
Perceived Barriers and Facilitators to Psychotherapy Utilisation and How They Relate to Patient’s Psychotherapeutic Goals
 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Empirical Findings for Barriers and Facilitators
1.2. Aims and Research Questions
2. Materials and Methods
2.1. The Field of Research
2.2. Recruitment
2.3. Data Collection
2.4. Participants
2.5. Data Analysis
2.5.1. Content Analysis
2.5.2. Across-Group Comparison
3. Results
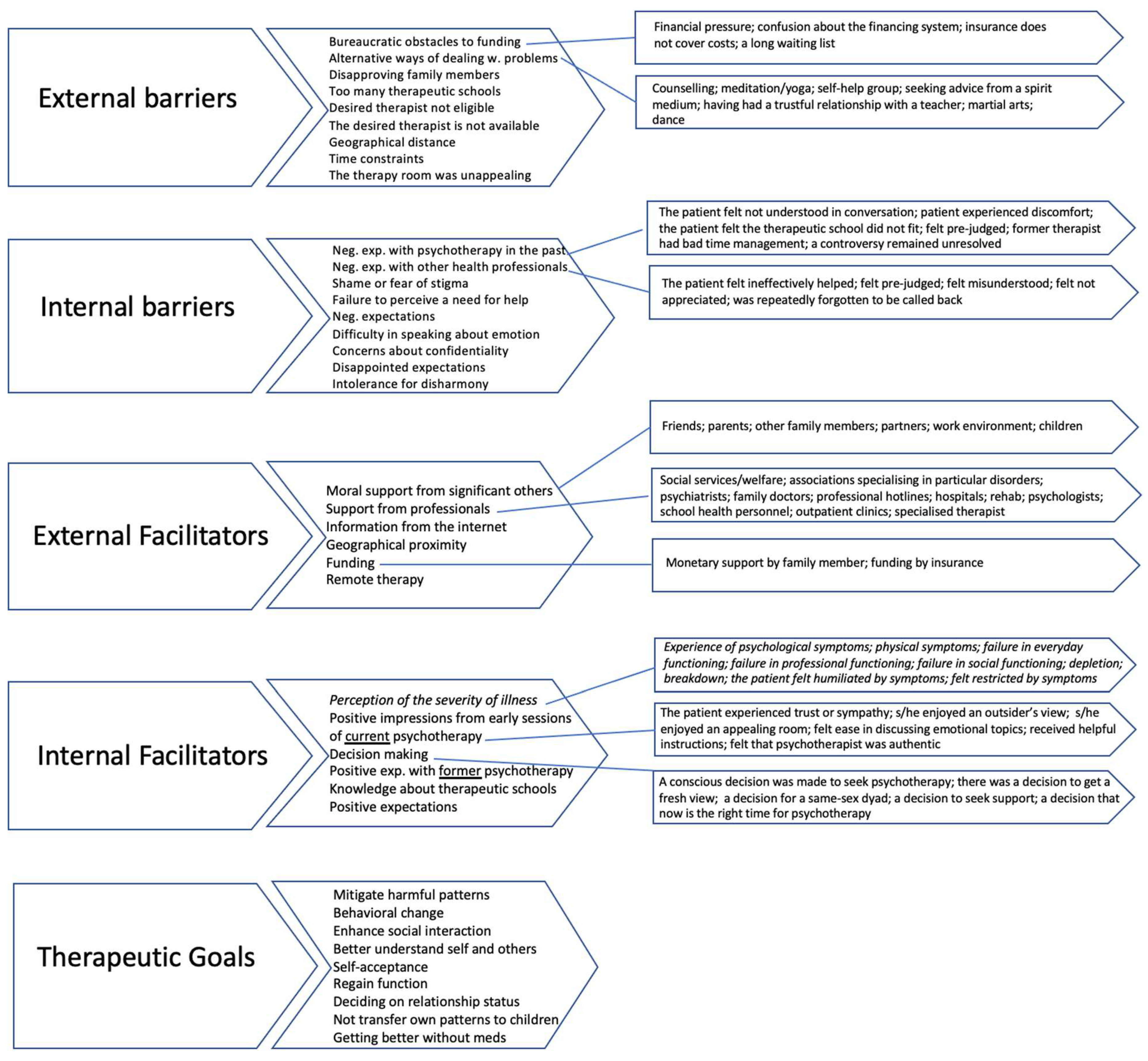
3.1. Description of Categories
3.1.1. External Barriers
(…) I thought, “I cannot afford this right now”. We [my husband and I] are self-employed, work in the arts and culture sector, and are massively affected by Covid. Moreover//um//I thought//um//the insurance pays a little extra, but it is marginal. So, therapy is something you must be able to afford (-)//be able//. So that was an issue. And I thought to myself, no, I cannot afford it now. And now I think, “yes, but I have to afford it” (female, age 45).
How did I get to my new therapy now? Well, it was pretty tricky. In the end, I did not go for treatment for half a year because, at that time, I was feeling terrible, really//shit//[not good]. At this time, I went to men’s counselling for a while (male, age 28).
I said: hey, I need something that gives me pleasure. Something that invigorates. And I sort of started dancing hip-hop. (--) And after one and a half years of hip-hop, it became breaking. Well, that is usually called breakdancing. (--) And that is when I found myself again (male, age 39).
… feels that now a therapist is allying//herself with his wife against him (female, age 45).
… I had an awful lot of first interviews, far too many, and I just did not manage to (-). I was completely overwhelmed with what was offered in Vienna because there were far too many therapists. I was utterly overwhelmed by the range of schools on offer because I did not know which type of therapy I should choose (male, age 28).
(…) I find that//I find it somehow tricky. The search, and also finding someone. What criteria should be followed (female, age 34)?
3.1.2. Internal Barriers
I also saw this therapist who just nodded the whole time, like “mhm,//mhm//mhm” I mean, he is not bad or anything. Still, the others also said that they did not like it, that he nods all the time, and so on.//Mhm//But I can understand it; it was just, he had a lot of work probably, a lot with Corona, too (female, age 20).
The problem was that he (-) gave me the feeling that I was treating him instead of him treating me. So, he rambled a lot and had many theories; I could not do anything with that. I think that was because of his orientation; it did not fit (male, age 43).
For us here, it [psychotherapy] is a somewhat notorious story. And I think almost no one in my circle has ever done one. Or just not told it, you know. It’s more of a secret discovery if someone finds out (laughs) (female, age 26).
I am one of those people for whom everything has to fit. Otherwise, if there is disharmony, if something does not run smoothly, I end things or just tell them what they want to hear, and that is not the purpose of therapy.//mhm//(female, age 36).
3.1.3. External Facilitators
And//mhm//I have a pretty good friend, yes, he is part of the family now, um, who regularly sees a therapist because he has epilepsy, and it is severe. And then we talked about it a bit. And that was then maybe all together, where I said, OK, now you tackle it and look for help.//mhm, mhm, yes//Yes (female, age 36).
My boss is accommodating, his ears are open to such things, and then we said together that it would not be a mistake//ah//if I make sure that I get help (male, age 31).
Um, the hospital was not open or did not pick up the phone, and then I called the//ahm//the telephone, the telephone helpline (-). And a trauma therapist picked up the phone. And I told her in a few minutes what was going on with me. And she said that I had emotional childhood trauma. She recognised it quickly and told me to seek body-oriented individual therapy (male, age 30).
Well, how I chose her was simple, I saw a picture of her, and I liked that. And her homepage was appealing. And with the others, I felt more like//ahm//I did not know if they would suit me because they were for older people, not younger people. And with her, I immediately felt that (-) we would fit (female, age 29).
I think it is essential that a therapist comes from the same region. Because she [the psychotherapist] has the same//um//background, she has grown up in the same circumstances//living the same village life (female, age 26).
We do it like this, um, I can do it via Skype,//aha//which helps me terribly because it’s a twenty-kilometre drive into the city. And with the children and my husband working shifts and then a shared car,//mhm, mhm//And she [the psychotherapist] only has certain days she is available, which narrows it down a lot. (…) It is very convenient for me that I can do it via Skype. And, um, I think that also helped with Corona greatly (female, age 36).
3.1.4. Internal Facilitators
It impressed me that she said: You do not have to stay here [in psychotherapy] only to visit. You may say: this does not fit me. Alternatively, you can always say it does not work for me anymore. So, I felt I could tell her that at any time. (-) And that//I think//already inspired much trust in me when I first saw her (female, age 26).
There are things I only want to discuss with a woman.//mhm, mhm//where I certainly do not need a man’s point of view (female, age 48).
I remember that last autumn, there was this lockdown, and I had the feeling that now we have, I do not know, two or three weeks where you can reflect on yourself (-). So you use this dark time of year, my birthday, it is always like that, and//ahm//to reflect, look at things that you do not usually get to, and tidy up from the inside. And that started this process (female, age 48).
Yeah, so, having done therapy before in 2019, I have known that it helps me (female, age 22).
Once I came to her, my priorities at that time were already bodywork and feeling understood; those were priorities number one (male, age 28).
I have never//wished//[to be in psychotherapy] as much as I did back then because I just knew it would help me (male, age 28).
3.1.5. Patients’ Psychotherapeutic Goals
I wanted to learn ways to work on specific memories, associations or experiences. They were always there anyway, but I never actively worked on them. It always felt very stagnant, and with psychotherapy, I learned to bring things into a flow (male, age 28).
I want to be able to go back to work and learn from my mistakes so that I do not slip into the old patterns again (female, age 37).
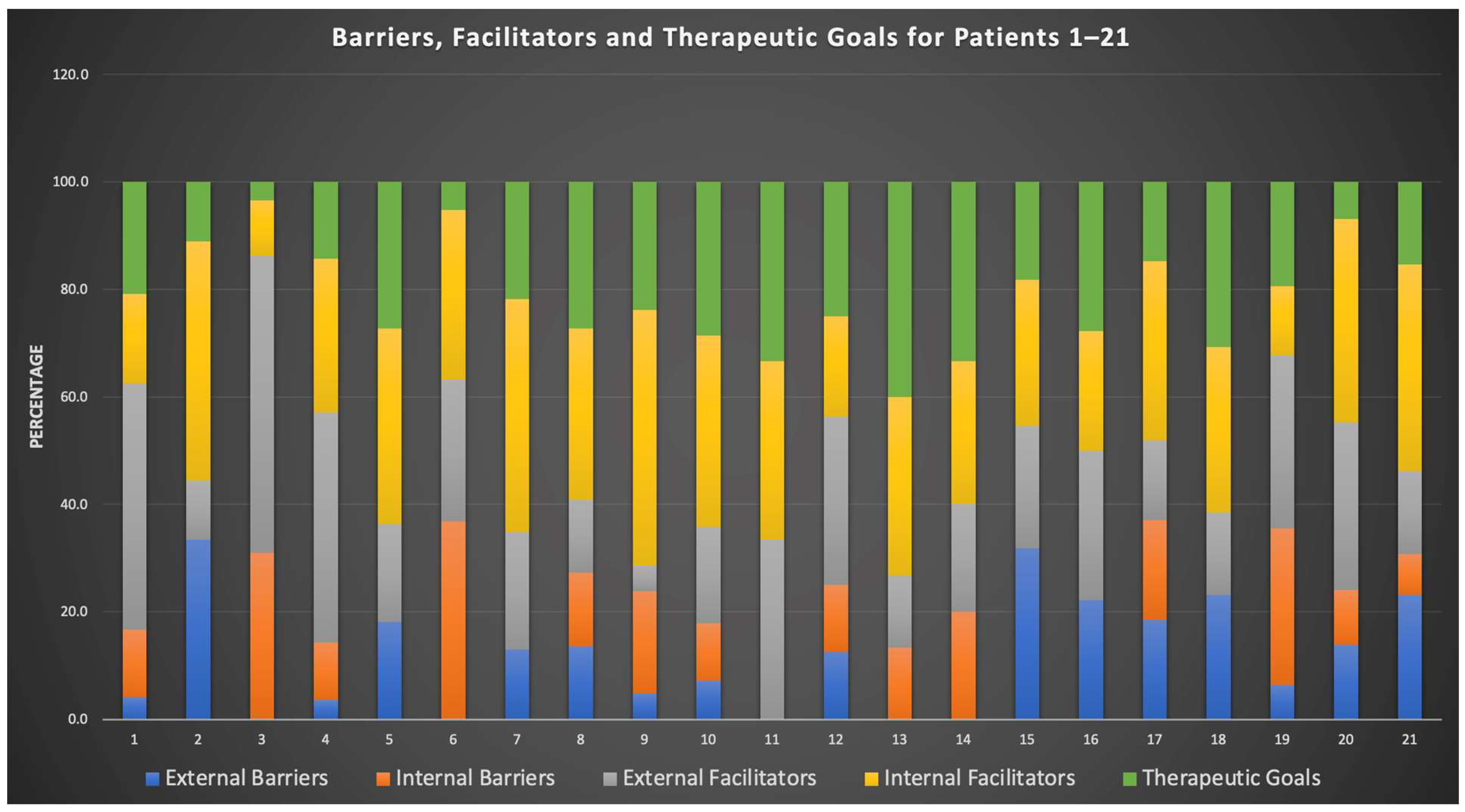
3.2. Distribution of Barriers, Facilitators and Psychotherapeutic Goals
3.2.1. Distribution per Case
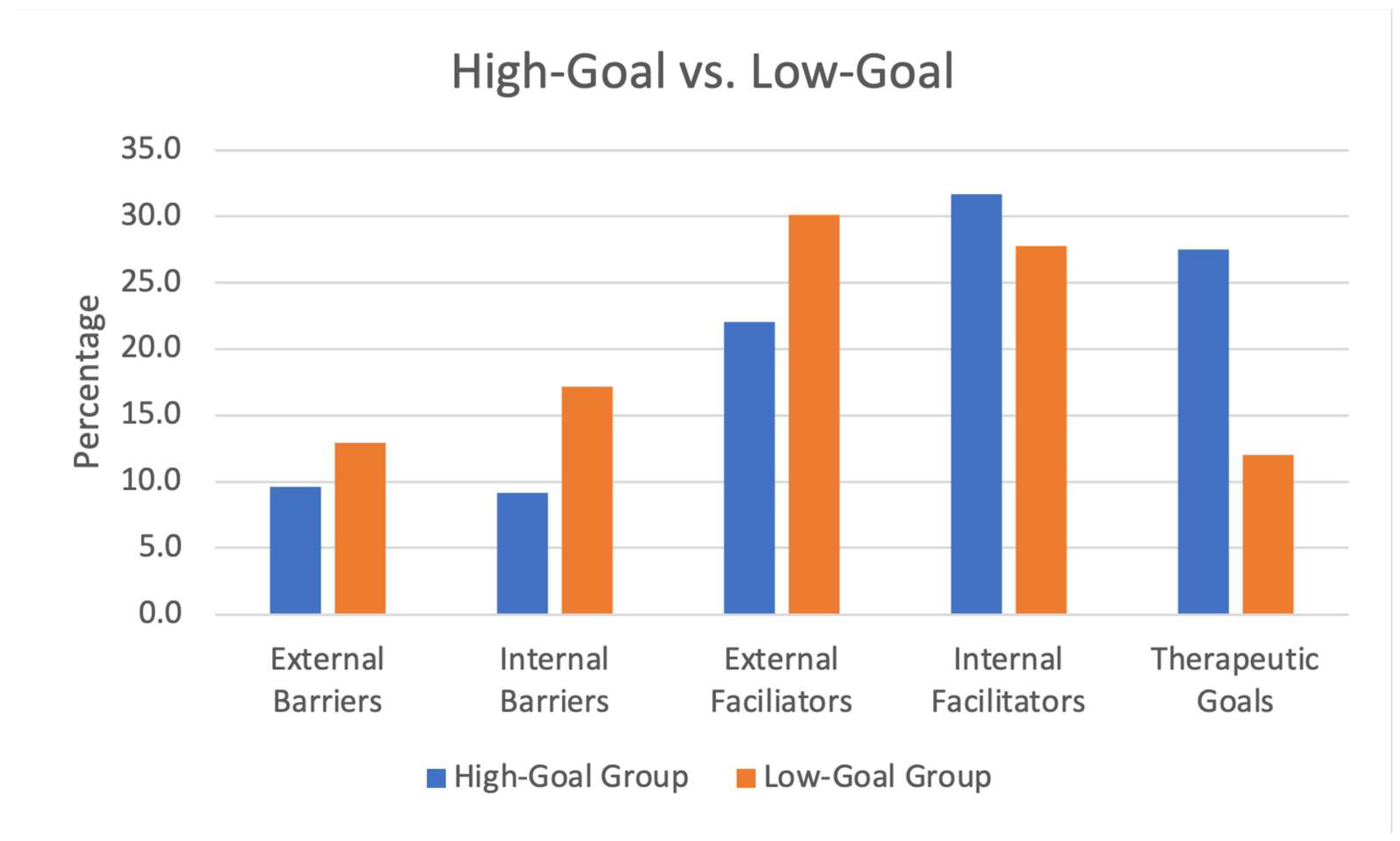
3.2.2. Distribution per Case in Two Groups
4. Discussion
4.1. Discussion of Categories
4.1.1. External Barriers
4.1.2. Internal Barriers
4.1.3. External Facilitators
4.1.4. Internal Facilitators
4.1.5. Psychotherapeutic Goals
4.2. Discussion of Distribution of Barriers, Facilitators and Psychotherapeutic Goals
4.3. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carbonell, Á.; Navarro-Pérez, J.J.; Mestre, M.V. Challenges and Barriers in Mental Healthcare Systems and Their Impact on the Family: A Systematic Integrative Review. Health Soc. Care Community 2020, 28, 1366–1379. [Google Scholar] [CrossRef] [Green Version]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Kavoor, A.R. The Missing Discourse on Mental Health of Psychiatrists during COVID-19. Aust. N. Z. J. Psychiatry 2021, 44, 325–326. [Google Scholar] [CrossRef]
- Doll, C.M.; Michel, C.; Rosen, M.; Osman, N.; Schimmelmann, B.G.; Schultze-Lutter, F. Predictors of Help-Seeking Behaviour in People with Mental Health Problems: A 3-Year Prospective Community Study. BMC Psychiatry 2021, 21, 432. [Google Scholar] [CrossRef] [PubMed]
- Plessen, Y.C.; Boeckle, M.; Liegl, G.; Leitner, A.; Schneider, A.; Preining, B.; Pieh, C. Bedarfsanalyse Für Ambulante Psychotherapie in Österreich. Demand for Psychotherapy in Austria. Psychol. Med. 2016, 27, 4–9. [Google Scholar]
- Sagerschnig, S.; Grabenhofer-Eggerth, A.; Kern, D.; Sator, M.; Zuba, M.; Mühlbacher, D. Inanspruchnahme von Psychotherapie und Psychiatrischer Rehabilitation im Kontext der Angebote; Ergebnisbericht: Vienna, Austria, 2018. [Google Scholar]
- Schigl, B.; Lerch, L.; Rohner, J. Erfahrungen von Wiener Psychotherapeut_innen Mit der Antragstellung und Bewilligungspraxis Der Krankenkassen. Psychother. Forum. 2021, 25, 44–53. [Google Scholar] [CrossRef]
- Löffler-Stastka, H.; Hochgerner, M. Versorgungswirksamkeit von Psychotherapie in Österreich. Psychopraxis Neuropraxis 2021, 24, 57–61. [Google Scholar] [CrossRef]
- Kantor, V.; Knefel, M.; Lueger-Schuster, B. Perceived Barriers and Facilitators of Mental Health Service Utilization in Adult Trauma Survivors: A Systematic Review. Clin. Psychol. Rev. 2017, 52, 52–68. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the Behavioral Model and Access to Medical Care: Does It Matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Pieh, C.; Budimir, S.; Probst, T. The Effect of Age, Gender, Income, Work, and Physical Activity on Mental Health during Coronavirus Disease (COVID-19) Lockdown in Austria. J. Psychosom. Res. 2020, 136, 110186. [Google Scholar] [CrossRef]
- Dale, R.; Budimir, S.; Probst, T.; Stippl, P.; Pieh, C. Mental Health during the COVID-19 Lockdown over the Christmas Period in Austria and the Effects of Sociodemographic and Lifestyle Factors. Int. J. Environ. Res. Public Health 2021, 18, 3679. [Google Scholar] [CrossRef]
- Shick Tryon, G. Goals and Psychotherapy Research. In Working with Goals in Psychotherapy and Counselling; Oxford University Press: Oxford, UK, 2018; pp. 87–110. [Google Scholar]
- Kantor, V.; Verginer, L.; Glück, T.M.; Knefel, M.; Lueger-Schuster, B. Barriers and Facilitators to Accessing Mental Health Services after Child Maltreatment in Foster Care: An Austrian Survivors’ Perspective. Eur. J. Trauma Dissociation 2022, 6, 100228. [Google Scholar] [CrossRef]
- Bance, S.; Links, P.S.; Strike, C.; Bender, A.; Eynan, R.; Bergmans, Y.; Hall, P.; O’Grady, J.; Antony, J. Help-Seeking in Transit Workers Exposed to Acute Psychological Trauma: A Qualitative Analysis. Work 2014, 48, 3–10. [Google Scholar] [CrossRef]
- Larsen, M.M.; Krohn, J.; Püschel, K.; Seifert, D. Experiences of Health and Health Care among Women Exposed to Intimate Partner Violence: Qualitative Findings from Germany. Health Care Women Int. 2014, 35, 359–379. [Google Scholar] [CrossRef]
- Gulliver, A.; Griffiths, K.M.; Christensen, H. Perceived Barriers and Facilitators to Mental Health Help-Seeking in Young People: A Systematic Review. BMC Psychiatry 2010, 113, 9. [Google Scholar] [CrossRef] [Green Version]
- Jankovic Gavrilovic, J.; Schützwohl, M.; Fazel, M.; Priebe, S. Who Seeks Treatment after a Traumatic Event and Who Does Not? A Review of Findings on Mental Health Service Utilization. J. Trauma Stress 2005, 18, 595–605. [Google Scholar] [CrossRef]
- Janzen, J. Therapy Management: Concept, Reality, Process. Med. Anthr. Q. 1987, 1, 68–84. [Google Scholar] [CrossRef]
- Pescosolido, B.A. Beyond Rational Choice: The Social Dynamics of How People Seek Help. Am. J. Sociol. 1992, 97, 1096–1138. [Google Scholar] [CrossRef]
- Rosenbaum, R.L.; Horowitz, M.J. Motivation for Psychotherapy: A Factorial and Conceptual Analysis. Psychother. Theory Res. Pract. 1983, 20, 346–354. [Google Scholar] [CrossRef]
- Michalak, J.; Holtforth, M.G. Where Do We Go from Here? The Goal Perspective in Psychotherapy. Clin. Psychol. Sci. Pract. 2006, 13, 346–365. [Google Scholar] [CrossRef]
- Pelletier, L.G.; Tuson, K.M.; Haddad, N.K. Client Motivation for Therapy Scale: A Measure of Intrinsic Motivation, Extrinsic Motivation, and a Motivation for Therapy. J. Pers. Assess 1997, 68, 414–435. [Google Scholar] [CrossRef]
- Lambert, M.J. The Efficacy and Effectiveness of Psychotherapy. In Bergin & Garfields Handbook of Psychotherapy and Behavior Change, 6th ed.; Bergin, A.E., Garfield, S.L., Eds.; Wiley: New York, NY, USA, 2013; pp. 169–2018. [Google Scholar]
- Ryan, R.M.; Lynch, M.F.; Vansteenkiste, M.; Deci, E.L. Motivation and Autonomy in Counseling, Psychotherapy, and Behavior Change: A Look at Theory and Practice 1ψ7. Couns. Psychol. 2011, 39, 193–260. [Google Scholar] [CrossRef]
- Shick Tryon, G.; Birch, S.E.; Verkuilen, J. Meta-Analyses of the Relation of Goal Consensus and Collaboration to Psychotherapy Outcome. Psychotherapy 2018, 55, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Bugas, J.; Silberschatz, G. How Patients Coach Their Therapists in Psychotherapy. Psychotherapy 2000, 37, 64–70. [Google Scholar] [CrossRef]
- Colorafi, K.J.; Evans, B. Qualitative Descriptive Methods in Health Science Research. HERD Health Environ. Res. Des. J. 2016, 9, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Mayring, P. Qualitative Forschungsdesigns in Der Psychologie. In Handbuch Qualitative Forschung in der Psychologie; Springer: Wiesbaden, Germany, 2018; pp. 1–15. [Google Scholar] [CrossRef]
- Bradshaw, C.; Atkinson, S.; Doody, O. Employing a Qualitative Description Approach in Health Care Research. Glob. Qual. Nurs. Res. 2017, 4, 2333393617742282. [Google Scholar] [CrossRef] [Green Version]
- Witzel, A. The Problem-Centered Interview. Forum Qual. Soz. Forum Qual. Soc. Res. 2000, 1, 142–150. [Google Scholar]
- Witzel, A. Das Problemzentrierte Interview. In Qualitative Forschung in der Psychologie: Grundfragen, Verfahrensweisen, Anwendungsfelder; Jüttemann, G., Ed.; Beltz Verlag: Weinheim, Germany, 1985; pp. 227–255. [Google Scholar]
- Doyle, L.; McCabe, C.; Keogh, B.; Brady, A.; McCann, M. An Overview of the Qualitative Descriptive Design within Nursing Research. J. Res. Nurs. 2020, 25, 443–455. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Content Analysis. Theoretical Foundation, Basic Procedures and Software Solution; SSOAR Open Acess Repos; GESIS–Leibniz Institute for the Social Sciences: Mannheim, Germany, 2014. [Google Scholar]
- Humer, E.; Schaffler, Y.; Schigl, B.; Probst, T. Process and Outcome of Psychotherapeutic Therapies under Practical Conditions in Austria. In Society of Psychotherapy Research, Proceedings of the 52nd Annual International SPR Meeting, Online Event, 23–26 June 2021; SPR: Heidelberg, Germany, 2021; Volume 5. [Google Scholar]
- Heidegger, K.E. The Situation of Psychotherapy in Austria 2017; Österreichischer Bundesverband für Psychotherapie (ÖBVP): Wien, Austria, 2017. [Google Scholar]
- Sagerschnig, S.; Nowotny, M. Psychotherapie, Klinische Psychologie, Gesundheitspsychologie, Musiktherapie. In Statistik Der Berufsgruppen 1991–2019; Ergebnisbericht: Vienna, Austria, 2020. [Google Scholar]
- Riedel, M. Modelle der Psychotherapieversorgung in Österreich; Institute for Advanced Study: Vienna, Austria, 2015. [Google Scholar]
- ATLAS.ti Scientific Software Development GmbH Atlas.Ti 2022. Available online: https://atlasti.com (accessed on 1 November 2022).
- Medjedović, I.; Witzel, A. Wiederverwendung Qualitativer Daten; Springer: New York, NY, USA, 2010; ISBN 9783531155715. [Google Scholar]
- Dezetter, A.; Briffault, X.; ben Lakhdar, C.; Kovess-Masfety, V. Costs and Benefits of Improving Access to Psychotherapies for CommonMental Disorders. J. Ment. Health Policy Econ. 2013, 16, 161–177. [Google Scholar]
- Blasco-Belled, A.; Tejada-Gallardo, C.; Fatsini-Prats, M.; Alsinet, C. Mental Health among the General Population and Healthcare Workers during the COVID-19 Pandemic: A Meta-Analysis of Well-Being and Psychological Distress Prevalence. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef]
- Mahmud, S.; Mohsin, M.; Dewan, M.N.; Muyeed, A. The Global Prevalence of Depression, Anxiety, Stress, and Insomnia Among General Population during COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Trends Psychol. 2022, 1–28. [Google Scholar] [CrossRef]
- Necho, M.; Tsehay, M.; Birkie, M.; Biset, G.; Tadesse, E. Prevalence of Anxiety, Depression, and Psychological Distress among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Soc. Psychiatry 2021, 67, 892–906. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, H.; Iosifidis, C.; Agha, M.; Aghaf, R. The Socio-Economic Implications of the Coronavirus Pandemic (COVID-19): A Review. Int. J. Surg. 2020, 78, 904–919. [Google Scholar] [CrossRef]
- Oddli, H.W.; Halvorsen, M.S. Experienced Psychotherapists’ Reports of Their Assessments, Predictions, and Decision Making in the Early Phase of Psychotherapy. Psychotherapy 2014, 51, 295–307. [Google Scholar] [CrossRef]
- Oddli, H.W.; McLeod, J.; Reichelt, S.; Rønnestad, M.H. Strategies Used by Experienced Therapists to Explore Client Goals in Early Sessions of Psychotherapy. Eur. J. Psychother. Couns. 2014, 16, 245–266. [Google Scholar] [CrossRef]
- von Below, C.; Werbart, A. Dissatisfied Psychotherapy Patients: A Tentative Conceptual Model Grounded in the Participants’ View. Psychoanal. Psychother. 2012, 26, 211–229. [Google Scholar] [CrossRef]
- Dezetter, A.; Vasiliadis, H.-M. The Economic Benefits of Improved Access to Psychotherapy: Two Studies. Quintessence 2014, 6, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Elliott, K.P.; Westmacott, R.; Hunsley, J.; Rumstein-Mckean, O.; Best, M. The Process of Seeking Psychotherapy and Its Impact on Therapy Expectations and Experiences. Clin. Psychol. Psychother. 2014, 22, 399–408. [Google Scholar] [CrossRef]
- Saunders, S.M. Applicants’ Experience of the Process of Seeking Therapy. Psychotherapy 1993, 30, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Horvath, A.O.; Symonds, B.D. Relation Between Working Alliance and Outcome in Psychotherapy: A Meta-Analysis. J. Couns. Psychol. 1991, 38, 139. [Google Scholar] [CrossRef]
- Horvath, A.O. The Therapeutic Relationship: From Transference to Alliance. J. Clin. Psychol. 2000, 56, 163–173. [Google Scholar] [CrossRef]
- Schigl, B.; Gahleitner, S.B. Fehler Machen—Aus Fehlern Lernen?—Perspektiven Zur Klassifizierung von Psychotherapeutischen Fehlern Und Dem Umgang Damit. Psychotherapiewissenschaft 2013, 3, 22–33. [Google Scholar]
- Schigl, B. Gender Als Notwendige Perspektive Psychotherapeutischen Handelns. Psychother. Forum 2019, 23, 18–24. [Google Scholar] [CrossRef]
- Leitner, A.; Märtens, M.; Koschier, A.; Gerlich, K.; Liegl, G.; Hinterwallner, H.; Schnyder, U. Patients’ Perceptions of Risky Developments during Psychotherapy. J. Contemp. Psychother. 2013, 43, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Keithly, L.J.; Samples, S.J.; Strupp, H.H. Patient Motivation as a Predictor of Process and Outcome in Psychotherapy. Psychother. Psychosom. 1980, 33, 87–97. [Google Scholar] [CrossRef]
- Greenberg, R.P.; Constantino, M.J.; Bruce, N. Are Patient Expectations Still Relevant for Psychotherapy Process and Outcome? Clin. Psychol. Rev. 2006, 26, 657–678. [Google Scholar] [CrossRef]
- Wollburg, E.; Braukhaus, C. Goal Setting in Psychotherapy: The Relevance of Approach and Avoidance Goals for Treatment Outcome. Psychother. Res. 2010, 20, 488–494. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content Analysis and Thematic Analysis: Implications for Conducting a Qualitative Descriptive Study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Gender | ||
| Female | 16 | 76.2 |
| Male | 5 | 23.8 |
| Age in years | ||
| 18–29 | 9 | 42.9 |
| 30–39 | 7 | 33.3 |
| 40–49 | 4 | 19.0 |
| 50–59 | 1 | 4.8 |
| Highest level of education | ||
| Secondary school | 4 | 19.0 |
| Apprenticeship | 1 | 4.8 |
| High school | 10 | 47.6 |
| University | 6 | 28.6 |
| Residence | ||
| ≤5000 inhabitants | 5 | 23.8 |
| ≥5000/≤25,000 inhabitants | 5 | 23.8 |
| ≥25,000 inhabitants | 11 | 52.4 |
| Therapy costs | ||
| Fully funded by insurance | 4 | 19.0 |
| Fully privately funded | 2 | 9.5 |
| Partial reimbursement through insurance | 15 | 71.4 |
| Orientation | ||
| Psychodynamic | 7 | 33.3 |
| Humanistic | 10 | 47.6 |
| Systemic | 3 | 14.3 |
| Behavioural | 1 | 4.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schaffler, Y.; Probst, T.; Jesser, A.; Humer, E.; Pieh, C.; Stippl, P.; Haid, B.; Schigl, B. Perceived Barriers and Facilitators to Psychotherapy Utilisation and How They Relate to Patient’s Psychotherapeutic Goals. Healthcare 2022, 10, 2228. https://doi.org/10.3390/healthcare10112228
Schaffler Y, Probst T, Jesser A, Humer E, Pieh C, Stippl P, Haid B, Schigl B. Perceived Barriers and Facilitators to Psychotherapy Utilisation and How They Relate to Patient’s Psychotherapeutic Goals. Healthcare. 2022; 10(11):2228. https://doi.org/10.3390/healthcare10112228
Chicago/Turabian StyleSchaffler, Yvonne, Thomas Probst, Andrea Jesser, Elke Humer, Christoph Pieh, Peter Stippl, Barbara Haid, and Brigitte Schigl. 2022. "Perceived Barriers and Facilitators to Psychotherapy Utilisation and How They Relate to Patient’s Psychotherapeutic Goals" Healthcare 10, no. 11: 2228. https://doi.org/10.3390/healthcare10112228