
The Production of the PHAR-QA Competence Framework †

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Background
2.1. Rationale: Why Carry Out the PHAR-QA Project
2.2. The Starting Points: Existing Competence Frameworks
3. Methodology
3.1. Type of Competence
3.2. The Two-Panel Delphi Process: The Small and Large Panels
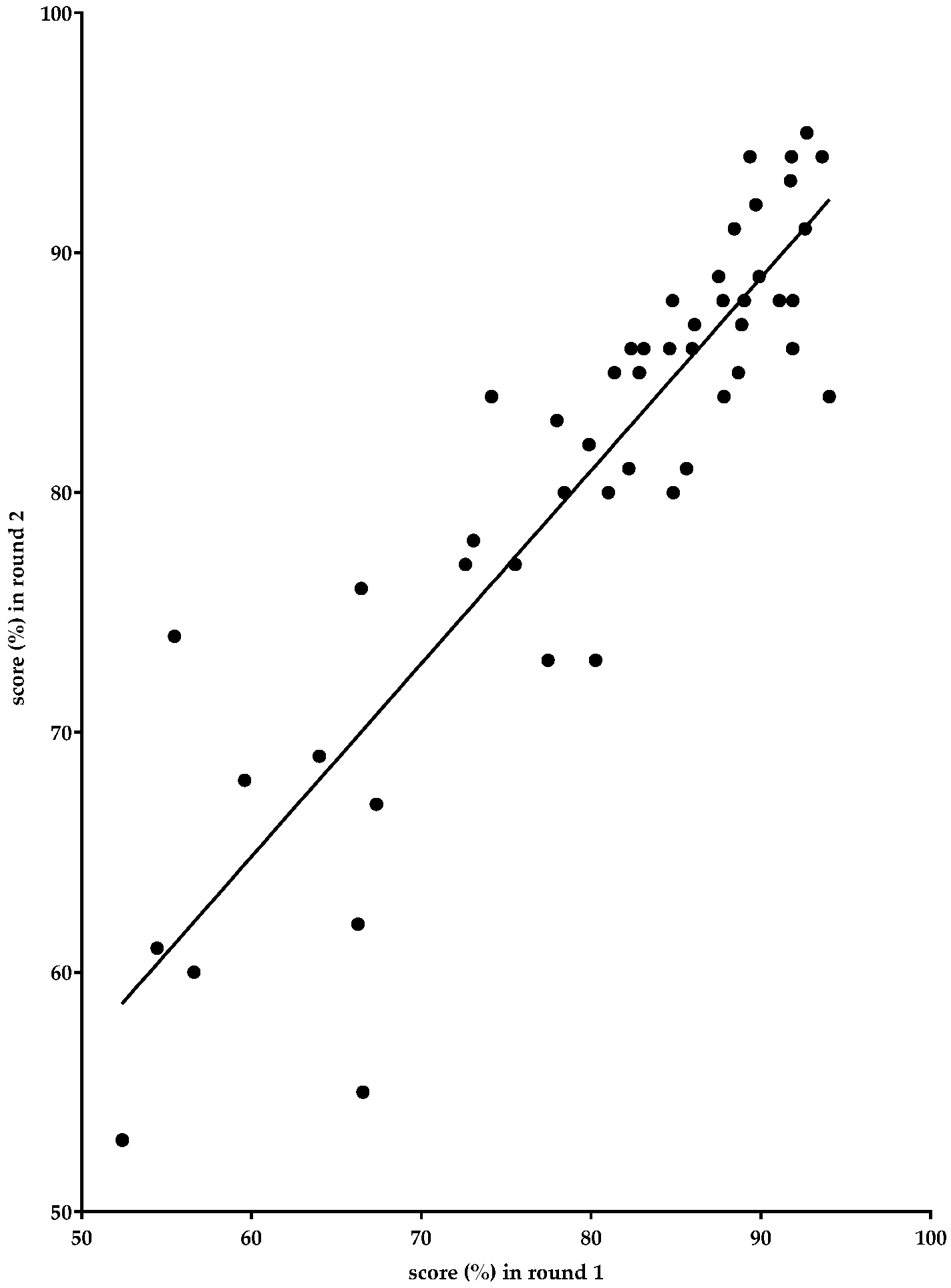
3.3. Iteration versus Anonymity—Implications for the Repeatability of the Results
3.4. Correlations between Results Obtained in the Two Delphi Rounds of the Large Panel
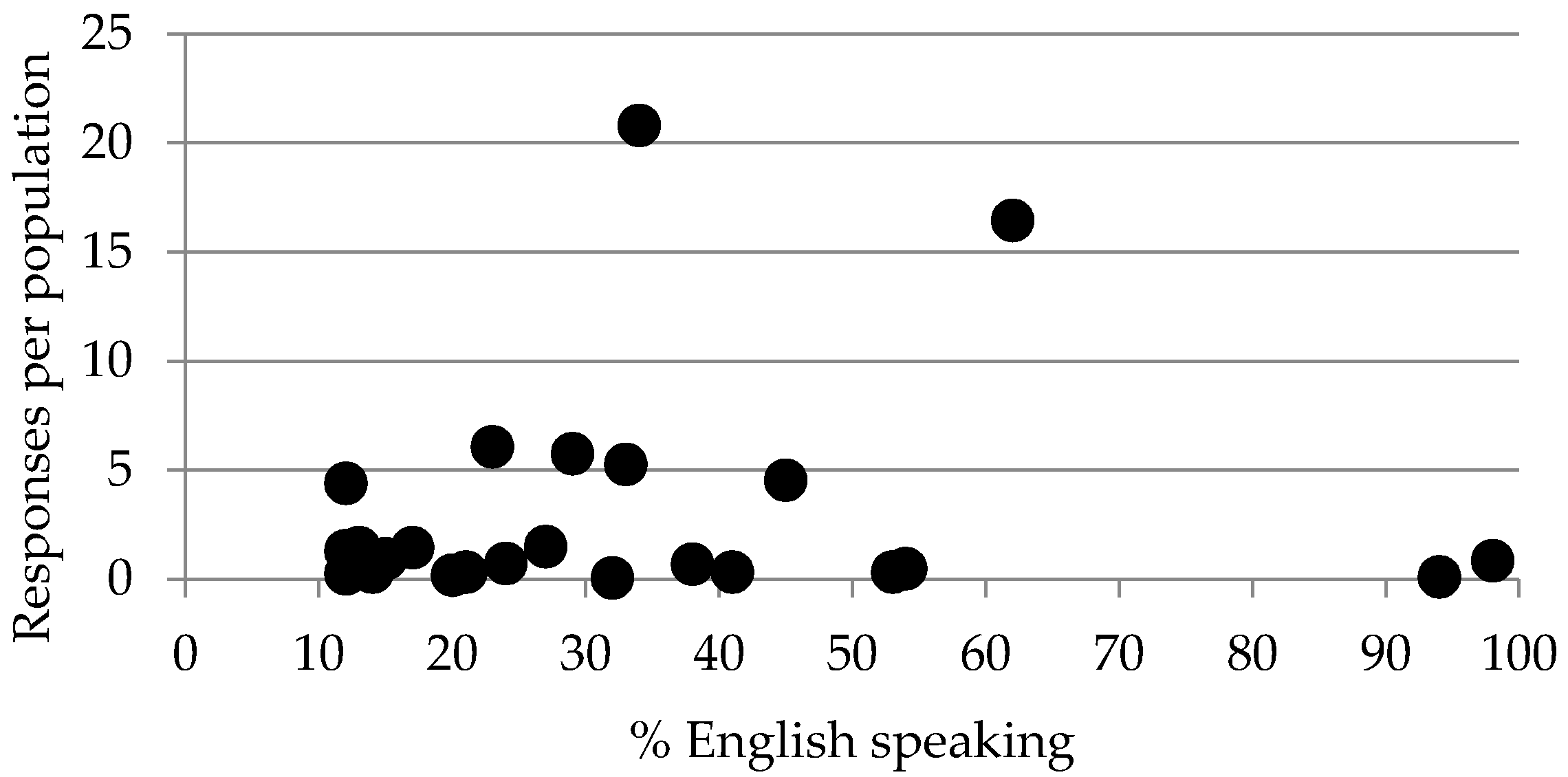
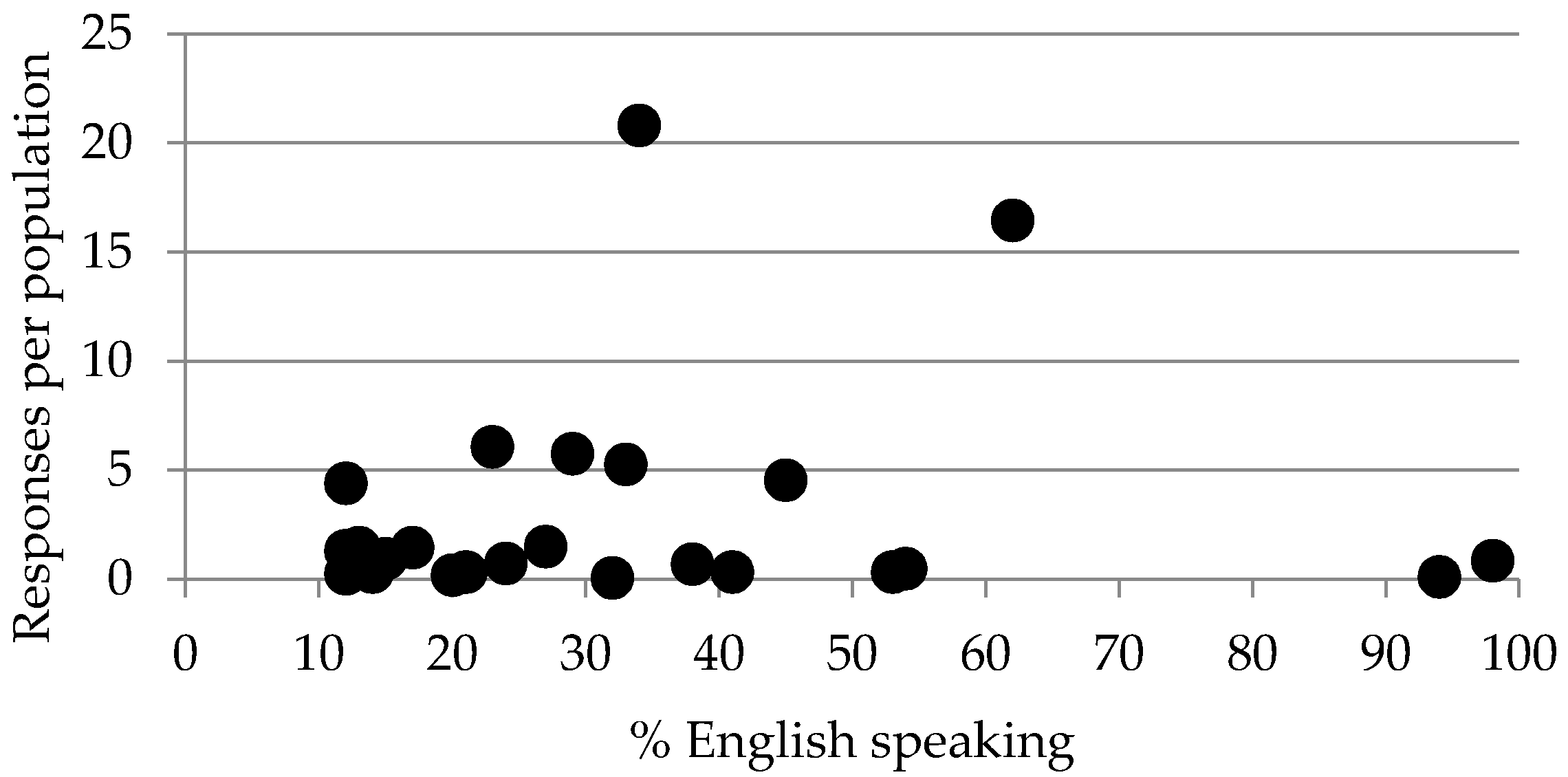
3.5. Biases
4. Conclusions and Perspectives
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PET | pharmacy education and training |
| EU | European Union |
Appendix
- Jeffrey Atkinson, Pharmacology Department, Lorraine University, 5 rue Albert Lebrun, 54000 Nancy, and Pharmacolor Consultants Nancy, 12 rue de Versigny, 54600 Villers, France; [email protected].
- Kristien De Paepe, Pharmacy Faculty, Vrije Universiteit Brussel, Laarbeeklaan 103, Brussels 1090, Belgium; [email protected]. Kristien De Paepe replaced Bartholomew Rombaut who passed away on the 23 January 2014.
- Antonio Sánchez Pozo, Faculty of Pharmacy, University of Granada, Campus Universitario de la Cartuja s/n, Granada 18701, Spain; [email protected].
- Dimitrios Rekkas, School of Pharmacy, National and Kapodistrian University Athens, Panepistimiou 30, Athens 10679, Greece; [email protected].
- Daisy Volmer, Pharmacy Faculty, University of Tartu, Nooruse 1, Tartu 50411, Estonia; [email protected].
- Jouni Hirvonen, Pharmacy Faculty, University of Helsinki, Yliopistonkatu 4, P.O. Box 33-4, Helsinki 00014, Finland; [email protected].
- Borut Bozic, Faculty of Pharmacy, University of Ljubljana, Askerceva cesta 7, Ljubljana 1000, Slovenia; [email protected].
- Agnieska Skowron, Pharmacy Faculty, Jagiellonian University, Golebia 24, Krakow 31-007, Poland; [email protected].
- Constantin Mircioiu, Pharmacy Faculty, University of Medicine and Pharmacy “Carol Davila” Bucharest, Dionisie Lupu 37, Bucharest 020021, Romania; [email protected].
- Annie Marcincal, Faculty of Pharmacy, European Association of Faculties of Pharmacy, Université de Lille 2, Lille 59000, France; [email protected].
- Andries Koster, Department of Pharmaceutical Sciences, European Association of Faculties of Pharmacy, Utrecht University, PO Box 80082, 3508 TB Utrecht, The Netherlands; [email protected].
- Keith Wilson, School of Life and Health Sciences, Aston University, Birmingham B47ET, UK; [email protected].
- Chris van Schravendijk, Medical Faculty, Vrije Universiteit Brussel, Laarbeeklaan 103, 1090 Brussels, Belgium; [email protected].
- Lea Noel, Pharmacy Faculty, Vrije Universiteit Brussel, Laarbeeklaan 103, 1090 Brussels, Belgium; [email protected] (consortial secretary).
- Richard Price, the European Hospital Pharmacists’ Association. Available online: http://www.eahp.eu/ (accessed on13 January 2017).
- Jamie Wilkinson, the Pharmacists’ Group of the European Union. Available online: http://www.pgeu.eu/fr/accueil.html (accessed on13 January 2017).
- Jane Nicholson, European Industrial Pharmacists’ Group. Available online: http://eipg.eu/ (accessed on 13 January 2017).
- The President, European Pharmacy Students’ Association, Available online: http://eafponline.eu/ (accessed on 13 January 2017).
- The President, European Association of Faculties of Pharmacy. Available online: http://eafponline.eu/ (accessed on 13 January 2017).
References
- The PHAR-QA Project. Quality Assurance in European Pharmacy Education and Training. Available online: www.phar-qa.eu (accessed on 13 January 2017).
- Atkinson, J.; de Paepe, K.; Sánchez Pozo, A.; Rekkas, D.; Volmer, D.; Hirvonen, J.; Bozic, B.; Skowron, A.; Mircioiu, C.; Marcincal, A.; et al. The Second Round of the PHAR-QA Survey of Competences for Pharmacy Practice. Pharmacy 2016, 4, 27. [Google Scholar] [CrossRef]
- The PHARMINE (Pharmacy Education in Europe) Consortium. Work Programme 3: Final Report Identifying and Defining Competences for Pharmacists. Available online: http://www.pharmine.org/wp-content/uploads/2014/05/PHARMINE-WP3-Final-ReportDEF_LO.pdf (accessed on 13 January 2017).
- Atkinson, J. Heterogeneity of Pharmacy Education in Europe. Pharmacy 2014, 2, 231–243. [Google Scholar] [CrossRef]
- Bourlioux, P. Second European Meeting of the Faculties, Schools and Institutes of Pharmacy, Berlin, Germany, 27–28 September 1994.
- The EU Directive 2013/55/EU on the Recognition of Professional Qualifications. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2005:255:0022:0142:EN:PDF (accessed on 13 January 2017).
- The EU Directive 2011/24/EU on Patients' Rights in Cross-border Healthcare. Available online: http://ec.europa.eu/health/cross_border_care/towards_legislative_framework/index_en.htm (accessed on 13 January 2017).
- Atkinson, J.; Rombaut, B.; Sánchez Pozo, A.; Rekkas, D.; Veski, P.; Hirvonen, J.; Bozic, B.; Skowron, A.; Mircioiu, C.; Marcincal, A.; et al. Systems for Quality Assurance in Pharmacy Education and Training in the European Union. Pharmacy 2014, 2, 17–26. [Google Scholar] [CrossRef]
- Miller, G.E. The assessment of clinical skills/competences/performance. Acad. Med. 1990, 65, 63–67. [Google Scholar] [CrossRef]
- MEDINE: Medical Education in Europe. MEDINE Is Concerned with the Mobility of Medical Students and Practitioners, the Standards and Content of Medical Education Programmes, the Transparency and Comparability of Qualifications, the Application of the Bologna Principles to Medical Education, and the Application of Medical Research to Education. Available online: http://medine2.com/Public/about.html (accessed on 13 January 2017).
- Europeans and Their Languages. “Special Eurobarometer 386” of the European Commission (2012). Available online: ec.europa.eu/public_opinion/archives/ebs/ebs_386_en.pdf (accessed on 13 January 2017).

© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atkinson, J. The Production of the PHAR-QA Competence Framework. Pharmacy 2017, 5, 19. https://doi.org/10.3390/pharmacy5020019
Atkinson J. The Production of the PHAR-QA Competence Framework. Pharmacy. 2017; 5(2):19. https://doi.org/10.3390/pharmacy5020019
Chicago/Turabian StyleAtkinson, Jeffrey. 2017. "The Production of the PHAR-QA Competence Framework" Pharmacy 5, no. 2: 19. https://doi.org/10.3390/pharmacy5020019
APA StyleAtkinson, J. (2017). The Production of the PHAR-QA Competence Framework. Pharmacy, 5(2), 19. https://doi.org/10.3390/pharmacy5020019