
Using Machine Learning to Explore the Crucial Factors of Assistive Technology Assessments: Cases of Wheelchairs
Abstract
:1. Introduction
“There are three assistive device assessors in our center, and their usual business volume is enormous. In addition to the main evaluation business, they also provide consultation, assistance in applying for subsidies, inspection, training, and follow-ups. After the launch of Long-term Care 2.0 two years ago, they must also perform fixed-point and on-site evaluation services. The manpower is obviously insufficient, and it is almost impossible to sustain all operations.”
2. Literature Discussion
2.1. Assistive Technology
2.2. Assistive Technology Services
2.3. Machine Learning for Healthcare Diagnosis
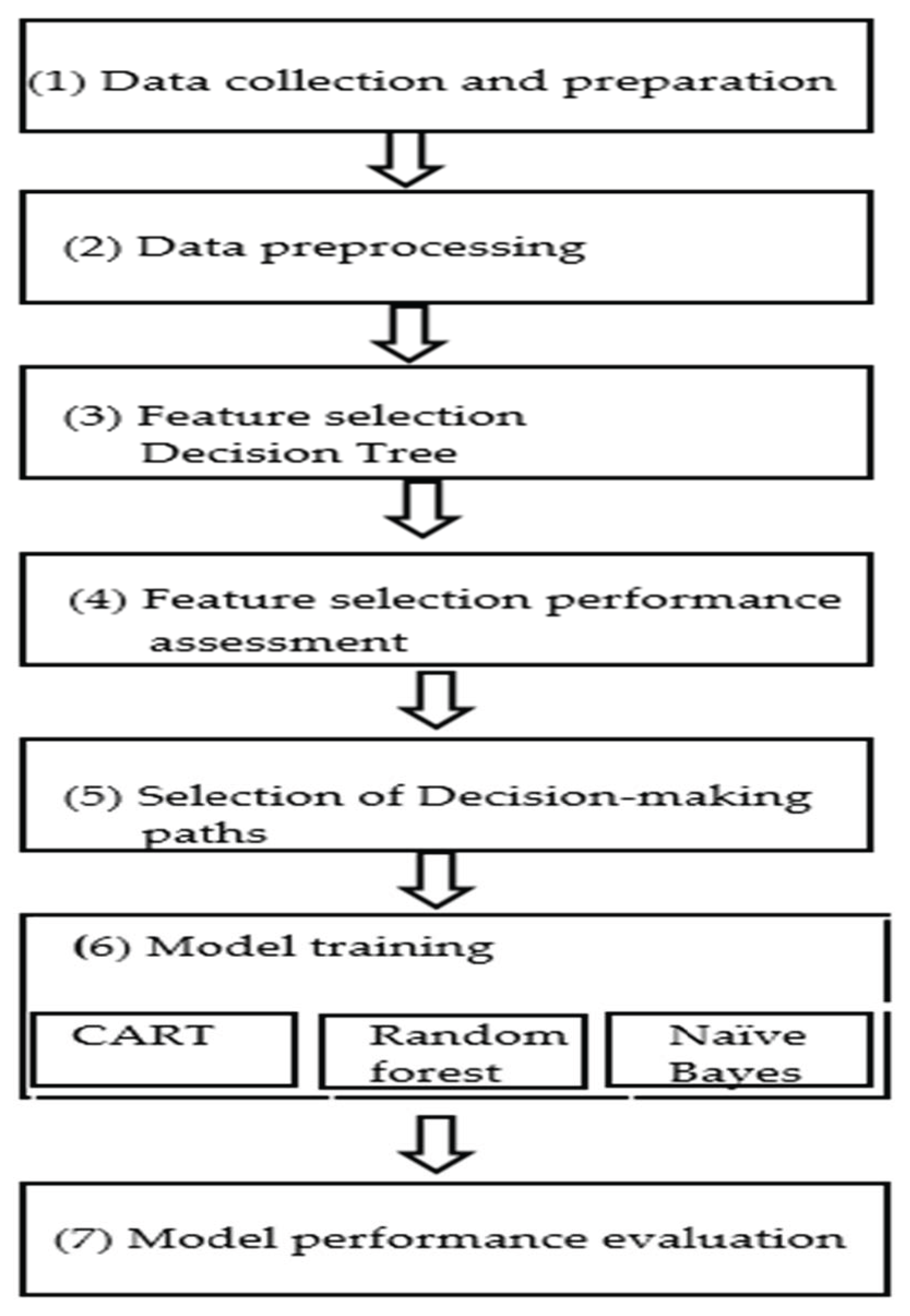
3. Research Method
3.1. Study Design
3.2. Data Collection
3.3. Machine Learning Algorithms
- Divide the training data into N sub-training sets through bagging to collect N decision trees.
- Carry out the growth of the decision tree. Each node is divided by randomly selected features, and each tree grows to be complete without pruning until all features are run out.
- Integrate the outputs of all classifiers and then perform a majority vote or average the outputs.
3.4. Performance Evaluation
- True positive (TP): The actual situation is a “positive category” and the predicted result is also a “positive category”.
- False negative (FN): The actual situation is a “positive category,” but the predicted result is a “negative category”.
- True negative (TN): The actual situation is a “negative category” and the prediction result is also a “negative category”.
- False positive (TP): The actual situation is a “negative category,” but the predicted result is a “positive category”.
4. Data Analysis
4.1. Data Preparation and Preprocessing
4.1.1. Missing Value Handling
- (1)
- Replace the blank value of “Without Handicap Handbook” because there is no new handicap classification for them.
- (2)
- Replace the blank values of “Hazard level,” “The pelvis status when in a sitting position”, and “The body will fall backward when not supported” with “normal”, because the above three characteristics belong to the second layer of problems. In this way, when the first-level question is “normal”, the second-level question does not need to be answered.
- (3)
- “Pelvis”, “Spine”, “Knee”, “Ankle”, “Cognitive ability”, “Judgment ability”, “Visual perception ability”, and “Emotion control”, associated with blank value were replaced with “cannot be measured”. According to evaluation experts, the case may be bedridden due to illness, unconsciousness, and other factors. Consequently, the evaluation cannot be performed.
4.1.2. Feature Deletion
4.1.3. Data Transformation
4.2. Decision Tree Analysis
- A.
- When the case “head movement control status” is abnormal, then, go to the left subtree:
- (1)
- A total of 99 out of 112 samples (88.4%) belong to “reclining and tilting wheelchairs”.
- (2)
- When the “cognitive ability” of the case was normal, 66 of the 71 samples (92.9%) belonged to “reclining and tilting wheelchairs”.
- (3)
- When the “cognitive ability” of the case was abnormal, 33 of the 41 samples (80.5%) belonged to “reclining and tilting wheelchairs”.
- B.
- When the case’s “head movement control status” is normal then, go to the right subtree:
- (1)
- A total of 98 of the 180 samples (54.4%) belonged to the “transit wheelchair”.
- (2)
- When the “age” of the case is less than 71 years old (the node is represented as 70.5), the GINI coefficient is 0.33, and it belongs to the “transit wheelchair” category.
- C.
- In cases where the “head movement control status” is normal and the “age” is higher than 71 years old:
- (1)
- When the “pelvic condition” of the case was abnormal, 35 of the 44 samples (79.5%) belonged to “reclining and tilting wheelchairs”.
- (2)
- When the “pelvic condition” of the case is normal, the GINI coefficient is 0.5, which belongs to “reclining and tilting wheelchairs”.
- D.
- When the case’s “head movement control status” is normal, “age” is higher than 71 years old, and “pelvic condition” is normal:
- (1)
- When the “judgment ability” of the case is abnormal, the GINI coefficient is 0.5, and it is mainly a “transit wheelchair”.
- (2)
- When the “judgment ability” of the case is normal, the GINI coefficient is 0.498, which mainly belongs to “reclining and tilting wheelchairs”.
- A.
- Transit wheelchair:
- B.
- Reclining and tilting wheelchairs:
- (1)
- “Head movement control” is abnormal. One possible explanation related to this is that when the head cannot maintain a fixed position naturally, the head would be tilted, which might cause physical discomfort or deformation in the long term. Therefore, the function of lying on the back or tilting is required to adjust the sitting posture.
- (2)
- “Head movement control” is normal, “age” is higher than 71 years old, and “pelvic condition” is abnormal. The reason, in terms of the above scenarios, is that if the pelvis is tilted forward, backward, or offset, it would lead to a poor sitting posture and the case would need “reclining and tilting wheelchairs” for assistance.
- C.
- Transit wheelchair or reclining and tilting wheelchairs:
4.3. Model Comparison
4.4. Application Interface Design for Users
5. Conclusions and Research Suggestions
5.1. Conclusions
5.2. Research Suggestions
5.2.1. Data
- (1)
- This study only analyzed 365 diagnostic records from a specific assistive device center. Although the minimum number of samples for model classification is reached, future studies should add more samples so as to enhance the model’s classification accuracy and more completely assess generalizability of findings.
- (2)
- In a similar sense, the study deleted some features of body size measurement. Future studies should not only consider users’ convenience but also combine these features with a LINE BOT to allow the users or the users’ family to report their situation.
- (3)
- From the viewpoint of feature selection, the researchers should keep in mind to the correspondence table between the new system (8 categories) and the old system (16 categories) of disability categories and codes has been amended.
- (4)
- This study is only for the prediction and classification of “transit wheelchairs” and “reclining and tilting wheelchairs”. With numerous calls for wheelchairs in an “aging society”, further research can include other wheelchair types to enrich the precision of results.
5.2.2. Application
- (1)
- At its most basic, when the patient is ready to be discharged from the hospital, the hospital can physically provide the patient to use the assessment assistive device, LINE BOT, on his/her mobile phone. Essentially, this enables the patient to learn the type of assistive device they need during the referral of the assistive device center at the hospital and notify the assistive device center to prepare for follow-up assessment services.
- (2)
- When calling the assistive device center for inquiry, the case can be reminded to join the LINE BOT with his/her mobile phone for preliminary self-assessment during telephone consultation. Moreover, the QR Code of the LINE BOT can be added to the webpage of the assistive devices center, and provide case scanning in order to link LINE BOT in a cyberspace environment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (Feature) | Data Type | Field Number |
|---|---|---|
| Assistive device specification configuration suggestion (target value) | Category type | 3-1-A |
| The old system—disability handbook category | Class type (multi-class) | 1-7-2 |
| The new system—classification system for physical and physical disabilities | Class type (multi-class) | 1-7-3 |
| Handicap level | Isomorphism | 1-8 |
| Purpose of use and activity requirements | Class type (multi-class) | 2-1 |
| Assistive device usage environment | Class type (multi-class) | 2-2 |
| Assistive device control capabilities | Category type | 2-3 |
| Current wheelchair assistive device | Numerical type | 2-4 |
| Diagnostics related to assistive device | Class type (multi-class) | 2-5-A |
| Height | Numerical type | 2-5-b1 |
| Weight | Numerical type | 2-5-b2 |
| Elbow height | Numerical type | 2-5-B-11 |
| Hip to knee length | Numerical type | 2-5-B-4 |
| Knee height | Numerical type | 2-5-B-5 |
| Knee angle | Numerical type | 2-5-B-1 |
| Popliteal angle | Numerical type | 2-5-B-2 |
| Shoulder width | Numerical type | 2-5-B-10 |
| Chest width | Numerical type | 2-5-B-9 |
| Hip width | Numerical type | 2-5-B-3 |
| Head height | Numerical type | 2-5-B-8 |
| Shoulder height | Numerical type | 2-5-B-7 |
| High subscapular angle | Numerical type | 2-5-B-6 |
| Sitting balance | Category type | 2-5-c1 |
| Seated balance—with support in place, the body is clearly oriented | Category type | 2-5-c2 |
| Pelvis | Category type | 2-5-d1 |
| Pelvis—the pelvis in the sitting position | Category type | 2-5-d2 |
| Body parts—spine | Category type | 2-5-E |
| Body parts—head movement controls | Category type | 2-5-F |
| Body parts—shoulders | Category type | 2-5-G |
| Body parts—hip | Category type | 2-5-H |
| Body parts—knees | Category type | 2-5-I |
| Body parts—ankle | Category type | 2-5-J |
| Cognitive ability | Category type | 2-5-K |
| Visual perception ability | Category type | 2-5-L |
| Judgment | Category type | 2-5-M |
| Emotional control | Category type | 2-5-N |
| Skin sensing | Category type | 2-5-O |
| Pressure ulcers—grading | Isomorphism | 2-5-P |
| Operating skills—activate/deactivate break | Category type | 2-5-Q-1 |
| Operating skills—execution, forward, backward, steering, and stopping on levels and slopes | Category type | 2-5-Q-2 |
| Operation skills—enter and exit the elevator within the door opening time limit by forward and backward | Bollinger pattern | 2-5-Q-3 |
| Operational skills—separate and pass safely by yourself | Bollinger pattern | 2-5-Q-4 |
| Operational skills—stably push forward 5 m in a narrow pass | Bollinger pattern | 2-5-Q-5 |
| Operational skills—going in and out of the car or between toilets and beds | Category type | 2-5-Q-6 |
| Operation skills—moving up and down 10 cm steps | Category type | 2-5-Q-7 |
References
- United Nations. World Population Prospects 2019: Highlights; Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2019. [Google Scholar]
- Ministry of Health and Welfare. Long-Term Care Ten-Year Plan 2.0 (106–115 Years), Approved Version. 2018. Available online: https://1966.gov.tw/LTC/cp-4001-42414-201.html (accessed on 31 August 2022).
- Austin, V.; Holloway, C.; Vermehren, I.O.; Dumbuya, A.; Barbareschi, G.; Walker, J. “Give us the chance to be part of you, we want our voices to be heard”: Assistive technology as a mediator of participation in (formal and informal) citizenship activities for persons with disabilities who are slum dwellers in freetown, Sierra Leone. Int. J. Environ. Res. Public Health 2021, 18, 5547. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Eide, A.H.; Pryor, W.; Khasnabis, C.; Borg, J. Measuring self-reported access to assistive technology using the WHO rapid assistive technology assessment (rATA) questionnaire: Protocol for a multi-country study. Int. J. Environ. Res. Public Health 2021, 18, 13336. [Google Scholar] [CrossRef] [PubMed]
- The Social Welfare Department. 108 Annual Assistive Services Aggregation Analysis Report. 2020. Available online: https://newrepat.sfaa.gov.tw/home/download?conditions%5bcategory.id%5d=2c90e4c76705ab7f01671535b6e40d29 (accessed on 31 August 2022).
- Lin, M.J. Application of Decision Tree in the Assessment of Electronic Wheelchairs for Persons with Disabilities. Master’s Thesis, Department of Industrial Management, National Taiwan University of Science and Technology, Taipei, Taiwan, 2012. [Google Scholar]
- Ndlovu, S. Provision of assistive technology for students with disabilities in South African Higher Education. Int. J. Environ. Res. Public Health 2021, 18, 3892. [Google Scholar] [CrossRef] [PubMed]
- The Social Welfare Department. What is Assistive Technology? 2018. Available online: https://newrepat.sfaa.gov.tw/home/question/detail/2c90e4c76633b9e0016633c8cc0c26cc (accessed on 31 August 2022).
- Lin, S.M. An Overview of Assistive Technology Equipment and Services: An Introduction to Relevant Regulations. 2004. Available online: http://sencir.spc.ntnu.edu.tw/site/c_file/a_download/t_key/3876 (accessed on 31 August 2022).
- Cook, A.M.; Polgar, J.M. Assistive Technologies-e-Book: Principles and Practice, 4th ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Fatima, M.; Pasha, M. Survey of machine learning algorithms for disease diagnostic. J. Intell. Learn. Syst. Appl. 2017, 9, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Bhagat, A.; Sharma, A.; Chettri, S. Machine learning based sentiment analysis for text messages. Int. J. Comput. Technol. 2020, 7, 2348–6090. [Google Scholar]
- Keerthi, S.S.; Lin, C.J. Asymptotic behaviors of support vector machines with Gaussian kernel. Neural Comput. 2003, 15, 1667–1689. [Google Scholar] [CrossRef] [Green Version]
- Sarwar, A.; Sharma, V. Intelligent Naïve Bayes approach to diagnose diabetes Type-2. Int. J. Comput. Appl. 2012, 3, 14–16. [Google Scholar]
- Jain, D.; Singh, V. Feature selection and classification systems for chronic disease prediction: A review. Egypt. Inform. J. 2018, 19, 179–189. [Google Scholar] [CrossRef]
- Hashi, E.K.; Zaman, M.S.U.; Hasan, M.R. An Expert Clinical Decision Support System to Predict Disease Using Classification Techniques. In Proceedings of the 2017 International Conference on Electrical, Computer and Communication Engineering, Cox’s Bazar, Bangladesh, 16–18 February 2017. [Google Scholar]
- Vermeir, P.; Degroote, S.; Vandijck, D.; Van Tiggelen, H.; Peleman, R.; Verhaeghe, R.; Mariman, A. The patient perspective on the effects of medical record accessibility: A systematic review. Acta Clin. Belg. 2017, 72, 186–194. [Google Scholar] [CrossRef]
- Yan, Z.; Wang, T.; Chen, Y.; Zhang, H. Knowledge sharing in online health communities: A social exchange theory perspective. Inf. Manag. 2016, 53, 643–653. [Google Scholar] [CrossRef]
- Tufail, A.B.; Ullah, I.; Khan, W.U.; Asif, M.; Ahmad, I.; Ma, Y.K.; Khan, R.; Ali, M. Diagnosis of diabetic retinopathy through retinal fundus images and 3D convolutional neural networks with limited number of samples. Wirel. Commun. Mob. Comput. 2021, 2021, 6013448. [Google Scholar] [CrossRef]
- Ahmad, I.; Ullah, I.; Khan, W.U.; Ur Rehman, A.; Adrees, M.S.; Saleem, M.Q.; Cheikhrouhou, O.; Hamam, H.; Shafiq, M. Efficient algorithms for e-healthcare to solve multi-object fuse detection problem. J. Healthc. Eng. 2021, 2021, 9500304. [Google Scholar] [CrossRef]
- Sathyadevi, G. Application of CART algorithm in Hepatitis disease diagnosis. In Proceedings of the 2011 International Conference on Recent Trends in Information Technology, MIT, Anna University, Chennai, India, 3–5 June 2011. [Google Scholar]
- Saxena, K.; Sharma, R. Efficient heart disease prediction system using decision tree. In Proceedings of the International Conference on Computing, Communication & Automation, MIT, Anna University, Chennai, India, 3–5 June 2015. [Google Scholar]
- Maji, S.; Arora, S. Decision tree algorithms for prediction of heart disease. Inf. Commun. Technol. Compet. Strateg. 2019, 40, 447–454. [Google Scholar]
- Jaing, W.L. A Study on the Choice on Ward Types Using Decision Tree: An Example of Regional Hospital. Master’s Thesis, Department of Information Management, Natinal Chung Cheng University, Chiayi, Taiwan, 2019. [Google Scholar]
- Mariana, B.; Lucian, D. Random forest in remote sensing: A review of applications and future directions ISPRS. J. Photogramm. Remote Sens. 2016, 114, 24–31. [Google Scholar]
- Azar, A.T.; Elshazly, H.I.; Hassanien, A.E.; Elkorany, A.M. A random forest classifier for Lymph diseases. Comput. Methods Programs Biomed. 2014, 113, 465–473. [Google Scholar] [CrossRef]
- Nguyen, C.; Wang, Y.; Nguyen, H.N. Random forest classifier combined with feature selection for breast cancer diagnosis and prognostic. J. Biomed. Sci. Eng. 2013, 6, 551–560. [Google Scholar] [CrossRef]
- Shahzad, A.; Zafar, B.; Ali, N.; Jamil, U.; Alghadhban, A.J.; Assam, M.; Ghamry, N.A.; Eldin, E.T. COVID-19 vaccines related user’s response categorization using machine learning techniques. Computation 2022, 10, 141. [Google Scholar] [CrossRef]
- Jović, A.; Brkić, K.; Bogunović, N. A review of feature selection methods with applications. In Proceedings of the 38th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 25–29 May 2015. [Google Scholar] [CrossRef]
- Safavian, S.R.; Landgrebe, D. A survey of decision tree classifier methodology. IEEE Trans. Syst. Man Cybern. 1991, 21, 660–674. [Google Scholar] [CrossRef] [Green Version]
- Charbuty, B.; Abdulazeez, A. Classification based on decision tree algorithm for machine learning. J. Appl. Sci. Technol. Trends 2021, 2, 20–28. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Borgelt, C.; Gebhardt, J. A naive bayes style possibilistic classifier. In Proceedings of the 7th European Congress on Intelligent Techniques and Soft Computing (EUFIT’99), Aachen, Germany, 13–16 September 1999. [Google Scholar]
- Latif, A.; Rasheed, A.; Sajid, U.; Ahmed, J.; Ali, N.; Ratyal, N.I.; Zafar, B.; Dar, S.H.; Sajid, M.; Khalil, T. Content-based image retrieval and feature extraction: A comprehensive review. Math. Probl. Eng. 2019, 2019, 9658350. [Google Scholar] [CrossRef]
- Shabbir, A.; Ali, N.; Ahmed, J.; Zafar, B.; Rasheed, A.; Sajid, M.; Ahmed, A.; Dar, S.H. Satellite and scene image classification based on transfer learning and fine tuning of ResNet50. Math. Probl. Eng. 2021, 2021, 5843816. [Google Scholar] [CrossRef]
- Rodriguez, J.D.; Perez, A.; Lozano, J.A. Sensitivity analysis of k-fold cross validation in prediction error estimation. IEEE Trans. Pattern Anal. Mach. Intell. 2009, 32, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Bengio, Y.; Grandvalet, Y. No unbiased estimator of the variance of k-fold cross-validation. J. Mach. Learn. Res. 2004, 5, 1089–1105. [Google Scholar]
- He, H.; Garcia, E.A. Learning from imbalanced data. IEEE Trans. Knowl. Data Eng. 2009, 21, 1263–1284. [Google Scholar]
- López, V.; Fernández, A.; García, S.; Palade, V.; Herrera, F. An insight into classification with imbalanced data: Empirical results and current trends on using data intrinsic characteristics. Inf. Sci. 2013, 250, 113–141. [Google Scholar] [CrossRef]
- Beleites, C.; Neugebauer, U.; Bocklitz, T.; Krafft, C.; Popp, J. Sample size planning for classification models. Anal. Chim. Acta 2013, 760, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Torkzadeha, G.; Cios, K.J.; Pflughoefta, K.A. Inductive machine learning for instrument development. Inf. Manag. 1996, 31, 47–55. [Google Scholar] [CrossRef]




| Before Encoding | After Encoding |
|---|---|
| Daily life | 1 |
| Medical | 10 |
| School | 11 |
| Work | 100 |
| Leisure activities | 101 |
| Feature Selection | Accuracy | “Transit Wheelchair” Recall Rate | “Reclining and Tilting Wheelchairs” Recall Rate | |
|---|---|---|---|---|
| CART | yes | 70.70% | 63.70% | 74.20% |
| no | 68.50% | 56% | 74.60% | |
| Naïve Bayes | yes | 72.00% | 71.20% | 72.60% |
| no | 68.70% | 45.40% | 80.10% | |
| Random forest | yes | 70.90% | 72.00% | 70.50% |
| no | 73.20% | 68.70% | 75.40% |
| Decision Tree Node (Feature) | Question | Reply Option |
|---|---|---|
| Head movement control | Q1: Can the head be maintained in a fixed position (sitting position)? | Yes: normal head movement control No: abnormal head movement control |
| Cognitive ability | Q2: Can a wheelchair user leave without paying when they go shopping? (If the wheelchair user is confused or unable to answer, please write “Yes”) | Yes: poor cognitive and judgment skills No: normal cognitive and judgment skills |
| Judgment ability | ||
| Age of 71 | Q3: Is the wheelchair user over 71 years old (inclusive)? | Yes: age over 71 No: younger than 71 years old |
| Pelvis status | Q4: Which of the following pictures shows the sitting habits of the wheelchair user, A or B or C? | A: pelvis normal B: posterior pelvic tilt, abnormal C: anterior pelvic tilt, abnormal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, K.-T.; Ping, C.-H. Using Machine Learning to Explore the Crucial Factors of Assistive Technology Assessments: Cases of Wheelchairs. Healthcare 2022, 10, 2238. https://doi.org/10.3390/healthcare10112238
Fang K-T, Ping C-H. Using Machine Learning to Explore the Crucial Factors of Assistive Technology Assessments: Cases of Wheelchairs. Healthcare. 2022; 10(11):2238. https://doi.org/10.3390/healthcare10112238
Chicago/Turabian StyleFang, Kwo-Ting, and Ching-Hsiang Ping. 2022. "Using Machine Learning to Explore the Crucial Factors of Assistive Technology Assessments: Cases of Wheelchairs" Healthcare 10, no. 11: 2238. https://doi.org/10.3390/healthcare10112238