Abstract
While contraception prescribing by pharmacists has seen rapid growth in recent years, pharmacist-provided services that can impact maternal health encompass more than just contraception. Each phase of maternal health—preconception, pregnancy, and post-pregnancy—has unique needs, and pharmacists are well equipped to provide services to meet those needs and are more accessible than other healthcare providers. While pharmacist-provided maternal health services may lead to significant savings to the healthcare system, additional research to more fully capture the value of pharmacist-provided maternal health services is needed. Robust implementation of a pharmacist-provided maternal health services program will require partnerships between providers, payers, and pharmacists. Infant and maternal mortality, preterm birth, and unintended pregnancies are significant public health issues, and pharmacists should be seen as a capable workforce who can provide needed maternal health care and serve as a gateway into the healthcare system for those capable of pregnancy.
1. Introduction
Maternal health refers to the health of women during the pre-pregnancy, pregnancy, and postpartum periods [1]. The purpose of providing maternal health care is to improve the health of women, as well as the outcome of any pregnancy they may choose to have. In the United States (U.S.), maternal health is monitored and evaluated through assessment of the prevalence of chronic disease states and health behaviors among women of reproductive age as well as pregnancy-related morbidity and mortality [2]. Higher rates of chronic health conditions, obesity, and maternal morbidity and mortality along with higher rates of infant mortality than comparable countries demonstrate the need for provision of routine maternal health care in the U.S. [3].
When conceptualizing maternal health, it is important to recognize that there are a broad series of factors that can adversely impact health through one’s lifetime. These health burdens not only may adversely impact women of childbearing age themselves, but also may impact a pregnancy [2]. Waiting for a patient to receive prenatal care is likely too late to address many risk factors for adverse maternal-fetal outcomes, especially as nearly half of pregnancies in the U.S. are unintended [4]; further, 1 in 16 pregnant women in the U.S. receive no or inadequate prenatal care [5]. Ensuring access to affordable and comprehensive health care is a key component to improving health outcomes [6].
Currently, however, the U.S. health care system suffers from a shortage of primary care providers, including obstetricians and gynecologists, and financial barriers to care [6]. It is estimated 11% of women in the United States are uninsured, with millions more underinsured [7]. Women may not be able to access routine, preventive health care services or may delay needed care [6]. As part of the comprehensive health care team, pharmacists are well-positioned to close many of these gaps in maternal health care [8]. While much attention has been given in recent years to legislation that grants pharmacists prescriptive authority over contraception products, it must be made clear that pharmacy-based maternal health services do not stop at the provision of contraception.
The purpose of this perspective is to describe the broad impact pharmacists may have on the provision of maternal health services, as well as forward-looking considerations to accelerate service implementation and expansion. Within the context of this article, it should also be noted that not all people who become pregnant or give birth identify as women; therefore, while “women’s health” and related terms may exist in the body of literature and may continue to be used in this area in some publications referenced in this perspective, terms used throughout this perspective should be interpreted to imply inclusive and intentional care for all who are capable of becoming pregnant.
2. Pharmacists’ Potential to Fill Gaps in Care
Maternal health refers to health in the pre-pregnancy, pregnancy, and postpartum periods [1]. Patients need high quality healthcare services, education and support before, during, and after pregnancy as part of comprehensive primary care [9,10]. All healthcare providers and teams should be cognizant of the factors that contribute to overall health and should regularly identify and intervene on potential risks for reproductive-age patients (typically 15–45 years) [2]. Every patient interaction with a healthcare provider represents an opportunity to ensure that evidence-based standards of care as well as social needs are being met in a culturally appropriate manner [2,11]. Although usually framed as well-woman care, these services should be provided as appropriate to all patients capable of becoming pregnant regardless of gender [11].
About 96% of the total population lives within 10 miles of a community pharmacy [12]. Such accessibility can be helpful for patients that would otherwise travel long distances to see a physician. In addition, patients are much more likely to frequent a pharmacy than a physician’s office. Specific to the Medicare population, the median number of annual visits to community pharmacies is nearly double that which is observed among primary care physician office visits [13]. Across a more general population, the difference widens, with 35 visits to pharmacies as compared to 4 visits to primary care providers [14]. Therefore, pharmacists as providers of women’s and maternal health care services may be logical from a convenience, accessibility, and cost standpoint.
Pharmacists are trained to provide comprehensive, quality health care services. Studies have shown positive outcomes when pharmacists are involved in the management of chronic medical conditions, and immunization rates have improved since pharmacists have been authorized to administer vaccines [15]. Pharmacists are providing medical screening, health and wellness counseling, medication management services, and patient education. Primary care services, including women’s health, can be provided by pharmacists to help alleviate the shortage of primary care physicians [16].
Pharmacists are capable of providing many of the needed maternal health services and, given their accessibility, may fill a gap for patients not receiving these services elsewhere [8]. For a few of the services listed below, pharmacists will need to refer patients to other healthcare providers through clinical-community linkages [8]. In addition to prevention services, pharmacists play an important role in disease state management; chronic conditions such as hypertension and diabetes need to be well-controlled pre-pregnancy to optimize the health of patients and mitigate risks for adverse maternal-fetal outcomes [11]. Yet, a recent study showed that for non-pregnant women aged 20–44 years with hypertension, nearly 41% were uncontrolled and among those with diagnosed diabetes, nearly 52% were uncontrolled [17]. Furthermore, pharmacists are in a perfect position to review and assess a patient’s current medication profile to identify potentially teratogenic medications and supplements that may need to be discontinued prior to conception, and to ensure effective contraceptive coverage in the meantime to avoid inadvertent exposures [11].
3. Clinical and Service Considerations
Community pharmacists wanting to initiate such services should consult evidence-based resources to determine where to begin. Table 1 summarizes the current recommendations from the Women’s Preventive Services Initiative (WPSI) regarding well-woman care for reproductive-age women [18]; as these are updated annually, clinicians should ensure they are referencing the latest version of the guidelines [19]. For the purpose of this manuscript, the WPSI Recommendations are referenced, but it should be noted that additional resources have been produced by other organizations that may be helpful to pharmacists. For instance, the U.S. Centers for Disease Control and Prevention (CDC) also has several resources available around preventive, preconception, and pregnancy planning services that pharmacists can reference [20].

Table 1.
Women’s Preventive Services Initiative (WPSI) Recommendations Regarding Well-Woman Care for Reproductive-Age Women, 2022.
After reviewing Table 1, a pharmacist may realize that they already provide one or more of these services and can consider how they may want to frame and promote the services as related to maternal health, and which new services may make sense to add onto the existing ones. Similarly, if a community pharmacist is already providing direct access to contraceptive services or dispensing a contraceptive product, it may not be a stretch to add on other needed services as appropriate [21]. Pharmacists may find it helpful to consult outside resources to receive practical guidance on how to implement or expand a pharmacy service [22,23,24,25,26,27,28,29,30].
Figure 1 shows the recommended pharmacists’ maternal health services sets and provides a visualization for how the services relate and should be implemented. All patients, regardless of pregnancy status, should receive the Women’s Health Services Set [8]. Pregnant patients should receive the Pregnancy Services set as appropriate [8]. For non-pregnant patients of reproductive potential, pharmacists should assess ability or desire to conceive in the next year (also known as the “One Key Question Initiative®”) [8,11]. Patients not currently planning a pregnancy should be offered contraceptive services if desired and should also still receive education and counseling to reduce risks, should unintended pregnancy occur. Patients desiring a pregnancy should receive the Preconception (prior to first pregnancy) or Interconception (between pregnancy) Service Set in order to optimize health before pregnancy [8]. Once the recommended intervention has been performed, the pharmacist should follow-up as appropriate to ensure the patient receives any additional required services; for example, blood pressure screening may result in pharmacist-provided management of the disease state or a referral to a prescriber, per scope of practice.
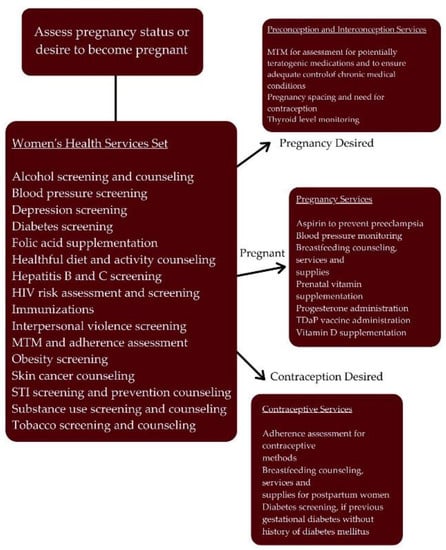
Figure 1.
Women’s Health Services Set Flowchart. Reprinted with permission from the National Alliance of State Pharmacy Associations (NASPA).
Regardless of which service set is applied, pharmacists should not lose sight of care foundations that would apply to other conditions and populations. For example, when providing care, documentation and communication to ensure coordinated care is paramount. Enhanced interoperability of electronic health records, such as integration of community pharmacies into health information exchange, will facilitate care coordination and reduce fragmented care [2]. In addition, while there are multiple clinical considerations to be addressed, pharmacists must also consider social determinants of health (SDoH) that have a large impact for some patients [2,6,11]. Using the Pharmacists’ Patient Care Process, pharmacists can identify and address patient SDoH-related needs [31]. Through this, pharmacists may be able to help address disparities currently seen in maternal health based on geography or race/ethnicity [2].
4. Value of Interventions
The return on investment of maternal health services is difficult to quantify due to the limited studies on the topic, the varied nature of interventions, and the extended time horizon to see potential benefits [32,33]. In order to develop strong economic data, consensus and standardization of study approaches would be helpful [33]. Until greater clarity emerges on long-term economic impacts of interventions, other strategies, such as comparing cost per intervention when provided by a physician versus when provided by a pharmacist, may be useful in the near term. Such analyses may still be difficult to conduct as a physician may, for instance, prescribe a contraception product during another visit, with a total cost that accounts for multiple interventions. However, knowing that there are visits that are essentially exclusively for the provision of contraception prescriptions, simpler math may be done to suggest cost savings when pharmacists prescribe contraception products. While one could argue that pharmacist-provided services may reduce physician visits, which could reduce other cost-effective and beneficial screenings, recent studies do not suggest that this objection should be a hindrance to pharmacist-prescribed contraception [34]. In some cases, particularly in areas with a primary care provider shortage, leveraging pharmacists to provide this service may help with local health care capacity issues as well. Therefore, consideration of the direct and indirect costs of pharmacist-provided service provision may allow for simpler justification for selected pharmacist interventions.
A study in Oregon, the first U.S. state to authorize pharmacists to independently prescribe hormonal contraceptives, showed significant benefit to the state Medicaid program when pharmacists were involved. Within the first two years of the policy change, pharmacists wrote 10% of new prescriptions for hormonal contraceptives, with 74% of those patients not using any form of birth control in the month prior to the pharmacist’s prescription. The study also showed that pharmacists prevented more than 50 unintended pregnancies and saved the state $1.6 million in public costs [35]. A 2010 study in North Carolina demonstrated that administration of subcutaneous medroxyprogesterone acetate by community pharmacists was not only feasible but showed continuation rates and patient satisfaction comparable to the family planning clinic [36].
Interventions conducted by pharmacists can vary drastically. For instance, the aforementioned “One Key Question®” could be a simple question routinely built into existing patient counseling that is routinely offered in community pharmacies nationwide. Accounting for the time spent by adding that question to counseling would be minimal but could have substantial impact if it results in a change in therapy or other more complex intervention. Such interventions have been described in the literature, where pharmacists have billed for targeted medication reviews to offset direct costs associated with the clinical intervention [21,37]. Further, pharmacists have demonstrated success in billing for contraception prescribing in multiple U.S. states [34]. In the case of contraception prescribing, pharmacist fees for service are consistently less than the charge for a physician office visit, which may demonstrate a cost savings. In addition, the increased accessibility of the community pharmacy, frequently offering operating hours longer into the evening and weekend than a traditional physician’s office, may result in fewer absences from work. Convenience may be further improved by offering the visit and dispensing of the contraception product in one location, as compared to the patient needing to travel to the physician’s office and then separately to the pharmacy. Therefore, we believe there to be value to the health care system and its patients when pharmacists are involved not only in contraception provision, but also in broader interventions to support maternal health.
5. Accelerating Action
Successful implementation of maternal health services requires pharmacists to be able to practice at the top of their education and training. This includes prescriptive and immunizing authority, the ability to order and interpret relevant tests, and the authority to make and receive patient referrals. Several states in the U.S. have limited regulatory barriers to the extent that pharmacists can leverage their education and training to more fully engage in providing patient care services [38].
Many of the services included as part of a maternal health service are already within the scope of pharmacist practice in all U.S. states. Medication management services are services that pharmacists routinely provide with most encounters focusing on chronic medical conditions. Patients capable of pregnancy may have chronic medical conditions and some of the medications used to treat those conditions are contraindicated in pregnancy. Pharmacists have the expertise needed to create a treatment plan based on the benefits and risks of medication therapy. In some cases, the patient’s chronic medical condition may present a greater risk to the baby if left untreated. Pharmacists can collaborate with the prescriber to tailor the medication regimen to minimize the risk to both mother and child.
At the time of this writing, 21 U.S. jurisdictions have passed statutes or implemented regulations that allow pharmacists to prescribe contraceptives: Arizona, Arkansas, California, Colorado, Delaware, District of Columbia, Hawaii, Idaho, Illinois, Maryland, Minnesota, Nevada, New Hampshire, New Mexico, North Carolina, Oregon, South Carolina, Utah, Vermont, Virginia, and West Virginia [39]. Additionally, several states have broad collaborative practice authority allowing pharmacists to prescribe contraceptives under a collaborative practice agreement with another provider [40].
Approximately 5% of pregnant women use one or more addictive substances, which include alcohol, tobacco and illicit drugs. The use of one of these substances is associated with at least a two times higher incidence of stillbirth [41]. Use of these substances during pregnancy can also lead to preterm birth, low birthweight, birth defects, small head circumference, neonatal abstinence syndrome (NAS), or sudden infant death syndrome (SIDS). Substance use is the leading cause of maternal death in the U.S. Pharmacists are well-trained to provide smoking cessation counseling and education, and in several U.S. states are able to prescribe smoking cessation therapies [42]. In a study including over 1400 participants, researchers showed that pharmacist-provided smoking cessation interventions have quit rates on par with other healthcare professionals [43]. Support to treat addiction represents yet another way that pharmacists can simultaneously support the health of the patient and a potential pregnancy should the patient choose to become pregnant.
While pharmacists in many states in the U.S. are seeing their scope of practice broaden to be able to address such clinical needs, the requisite reimbursement for services may be lacking. Studies have shown barriers to the development of new clinical services in community pharmacies include lack of reimbursement and access to patient medical records as well as workflow and time constraints [44,45,46,47]. Ensuring reimbursement for services provided may help to alleviate challenges related to workflow and time, as it may allow for hiring of additional staff and defraying of other related costs. Demonstration projects have shown that when incentivized, community pharmacists incorporate interventions related to maternal health into their patient care activities [21,37]. Another example of the driver reimbursement can be in the development of such services is the comparison of the availability of pharmacist-prescribed contraception based on statewide policies regarding reimbursement [48,49,50]. Therefore, addressing such barriers as adequate reimbursement for cognitive services and incorporating community pharmacies in health information exchanges are key factors to fully accelerate implementation of provision of maternal health services in community pharmacies [50,51].
6. Priorities and the Patient’s Perspective
Different issues may be prioritized at the patient level, such as cost, accessibility, and convenience. Specific to cost, pharmacists may be an affordable source of women’s and maternal health care services. Even though most payers still need to reimburse pharmacists for these services, patients may find out-of-pocket costs for pharmacy services affordable, especially if they have high-deductible plans. As mentioned above, if fees for a patient appointment in a pharmacy are less than similar fees charged by a physician’s office, there is potential for patient-focused cost savings in addition to overall health care cost savings. For instance, concern exists that patients with high deductible health plans and low health literacy may forego preventive and non-preventive health services [52]. If a patient on a high deductible or similar health insurance plan is required to pay for the full cost of the visit, the patient may be highly supportive of a less costly visit with a pharmacist. Additional research suggests that patients on high deductible health plans experience a lower birth rate, but not a significant change in contraception rates [53]. Further research may help to clarify demographics or populations that may find personal economic or other benefits from pharmacist-provided contraception services.
As pharmacists frequently counsel patients about medications, they are also well suited to provide needed counseling for reproductive-age patients. For example, a recent analysis of data collected from women who had a live birth found that less than half with pre-pregnancy diabetes and/or hypertension received recommended counseling prior to conception [54]. Pharmacists can tailor their counseling practices based on patient-specific factors and adapt language according to each patient’s needs. A patient’s receptiveness to needed services may vary based on whether the patient is considering pregnancy in the near future (“contemplator”) or not (“non-contemplator”). For non-contemplators, suggested interventions should be framed as beneficial for their overall health. For those contemplating a pregnancy, emphasizing the benefits of the suggested intervention for pregnancy and infant outcomes may resonate more than with a non-contemplator [55].
Furthermore, there is a need to raise awareness among patients and the general public that that community pharmacists are able and capable to provide maternal health services. One study showed that while over 90% of female patients surveyed at two independent pharmacies had a need for at least one pharmacist-provided preconception health service, only 56% were interested in learning more about such services provided at the community pharmacy and 19% were interested to make an appointment with the pharmacist [56]. Another study showed that less than a third of patients in a state where pharmacists can prescribe hormonal contraception were aware of the option [57]. Community pharmacists must do more to publicize the availability and importance of maternal health services.
7. Conclusions
Pharmacists are well-positioned to provide many of the services needed to close the gaps in maternal health care, including but not limited to the prescribing and provision of contraception. The convenience and accessibility of pharmacist-provided services can reduce barriers to care for many individuals. While some studies are available that show the positive impact of pharmacists on specific elements of maternal health care, future studies are needed to show their impact on a more comprehensive suite of maternal health services. Riding on the momentum of recent work to advance contraception prescribing by pharmacists, pilot programs could be conducted to determine the return on investment for pharmacist-provided maternal health services and used to advocate for compensation for these services. Expansion of such services will be essential to ensuring access to care for patients already being served by community pharmacists. We call upon community pharmacists to drive service implementation and expansion to provide proactive maternal health care.
Author Contributions
Writing—original draft preparation, D.B., N.D.M. and A.J.S.; writing—review and editing, D.B., N.D.M. and A.J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors appreciate the permission from the National Alliance of State Pharmacy Associations to reprint Figure 1.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Noursi, S.; Clayton, J.A.; Bianchi, D.W.; Fink, D. Maternal Morbidity and Mortality. J. Womens Health 2021, 30, 145–146. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Improve Maternal Health. Available online: https://www.hhs.gov/sites/default/files/call-to-action-maternal-health.pdf (accessed on 30 August 2022).
- Tikkanen, R.; Fields, K. Multinational Comparisons of Health Systems Data 2020. The Commonwealth Fund. Available online: https://www.commonwealthfund.org/publications/other-publication/2021/feb/multinational-comparisons-health-systems-data-2020 (accessed on 30 August 2022).
- Guttmacher Institute. Unintended Pregnancy in the United States. Available online: https://www.guttmacher.org/fact-sheet/unintended-pregnancy-united-states (accessed on 30 August 2022).
- America’s Health Rankings. Adequate Prenatal Care. Available online: https://www.americashealthrankings.org/explore/health-of-women-and-children/measure/prenatalcare_adquate/state/ALL (accessed on 2 November 2022).
- Crear-Perry, J.; Correa-de-Araujo, R.; Lewis Johnson, T.; McLemore, M.R.; Neilson, E.; Wallace, M. Social and Structural Determinants of Health Inequities in Maternal Health. J. Womens Health 2021, 30, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Kaiser Family Foundation. Women’s Health Insurance Coverage. Available online: https://www.kff.org/womens-health-policy/fact-sheet/womens-health-insurance-coverage/ (accessed on 2 November 2022).
- National Alliance of State Pharmacy Associations. Maternal Health Service Set for Pharmacists. Available online: https://naspa.us/resource/maternal-health-service-set-for-pharmacists/ (accessed on 30 August 2022).
- World Health Organization. Women and Health: Today’s Evidence, Tomorrow’s Agenda. Available online: https://apps.who.int/iris/bitstream/handle/10665/44168/9789241563857_eng.pdf?sequence=1 (accessed on 30 August 2022).
- Daniel, H.; Erickson, S.M.; Bornstein, S.S. Women’s Health Policy in the United States. Ann. Intern. Med. 2019, 170, 281–282. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstet. Gynecol. 2019, 133, e78–e89. [Google Scholar] [CrossRef]
- Berenbrok, L.A.; Tang, S.; Gabriel, N.; Guo, J.; Sharareh, N.; Patel, N.; Dickson, S.; Hernandez, I. Access to community pharmacies: A nationwide geographic information systems cross-sectional analysis. J. Am. Pharm. Assoc. 2022, 62, 1816–1822. [Google Scholar] [CrossRef]
- Berenbrok, L.A.; Gabriel, N.; Coley, K.C.; Hernandez, I. Evaluation of Frequency of Encounters with Primary Care Physicians vs Visits to Community Pharmacies among Medicare Beneficiaries. JAMA Netw. Open 2020, 3, e209132. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, F. Going beyond dispensing: The future of pharmacist roles. Drug Topics 2020, 164, 10–12. Available online: https://www.drugtopics.com/view/going-beyond-dispensing-future-pharmacist-roles (accessed on 30 August 2022).
- Giberson, S.; Yoder, S.; Lee, M.P. Improving Patient and Health System Outcomes through Advanced Pharmacy Practice: A Report to the U.S. Surgeon General. Office of the Chief Pharmacist, U.S. Public Health Service. Available online: https://www.accp.com/docs/positions/misc/improving_patient_and_health_system_outcomes.pdf (accessed on 30 August 2022).
- Jain, S.H. Can Pharmacists Help Reinvent Primary Care in the United States? Forbes. Available online: https://www.forbes.com/sites/sachinjain/2018/10/10/can-pharmacists-help-reinvent-primary-care-in-the-united-states/#2307a69f590b (accessed on 30 August 2022).
- Azeez, O.; Kulkarni, A.; Kuklina, E.V.; Kim, S.Y.; Cox, S. Hypertension and diabetes in non-pregnant women of reproductive age in the United States. Prev. Chronic. Dis. 2019, 16, E146. [Google Scholar] [CrossRef] [PubMed]
- WPSI Recommendations for Well-Woman Care: Clinical Summary Tables; ACOG Foundation: Washington, DC, USA, 2022; Available online: https://www.womenspreventivehealth.org/wp-content/uploads/FINAL_WPSI_WWC_11x17_2022Update-1.pdf (accessed on 30 August 2022).
- Women’s Preventive Services Institute. Recommendations. Available online: https://www.womenspreventivehealth.org/recommendations/ (accessed on 30 August 2022).
- Centers for Disease Control and Prevention. Before Pregnancy. Available online: https://www.cdc.gov/preconception/index.html (accessed on 2 November 2022).
- Bright, D.R.; DiPietro Mager, N.A. Preconception care and contraception services: Opportunities for community pharmacists. J. Am. Coll. Clin. Pharm. 2019, 2, 414–422. [Google Scholar] [CrossRef]
- Klepser, M.; Adams, A.J.; Klepser, D. Clinical service implementation in the face of initial regulatory uncertainty. J. Am. Pharm. Assoc. 2016, 56, 492. [Google Scholar] [CrossRef]
- Kondic, A.M.S.; Trygstad, T.; McDonough, R.; Osterhaus, M. Scaling Community pharmacy transformation with the ‘Flip the Pharmacy’ implementation model: Program origins. Innov. Pharm. 2020, 11. [Google Scholar] [CrossRef]
- Hake, K.L.; Carroll, J.C.; Somma McGivney, M.A.; Coley, K.C. Pharmacist peer coaching in a traditional community chain pharmacy: Implementation and perceptions. J. Am. Pharm. Assoc. 2021, 61, S85–S90. [Google Scholar] [CrossRef] [PubMed]
- North Carolina Association of Pharmacists. A Toolkit for Establishing Clinical Pharmacy Services: The Feasibility, Implementation, Performance and Sustainability Assessments. Available online: https://ncap.memberclicks.net/assets/docs/NCAP%20Toolkit_FINAL_4May2021.pdf (accessed on 2 November 2022).
- McDonough, M. Writing a Business Plan for a New Pharmacy Service. Available online: https://aphanet.pharmacist.com/sites/default/files/files/mtm_writing_business_plan.pdf (accessed on 2 November 2022).
- DiPietro Mager, N.A. Expanding pharmacy services to support public health. Innov. Pharm. 2021, 12, 141. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Creating Community-Clinical Linkages between Community Pharmacists and Physicians. Available online: https://www.cdc.gov/dhdsp/pubs/docs/ccl-pharmacy-guide.pdf (accessed on 2 November 2022).
- Centers for Disease Control and Prevention. Collaborative Practice Agreements and Pharmacists’ Patient Care Services. Available online: https://www.cdc.gov/dhdsp/pubs/docs/Translational_Tools_Pharmacists.pdf (accessed on 2 November 2022).
- DiPietro Mager, N.A.; Bright, D.R.; Murphy, B.L.; Rondon-Begazo, A.; Kelling, S.E. Opportunities for pharmacists and student pharmacists to provide clinical preventive services. Innov. Pharm. 2017, 8, 11. [Google Scholar] [CrossRef]
- Kiles, T.M.; Borja-Hart, N.; Wofford, B.R.; Renfro, C.P. Screening for social determinants of health in community pharmacy: Identifying best practices, barriers, and strategies for success. J. Am. Pharm. Assoc. 2021, 61, e59–e63. [Google Scholar] [CrossRef]
- Grosse, S.D.; Sotnikov, S.V.; Leatherman, S.; Curtis, M. The business case for preconception care: Methods and issues. Matern. Child Health J. 2006, 10, S93–S99. [Google Scholar] [CrossRef]
- Banke-Thomas, A.; Madaj, B.; Kumar, S.; Ameh, C.; van den Broek, N. Assessing value-for-money in maternal and newborn health. BMJ Glob. Health 2017, 2, e000310. [Google Scholar] [CrossRef]
- Mitchell, M.; Stauffenberg, C.; Vernon, V.; Mospan, C.M.; Shipman, A.J.; Rafie, S. Opposition to pharmacist contraception services: Evidence for rebuttal. Pharmacy 2020, 8, 176. [Google Scholar] [CrossRef]
- Rodriguez, M.I.; Hersh, A.; Anderson, L.B.; Harting, D.M.; Edelman, A.B. Association of pharmacist prescription of hormonal contraception with unintended pregnancies and Medicaid costs. Obstet. Gynecol. 2019, 133, 1238–1246. [Google Scholar] [CrossRef]
- Picardo, C.; Ferreri, S. Pharmacist-administered subcutaneous depot medroxyprogesterone acetate: A pilot randomized controlled trial. Contraception 2010, 82, 160–167. [Google Scholar] [CrossRef]
- DiPietro Mager, N.A.; Bright, D.R.; Markus, D.; Weis, L.; Hartzell, D.M.; Gartner, J. Use of targeted medication reviews to deliver preconception care: A demonstration project. J. Am. Pharm. Assoc. 2017, 57, 90–94. [Google Scholar] [CrossRef]
- Adams, A.J.; Frost, T.; Weaver, K. Pharmacy Regulatory Innovation Index: Benchmarking the regulatory environment in 10 western states. J. Am. Pharm. Assoc. 2021, 61, e84–e89. [Google Scholar] [CrossRef] [PubMed]
- National Alliance of State Pharmacy Associations. Pharmacist Prescribing: Hormonal Contraceptives. Available online: https://naspa.us/resource/contraceptives/ (accessed on 5 September 2022).
- National Alliance of State Pharmacy Associations. Collaborative Practice Agreements: Resources and More. Available online: https://naspa.us/resource/cpa/ (accessed on 30 August 2022).
- National Institute on Drug Abuse. Substance Use in Women: Substance Use while Pregnant and Breastfeeding. Available online: https://www.drugabuse.gov/publications/substance-use-in-women/substance-use-while-pregnant-breastfeeding (accessed on 30 August 2022).
- National Alliance of State Pharmacy Associations. Pharmacist Prescribing: Tobacco Cessation Aids. Available online: https://naspa.us/resource/tobacco-cessation/ (accessed on 30 August 2022).
- Shen, X.; Bachyrycz, A.; Anderson, J.R.; Tinker, D.; Raisch, D.W. Quitting patterns and predictors of success among participants in a tobacco cessation program provided by pharmacists in New Mexico. J. Manag. Care Spec. Pharm. 2014, 20, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Blazejewski, L.; Vaidya, V.; Pinto, S.; Gaither, C. Pharmacists’ perceived barriers providing non-dispensing services to underserved populations. J. Community Health. 2013, 38, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Rafie, S.; Cieri-Hutcherson, N.E.; Frame, T.R.; Griffin, B.; Harris, J.B.; Horlen, C.; Shealy, K.; Stein, A.B.; Stone, R.H.; Vest, K.; et al. Pharmacists’ Perspectives on Prescribing and Expanding Access to Hormonal Contraception in Pharmacies in the United States. J. Pharm. Pract. 2021, 34, 230–238. [Google Scholar] [CrossRef]
- Salgado, T.M.; Rosenthal, M.M.; Coe, A.B.; Kaefer, T.N.; Dixon, D.L.; Farris, K.B. Primary healthcare policy and vision for community pharmacy and pharmacists in the United States. Pharm. Pract. 2020, 18, 2160. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.I.; Herman, A.M.; Espey, E.; Hersh, A.R.; Bachyrycz, A.M. Pharmacists’ perspectives and experience prescribing hormonal contraception in rural and urban New Mexico. J. Am. Pharm. Assoc. 2021, 61, e140–e144. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Hartung, D.M.; Middleton, L.; Rodriguez, M.I. Pharmacist provision of hormonal contraception in the Oregon Medicaid population. Obstet. Gynecol. 2019, 133, 1231–1237. [Google Scholar] [CrossRef]
- Batra, P.; Rafie, S.; Zhang, Z.; Singh, A.V.; Bird, C.E.; Sridhar, A.; Sullivan, J.G. An evaluation of the implementation of pharmacist-prescribed hormonal contraceptives in California. Obstet. Gynecol. 2018, 131, 850–855. [Google Scholar] [CrossRef]
- Facciolo, F.; Farley, J. Minnesota policy on pharmacist-prescribed contraceptives: Benefits, limitations, and opportunities for improvement. Innov. Pharm. 2021, 12. [Google Scholar] [CrossRef]
- Chim, C.; Sharma, P. Pharmacists prescribing hormonal contraceptives: A status update. US Pharm. 2021, 46, 45–49. [Google Scholar]
- Tiirneni, R.; Politi, M.C.; Kullgren, J.T.; Kieffer, E.C.; Goold, S.D.; Scherer, A.M. Association between health insurance literacy and avoidance of health care services owing to cost. JAMA Netw. Open 2018, 1, e184796. [Google Scholar] [CrossRef] [PubMed]
- Graves, A.J.; Kozhimannil, K.B.; Kleinman, K.P.; Wharam, J.F. The association between high-deductible health plan transition and contraception and birth rates. Health Serv. Res. 2016, 51, 187–204. [Google Scholar] [CrossRef] [PubMed]
- Marshall, C.J.; Huma, Z.; Deardorff, J.; Britton, L.E. Prepregnancy counseling among U.S. women with diabetes and hypertension, 2016–2018. Am. J. Prev. Med. 2021, 61, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Prevention and Health Communication Team; National Center on Birth Defects and Developmental Disabilities and Centers for Disease Control and Prevention. Media Campaigns: Implementation Kit. Available online: www.cdc.gov/ncbddd/folicacid/documents/mediacampaignkit.pdf (accessed on 30 August 2022).
- Luli, A.J.; Tran, N.; Ataya, A.; Rafie, S. Patient screenings for preconception health interventions at a community pharmacy. Pharmacy 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.M.; Rafie, S.; Garner-Ford, E.; Arcara, J.; Arteaga, S.; Britter, M.; De La Cruz, M.; Gleaton, S.K.; Gomez-Vidal, C.; Luna, B.; et al. Community perspectives on pharmacist-prescribed hormonal contraception in rural California. Contraception 2022, 114, 10–17. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).