Learning from Mistakes—Dental Students’ Learning Experiences from Adverse Clinical Events

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
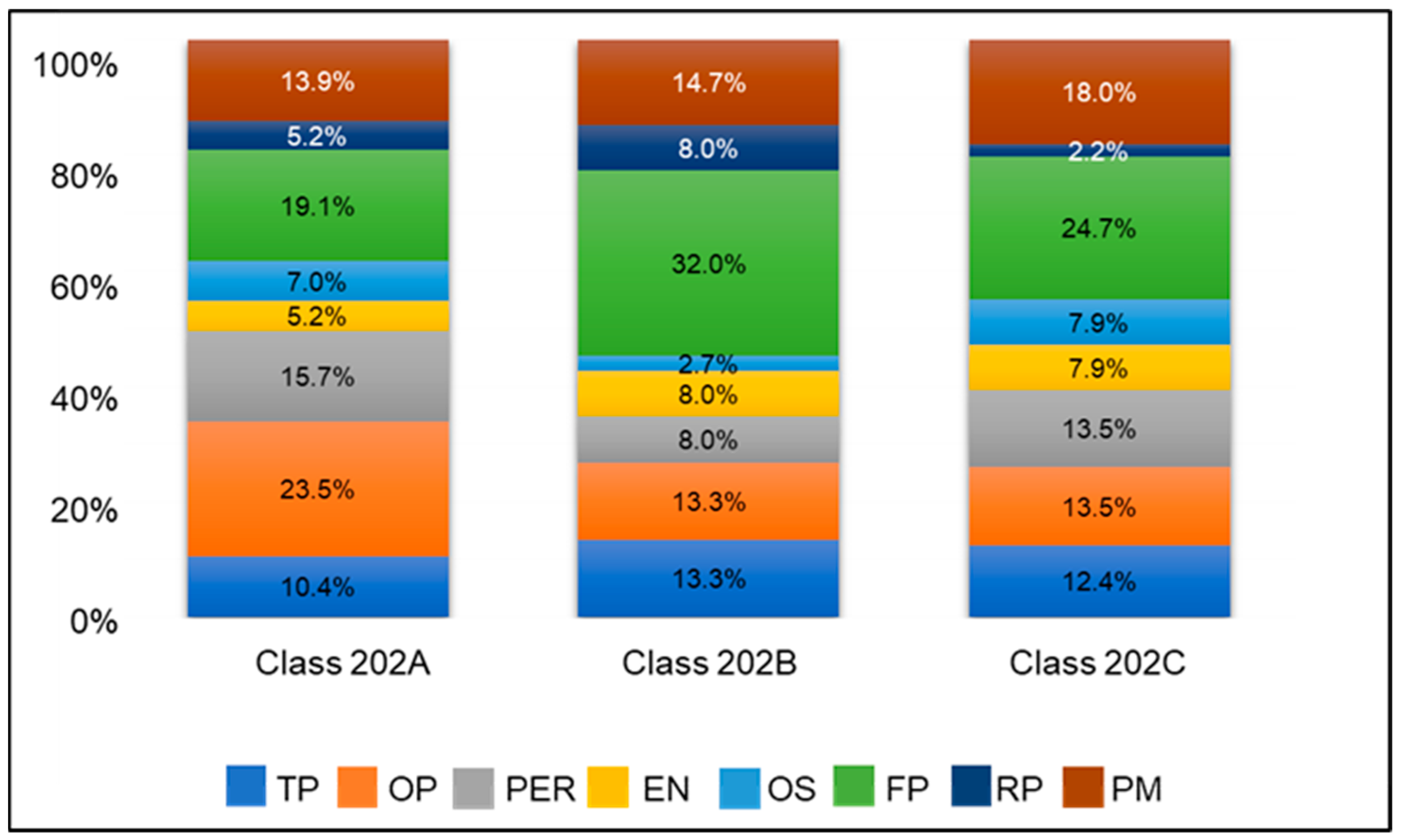
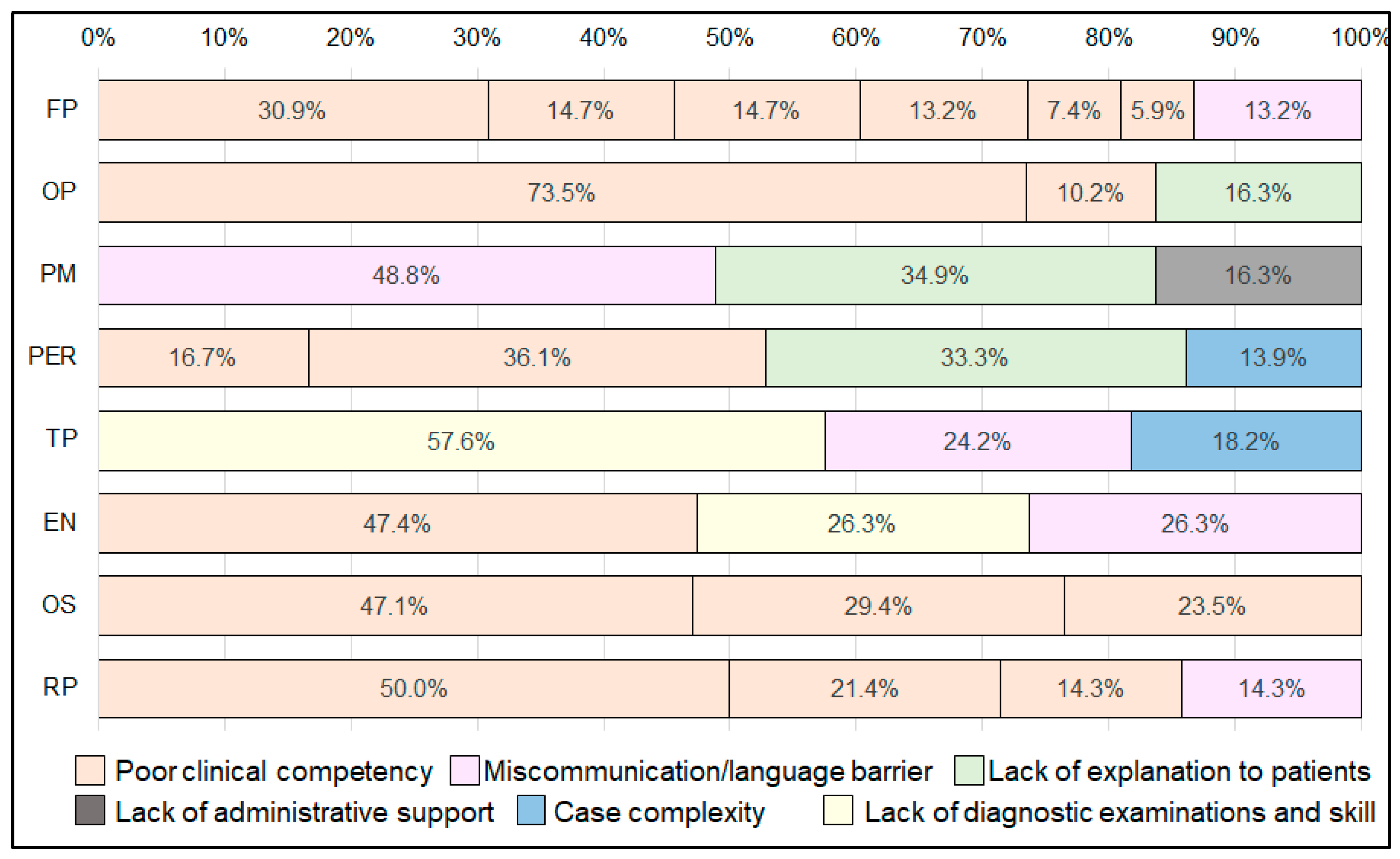
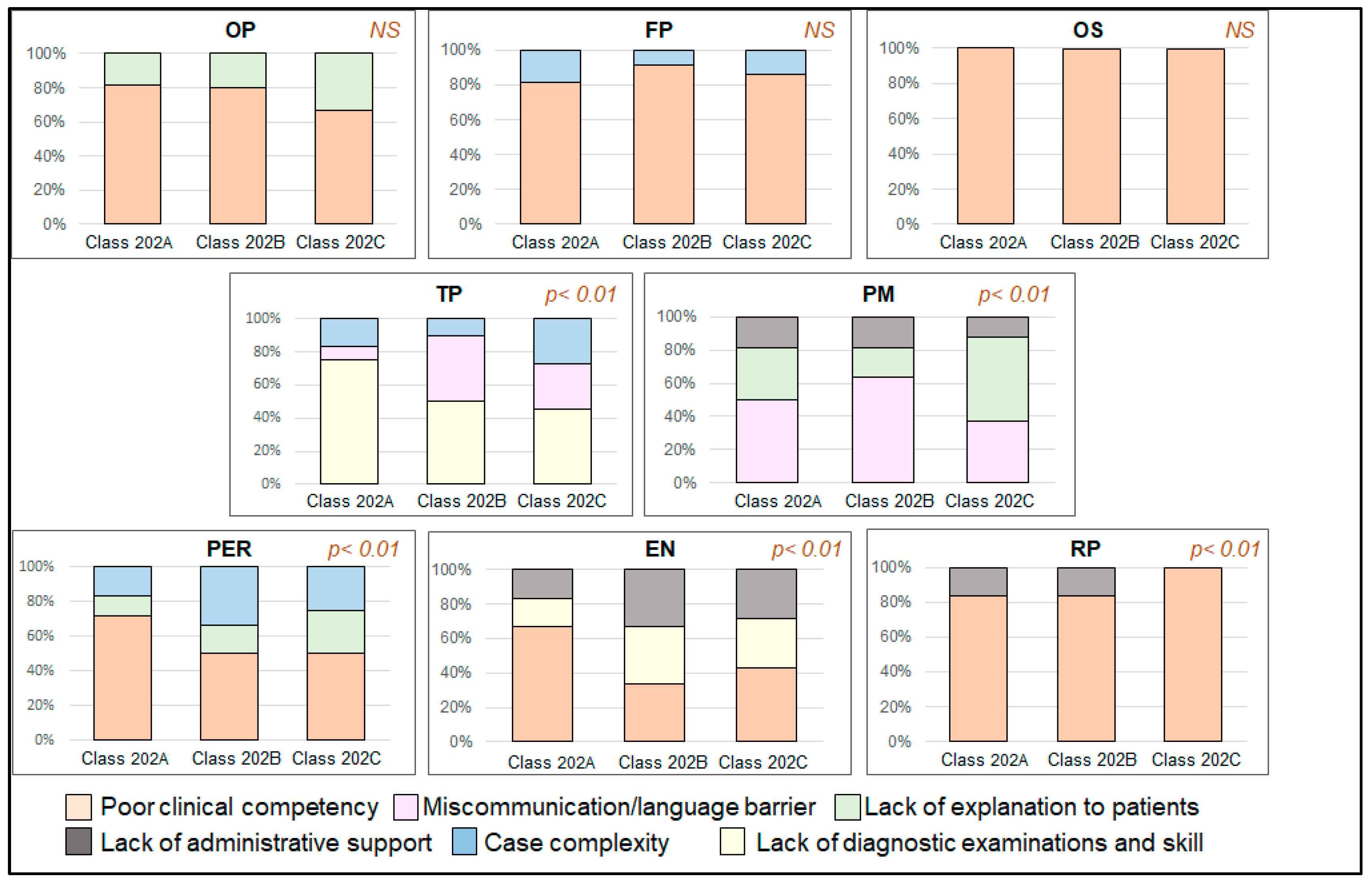
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ADEA Commission on Change and Innovation in Dental Education; Haden, N.K.; Andrieu, S.C.; Chadwick, D.G.; Chmar, J.E.; Cole, J.R.; George, M.C.; Glickman, G.N.; Glover, J.F.; Goldberg, J.S.; et al. The dental education environment. J. Dent. Educ. 2006, 70, 1265–1270. [Google Scholar]
- Serrano, C.M.; Lagerweij, M.D.; de Boer, I.R.; Bakker, D.R.; Koopman, P.; Wesselink, P.R.; Vervoorn, J.M. Students’ learning environment perception and the transition to clinical training in dentistry. Eur. J. Dent. Educ. 2021, 25, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, A.A.; El Tantawi, M.M.A. Predicting academic performance of dental students using perception of educational environment. J. Dent. Educ. 2015, 79, 337–344. [Google Scholar] [CrossRef]
- Subramanian, J.; Anderson, V.; Morgaine, K.; Thomson, W. The importance of ‘student voice’ in dental education. Eur. J. Dent. Educ. 2013, 17, e136–e141. [Google Scholar] [CrossRef]
- Henzi, D.; Davis, E.; Jasinevicius, R.; Hendricson, W.; Cintron, L.; Isaacs, M. Appraisal of the dental school learning environment: The students’ view. J. Dent. Educ. 2005, 69, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Schonwetter, D.J.; Lavigne, S.; Mazurat, R.; Nazarko, O. Students’ perceptions of effective classroom and clinical teaching in dental and dental hygiene education. J. Dent. Educ. 2006, 70, 624–635. [Google Scholar] [CrossRef]
- Divaris, K.; Barlow, P.J.; Chendea, S.A.; Cheong, W.S.; Dounis, A.; Dragan, I.F.; Hamlin, J.; Hosseinzadeh, L.; Kuin, D.; Mitrirattanakul, S.; et al. The academic environment: The students’ perspective. Eur. J. Dent. Educ. 2008, 12, 120–130. [Google Scholar] [CrossRef]
- Howell, T.H.; Matlin, K. Damn the torpedoes—Innovations for the future: The new curriculum at the Harvard School of Dental Medicine. J. Dent. Educ. 1995, 59, 893–898. [Google Scholar] [CrossRef]
- Holmes, D.C.; Boston, D.W.; Budenz, A.W.; Licari, F.W. Predoctoral clinical curriculum models at U.S. and Canadian dental schools. J. Dent. Educ. 2003, 67, 1302–1311. [Google Scholar] [CrossRef]
- Holmes, D.C.; Trombly, R.M.; Garcia, L.T.; Kluender, R.L.; Keith, C.R. Student productivity in a comprehensive care program without numeric requirements. J. Dent. Educ. 2000, 64, 745–754. [Google Scholar] [CrossRef]
- Evangelidis-Sakellson, V. Student productivity under requirement and comprehensive care system. J. Dent. Educ. 1999, 63, 407–413. [Google Scholar] [CrossRef]
- Park, S.E.; Timothé, P.; Nalliah, R.; Karimbux, N.Y.; Howell, T.H. A case completion curriculum for clinical dental education: Replacing numerical requirements with patient-based comprehensive care. J. Dent. Educ. 2011, 75, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Susarla, H.K.; Nalliah, R.; Timothé, P.; Howell, T.H.; Karimbux, N.Y. Does a Case Completion Curriculum Influence Dental Students’ Clinical Productivity? J. Dent. Educ. 2012, 76, 602–608. [Google Scholar] [CrossRef]
- Park, S.E.; Howell, T.H. Implementation of a patient-centered approach to clinical dental education: A five-year reflection. J. Dent. Educ. 2015, 79, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E. Ten-year follow-up of patient-centered comprehensive care using case completion curriculum. J. Dent. Educ. 2021, 85, 1408–1414. [Google Scholar] [CrossRef] [PubMed]
- NHS Patient Safety. 2011. Available online: http://www.nrls.npsa.nhs.uk/report-a-patient-safety-incident/ (accessed on 13 July 2014).
- Brennan, T.A.; Leape, L.L.; Laird, N.M.; Hebert, L.; Localio, A.R.; Lawthers, A.G.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H.H. Incidence of adverse events and negligence in hospitalized patients: Results of the Harvard Medical Practice Study I. N. Engl. J. Med. 1991, 324, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.J.; Studdert, D.M.; Burstin, H.R.; Orav, E.J.; Zeena, T.; Williams, E.J.; Howard, K.M.; Weiler, P.C.; Brennan, T.A. Incidence and types of adverse events and negligent care in Utah and Colorado. Med. Care 2000, 38, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.M.; Runciman, W.B.; Gibberd, R.W.; Harrison, B.T.; Newby, L.; Hamilton, J.D. The Quality in Australian Health Care Study. Med. J. Aust. 1995, 163, 458–471. [Google Scholar] [CrossRef] [PubMed]
- Vincent, C.; Neale, G.; Woloshynowych, M. Adverse events in British hospitals: Preliminary retrospective record review. Br. Med. J. 2001, 322, 517–519. [Google Scholar] [CrossRef]
- Davis, P.; Lay-Yee, R.; Briant, R.; Ali, W.; Scott, A.; Schug, S. Adverse events in New Zealand public hospitals I: Occurrence and impact. N. Z. Med. J. 2002, 115, U271. [Google Scholar]
- Baker, G.R.; Norton, P.G.; Flintoff, V.; Blais, R.; Brown, A.; Cox, J.; Etchells, E.; Ghali, W.A.; Hébert, P.; Majumdar, S.R.; et al. The Canadian Adverse Events Study: The incidence of adverse events among hospital patients in Canada. J. Can. Med. Assoc. 2004, 170, 1678–1686. [Google Scholar] [CrossRef]
- Miguel Hernandez University; Ministry of Health and Consumer Affairs. National Study on Hospitalisation-Related Adverse Events ENEAS 2005; Quality Agency Administration National Health System, Ed.; Ministry of Health and Consumer Affairs: Madrid, Spain, 2006. Available online: http://www.who.int/patientsafety/information_centre/reports/ENEAS-EnglishVersion-SPAIN.pdf (accessed on 28 January 2024).
- Soop, M.; Fryksmark, U.; Koster, M.; Haglund, B. The incidence of adverse events in Swedish hospitals: A retrospective medical record review study. Int. J. Qual. Health Care 2009, 21, 285–291. [Google Scholar] [CrossRef]
- Zegers, M.; Bruijne, M.C.d.; Wagner, C.; Hoonhout, L.H.F.; Waaijman, R.; Smits, M.; Hout, F.A.G.; Zwaan, L.; Christiaans-Dingelhoff, I.; Timmermans, D.R.M.; et al. Adverse events and potentially preventable deaths in Dutch hospitals: Results of a retrospective patient record review study. Qual. Saf. Health Care 2009, 18, 297–302. [Google Scholar] [CrossRef]
- Sari, A.B.-A.; Sheldon, T.A.; Cracknell, A.; Turnbull, A.; Dobson, Y.; Grant, C.; Gray, W.; Richardson, A. Extent, nature and consequences of adverse events: Results of a retrospective casenote review in a large NHS hospital. Qual. Saf. Health Care 2007, 16, 434–439. [Google Scholar] [CrossRef]
- Bates, D.W.; O’Neil, A.C.; Petersen, L.A.; Lee, T.H.; Brennan, T.A. Evaluation of screening criteria for adverse events in medical patients. Med. Care 1995, 33, 452–462. [Google Scholar] [CrossRef]
- Fischer, M.A.; Mazor, K.M.; Baril, J.; Alper, E.; DeMarco, D.; Pugnaire, M. Learning from Mistakes. Factors that Influence How Students and Residents Learn from Medical Errors. J. Gen. Intern. Med. 2006, 21, 419–423. [Google Scholar] [CrossRef]
- Kravet, S.J.; Howell, E.; Wright, S.M. Morbidity and Morality Conference, Grand Rounds, and the ACGME’s Core Competencies. J. Gen. Intern. Med. 2006, 21, 1192–1194. [Google Scholar] [CrossRef]
- Ripolles, P.; Marco-Pallares, J.; Alicart, H.; Tempelmann, C.; Rodríguez-Fornells, A.; Noesselt, T. Intrinsic monitoring of learning success facilitates memory encoding via the activation of the SN/VTA-Hippocampal loop. eLife 2016, 5, e17441. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Discipline | Common Areas of Adverse Events | Causes |
|---|---|---|
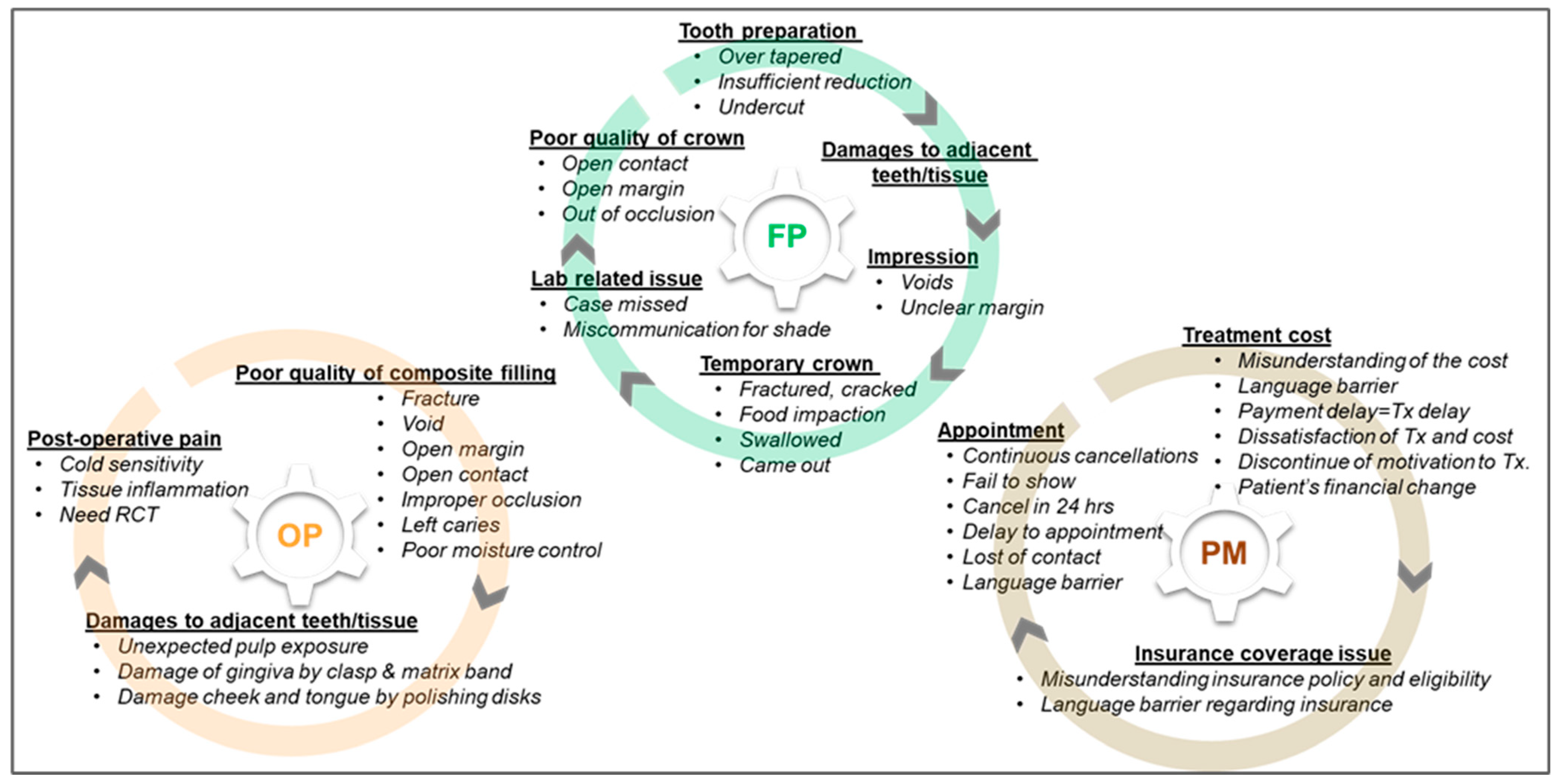
| FP | Temporary crown. Tooth preparation. Impression. Damage to adjacent teeth/tissue. Poor quality of crown. Lab-related issues. | Poor clinical competency in fabricating temporary crown. Poor clinical competency in tooth preparation. Poor clinical competency in capturing bite registrations. Poor clinical competency in material use/instrument control Poor clinical competency in obtaining proper moisture control. Inaccurate shade selection. Miscommunication with dental laboratory. |
| OP | Poor quality of fillings. Post-operative pain. Damage to other tissue. | Poor clinical competency in composite restoration techniques. Poor clinical competency in material use/instrument control. Insufficient explanation. |
| PM | Cancellation of appointment. Treatment costs. Insurance coverage. | Miscommunication (language barrier). Poor patient communication. Lack of administrative support. |
| PER | Surgical procedure. Treatment costs. Damage to other tissue. | Poor clinical techniques. Poor procedural preparation. Lack of administrative support. Case complexity. |
| TP | Diagnosis. Treatment plan comprehension. | Deficient skills in diagnostic examinations. Miscommunication (language barrier). Case complexity. |
| EN | Obturation. Diagnosis. Post-operative pain. Restorative work delays. | Poor clinical techniques. Deficient skills in diagnostic examinations. Miscommunication (language barrier). Poor patient communication. |
| OS | Extraction. Anesthesia. Damage to adjacent tissue/teeth. | Poor clinical competency in anesthesia techniques. Poor clinical competency in extraction techniques. Poor clinical competency in surgical procedures. |
| RP | Occlusion. Post-operative pain. Integrity of dentures. Scheduling issues. | Poor clinical competency in capturing bite registrations. Poor clinical competency in taking impressions. Poor clinical competency in adjustment procedures. Miscommunication (language barrier). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, H.; Valdes, L.; Xie, J.; Ohyama, H.; Tate, I.; Maeno, M.; Shiba, T.; Nagai, S. Learning from Mistakes—Dental Students’ Learning Experiences from Adverse Clinical Events. Educ. Sci. 2024, 14, 416. https://doi.org/10.3390/educsci14040416
Ishikawa H, Valdes L, Xie J, Ohyama H, Tate I, Maeno M, Shiba T, Nagai S. Learning from Mistakes—Dental Students’ Learning Experiences from Adverse Clinical Events. Education Sciences. 2024; 14(4):416. https://doi.org/10.3390/educsci14040416
Chicago/Turabian StyleIshikawa, Hiroshi, Layra Valdes, Juanna Xie, Hiroe Ohyama, Isabel Tate, Masahiko Maeno, Takahiko Shiba, and Shigemi Nagai. 2024. "Learning from Mistakes—Dental Students’ Learning Experiences from Adverse Clinical Events" Education Sciences 14, no. 4: 416. https://doi.org/10.3390/educsci14040416