

The Impact of Atmospheric Temperature Variations on Glycaemic Patterns in Children and Young Adults with Type 1 Diabetes

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Medical Data
2.3. Meteorological Data
3. Results
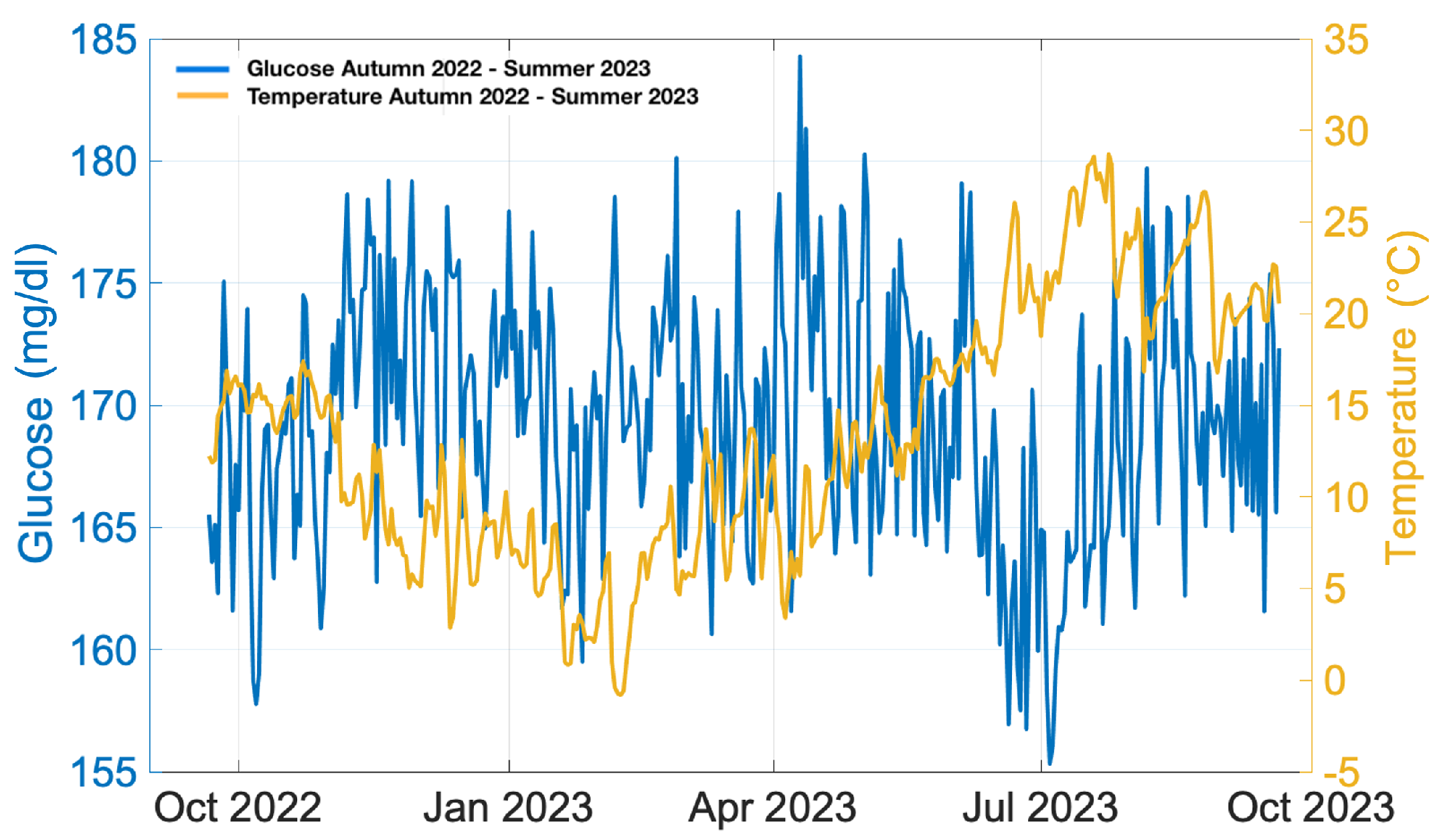
3.1. Annual Analysis
- Number of days for which the sensor was worn (recommended ≥ 14 days)
- CGM utilisation rate (recommended >70%)
- Average blood glucose
- Estimated glycated haemoglobin
- Glycaemic variability (target CV ≤ 36%)
- TAR (>250 mg/dL) [Level 2]: <5%
- TAR (181–250 mg/dL) [Level 1]: <25%
- TIR (70–180 mg/dL): >70%
- TBR (54–69 mg/dL) [Level 1]: <4%
- TBR (<54 mg/dL) [Level 2]: <1%
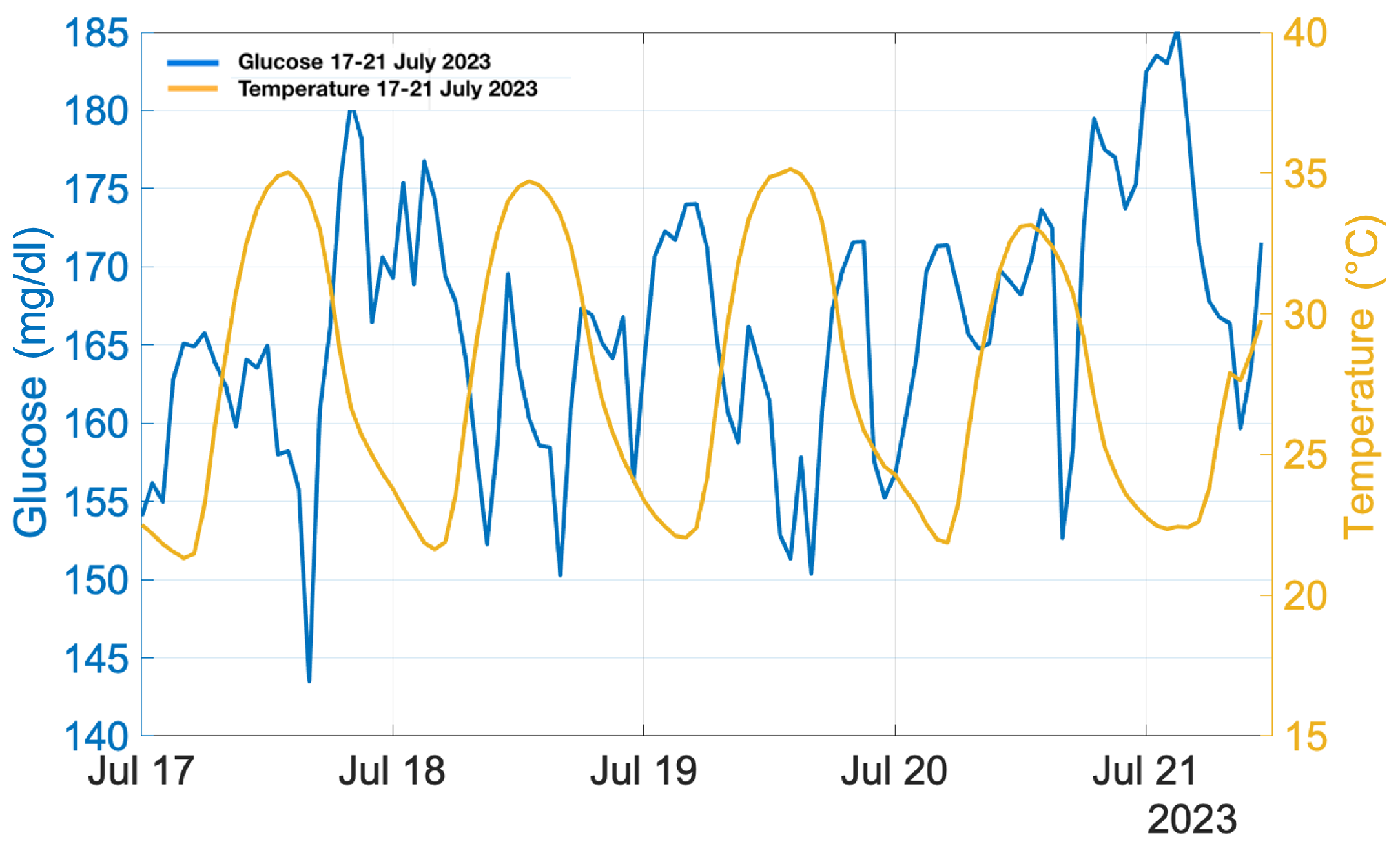
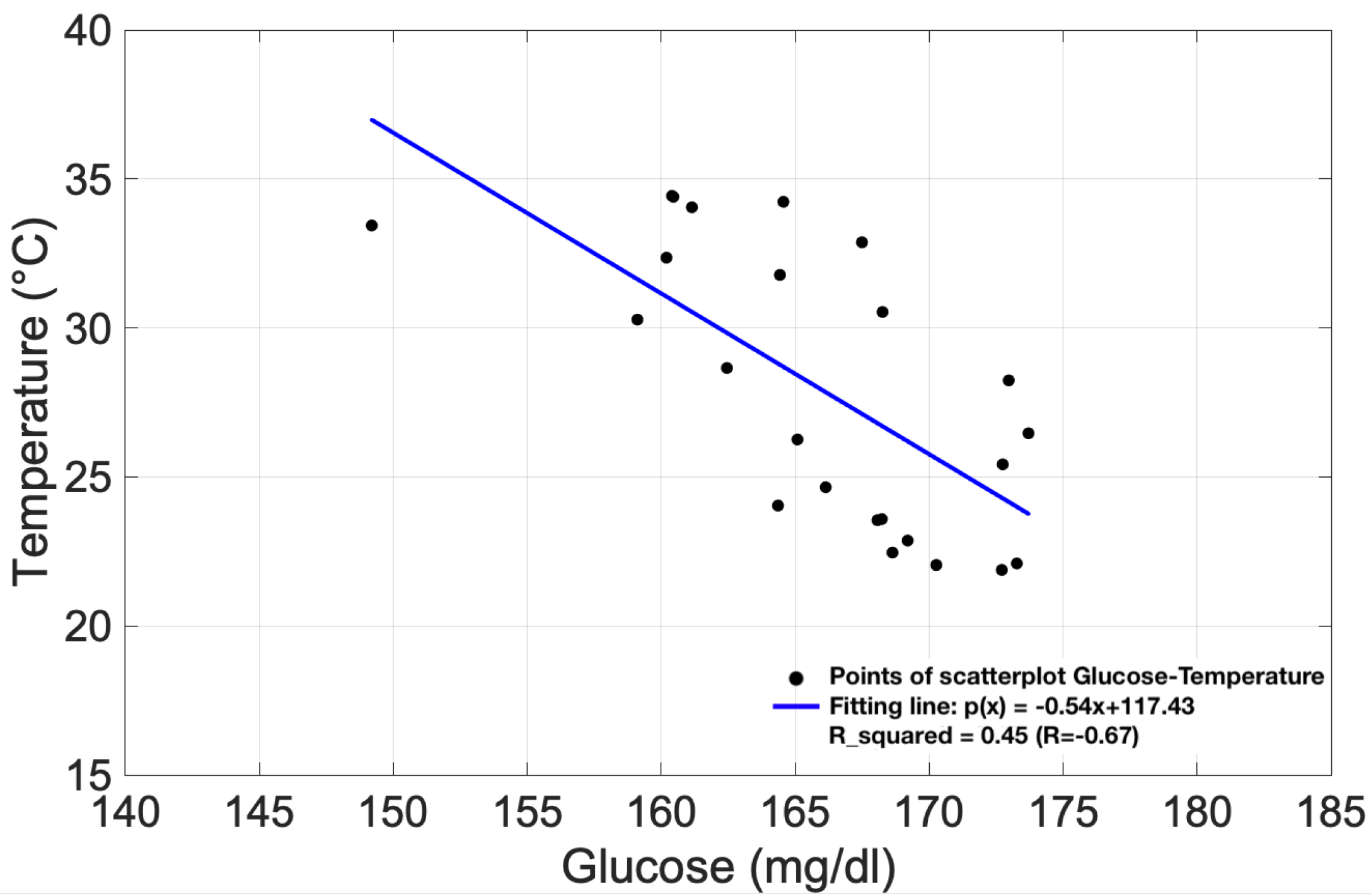
3.2. Heatwave Analysis
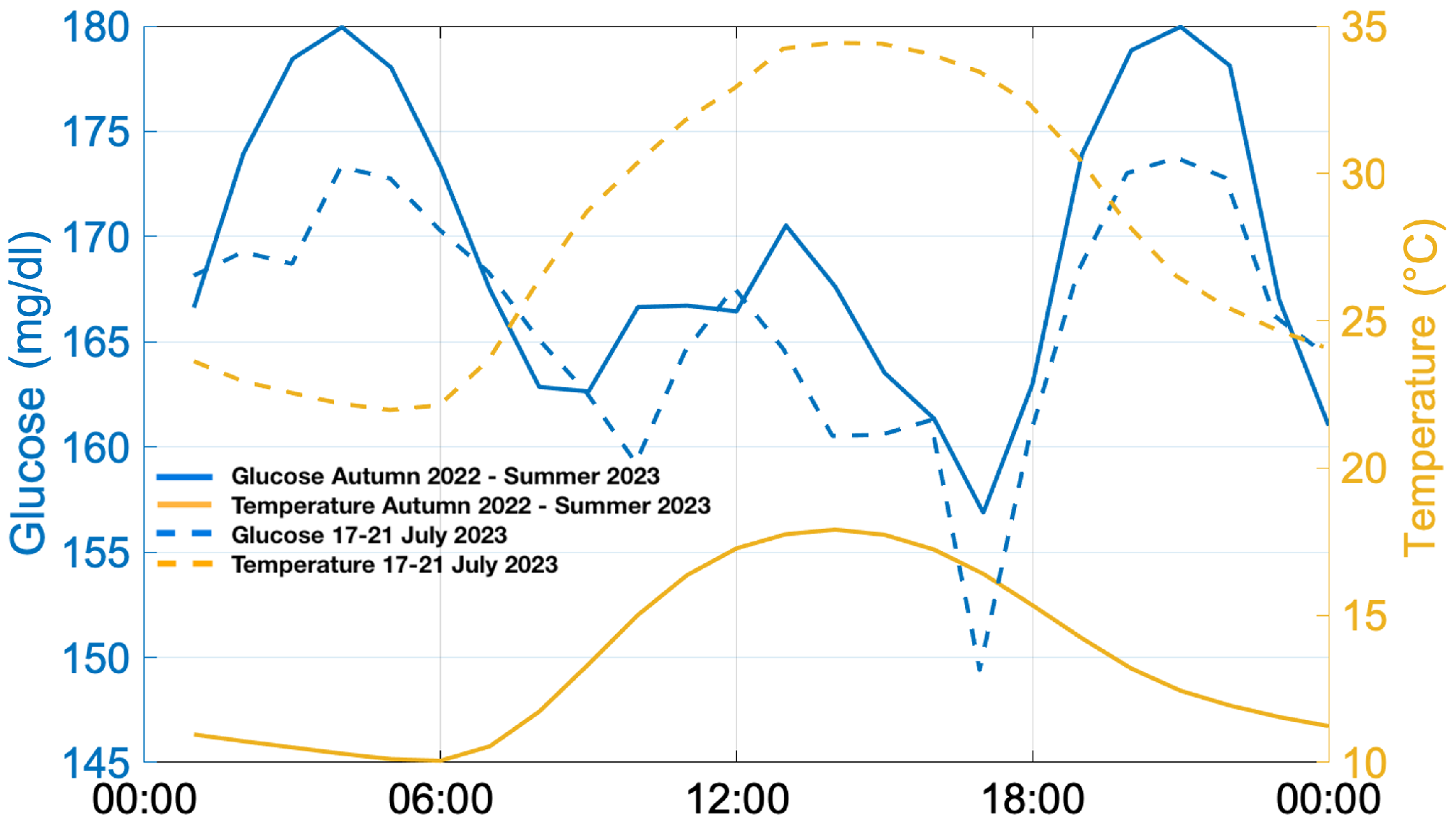
3.3. Overall Results Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gale, E.A.M. Type 1 diabetes in the young: The harvest of sorrow goes on. Diabetologia 2005, 48, 1435–1438. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.J.; Wherrett, D.K. Care of diabetes in children and adolescents: Controversies, changes, and consensus. Lancet 2015, 385, 2096–2106. [Google Scholar] [CrossRef] [PubMed]
- Clements, M.A.; Foster, N.C.; Maahs, D.M.; Schatz, D.A.; Olson, B.A.; Tsalikian, E.; Lee, J.M.; Burt-Solorzano, C.M.; Tamborlane, W.V.; Chen, V.; et al. Hemoglobin A1c (HbA1c) changes over time among adolescent and young adult participants in the T1D exchange clinic registry. Pediatr. Diabetes 2016, 17, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Addala, A.; Ding, V.; Zaharieva, D.P.; Bishop, F.K.; Adams, A.S.; King, A.C.; Johari, R.; Scheinker, D.; Hood, K.K.; Desai, M.; et al. Disparities in hemoglobin A1c levels in the first year after diagnosis among youths with type 1 diabetes offered continuous glucose monitoring. JAMA Netw. Open 2023, 6, e238881. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.R.; Barnett, A.G.; Connell, D.; Tong, S. Ambient Temperature and Cardiorespiratory Morbidity. Epidemiology 2012, 23, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Cicci, K.R.; Maltby, A.; Clemens, K.K.; Vicedo-Cabrera, A.M.; Gunz, A.C.; Lavigne, E.; Wilk, P. High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 11243. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yin, P.; Zhou, M.; Ou, C.Q.; Guo, Y.; Gasparrini, A.; Liu, Y.; Yue, Y.; Gu, S.; Sang, S.; et al. Cardiovascular mortality risk attributable to ambient temperature in China. Heart 2015, 101, 1966. [Google Scholar] [CrossRef]
- Zheng, S.; Zhang, X.; Zhu, W.; Nie, Y.; Ke, X.; Liu, S.; Wang, X.; You, J.; Kang, F.; Bai, Y.; et al. A study of temperature variability on admissions and deaths for cardiovascular diseases in Northwestern China. BMC Public Health 2023, 23, 1751. [Google Scholar] [CrossRef]
- Gasparrini, A.; Guo, Y.; Hashizume, M.; Lavigne, E.; Zanobetti, A.; Schwartz, J.; Tobias, A.; Tong, S.; Rocklöv, J.; Forsberg, B.; et al. Mortality risk attributable to high and low ambient temperature: A multicountry observational study. Lancet 2015, 386, 369–375. [Google Scholar] [CrossRef]
- Lu, C.L.; Chang, H.H.; Chen, H.F.; Ku, L.J.E.; Chang, Y.H.; Shen, H.N.; Li, C.Y. Inverse relationship between ambient temperature and admissions for diabetic ketoacidosis and hyperglycemic hyperosmolar state: A 14-year time-series analysis. Environ. Int. 2016, 94, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Zhao, Q.; Coelho, M.S.; Saldiva, P.H.; Zoungas, S.; Huxley, R.R.; Abramson, M.J.; Guo, Y.; Li, S. Association between Heat Exposure and Hospitalization for Diabetes in Brazil during 2000–2015: A Nationwide Case-Crossover Study. Environ. Health Perspect. 2019, 127, 117005. [Google Scholar] [CrossRef]
- Miyamura, K.; Nawa, N.; Nishimura, H.; Fushimi, K.; Fujiwara, T. Association between heat exposure and hospitalization for diabetic ketoacidosis, hyperosmolar hyperglycemic state, and hypoglycemia in Japan. Environ. Int. 2022, 167, 107410. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, T.; Yamamoto-Honda, R.; Kajio, H.; Kishimoto, M.; Noto, H.; Hachiya, R.; Kimura, A.; Kakei, M.; Noda, M. Seasonal Variations of Severe Hypoglycemia in Patients With Type 1 Diabetes Mellitus, Type 2 Diabetes Mellitus, and Non-diabetes Mellitus. Medicine 2014, 93, e148. [Google Scholar] [CrossRef]
- Lanzinger, S.; Biester, T.; Siegel, E.; Schneider, A.; Schöttler, H.; Placzek, K.; Klinkert, C.; Heidtmann, B.; Ziegler, J.; Holl, R. The impact of daily mean air temperature on the proportion of time in hypoglycemia in 2582 children and adolescents with type 1 diabetes—Is this association clinically relevant? Environ. Res. 2023, 233, 116488. [Google Scholar] [CrossRef]
- Bernstein, A.S.; Sun, S.; Weinberger, K.R.; Spangler, K.R.; Sheffield, P.E.; Wellenius, G.A. Warm Season and Emergency Department Visits to U.S. Children’s Hospitals. Environ. Health Perspect. 2022, 130, 017001. [Google Scholar] [CrossRef] [PubMed]
- Bogar, K.; Brensinger, C.M.; Hennessy, S.; Flory, J.H.; Bell, M.L.; Shi, C.; Bilker, W.B.; Leonard, C.E. Climate Change and Ambient Temperature Extremes: Association With Serious Hypoglycemia, Diabetic Ketoacidosis, and Sudden Cardiac Arrest/Ventricular Arrhythmia in People with Type 2 Diabetes. Diabetes Care 2022, 45, e171–e173. [Google Scholar] [CrossRef]
- Al-Qaissi, A.; Papageorgiou, M.; Javed, Z.; Heise, T.; Rigby, A.S.; Garrett, A.T.; Hepburn, D.; Kilpatrick, E.S.; Atkin, S.L.; Sathyapalan, T. Environmental effects of ambient temperature and relative humidity on insulin pharmacodynamics in adults with type 1 diabetes mellitus. Diabetes Obes. Metab. 2019, 21, 569–574. [Google Scholar] [CrossRef]
- Smith, C.J. Pediatric Thermoregulation: Considerations in the Face of Global Climate Change. Nutrients 2019, 11, 2010. [Google Scholar] [CrossRef]
- Perera, F.; Nadeau, K. Climate Change, Fossil-Fuel Pollution, and Children’s Health. N. Engl. J. Med. 2022, 386, 2303–2314. [Google Scholar] [CrossRef] [PubMed]
- Morandi, A.; Piona, C.; Corradi, M.; Marigliano, M.; Giontella, A.; Orsi, S.; Emiliani, F.; Tagetti, A.; Marcon, D.; Fava, C.; et al. Risk factors for pre-clinical atherosclerosis in adolescents with type 1 diabetes. Diabetes Res. Clin. Pract. 2023, 198, 110618. [Google Scholar] [CrossRef]
- Mannucci, E.; Monami, M.; Dicembrini, I.; Piselli, A.; Porta, M. Achieving HbA1c targets in clinical trials and in the real world: A systematic review and meta-analysis. J. Endocrinol. Investig. 2014, 37, 477–495. [Google Scholar] [CrossRef] [PubMed]
- Freckmann, G.; Schauer, S.; Beltzer, A.; Waldenmaier, D.; Buck, S.; Baumstark, A.; Jendrike, N.; Link, M.; Zschornack, E.; Haug, C.; et al. Continuous Glucose Profiles in Healthy People With Fixed Meal Times and Under Everyday Life Conditions. J. Diabetes Sci. Technol. 2024, 18, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Danne, T.; Nimri, R.; Battelino, T.; Bergenstal, R.M.; Close, K.L.; DeVries, J.H.; Garg, S.; Heinemann, L.; Hirsch, I.; Amiel, S.A.; et al. International consensus on use of continuous glucose monitoring. Diabetes Care 2017, 40, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Medium-Range Weather Forecasts (ECMWF), C.D.N. Heat Stress and the European Heatwave of 2023. 2023. Available online: https://www.ecmwf.int/en/about/media-centre/science-blog/2023/heat-stress-and-european-heatwave-2023 (accessed on 11 May 2024).
- Copernicus. European Summer 2023: A Season of Contrasting Extremes. 2023. Available online: https://climate.copernicus.eu/european-summer-2023-season-contrasting-extremes (accessed on 11 May 2024).
- Copernicus. The European Heatwave of July 2023 in a Longer-Term Context. 2023. Available online: https://climate.copernicus.eu/european-heatwave-july-2023-longer-term-context (accessed on 11 May 2024).
- Fiorillo, E.; Brilli, L.; Carotenuto, F.; Cremonini, L.; Gioli, B.; Giordano, T.; Nardino, M. Diurnal Outdoor Thermal Comfort Mapping through Envi-Met Simulations, Remotely Sensed and In Situ Measurements. Atmosphere 2023, 14, 641. [Google Scholar] [CrossRef]
- Kalliora, M.I.; Vazeou, A.; Delis, D.; Bozas, E.; Thymelli, I.; Bartsocas, C.S. Seasonal variation of type 1 diabetes mellitus diagnosis in Greek children. Hormones 2011, 10, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Mianowska, B.; Fendler, W.; Szadkowska, A.; Baranowska, A.; Grzelak-Agaciak, E.; Sadon, J.; Keenan, H.; Mlynarski, W. HbA1c levels in schoolchildren with type 1 diabetes are seasonally variable and dependent on weather conditions. Diabetologia 2011, 54, 749–756. [Google Scholar] [CrossRef]
- Shephard, R.J.; Aoyagi, Y. Seasonal variations in physical activity and implications for human health. Eur. J. Appl. Physiol. 2009, 107, 251–271. [Google Scholar] [CrossRef]
- Bhutani, S.; Wells, N.; Finlayson, G.; Schoeller, D.A. Change in eating pattern as a contributor to energy intake and weight gain during the winter holiday period in obese adults. Int. J. Obes. 2020, 44, 1586–1595. [Google Scholar] [CrossRef]
- Lai, S.W.; Chang, W.C.; Lin, C.L.; Chou, I.C.; Tsai, F.J.; Lai, Y.J. Low ambient temperatures correlate with increased risk of hypoglycemia in patients with type 2 diabetes. Medicine 2020, 99, e19287. [Google Scholar] [CrossRef]
- Tumini, S.; Comegna, L.; Fioretti, E.; Guidone, P.; Levantini, G.; Panichi, D.; Catenaro, M.; Rossi, I.; Amaro, F.; Graziano, G.; et al. Effectiveness and safety of flexible therapeutic schemes including first- and secondgeneration basal insulins during a pediatric summer diabetes camp. Pediatr. Rep. 2020, 12, 8254. [Google Scholar] [CrossRef] [PubMed]
- Tumini, S.; Fioretti, E.; Rossi, I.; Cipriano, P.; Franchini, S.; Guidone, P.I.; Petrosino, M.I.; Saggino, A.; Tommasi, M.; Picconi, L.; et al. Fear of hypoglycemia in children with type 1 diabetes and their parents: Validation of the Italian version of the Hypoglycemia Fear Survey for Children and for Parents. Pediatr. Diabetes 2022, 23, 126–138. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 138 |
| Gender (M/F) | |
| Males | 47% |
| Females | 53% |
| Age | |
| 0–6 years | 3% |
| 7–8 years | 7% |
| 9–11 years | 11% |
| 12–17 | 53% |
| 18–21 | 26% |
| Concomitant illness | |
| Celiac disease | 11% |
| Hypothyroidism | 9% |
| Diabetes duration (years) | 1–8 |
| Mean HbA1c % (mmol/mol) | 7.08 ± 1.2 (54 ± 13) |
| % of patients characterised by HbA1c target [22] | |
| HbA1c % (<58 mmol/mol) | 63% |
| HbA1c % (≥58 mmol/mol) | 37% |
| Type of insulin | |
| Pre-prandial insulin/kg (mean value) | 0.47 IU/kg |
| Basal insulin/kg (mean value) | 0.38 IU/kg |
| Season-Year | % of Patients |
|---|---|
| Autumn-2022 | 33% |
| Winter-2022 | 30% |
| Spring-2023 | 30% |
| Summer-2023 | 31% |
| Parameter | Recommended Value | % of Patients Autumn 2022 | % of Patients Winter 2022 | % of Patients Spring 2023 | % of Patients Summer 2023 |
|---|---|---|---|---|---|
| TAR (>250 mg/dL) | <5% | 60% | 55% | 63% | 60% |
| TAR (181–250 mg/dL) | <25% | 78% | 71% | 73% | 79% |
| TIR (70–180 mg/dL) | >70% | 27% | 26% | 27% | 21% |
| TBR (54–69 mg/dL) | <4% | 100% | 98% | 98% | 93% |
| TBR (<54 mg/dL) | <1% | 100% | 100% | 100% | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiacchiaretta, P.; Tumini, S.; Mascitelli, A.; Sacrini, L.; Saltarelli, M.A.; Carabotta, M.; Osmelli, J.; Di Carlo, P.; Aruffo, E. The Impact of Atmospheric Temperature Variations on Glycaemic Patterns in Children and Young Adults with Type 1 Diabetes. Climate 2024, 12, 121. https://doi.org/10.3390/cli12080121
Chiacchiaretta P, Tumini S, Mascitelli A, Sacrini L, Saltarelli MA, Carabotta M, Osmelli J, Di Carlo P, Aruffo E. The Impact of Atmospheric Temperature Variations on Glycaemic Patterns in Children and Young Adults with Type 1 Diabetes. Climate. 2024; 12(8):121. https://doi.org/10.3390/cli12080121
Chicago/Turabian StyleChiacchiaretta, Piero, Stefano Tumini, Alessandra Mascitelli, Lorenza Sacrini, Maria Alessandra Saltarelli, Maura Carabotta, Jacopo Osmelli, Piero Di Carlo, and Eleonora Aruffo. 2024. "The Impact of Atmospheric Temperature Variations on Glycaemic Patterns in Children and Young Adults with Type 1 Diabetes" Climate 12, no. 8: 121. https://doi.org/10.3390/cli12080121
APA StyleChiacchiaretta, P., Tumini, S., Mascitelli, A., Sacrini, L., Saltarelli, M. A., Carabotta, M., Osmelli, J., Di Carlo, P., & Aruffo, E. (2024). The Impact of Atmospheric Temperature Variations on Glycaemic Patterns in Children and Young Adults with Type 1 Diabetes. Climate, 12(8), 121. https://doi.org/10.3390/cli12080121