
Patterns of Changes in Oncological Care due to COVID-19: Results of a Survey of Oncological Nurses and Physicians from the Region of Hanover, Germany


Abstract
:1. Background
2. Methods
2.1. Sample
2.2. Variables
2.3. Data Analysis
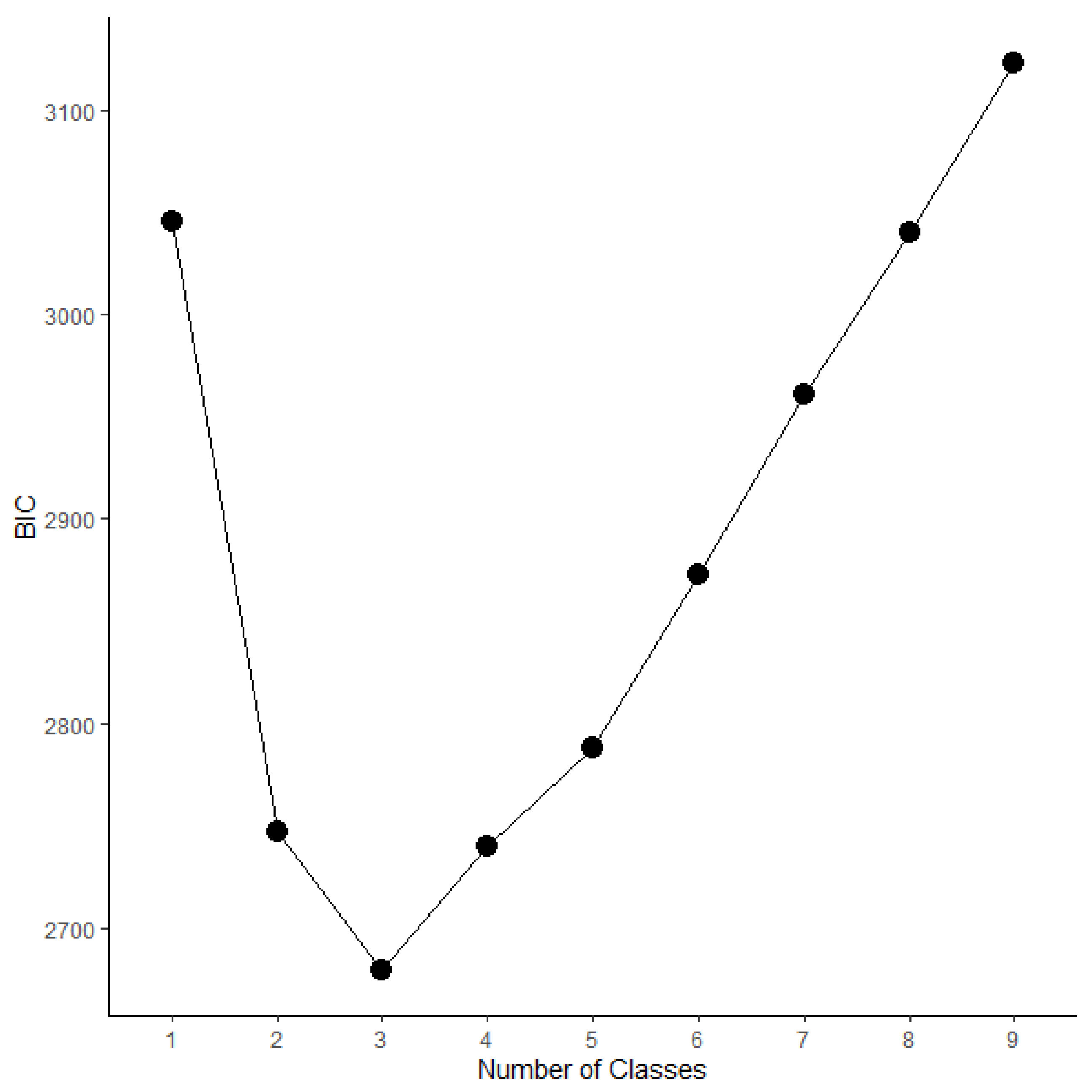
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Tougeron, D.; Michel, P.; Lièvre, A.; Ducreux, M.; Gaujoux, S.; Guiu, B.; Huguet, F.; Lecomte, T.; Lepage, C.; Louvet, C.; et al. Management of digestive cancers during the COVID-19 second wave: A French intergroup point of view (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, ACHBT, SFR). Dig. Liver Dis. 2021, 53, 306–308. [Google Scholar] [CrossRef] [PubMed]
- Brugel, M.; Carlier, C.; Essner, C.; Debreuve-Theresette, A.; Beck, M.F.; Merrouche, Y.; Bouché, O. Dramatic Changes in Oncology Care Pathways During the COVID -19 Pandemic: The French ONCOCARE-COV Study. Oncologist 2020, 26, e338–e341. [Google Scholar] [CrossRef] [PubMed]
- Büntzel, J.; Klein, M.; Keinki, C.; Walter, S.; Büntzel, J.; Hübner, J. Oncology services in corona times: A flash interview among German cancer patients and their physicians. J. Cancer Res. Clin. Oncol. 2020, 146, 2713–2715. [Google Scholar] [CrossRef] [PubMed]
- Jazieh, A.R.; Akbulut, H.; Curigliano, G.; Rogado, A.; Alsharm, A.A.; Razis, E.D.; Mula-Hussain, L.; Errihani, H.; Khattak, A.; De Guzman, R.B.; et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob. Oncol. 2020, 6, 1428–1438. [Google Scholar] [CrossRef]
- Reichardt, P.; Bollmann, A.; Hohenstein, S.; Glass, B.; Untch, M.; Reichardt, A.; Amrein, D.; Kuhlen, R. Decreased Incidence of Oncology Admissions in 75 Helios Hospitals in Germany during the COVID-19 Pandemic. Oncol. Res. Treat. 2020, 44, 71–74. [Google Scholar] [CrossRef]
- Scheidt-Nave, C.; Barnes, B.; Beyer, A.-K.; Busch, M.; Hapke, U.; Heidemann, C.; Imhoff, M.; Mumm, R.; Paprott, R.; Steppuhn, H.; et al. Care for the chronically ill in Germany—The challenges during the COVID-19 pandemic. J. Health Monitor. 2020, 5 (Suppl. 10). [Google Scholar] [CrossRef]
- Spencer, K.; Jones, C.M.; Girdler, R.; Roe, C.; Sharpe, M.; Lawton, S.; Miller, L.; Lewis, P.; Evans, M.; Sebag-Montefiore, D.; et al. The impact of the COVID-19 pandemic on radiotherapy services in England, UK: A population-based study. Lancet Oncol. 2021, 22, 309–320. [Google Scholar] [CrossRef]
- Mori, M.; Krumholz, H.M.; Allore, H.G. Using Latent Class Analysis to Identify Hidden Clinical Phenotypes. JAMA 2020, 324, 700–701. [Google Scholar] [CrossRef]
- Zhou, M.; Thayer, W.M.; Bridges, J.F.P. Using Latent Class Analysis to Model Preference Heterogeneity in Health: A Systematic Review. PharmacoEconomics 2018, 36, 175–187. [Google Scholar] [CrossRef]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral and Health Sciences; Wiley: Hoboken, NJ, USA, 2010. [Google Scholar]
- Ulbricht, C.M.; Chrysanthopoulou, S.A.; Levin, L.; Lapane, K.L. The use of latent class analysis for identifying subtypes of depression: A systematic review. Psychiatry Res. 2018, 266, 228–246. [Google Scholar] [CrossRef]
- Xiao, Y.; Romanelli, M.; Lindsey, M.A. A latent class analysis of health lifestyles and suicidal behaviors among US adolescents. J. Affect. Disord. 2019, 255, 116–126. [Google Scholar] [CrossRef]
- Stekhoven, D.J.; Buhlmann, P. MissForest--non-parametric missing value imputation for mixed-type data. Bioinformatics 2012, 28, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent Class Analysis: A Guide to Best Practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Spurk, D.; Hirschi, A.; Wang, M.; Valero, D.; Kauffeld, S. Latent profile analysis: A review and “how to” guide of its application within vocational behavior research. J. Vocat. Behav. 2020, 120, 103445. [Google Scholar] [CrossRef]
- Nylund-Gibson, K.; Choi, A.Y. Ten frequently asked questions about latent class analysis. Transl. Issues Psychol. Sci. 2018, 4, 440–461. [Google Scholar] [CrossRef]
- Wurpts, I.C.; Geiser, C. Is adding more indicators to a latent class analysis beneficial or detrimental? Results of a Monte-Carlo study. Front. Psychol. 2014, 5, 920. [Google Scholar] [CrossRef] [Green Version]
- Hanna, T.P.; Evans, G.A.; Booth, C.M. Cancer, COVID-19 and the precautionary principle: Prioritizing treatment during a global pandemic. Nat. Rev. Clin. Oncol. 2020, 17, 268–270. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Psychosocial Services to Cancer Patients/Families in a Community Setting. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs; National Academies Press: Washington, DC, USA, 2008. [Google Scholar]
- Weisel, K.C.; Morgner-Miehlke, A.; Petersen, C.; Fiedler, W.; Block, A.; Schafhausen, P.; Knobloch, J.K.; Bokemeyer, C. Implications of SARS-CoV-2 Infection and COVID-19 Crisis on Clinical Cancer Care: Report of the University Cancer Center Hamburg. Oncol. Res. Treat. 2020, 43, 307–313. [Google Scholar] [CrossRef]
- Onesti, C.E.; Rugo, H.S.; Generali, D.; Peeters, M.; Zaman, K.; Wildiers, H.; Harbeck, N.; Martin, M.; Cristofanilli, M.; Cortes, J.; et al. Oncological care organisation during COVID-19 outbreak. ESMO Open 2020, 5, e000853. [Google Scholar] [CrossRef]
- Vallelonga, F.; Elia, F. Doctor–patient relationship at the time of COVID-19: Travel notes. Intensiv. Care Med. 2020, 46, 1802. [Google Scholar] [CrossRef]
- Borges, L.M.; Barnes, S.M.; Farnsworth, J.K.; Bahraini, N.H.; Brenner, L.A. A commentary on moral injury among health care providers during the COVID-19 pandemic. Psychol. Trauma: Theory Res. Pr. Policy 2020, 12, S138–S140. [Google Scholar] [CrossRef]
- Koffman, J.; Gross, J.; Etkind, S.N.; Selman, L. Uncertainty and COVID-19: How are we to respond? J. R. Soc. Med. 2020, 113, 211–216. [Google Scholar] [CrossRef]
- Rutter, H.; Wolpert, M.; Greenhalgh, T. Managing uncertainty in the COVID-19 era. BMJ 2020, 370, m3349. [Google Scholar] [CrossRef]
- Williams, J.A.; Zimmerman, F.; Bell, J.F. Norms and Trends of Sleep Time Among US Children and Adolescents. JAMA Pediatr. 2013, 167, 55–60. [Google Scholar] [CrossRef] [Green Version]
- De La Fuente-Solana, E.I.; Pradas-Hernández, L.; Ramiro-Salmerón, A.; Suleiman-Martos, N.; Gómez-Urquiza, J.L.; Albendín-García, L.; Cañadas-De La Fuente, G. Burnout Syndrome in Paediatric Oncology Nurses: A Systematic Review and Meta-Analysis. Healthcare 2020, 8, 309. [Google Scholar] [CrossRef]
- Kagan, I.; Hendel, T.; Savitsky, B. Personal initiative and work environment as predictors of job satisfaction among nurses: Cross-sectional study. BMC Nurs. 2021, 20, 1–10. [Google Scholar] [CrossRef]
- Arnholdt, J.; Haier, J. Cancer patients’ preferences for therapy decisions can be grouped into categories and separated by demographic factors. J. Cancer Res. Clin. Oncol. 2017, 143, 1573–1584. [Google Scholar] [CrossRef]
- Rosenman, R.; Tennekoon, V.; Hill, L.G. Measuring bias in self-reported data. Int. J. Behav. Heal. Res. 2011, 2, 320–332. [Google Scholar] [CrossRef]
- Geyer, S. Social inequalities in the incidence and case fatality of cancers of the lung, the stomach, the bowels, and the breast. Cancer Causes Control. 2008, 19, 965–974. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | Level | %/M (SD) |
|---|---|---|
| Age | 43.16 (10.99) | |
| Gender | Male | 33.5% |
| Female | 66.5% | |
| Work Experience | 18.02 (11.66) | |
| Leadership Role | No Leadership role | 59.0% |
| Leadership role | 41.0% | |
| Group | Physicians | 46.5% |
| Nurses | 53.5% |
| Variable | Level | %/M (SD) |
|---|---|---|
| Changes in Prevention | Not at all | 15.0% |
| To a small degree | 18.0% | |
| To a medium degree | 24.5% | |
| To a large degree | 33.5% | |
| Completely | 9.0% | |
| Changes in Curative Therapy | Not at all | 36.5% |
| To a small degree | 31.5% | |
| To a medium degree | 14.0% | |
| To a large degree | 16.0% | |
| Completely | 2.0% | |
| Changes in Advanced Cancer Care | Not at all | 33.5% |
| To a small degree | 31.0% | |
| To a medium degree | 20.5% | |
| To a large degree | 12.0% | |
| Completely | 3.0% | |
| Changes in Palliative Care | Not at all | 24.5% |
| To a small degree | 31.0% | |
| To a medium degree | 23.0% | |
| To a large degree | 17.0% | |
| Completely | 4.5% | |
| Changes in Psychosocial Care | Not at all | 13.5% |
| To a small degree | 18.5% | |
| To a medium degree | 27.0% | |
| To a large degree | 29.0% | |
| Completely | 12.0% | |
| Decision Conflicts | Yes | 67.0% |
| No | 33.0% | |
| Decision Uncertainty | Not at all | 23.5% |
| To a small degree | 41.0% | |
| To a medium degree | 20.0% | |
| To a large degree | 13.5% | |
| Completely | 2.0% | |
| Changes in Communication with Patients | Much worse | 5.0% |
| Slightly worse | 27.5% | |
| About the same | 57.0% | |
| Slightly better | 9.0% | |
| Much better | 1.5% | |
| Psychological distress | 1.78 (0.59) | |
| Changes in Work stress | Much worse | 4.0% |
| Slightly worse | 14.0% | |
| About the same | 22.5% | |
| Slightly better | 40.5% | |
| Much better | 19.0% | |
| Changes in Process Quality | Much worse | 12.5% |
| Slightly worse | 47.0% | |
| About the same | 26.5% | |
| Slightly better | 13.0% | |
| Much better | 1.0% | |
| Changes in Personnel Resources | Much worse | 9.5% |
| Slightly worse | 38.5% | |
| About the same | 43.5% | |
| Slightly better | 7.5% | |
| Much better | 1.0% |
| Socio-Demographic/Risk Behavior Characteristics | Few Changes Profile | Medium Changes Profile | Severe Changes Profile | p |
|---|---|---|---|---|
| Age (M ± SD) | 45.98 ± 10.8 | 40.6 ± 10.76 | 43.85 ± 10.80 | 0.007 |
| Gender (%) | 71% | 62% | 69% | 0.431 |
| Work Experience (M ± SD) | 21.03 ± 12.34 | 14.92 ± 10.78 | 19.44 ± 11.06 | 0.006 |
| Leadership Role (leadership %) | 44% | 41% | 38% | 0.786 |
| Group (Nurses %) | 59% | 40% | 71% | 0.001 |
| Decision Conflicts (Yes %) | 18% | 35% | 50% | 0.002 |
| Decision Uncertainty (M ± SD) | 1.85 ± 1.06 | 2.28 ± 0.85 | 2.94 ± 1.00 | <0.001 |
| Communication with Patients (M ± SD) | 2.91 ± 0.57 | 2.7 ± 0.80 | 2.60 ± 0.84 | 0.013 |
| Psychological Distress (M ± SD) | 1.70 ± 0.52 | 1.80 ± 0.61 | 1.85 ± 0.62 | 0.554 |
| Work Stress (M ± SD) | 3.62 ± 1.05 | 3.53 ± 1.04 | 3.54 ± 1.18 | 0.916 |
| Process Organization (M ± SD) | 2.68 ± 0.9 | 2.31 ± 0.86 | 2.29 ± 0.94 | 0.012 |
| Personnel Resources (M ± SD) | 2.65 ± 0.71 | 2.47 ± 0.82 | 2.44 ± 0.90 | 0.138 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beller, J.; Schäfers, J.; Geyer, S.; Haier, J.; Epping, J. Patterns of Changes in Oncological Care due to COVID-19: Results of a Survey of Oncological Nurses and Physicians from the Region of Hanover, Germany. Healthcare 2022, 10, 15. https://doi.org/10.3390/healthcare10010015
Beller J, Schäfers J, Geyer S, Haier J, Epping J. Patterns of Changes in Oncological Care due to COVID-19: Results of a Survey of Oncological Nurses and Physicians from the Region of Hanover, Germany. Healthcare. 2022; 10(1):15. https://doi.org/10.3390/healthcare10010015
Chicago/Turabian StyleBeller, Johannes, Jürgen Schäfers, Siegfried Geyer, Jörg Haier, and Jelena Epping. 2022. "Patterns of Changes in Oncological Care due to COVID-19: Results of a Survey of Oncological Nurses and Physicians from the Region of Hanover, Germany" Healthcare 10, no. 1: 15. https://doi.org/10.3390/healthcare10010015