
Clinical and Psychological Variables in Female Patients with Cervical Syndromes: A Cross-Sectional and Correlational Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
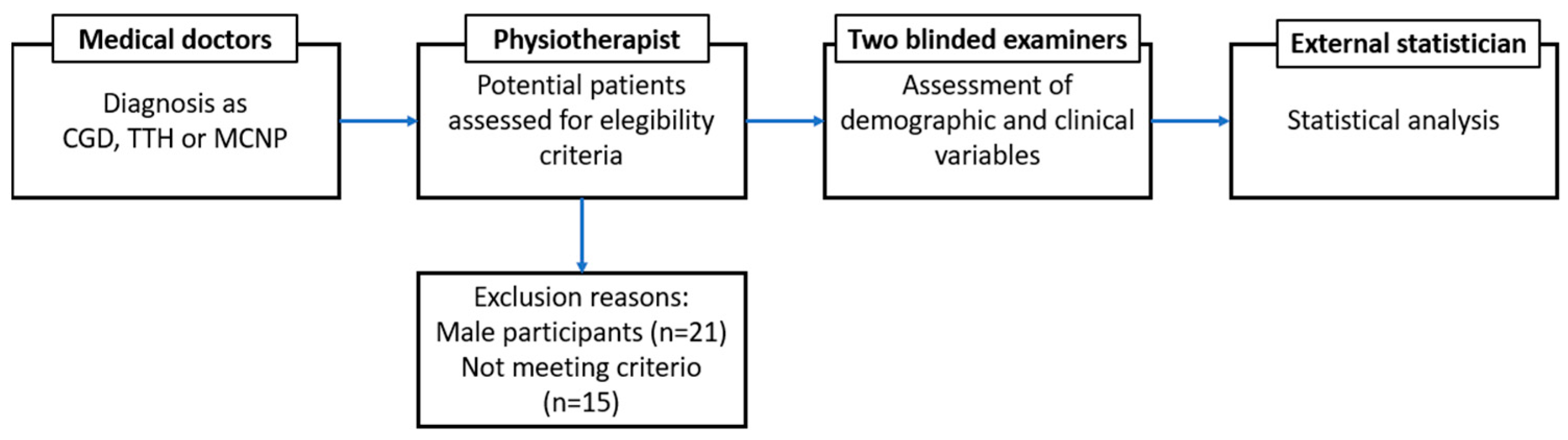
2.2. Participants
2.3. Procedure
2.4. Outcome Variables
2.4.1. Pain Intensity
2.4.2. Cervical ROM
2.4.3. Psychological Distress
2.4.4. Kinesiophobia
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fejer, R.; Kyvik, K.O.; Hartvigsen, J. The prevalence of neck pain in the world population: A systematic critical review of the literature. Eur. Spine. J. 2006, 15, 834–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Burden of Disease Collaborators. The state of US health, 1990-2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, B.K.; Jensen, R.; Schroll, M.; Olesen, J. Epidemiology of headache in a general population—A prevalence study. J. Clin. Epidemiol. 1991, 44, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Blanpied, P.R.; Gross, A.R.; Elliott, J.M.; Devaney, L.L.; Clewley, D.; Walton, D.M.; Sparks, C.; Robertsonet, E.K. Neck Pain, Revision 2017. J. Orthop. Sport. Phys. Therapy. Mov. Sci. Media 2017, 47, A1–A83. [Google Scholar] [CrossRef] [Green Version]
- Croft, P.R.; Lewis, M.; Papageorgiou, A.C.; Thomas, E.; Jayson, M.I.; Macfarlane, G.J.; Silman, A.J. Risk factors for neck pain: A longitudinal study in the general population. Pain 2001, 3, 317–325. [Google Scholar] [CrossRef]
- Liu, R.; Kurihara, C.; Tsai, H.T.; Silvestri, P.J.; Bennett, M.I.; Pasquina, P.F.; Cohen, S.P. Classification and Treatment of Chronic Neck Pain: A Longitudinal Cohort Study. Reg. Anesth. Pain Med. 2017, 42, 52–61. [Google Scholar] [CrossRef]
- Griggs, R.K.L.; Cook, J.; Gargan, M.; Bannister, G.; Amirfeyz, R. Mid-term follow-up of whiplash with Bournemouth Questionnaire: The significance of the initial depression to pain ratio. J. Back. Musculoskelet. Rehabil. 2015, 28, 443–446. [Google Scholar] [CrossRef]
- Robinson, J.P.; Burwinkle, T.; Turk, D.C. Perceived and actual memory, concentration, and attention problems after whiplash-associated disorders (grades I and II): Prevalence and predictors. Arch. Phys. Med. Rehabil. 2007, 88, 774–779. [Google Scholar] [CrossRef]
- Treleaven, J. Sensorimotor disturbances in neck disorders affecting postural stability, head and eye movement control. Man. Ther. 2008, 13, 2–11. [Google Scholar] [CrossRef]
- Blozik, E.; Laptinskaya, D.; Herrmann-Lingen, C.; Schaefer, H.; Kochen, M.M.; Himmel, W.; Scherer, M. Depression and anxiety as major determinants of neck pain: A cross-sectional study in general practice. BMC Musculoskelet. Disord. 2009, 10, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhauser, H.K.; Radtke, A.; von Brevern, M.; Lezius, F.; Feldmann, M.; Lempert, T. Burden of dizziness and vertigo in the community. Arch. Intern. Med. 2008, 168, 2118–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [CrossRef] [PubMed] [Green Version]
- Reid, S.; Rivett, D.; Katekar, M.; Callister, R. Sustained natural apophyseal glides (SNAGs) are an effective treatment for cervicogenic dizziness. Man. Ther. 2008, 13, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Trujillo, I.; López-De-Andrés, A.; del Barrio, J.L.; Hernández-Barrera, V.; Valero-De-Bernabé, M.; Jiménez-García, R. Gender Differences in the Prevalence and Characteristics of Pain in Spain: Report from a Population-Based Study. Pain Med. 2019, 20, 2349–2359. [Google Scholar] [CrossRef] [PubMed]
- Vural, M.; Karan, A.; Gezer, I.A.; Çalışkan, A.; Atar, S.; Aydın, F.Y.; Benlidayı, C.; Gökşen, A.; Doğan, K.; Karacan, G.; et al. Prevalence, etiology, and biopsychosocial risk factors of cervicogenic dizziness in patients with neck pain: A multi-center, cross-sectional study. Turk. J. Phys. Med. Rehabil. 2021, 67, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Bijur, P.E.; Silver, W.; Gallagher, E.J. Reliability of the visual analog scale for measurement of acute pain. Acad. Emerg. Med. 2001, 8, 1153–1157. [Google Scholar] [CrossRef]
- Strimpakos, N. The assessment of the cervical spine. Part 1: Range of motion and proprioception. J. Bodyw. Mov. Ther. 2011, 15, 114–124. [Google Scholar] [CrossRef] [Green Version]
- Benatto, M.T.; Bevilaqua-Grossi, D.; Carvalho, G.F.; Bragatto, M.M.; Pinheiro, C.F.; Straceri Lodovichi, S.; Dach, F.; Fernández-De-Las-Peñas, C.; Florencio, L.L. Kinesiophobia Is Associated with Migraine. Pain Med. 2019, 20, 846–851. [Google Scholar] [CrossRef]
- Nazari, G.; Bobos, P.; Billis, E.; MacDermid, J.C. Cervical flexor muscle training reduces pain, anxiety, and depression levels in patients with chronic neck pain by a clinically important amount: A prospective cohort study. Physiother. Res. Int. 2018, 23, e1712. [Google Scholar] [CrossRef]
- Javdaneh, N.; Saeterbakken, A.H.; Shams, A.; Barati, A.H. Pain Neuroscience Education Combined with Therapeutic Exercises Provides Added Benefit in the Treatment of Chronic Neck Pain. Int. J. Environ. Res. Public Health 2021, 18, 8848. [Google Scholar] [CrossRef] [PubMed]
- Puca, F.; Genco, S.; Prudenzano, M.P.; Savarese, M.; Bussone, G.; Amico, D.; Cerbo, R.; Gala, C.; Coppola, M.T.; GalIaiet, V.; et al. Psychiatric comorbidity and psychosocial stress in patients with tension-type headache from headache centers in Italy. The Italian Collaborative Group for the Study of Psychopathological Factors in Primary Headaches. Cephalalgia 1999, 19, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Probst, T.; Dinkel, A.; Schmid-Mühlbauer, G.; Radziej, K.; Limburg, K.; Pieh, C.; Lahmann, C. Psychological distress longitudinally mediates the effect of vertigo symptoms on vertigo-related handicap. J. Psychosom. Res. 2017, 93, 62–68. [Google Scholar] [CrossRef]
- Eckhardt-Henn, A.; Breuer, P.; Thomalske, C.; Hoffmann, S.O.; Hopf, H.C. Anxiety disorders and other psychiatric subgroups in patients complaining of dizziness. J. Anxiety Disord. 2003, 17, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, K.A.; Stensland, M.; Lipchik, G.L.; Hill, K.R.; O’Donnell, F.S.; Cordingley, G. Psychosocial correlates and impact of chronic tension-type headaches. Headache 2000, 40, 3–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Tousignant, M.; Breton, A.M. Range of Motion (CROM) Device for Rotational Range of Motion on Healthy. J. Orthop. Sport Phys. Therapy 2006, 36, 242–248. [Google Scholar] [CrossRef]
- Fletcher, J.P.; Bandy, W.D. Intrarater reliability of CROM measurement of cervical spine active range of motion in persons with and without neck pain. J. Orthop. Sport. Phys. Therapy 2008, 38, 640–645. [Google Scholar] [CrossRef]
- Rishi, P.; Rishi, E.; Maitray, A.; Agarwal, A.; Nair, S.; Gopalakrishnan, S. Hospital anxiety and depression scale assessment of 100 patients before and after using low vision care: A prospective study in a tertiary eye-care setting. Indian J. Opthalmology 2017, 65, 1203–1208. [Google Scholar] [CrossRef]
- Zigmond, A.; Snaith, R. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef]
- Nie, N.H. SPSS: Statistical Package for the Social Sciences; McGraw-Hill: New York, NY, USA, 1975; 675p. [Google Scholar]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sport. Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Bernal-Utrera, C.; Gonzalez-Gerez, J.J.; Anarte-Lazo, E.; Rodriguez-Blanco, C. Manual therapy versus therapeutic exercise in non-specific chronic neck pain: A randomized controlled trial. Trials 2020, 21, 682. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Uribarren, A.; Rodriguez-Sanz, J.; López-de-Celis, C.; Pérez-Guillen, S.; Tricás-Moreno, J.M.; Cabanillas-Barea, S. Short-term effects of the traction-manipulation protocol in dizziness intensity and disability in cervicogenic dizziness: A randomized controlled trial. Disabil Rehabil. 2021, 44, 3601–3609. [Google Scholar] [CrossRef] [PubMed]
- Tejera, D.M.; Beltran-Alacreu, H.; Cano-De-La-Cuerda, R.; Hernández, R.C.-D.J.V.L.; Martín-Pintado-Zugasti, A.; Calvo-Lobo, C.; Gil-Martínez, C.C.-L.A.; Fernández-Carnero, J. Effects of virtual reality versus exercise on pain, functional, somatosensory and psychosocial outcomes in patients with non-specific chronic neck pain: A randomized clinical trial. Int. J. Environ. Res. Public Health 2020, 17, 5950. [Google Scholar] [CrossRef]
- Micarelli, A.; Viziano, A.; Granito, I.; Micarelli, R.X.; Augimeri, I.; Alessandrini, M. Temporomandibular disorders and cervicogenic dizziness: Relations between cervical range of motion and clinical parameters. Cranio 2020, 40, 348–357. [Google Scholar] [CrossRef]
- Micarelli, A.; Viziano, A.; Augimeri, I.; Micarelli, B.; Capoccia, D.; Alessandrini, M. Diagnostic route of cervicogenic dizziness: Usefullness of posturography, objective and subjective testing implementation and their correlation. Disabil. Rehabil. 2019, 43, 1730–1737. [Google Scholar] [CrossRef] [PubMed]
- Benito-González, E.; Ceña, M.P.; Fernández-Muñoz, J.J.; Castaldo, M.; Wang, K.; Catena, A.; Arendt-Nielsen, L.; Fernández-De-Las-Peñas, C. Variables associated with sleep quality in chronic tension-type headache: A cross-sectional and longitudinal design. PLoS ONE 2018, 13, e0197381. [Google Scholar] [CrossRef] [Green Version]
- Grande-Alonso, M.; Moral Saiz, B.; Mínguez Zuazo, A.; Lerma Lara, S.; la Touche, R. Biobehavioural analysis of the vestibular system and posture control in patients with cervicogenic dizziness. A cross-sectional study. Neurologia 2018, 33, 121–128. [Google Scholar] [CrossRef]
- Minguez-Zuazo, A.; Grande-Alonso, M.; Saiz, B.M.; la Touche, R.; Lara, S.L. Therapeutic patient education and exercise therapy in patients with cervicogenic dizziness: A prospective case series clinical study. J. Exerc. Rehabi. 2016, 12, 216–225. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; Bartrina-Rodríguez, I.; Suso-Martí, L.; la Touche, R.; Ferrer-Peña, R. Association between somatosensory, motor and psychological variables by levels of disability in patients with cervicogenic dizziness. Somat. Mot. Res. 2018, 35, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, E.; Treleaven, J. Sensorimotor function and dizziness in neck pain: Implications for assessment and management. J. Orthop. Sport. Phys. Ther. Mov. Sci. Media 2009, 39, 364–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, S.; Callister, R.; Katekar, M.; Rivett, D. Effects of Cervical Spine Manual Therapy on Range of Motion, Head Repositioning and Balance in Participants with Cervicogenic Dizziness: A Randomized. Arch. Phys. Med. 2014, 95, 1603–1612. [Google Scholar] [CrossRef] [PubMed]
- Rushton, A.; Carlesso, L.C.; Flynn, T.; Kerry, W.A.; Rubinstein, R.; Vogel, S.M. International Framework for Examination of the Cervical Region for Potential of Vascular Pathologies of the Neck Prior to Orthopaedic Manual Therapy (OMT) Intervention: International IFOMPT Cervical Framework; IFOMPT: Auckland, New Zealand, 2020. [Google Scholar]
- Bier, J.D.; Scholten-Peeters, W.G.M.; Staal, J.B.; Pool, J.; van Tulder, M.W.; Beekman, E.; Knoop, J.; Meerhoff, G.; Verhagen, A.P. Clinical Practice Guideline for Physical Therapy Assessment and Treatment in Patients With Nonspecific Neck Pain. Phys. Ther. 2018, 98, 162–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corrêa Rangel, T.; Falcão Raposo, M.C.; Sampaio Rocha-Filho, P.A. The prevalence and severity of insomnia in university students and their associations with migraine, tension-type headache, anxiety and depression disorders: A cross-sectional study. Sleep Med. 2021, 88, 241–246. [Google Scholar] [CrossRef]
- Elbinoune, I.; Amine, B.; Shyen, S.; Gueddari, S.; Abouqal, R.; Hajjaj-Hassouni, N. Chronic neck pain and anxiety-depression: Prevalence and associated risk factors. Pan Afr. Med. J. 2016, 24, 86. [Google Scholar] [CrossRef]
- Grande-Alonso, M.; Moral Saiz, B.; Mínguez Zuazo, A.; Lerma Lara, S.; la Touche, R. Análisis bioconductual del sistema vestibular y el control postural en pacientes con mareo cervicogénico. Estudio observacional transversal. Neurología 2018, 33, 98–106. [Google Scholar] [CrossRef]
- Song, T.J.; Cho, S.J.; Kim, W.J.; Yang, K.I.; Yun, C.H.; Chu, M.K. Anxiety and Depression in Tension-Type Headache: A Population-Based Study. PLoS ONE 2016, 11, e0165316. [Google Scholar] [CrossRef]


{kind=link}
| CGD Group M (SD) (n = 32) | TTH Group M (SD) (n = 33) | MCNP Group M (SD) (n = 44) | p-Value G1–G2 G1–G3 G2–G3 | |
|---|---|---|---|---|
| Age (years) | 41.50 (12.12) | 40.33 (14.03) | 46.75 (14.75) | 0.721 10.104 0.057 |
| Weight (kg) | 63.59 (10.28) | 63.72 (11.94) | 64.95 (12.74) | 0.962 0.620 0.668 |
| Height (cm) | 160.00 (5.61) | 163.70 (5.62) | 162.05 (5.98) | 0.052 0.135 0.225 |
| BMI (kg/cm2) | 24.88 (4.10) | 23.35 (4.34) | 24.63 (4.33) | 0.149 0.800 0.204 |
| CGD Group M (SD) | TTH Group M (SD) | MCNP Group M (SD) | p-Value G1–G2–G3 | p-Value G1–G2 G1–G3 G2–G3 | |
|---|---|---|---|---|---|
| Pain intensity | 28.65 (22.00) | 22.97 (18.27) | 50.31 (18.53) | F = 21.32 <0.001 | 0.262 <0.001 <0.001 |
| Flexion ROM | 43.03 (10.70) | 46.30 (11.43) | 48.38 (8.51) | F = 2.47 0.089 | 0.238 0.021 0.375 |
| Extension ROM | 51.49 (11.27) | 52.69 (12.65) | 54.23 (13.38) | F = 0.44 0.640 | 0.689 0.352 0.609 |
| Right-lateral-flexion ROM | 29.31 (7.55) | 32.12 (7.50) | 32.79 (8.90) | F = 1.82 0.167 | 0.138 0.977 0.718 |
| Left-lateral-flexion ROM | 31.36 (9.36) | 34.63 (7.47) | 31.50 (9.19) | F = 1.52 0.222 | 0.124 0.949 0.114 |
| Right-rotation ROM | 57.17 (9.08) | 57.30 (7.18) | 58.43 (10.30) | F = 0.22 0.797 | 0.951 0.582 0.572 |
| Left-rotation ROM | 53.66 (10.68) | 57.96 (7.30) | 58.84 (10.30) | F = 2.32 0.103 | 0.062 0.065 0.705 |
| HADS | 13.75 (6.28) | 11.33 (7.48) | 10.59 (5.40) | F = 2.39 0.096 | 0.164 0.022 0.631 |
| HADS anxiety subscale | 7.93 (3.68) | 7.06 (4.33) | 7.36 (3.66) | F = 0.42 0.652 | 0.383 0.503 0.747 |
| HADS depression subscale | 5.81 (3.23) | 4.27 (3.97) | 3.22 (2.39) | F = 6.10 0.003 | 0.092 <0.001 0.186 |
| TSK-11 | 23.22 (6.70) | 19.94 (5.30) | 22.77 (6.76) | F = 2.65 0.075 | 0.032 0.776 0.043 |
| CGD Group | TTH Group | MCNP Group | p-Value | |
|---|---|---|---|---|
| HADS (A/N) | 27/5 | 21/12 | 30/14 | 0.146 |
| HADS anxiety (A/BA/N) | 8/9/15 | 6/4/23 | 9/8/27 | 0.402 |
| HADS depression (A/BA/N) | 3/7/22 | 2/3/28 | 0/2/42 | 0.032 |
| HADS | TSK-11 | |
|---|---|---|
| Pain intensity | ||
| CGD group | r = 0.061; p = 0.742 | r = 0.037; p = 0.843 |
| TTH group | r = 0.296; p = 0.094 | r = 0.280; p = 0.115 |
| MCNP group | r = 0.331; p = 0.028 | r = 0.315; p = 0.037 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabanillas-Barea, S.; Carrasco-Uribarren, A.; Medrano-de-la-Fuente, R.; Jiménez-del-Barrio, S.; Pardos-Aguilella, P.; Pérez-Guillén, S.; Ceballos-Laita, L. Clinical and Psychological Variables in Female Patients with Cervical Syndromes: A Cross-Sectional and Correlational Study. Healthcare 2022, 10, 2398. https://doi.org/10.3390/healthcare10122398
Cabanillas-Barea S, Carrasco-Uribarren A, Medrano-de-la-Fuente R, Jiménez-del-Barrio S, Pardos-Aguilella P, Pérez-Guillén S, Ceballos-Laita L. Clinical and Psychological Variables in Female Patients with Cervical Syndromes: A Cross-Sectional and Correlational Study. Healthcare. 2022; 10(12):2398. https://doi.org/10.3390/healthcare10122398
Chicago/Turabian StyleCabanillas-Barea, Sara, Andoni Carrasco-Uribarren, Ricardo Medrano-de-la-Fuente, Sandra Jiménez-del-Barrio, Pilar Pardos-Aguilella, Silvia Pérez-Guillén, and Luis Ceballos-Laita. 2022. "Clinical and Psychological Variables in Female Patients with Cervical Syndromes: A Cross-Sectional and Correlational Study" Healthcare 10, no. 12: 2398. https://doi.org/10.3390/healthcare10122398