
The Active Role of the Internet and Social Media Use in Nonpharmaceutical and Pharmaceutical Preventive Measures against COVID-19

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Measures
2.3. Data Analysis
2.4. Sample Attrition
3. Results
3.1. Descriptive Statistics
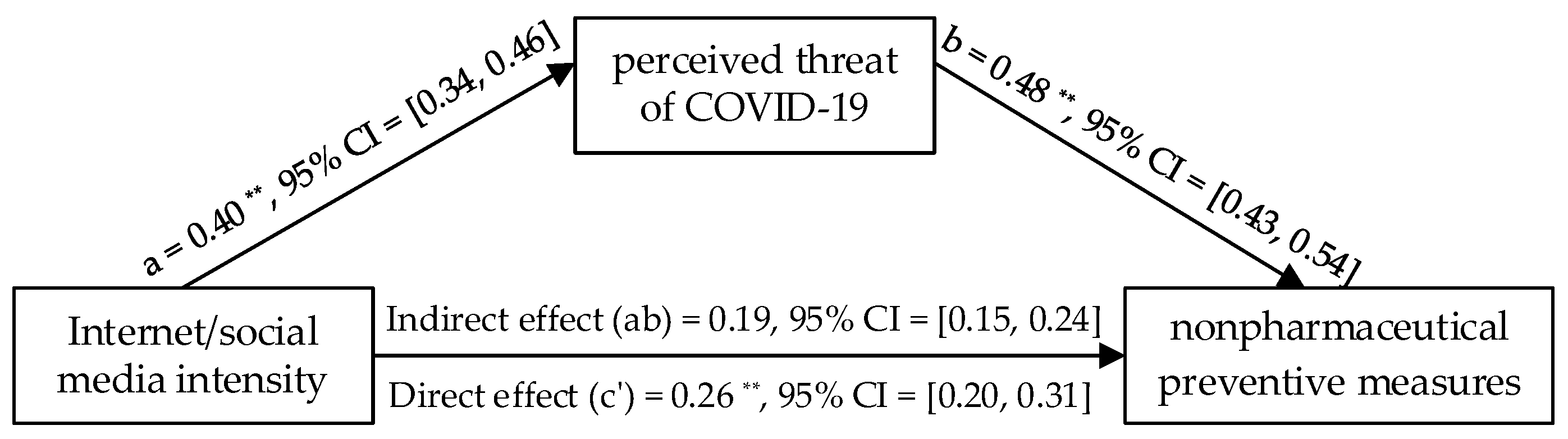
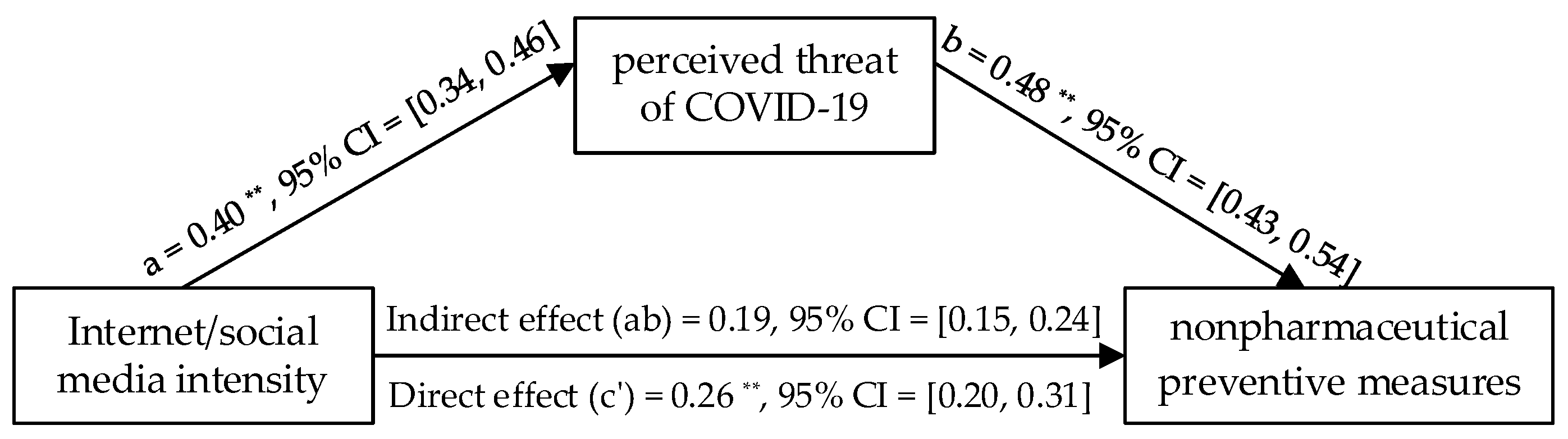
3.2. Mediation Analysis for Nonpharmaceutical Measures by Wave 1 Data
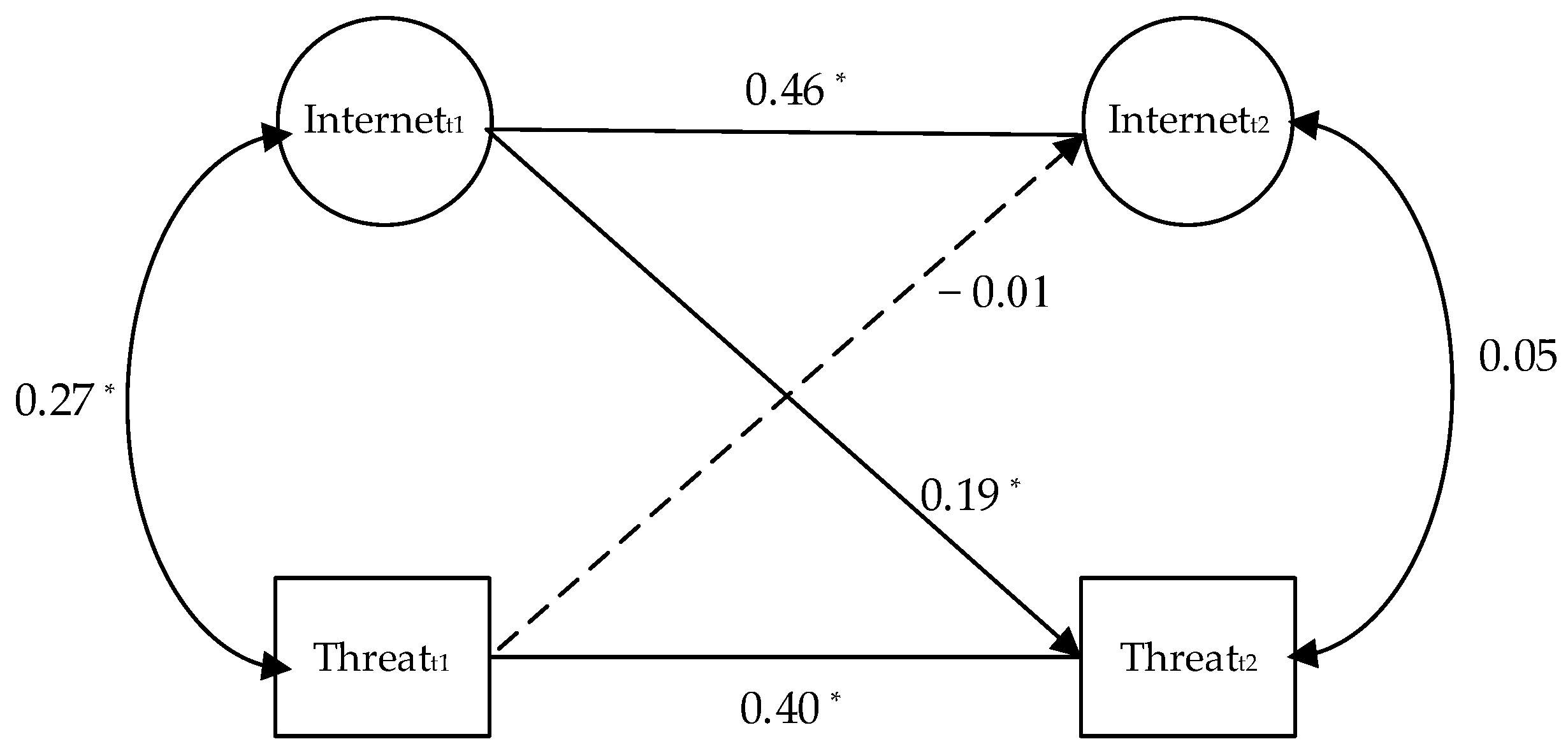
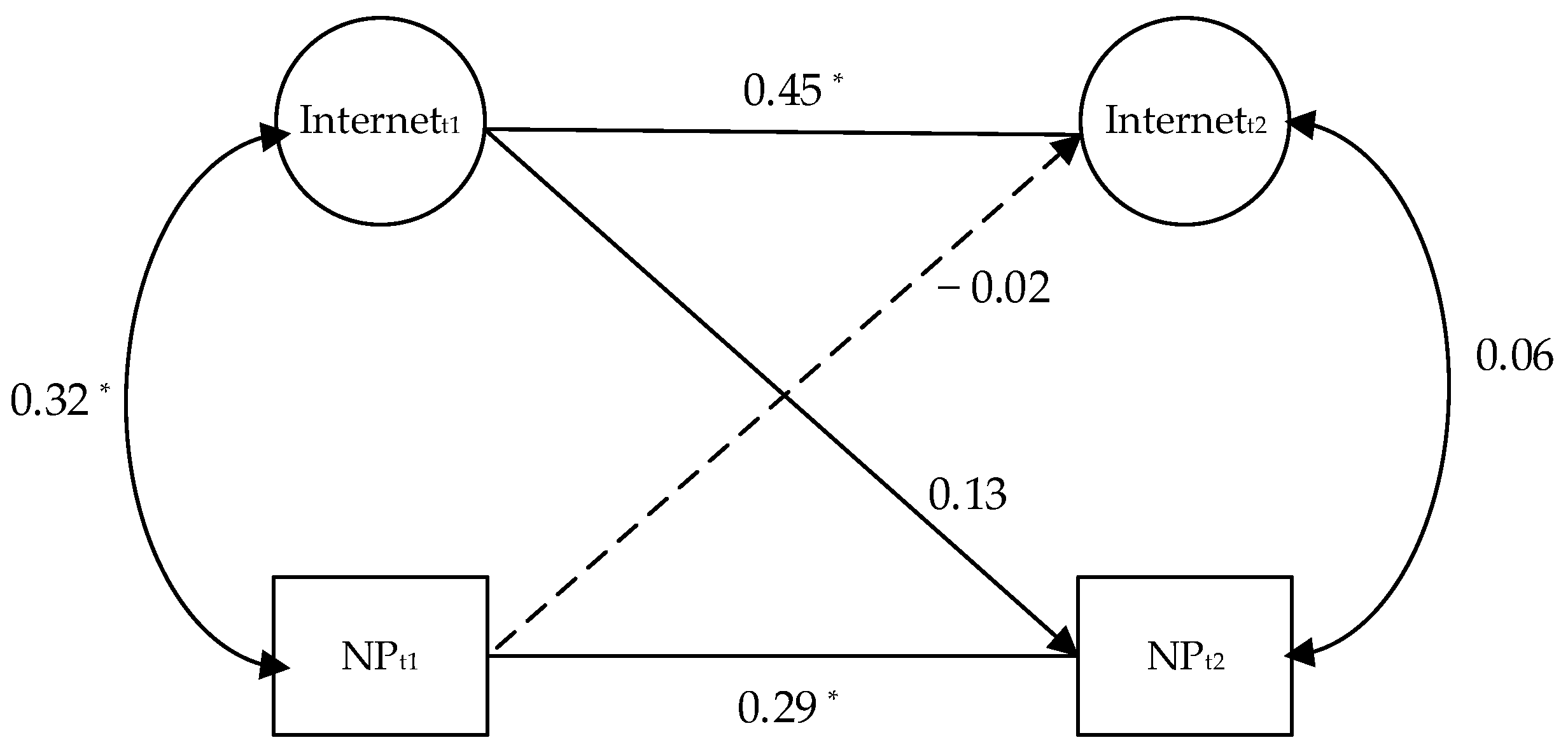
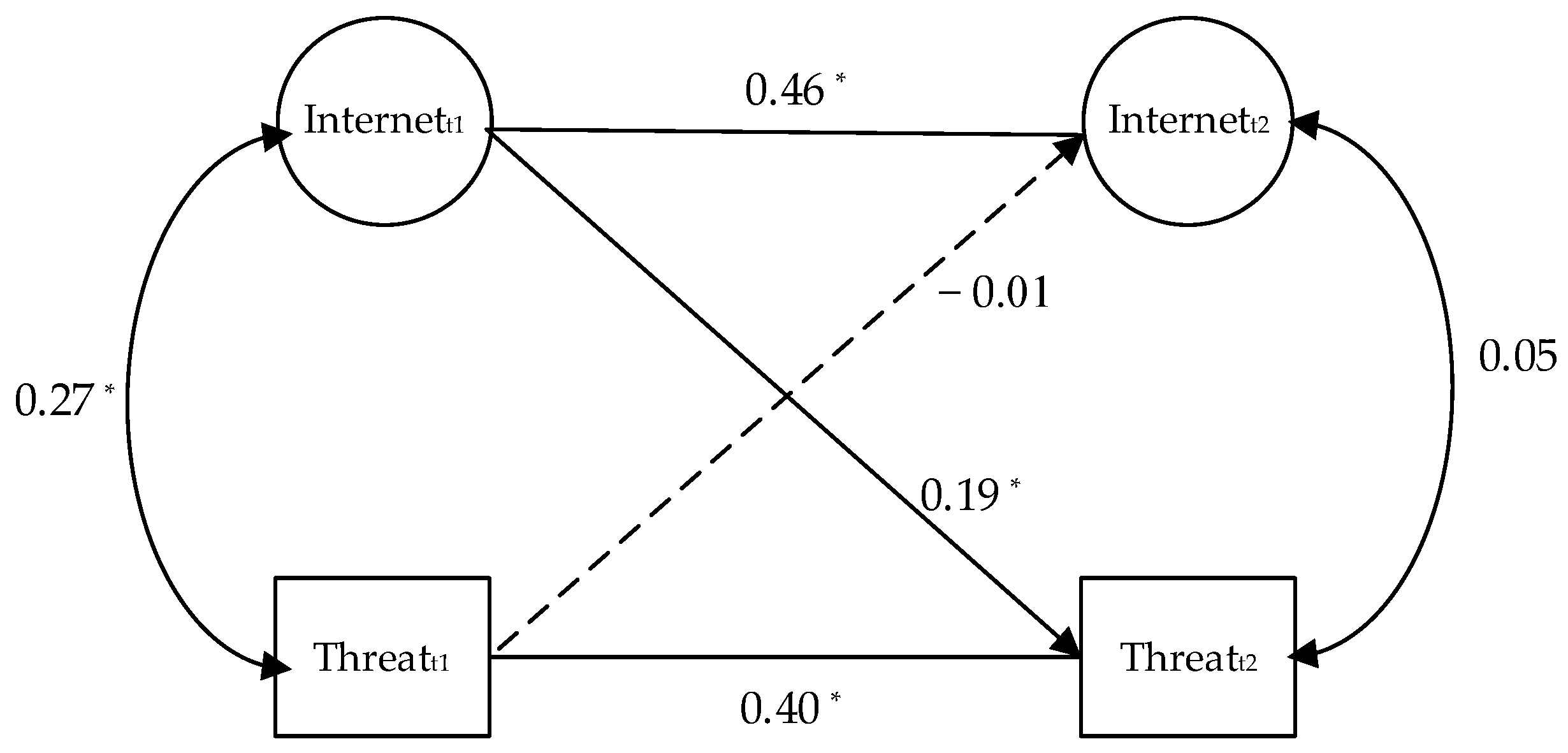
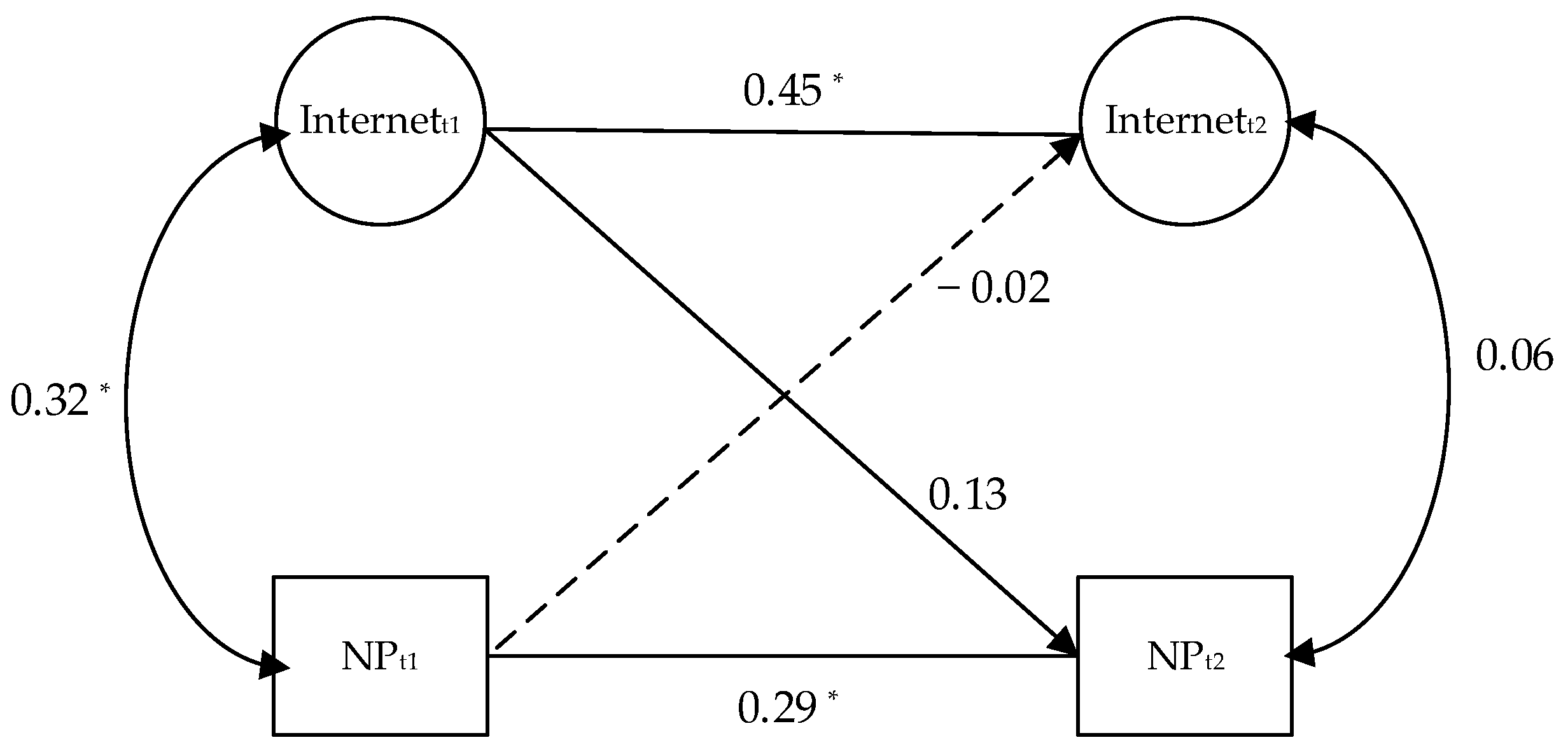
3.3. Cross-Lagged Analyses Using Both Wave 1 and Wave 2 Data
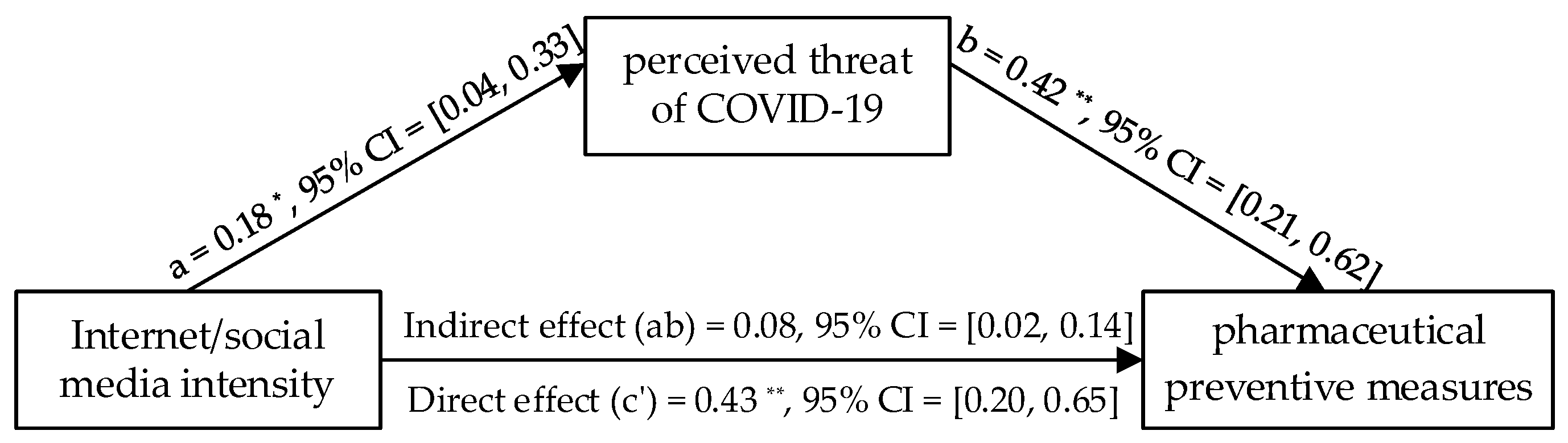
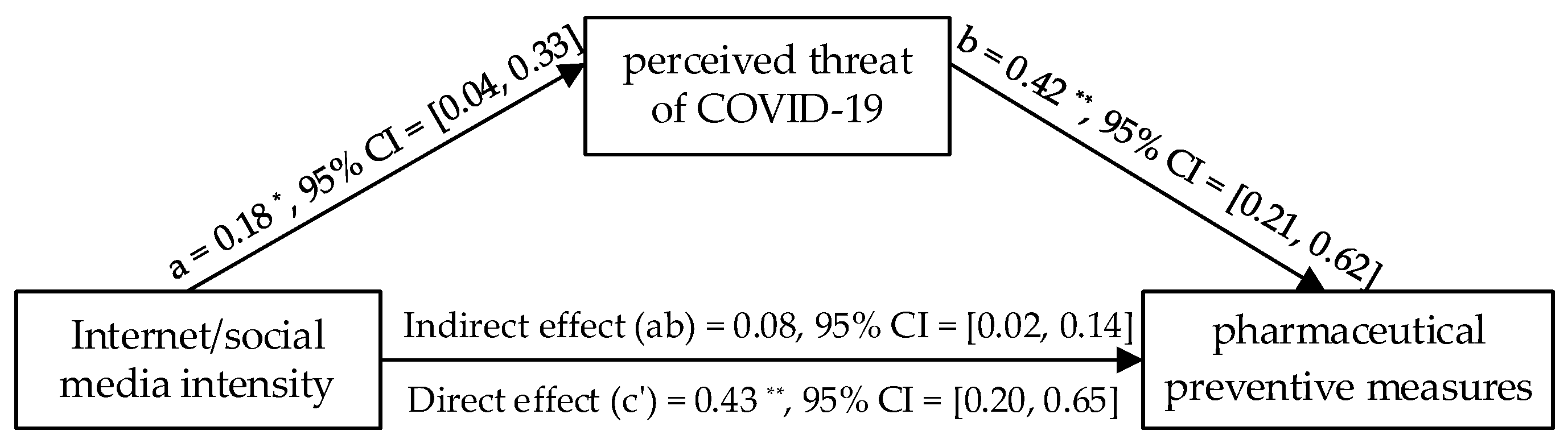
3.4. Mediation Analysis for Pharmaceutical Measures by Wave 2 Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard Oct-16th. 2021. Available online: https://covid19.who.int/ (accessed on 16 October 2021).
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Usage of Social Media as a News Source Worldwide. 2020. Available online: https://www.statista.com/statistics/718019/social-media-news-source/ (accessed on 16 October 2021).
- Sedgwick, R.; Epstein, S.; Dutta, R.; Ougrin, D. Social media, internet use and suicide attempts in adolescents. Curr. Opin. Psychiatr. 2019, 32, 534–541. [Google Scholar] [CrossRef]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Buchanan, M. Managing the infodemic. Nat. Phys. 2020, 16, 894. [Google Scholar] [CrossRef]
- Zeng, J.; Chan, C.A. cross-national diagnosis of infodemics: Comparing the topical and temporal features of misinformation around COVID-19 in China, India, the US, Germany and France. Online Inf. Rev. 2021, 45, 709–728. [Google Scholar] [CrossRef]
- Swire-Thompson, B.; Lazer, D. Public health and online misinformation: Challenges and recommendations. Annu. Rev. Public Health. 2019, 41, 433–451. [Google Scholar] [CrossRef] [Green Version]
- Cinelli, M.; Quattrociocchi, W.; Galeazzi, A.; Valensise, C.M.; Brugnoli, E.; Schmidt, A.L.; Zola, P.; Zollo, F.; Scala, A. The COVID-19 social media infodemic. Sci. Rep. 2020, 10, 16598. [Google Scholar] [CrossRef] [PubMed]
- Del Vicario, M.; Bessi, A.; Zollo, F.; Petroni, F.; Scala, A.; Caldarelli, G.; Stanley, H.E.; Quattrociocchi, W. The spreading of misinformation online. Proc. Natl. Acad. Sci. USA 2016, 113, 554–559. [Google Scholar] [CrossRef] [Green Version]
- Marwick, A.; Lewis, R. Media Manipulation and Disinformation Online; Data & Society Research Institute: New York, NY, USA, 2017. [Google Scholar]
- Tucker, J.A.; Guess, A.; Barberá, P.; Vaccari, C.; Siegel, A.; Sanovich, S.; Stukal, D.; Nyhan, B. Social Media, Political Polarization, and Political Disinformation: A Review of the Scientific Literature. 2018. Available online: https://ssrn.com/abstract=3144139 (accessed on 16 October 2021).
- Wang, Y.; McKee, M.; Torbica, A.; Stuckler, D. Systematic literature review on the spread of health-related misinformation on social media. Soc. Sci. Med. 2019, 240, 112552. [Google Scholar] [CrossRef]
- Guazzini, A.; Fiorenza, M.; Panerai, G.; Duradoni, M. What Went Wrong? Predictors of Contact Tracing Adoption in Italy during COVID-19 Pandemic. Future Internet 2021, 13, 286. [Google Scholar] [CrossRef]
- Roz, P. As Many as 130000 Lives Could Be Saved the Next 3 Months If Everyone Wore a Mask. 2020. Available online: https://www.healthline.com/health-news/as-many-as-130000-lives-could-be-saved-the-next-3-months-if-everyone-wore-a-mask (accessed on 16 October 2021).
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the US. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef] [PubMed]
- Berger, J.; Milkman, K.L. What makes online content viral? J. Mark. Res. 2012, 49, 192–205. [Google Scholar] [CrossRef] [Green Version]
- Chiu, Y.; Chiou, J.C.; Fang, W.; Lin, Y.J.; Wu, M. Design, fabrication, and control of components in MEMS-based optical pickups. IEEE Trans. Magn. 2007, 43, 780–784. [Google Scholar] [CrossRef]
- Brunvand, J.H. The Vanishing Hitchhiker: American Urban Legends and Their Meanings; WW Norton & Company: New York, NY, USA, 1981; p. 11. [Google Scholar]
- Allport, G.W.; Postman, L. The Psychology of Rumor; Henry Holt: New York, NY, USA, 1947. [Google Scholar]
- Feinberg, M.; Willer, R.; Stellar, J.; Keltner, D. The virtues of gossip: Reputational information sharing as prosocial behavior. J. Personal. Soc. Psychol. 2012, 102, 1015–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guess, A.; Nagler, J.; Tucker, J. Less than you think: Prevalence and predictors of fake news dissemination on Facebook. Sci. Adv. 2019, 5, eaau4586. [Google Scholar] [CrossRef] [Green Version]
- Temple, E.; Jaiswal, A.; Jaiswal, S. COVID-19 Related Knowledge, Risk Perceptions, and Practices amongst Irish Residents. COVID 2021, 1, 166–185. [Google Scholar] [CrossRef]
- Yin, C.; Baijie, A. Weibo Gives Rumors No Time to Thrive. 2011. Available online: https://www.chinadaily.com.cn/china/2011-11/04/content_14035335.htm (accessed on 16 October 2021).
- Zeng, J.; Chan, C.H.; Fu, K.W. How social media construct “truth” around crisis events: Weibo’s rumor management strategies after the 2015 Tianjin blasts. Policy Internet 2017, 9, 297–320. [Google Scholar] [CrossRef]
- National Health Commission of People’s Republic of China. Guidelines for Public Protection against Novel Coronavirus Infection. 2020. Available online: http://www.nhc.gov.cn/jkj/s7915/202001/bc661e49b5bc487dba182f5c49ac445b.shtml (accessed on 16 October 2021).
- Jang, K.; Park, N. The effects of repetitive information communication through multiple channels on prevention behavior during the 2015 MERS outbreak in South Korea. J. Health Commun. 2018, 23, 670–678. [Google Scholar] [CrossRef]
- Yoo, W.; Choi, D.H.; Park, K. The effects of SNS communication: How expressing and receiving information predict MERS-preventive behavioral intentions in South Korea. Comput. Hum. Behav. 2016, 62, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Duradoni, M.; Fiorenza, M.; Guazzini, A. When Italians Follow the Rules against COVID Infection: A Psychologi-cal Profile for Compliance. COVID 2021, 1, 246–262. [Google Scholar] [CrossRef]
- Liu, J.H.; Zhang, R.J.; Vilar, R.; Milojev, P.; Hakim, M.A.; de Zúñiga, H.G.; Schumann, S.; Páez, D. A typology of masspersonal information seeking repertoires (MISR): Global implications for political participation and subjective well-being. New Media Soc. 2021, 23, 2729–2753. [Google Scholar] [CrossRef]
- China Internet Network Information Center. The 47th China Statistical Report on Internet Development. 2021. Available online: http://www.gov.cn/xinwen/2021-02/03/content_5584518.htm (accessed on 16 October 2021).
- Corp, I. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp.: Armonk, NY, USA, 2018. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Fitzgerald, J.; Gottschalk, P.; Moffitt, R. An Analysis of Sample Attrition in Panel Data: The Michigan Panel Study of Income Dynamics. J. Hum. Resour. 1998, 33, 251–299. [Google Scholar] [CrossRef]
- Proto, E.; Zhang, A. COVID-19 and Mental Health of Individuals with Different Personalities. Proc. Natl. Acad. Sci. USA 2021, 118, e2109282118. [Google Scholar] [CrossRef] [PubMed]
- Rivenbark, J.; Arseneault, L.; Caspi, A.; Danese, A.; Fisher, H.L.; Moffitt, T.E.; Rasmussen, L.J.H.; Russell, M.A.; Odgers, C.L. Adolescents’ perceptions of family social status correlate with health and life chances: A twin difference longitudinal cohort study. Proc. Natl. Acad. Sci. USA 2020, 117, 23323–23328. [Google Scholar] [CrossRef] [Green Version]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addict. 2020, 19, 1875–1888. [Google Scholar] [CrossRef] [PubMed]
- Katapodi, M.C.; Lee, K.A.; Facione, N.C.; Dodd, M.J. Predictors of perceived breast cancer risk and the relation between perceived risk and breast cancer screening: A meta-analytic review. Prev. Med. 2004, 38, 388–402. [Google Scholar] [CrossRef]
- Miles, A.; Voorwinden, S.; Chapman, S.; Wardle, J. Psychologic predictors of cancer information avoidance among older adults: The role of cancer fear and fatalism. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1872–1879. [Google Scholar] [CrossRef] [Green Version]
- Starcevic, V.; Schimmenti, A.; Billieux, J.; Berle, D. Cyberchondria in the time of the COVID-19 pandemic. Hum. Behav. Emerg. Technol. 2021, 3, 53–62. [Google Scholar] [CrossRef]
- Jokic-Begic, N.; Lauri Korajlija, A.; Mikac, U. Cyberchondria in the age of COVID-19. PLoS ONE 2020, 15, e0243704. [Google Scholar] [CrossRef]
- Witte, K. Putting the fear back into fear appeals: The extended parallel process model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Relevant Instructions on Rumor Refuting Institutions on WeChat Public Platforms. Available online: https://kf.qq.com/faq/17030722muuu170307MFBny2.html (accessed on 16 October 2021).
- Lu, Z.; Jiang, Y.; Lu, C.; Naaman, M.; Wigdor, D. The government’s dividend: Complex perceptions of social media misinformation in China. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, New York, NY, USA, 25–30 April 2020; pp. 1–12. [Google Scholar] [CrossRef]
- Fineberg, H.V. Pandemic preparedness and response—Lessons from the H1N1 influenza of 2009. N. Engl. J. Med. 2014, 370, 1335–1342. [Google Scholar] [CrossRef] [Green Version]
- Fu, K.W.; Zhu, Y. Did the world overlook the media’s early warning of COVID-19? J. Risk Res. 2020, 23, 1047–1051. [Google Scholar] [CrossRef]
- Salzberger, B.; Glück, T.; Ehrenstein, B. Successful containment of COVID-19: The WHO-Report on the COVID-19 outbreak in China. Infection 2020, 48, 151–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.H.; Li, M.C.; Yue, X. Chinese social identity and intergroup relations: The influence of benevolent authority. In The Oxford Handbook of Chinese Psychology; Bond, M.H., Ed.; Oxford University Press: Oxford, UK, 2010; pp. 579–597. [Google Scholar]
- COVID-19 Misleading Information Policy. Available online: https://help.twitter.com/en/rules-and-policies/medical-misinformation-policy (accessed on 16 October 2021).
- Knobloch-Westerwick, S.; Johnson, B.K.; Westerwick, A. Confirmation bias in online searches: Impacts of selective exposure before an election on political attitude strength and shifts. J. Comput.-Mediat. Commun. 2015, 20, 171–187. [Google Scholar] [CrossRef] [Green Version]
- Pariser, E. The Filter Bubble: How the New Personalized Web Is Changing What We Read and How We Think; Penguin: London, UK, 2011. [Google Scholar]
- Sunstein, C. Republic.com 2.0.; Princeton University Press: Princeton, NJ, USA, 2007. [Google Scholar]
- Jamieson, K.H.; Cappella, J.N. Echo Chamber: Rush Limbaugh and the Conservative Media Establishment; Oxford University Press: New York, NY, USA, 2008. [Google Scholar]
- Bucher, T. Want to be on the top? Algorithmic power and the threat of invisibility on Facebook. New Media Soc. 2012, 14, 1164–1180. [Google Scholar] [CrossRef]
- Coronavirus Challenge on TikTok: Video Maker Infected after Licking Public Toilet Seat. 2020. Available online: https://timesofindia.indiatimes.com/gadgets-news/coronavirus-challenge-on-tiktok-video-maker-infected-after-licking-public-toilet-seat/articleshow/74839613.cms (accessed on 16 October 2021).
- Van der Voorn, T.; de Jong, M. Cope or Perish? Managing Tipping Points in Developing Coping Strategies for Emergency Response during the First Wave of the COVID-19 Outbreak in Europe. COVID 2021, 1, 39–70. [Google Scholar] [CrossRef]
- Liu, J.H. Majority world successes and European and American failure to contain COVID-19: Cultural collectivism and global leadership. Asian J. Soc. Psychol. 2021, 24, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.; Estrada-Villalta, S.; Sullivan, D.; Markus, H.R. The psychology of neoliberalism and the neoliberalism of psychology. J. Soc. Issues 2019, 75, 189–216. [Google Scholar] [CrossRef]
- Bettache, K.; Chiu, C.Y. The invisible hand is an ideology: Toward a social psychology of neoliberalism. J. Soc. Issues 2019, 75, 8–19. [Google Scholar] [CrossRef]
- Liu, J.H.; Leong, C.H.; Huang, S.Y.; Chen, S.X.; Choi, H.S.; Yamaguchi, S.; Lee, I.C.; Inoue, Y. Pandemic: Vigilance, civic responsibility critical to East Asia’s success. East Asia Forum Q. 2020, 12, 29–30. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | M | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Internet (n = 1016) | - | 5.11 | 0.92 | |||||||
| 2. Threat (n = 1017) | 0.35 ** | - | 6.30 | 0.91 | ||||||
| 3. OT (n = 1014) | 0.03 | −0.05 | - | 0.48 | 0.50 | |||||
| 4. NPM (n = 1016) | 0.41 ** | 0.56 ** | −0.04 | - | 6.25 | 0.94 | ||||
| 5. Age (n = 1014) | −0.18 ** | 0.08 ** | −0.17 ** | 0.00 | - | 37.25 | 10.32 | |||
| 6. Gender (n = 1015) | 0.04 | −0.03 | 0.14 ** | 0.01 | −0.28 ** | - | 0.52 | 0.50 | ||
| 7. Education (n = 1014) | 0.19 ** | −0.02 | 0.11 ** | 0.02 | −0.25 ** | 0.10 | - | 4.80 | 0.71 | |
| 8. Status (n = 1015) | 0.20 ** | −0.05 | 0.01 | 0.01 | −0.07 * | 0.03 | 0.20 | - | 5.42 | 1.55 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | M | SD |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Internet (n = 220) | — | 4.94 | 0.84 | |||||||
| 2. Threat (n = 220) | 0.13 | — | 6.35 | 0.84 | ||||||
| 3. OT (n = 220) | 0.04 | 0.00 | — | 0.53 | 0.50 | |||||
| 4. PM (n = 220) | 0.32 ** | 0.25 ** | −0.05 | — | 5.27 | 1.39 | ||||
| 5. Age (n = 220) | −0.19 ** | 0.18 ** | −0.00 ** | −0.12 | — | 36.40 | 8.98 | |||
| 6. Gender (n = 219) | 0.07 | −0.04 | 0.04 | −0.06 | −0.28 ** | — | 0.51 | 0.50 | ||
| 7. Education (n = 219) | 0.18 ** | −0.10 | 0.11 ** | 0.17 * | −0.21 ** | 0.02 | — | 4.83 | 0.61 | |
| 8. Status (n = 220) | 0.39 ** | −0.01 | −0.03 | 0.12 | −0.27 * | 0.11 | 0.26 ** | — | 5.63 | 1.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, T.; Tang, M.; Zhang, R.J.; Liu, J.H. The Active Role of the Internet and Social Media Use in Nonpharmaceutical and Pharmaceutical Preventive Measures against COVID-19. Healthcare 2022, 10, 113. https://doi.org/10.3390/healthcare10010113
Xie T, Tang M, Zhang RJ, Liu JH. The Active Role of the Internet and Social Media Use in Nonpharmaceutical and Pharmaceutical Preventive Measures against COVID-19. Healthcare. 2022; 10(1):113. https://doi.org/10.3390/healthcare10010113
Chicago/Turabian StyleXie, Tian, Meihui Tang, Robert Jiqi Zhang, and James H. Liu. 2022. "The Active Role of the Internet and Social Media Use in Nonpharmaceutical and Pharmaceutical Preventive Measures against COVID-19" Healthcare 10, no. 1: 113. https://doi.org/10.3390/healthcare10010113
APA StyleXie, T., Tang, M., Zhang, R. J., & Liu, J. H. (2022). The Active Role of the Internet and Social Media Use in Nonpharmaceutical and Pharmaceutical Preventive Measures against COVID-19. Healthcare, 10(1), 113. https://doi.org/10.3390/healthcare10010113