy of social, environmental, and health inequalities [58], some rural-to-urban migrants may experience health-related disadvantages. This effect becomes significant after considering the spatial accessibility to medical facilities and spatial heterogeneity, suggesting the coupling of institutional and spatial factors over space, which is consistent with the findings of previous studies [59]. The current EMS is concentrated in areas where large hospitals are located, thereby making it possible to quickly solve the first aid station office space problem. After relocation optimization, EMVs should be dispatched to different districts of the central city.
- (3)
- In addition, the reason some stations are not dispatched with EMVs and are closed in the potential application scenarios (Section 5.2) is that the selected EMS station locations may not be optimal; the same phenomenon has been observed in Amsterdam [27].
6.2. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, M.; Wang, F.; Kwan, M.-P.; Chen, J.; Wang, J. Equalizing the spatial accessibility of emergency medical services in Shanghai: A trade-off perspective. Comput. Environ. Urban Syst. 2022, 92, 101745. [Google Scholar] [CrossRef]
- He, Z.; Qin, X.; Xie, Y.; Guo, J. Service Location Optimization Model for Improving Rural Emergency Medical Services. Transp. Res. Rec. 2018, 2672, 83–93. [Google Scholar] [CrossRef]
- Alanis, R.; Ingolfsson, A.; Kolfal, B. A Markov Chain Model for an EMS System with Repositioning. Prod. Oper. Manag. 2013, 22, 216–231. [Google Scholar] [CrossRef]
- Nilsang, S.; Yuangyai, C.; Cheng, C.-Y.; Janjarassuk, U. Locating an ambulance base by using social media: A case study in Bangkok. Ann. Oper. Res. 2019, 283, 497–516. [Google Scholar] [CrossRef]
- Reuter-Oppermann, M.; Berg, P.L.V.D.; Vile, J.L. Logistics for Emergency Medical Service systems. Health Syst. 2017, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Aringhieri, R.; Bruni, M.E.; Khodaparasti, S.; van Essen, J.T. Emergency medical services and beyond: Addressing new challenges through a wide literature review. Comput. Oper. Res. 2017, 78, 349–368. [Google Scholar] [CrossRef]
- Jánošíková, Ľ.; Jankovič, P.; Kvet, M.; Zajacová, F. Coverage versus response time objectives in ambulance location. Int. J. Health Geogr. 2021, 20, 1–16. [Google Scholar] [CrossRef]
- Kwan, M.-P. Geographies of health. Ann. Assoc. Am. Geogr. 2012, 102, 891–892. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Z.; Zhu, X.; Wyatt, T. Covering models and optimization techniques for emergency response facility location and planning: A review. Math. Methods Oper. Res. 2011, 74, 281–310. [Google Scholar] [CrossRef]
- Bélanger, V.; Ruiz, A.; Soriano, P. Recent optimization models and trends in location, relocation, and dispatching of emergency medical vehicles. Eur. J. Oper. Res. 2019, 272, 1–23. [Google Scholar] [CrossRef]
- Yin, C.; He, Q.; Liu, Y.; Chen, W.; Gao, Y. Inequality of public health and its role in spatial accessibility to medical facilities in China. Appl. Geogr. 2018, 92, 50–62. [Google Scholar] [CrossRef]
- Wang, Z.; Tang, K.J.N.M. Combating COVID-19: Health equity matters. Nat. Med. 2020, 26, 458. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Wang, J. Big spatial data for urban and environmental sustainability. Geospat. Inf. Sci. 2020, 23, 125–140. [Google Scholar] [CrossRef]
- Garcia-Albertos, P.; Picornell, M.; Henar Salas-Olmedo, M.; Gutierrez, J. Exploring the potential of mobile phone records and online route planners for dynamic accessibility analysis. Transp. Res. Part A Policy Pract. 2018, 125, 294–307. [Google Scholar] [CrossRef]
- Rong, P.; Zheng, Z.; Kwan, M.-P.; Qin, Y. Evaluation of the spatial equity of medical facilities based on improved potential model and map service API: A case study in Zhengzhou, China. Appl. Geogr. 2020, 119, 102192. [Google Scholar] [CrossRef]
- Hajiali, M.; Teimoury, E.; Rabiee, M.; Delen, D. An interactive decision support system for real-time ambulance relocation with priority guidelines. Decis. Support Syst. 2022, 155, 113712. [Google Scholar] [CrossRef]
- Benabdouallah, M.; Bojji, C. A review on coverage models applied to emergency location. Int. J. Emerg. Manag. 2018, 14, 180–199. [Google Scholar] [CrossRef]
- Brotcorne, L.; Laporte, G.; Semet, F. Ambulance location and relocation models. Eur. J. Oper. Res. 2003, 147, 451–463. [Google Scholar] [CrossRef]
- Neira-Rodado, D.; Escobar-Velasquez, J.W.; McClean, S. Ambulances Deployment Problems: Categorization, Evolution and Dynamic Problems Review. ISPRS Int. J. Geo Inf. 2022, 11, 109. [Google Scholar] [CrossRef]
- Jagtenberg, C.J.; Bhulai, S.; van der Mei, R.D. An efficient heuristic for real-time ambulance redeployment. Health Care Manag. Sci. 2015, 4, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Van Barneveld, T.; Bhulai, S.; van der Mei, R.D. A dynamic ambulance management model for rural areas. Health Care Manag. Sci. 2017, 20, 165–186. [Google Scholar] [CrossRef]
- Repede, J.F.; Bernardo, J.J. Developing and validating a decision support system for locating emergency medical vehicles in Louisville, Kentucky. Eur. J. Oper. Res. 1994, 75, 567–581. [Google Scholar] [CrossRef]
- Gendreau, M.; Laporte, G.; Semet, F. A dynamic model and parallel tabu search heuristic for real-time ambulance relocation. Parallel Comput. 2001, 27, 1641–1653. [Google Scholar] [CrossRef] [Green Version]
- Rajagopalan, H.K.; Saydam, C.; Xiao, J. A multiperiod set covering location model for dynamic redeployment of ambulances. Comput. Oper. Res. 2008, 35, 814–826. [Google Scholar] [CrossRef]
- Schmid, V.; Doerner, K.F. Ambulance location and relocation problems with time-dependent travel times. Eur. J. Oper. Res. 2010, 207, 1293–1303. [Google Scholar] [CrossRef] [Green Version]
- Başar, A.; Çatay, B.; Ünlüyurt, T. A taxonomy for emergency service station location problem. Optim. Lett. 2012, 6, 1147–1160. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, P.L.; Aardal, K. Time-dependent MEXCLP with start-up and relocation cost. Eur. J. Oper. Res. 2015, 242, 383–389. [Google Scholar] [CrossRef]
- Wu, H.; Gui, Z.; Yang, Z. Geospatial big data for urban planning and urban management. Geo-Spat. Inf. Sci. 2020, 23, 273–274. [Google Scholar] [CrossRef]
- Wang, Y.; Tong, D.; Li, W.; Liu, Y. Optimizing the spatial relocation of hospitals to reduce urban traffic congestion: A case study of Beijing. Trans. GIS 2019, 23, 365–386. [Google Scholar] [CrossRef]
- Van Barneveld, T.; Jagtenberg, C.; Bhulai, S.; Van der Mei, R. Real-time ambulance relocation: Assessing real-time redeployment strategies for ambulance relocation. Socio-Econ. Plan. Sci. 2018, 62, 129–142. [Google Scholar] [CrossRef] [Green Version]
- Enayati, S.; Mayorga, M.E.; Rajagopalan, H.K.; Saydam, C. Real-time ambulance redeployment approach to improve service coverage with fair and restricted workload for EMS providers. Omega 2018, 79, 67–80. [Google Scholar] [CrossRef]
- Carvalho, A.S.; Captivo, M.E.; Marques, I. Integrating the ambulance dispatching and relocation problems to maximize system’s preparedness. Eur. J. Oper. Res. 2020, 283, 1064–1080. [Google Scholar] [CrossRef]
- Kochetov, Y.A.; Shamray, N.B. Optimization of the Ambulance Fleet Location and Relocation. J. Appl. Ind. Math. 2021, 15, 234–252. [Google Scholar] [CrossRef]
- Tong, D.; Murray, A.T. Spatial Optimization in Geography. Ann. Assoc. Am. Geogr. 2012, 102, 1290–1309. [Google Scholar] [CrossRef]
- Kwan, M.-P.; Murray, A.T.; O’Kelly, M.E.; Tiefelsdorf, M. Recent advances in accessibility research: Representation, methodology and applications. J. Geogr. Syst. 2003, 5, 129–138. [Google Scholar] [CrossRef]
- Wang, F. Measurement, optimization, and impact of health care accessibility: A methodological review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.; Tan, J.; Li, M.; Wang, J.; Wang, F. Impact of traffic on the spatiotemporal variations of spatial accessibility of emergency medical services in inner-city Shanghai. Environ. Plan. B Urban Anal. City Sci. 2018, 47, 841–854. [Google Scholar] [CrossRef]
- Wan, N.; Zou, B.; Sternberg, T. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Yao, J.; Murray, A.T.; Agadjanian, V. A geographical perspective on access to sexual and reproductive health care for women in rural Africa. Soc. Sci. Med. 2013, 96, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehead, J.; L. Pearson, A.; Lawrenson, R.; Atatoa-Carr, P. How can the spatial equity of health services be defined and measured? A systematic review of spatial equity definitions and methods. J. Health Serv. Res. Policy 2019, 24, 270–278. [Google Scholar] [CrossRef]
- Barbati, M.; Piccolo, C. Equality measures properties for location problems. Optim. Lett. 2016, 10, 903–920. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Tang, Q. Planning toward equal accessibility to services: A quadratic programming approach. Environ. Plan. B Plan. Des. 2013, 40, 195–212. [Google Scholar] [CrossRef]
- Zarandi, M.H.F.; Davari, S.; Sisakht, S.A.H. The large-scale dynamic maximal covering location problem. Math. Comput. Model. 2013, 57, 710–719. [Google Scholar] [CrossRef]
- Toro-Diaz, H.; Mayorga, M.E.; Chanta, S.; Mclay, L.A. Joint location and dispatching decisions for Emergency Medical Services. Comput. Ind. Eng. 2013, 64, 917–928. [Google Scholar] [CrossRef]
- Toro-Díaz, H.; Mayorga, M.; McLay, L.; Rajagopalan, H. Reducing disparities in large-scale emergency medical service systems. J. Oper. Res. Soc. 2015, 66, 1169–1181. [Google Scholar] [CrossRef]
- Naoum-Sawaya, J.; Elhedhli, S. A stochastic optimization model for real-time ambulance redeployment. Comput. Oper. Res. 2013, 40, 1972–1978. [Google Scholar] [CrossRef]
- Mccormack, R.; Coates, G. A simulation model to enable the optimization of ambulance fleet allocation and base station location for increased patient survival. Eur. J. Oper. Res. 2015, 247, 294–309. [Google Scholar] [CrossRef] [Green Version]
- Yan, K.; Jiang, Y.; Qiu, J.; Zhong, X.; Wang, Y.; Deng, J.; Lian, J.; Wang, T.; Cao, C. The equity of China’s emergency medical services from 2010–2014. Int. J. Equity Health 2017, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Järv, O.; Tenkanen, H.; Toivonen, T. Enhancing spatial accuracy of mobile phone data using multi-temporal dasymetric interpolation. Int. J. Geogr. Inf. Sci. 2017, 31, 1630–1651. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Zhen, F.; Zhang, H. The Dynamic Changes of Urban Space-time Activity and Activity Zoning Based on Check-in Data in Sina Web. Sci. Geogr. Sin. 2015, 35, 151–160. [Google Scholar] [CrossRef]
- Xia, N.; Cheng, L.; Chen, S.; Wei, X.; Zong, W.; Li, M. Accessibility based on Gravity-Radiation model and Google Maps API: A case study in Australia. J. Transp. Geogr. 2018, 72, 178–190. [Google Scholar] [CrossRef]
- Amap-Maps. Guides for Directions API. Available online: https://lbs.amap.com/api/webservice/guide/api/direction (accessed on 9 March 2023).
- Ren, F.; Tong, D.; Kwan, M.P. Space–time measures of demand for service: Bridging location modelling and accessibility studies through a time-geographic framework. Geogr. Ann. Ser. B Hum. Geogr. 2014, 96, 329–344. [Google Scholar] [CrossRef]
- Liu, D.; Cai, S. A spatial-temporal modeling approach to reconstructing land-cover change trajectories from multi-temporal satellite imagery. Ann. Assoc. Am. Geogr. 2012, 102, 1329–1347. [Google Scholar] [CrossRef]
- Xia, T.; Song, X.; Zhang, H.; Song, X.; Kanasugi, H.; Shibasaki, R. Measuring spatio-temporal accessibility to emergency medical services through big GPS data. Health Place 2019, 56, 53–62. [Google Scholar] [CrossRef]
- Dick, W.F. Anglo-American vs. Franco-German emergency medical services system. Prehospital Disaster Med. 2003, 18, 29–37. [Google Scholar] [CrossRef]
- Perc, M. The Matthew effect in empirical data. J. R. Soc. Interface 2014, 11, 20140378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, J.R.; Richardson, E.A.; Mitchell, R.J.; Shortt, N.K. Environmental justice and health: The implications of the socio-spatial distribution of multiple environmental deprivation for health inequalities in the United Kingdom. Trans. Inst. Br. Geogr. 2010, 35, 522–539. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Tao, Y. Associations between spatial access to medical facilities and health-seeking behaviors: A mixed geographically weighted regression analysis in Shanghai, China. Appl. Geogr. 2022, 139, 102644. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Iteration Count | Population Size | CP | MP | CC | MC | top | bottom | Average Fitness | Max Fitness |
|---|---|---|---|---|---|---|---|---|---|---|
| A1 | 250 | 200 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 10.54 | 19.47 |
| A2 | 500 | 200 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 9.9 | 18.86 |
| A3 | 1000 | 200 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 9.745 | 18.60 |
| B1 | 250 | 400 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 10.14 | 20.45 |
| B2 | 500 | 400 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 11.32 | 20.72 |
| B3 | 1000 | 400 | 0.8 | 0.2 | 8 | 8 | 15 | 1 | 11.20 | 19.25 |
| C1 | 500 | 200 | 0.9 | 0.1 | 8 | 8 | 15 | 1 | 11.87 | 21.61 |
| C2 | 500 | 200 | 0.7 | 0.3 | 8 | 8 | 15 | 1 | 10.00 | 17.22 |
| C3 | 500 | 200 | 0.6 | 0.4 | 8 | 8 | 15 | 1 | 7.31 | 17.24 |
| D1 | 500 | 200 | 0.8 | 0.2 | 4 | 4 | 15 | 1 | 14.45 | 23.38 |
| D2 | 500 | 200 | 0.8 | 0.2 | 12 | 12 | 15 | 1 | 8.81 | 16.82 |
| D3 | 500 | 200 | 0.8 | 0.2 | 16 | 16 | 15 | 1 | 6.99 | 15.91 |
| E1 | 500 | 200 | 0.8 | 0.2 | 8 | 8 | 20 | 1 | 11.72 | 21.15 |
| E2 | 500 | 200 | 0.8 | 0.2 | 8 | 8 | 10 | 1 | 11.14 | 19.32 |
| E3 | 500 | 200 | 0.8 | 0.2 | 8 | 8 | 10 | 0 | 19.99 | 42.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, X.; Chen, Y.; Li, Y.; Liu, B.; Yu, Z. Spatiotemporal Data-Driven Multiperiod Relocation Optimization of Emergency Medical Services: Maximum Equality Objective. ISPRS Int. J. Geo-Inf. 2023, 12, 269. https://doi.org/10.3390/ijgi12070269
Zhou X, Chen Y, Li Y, Liu B, Yu Z. Spatiotemporal Data-Driven Multiperiod Relocation Optimization of Emergency Medical Services: Maximum Equality Objective. ISPRS International Journal of Geo-Information. 2023; 12(7):269. https://doi.org/10.3390/ijgi12070269
Chicago/Turabian StyleZhou, Xinxin, Yujie Chen, Yingying Li, Bingjie Liu, and Zhaoyuan Yu. 2023. "Spatiotemporal Data-Driven Multiperiod Relocation Optimization of Emergency Medical Services: Maximum Equality Objective" ISPRS International Journal of Geo-Information 12, no. 7: 269. https://doi.org/10.3390/ijgi12070269