
Effect of Alpha-Lipoic Acid Supplementation on Low-Grade Squamous Intraepithelial Lesions—Double-Blind, Randomized, Placebo-Controlled Trial

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
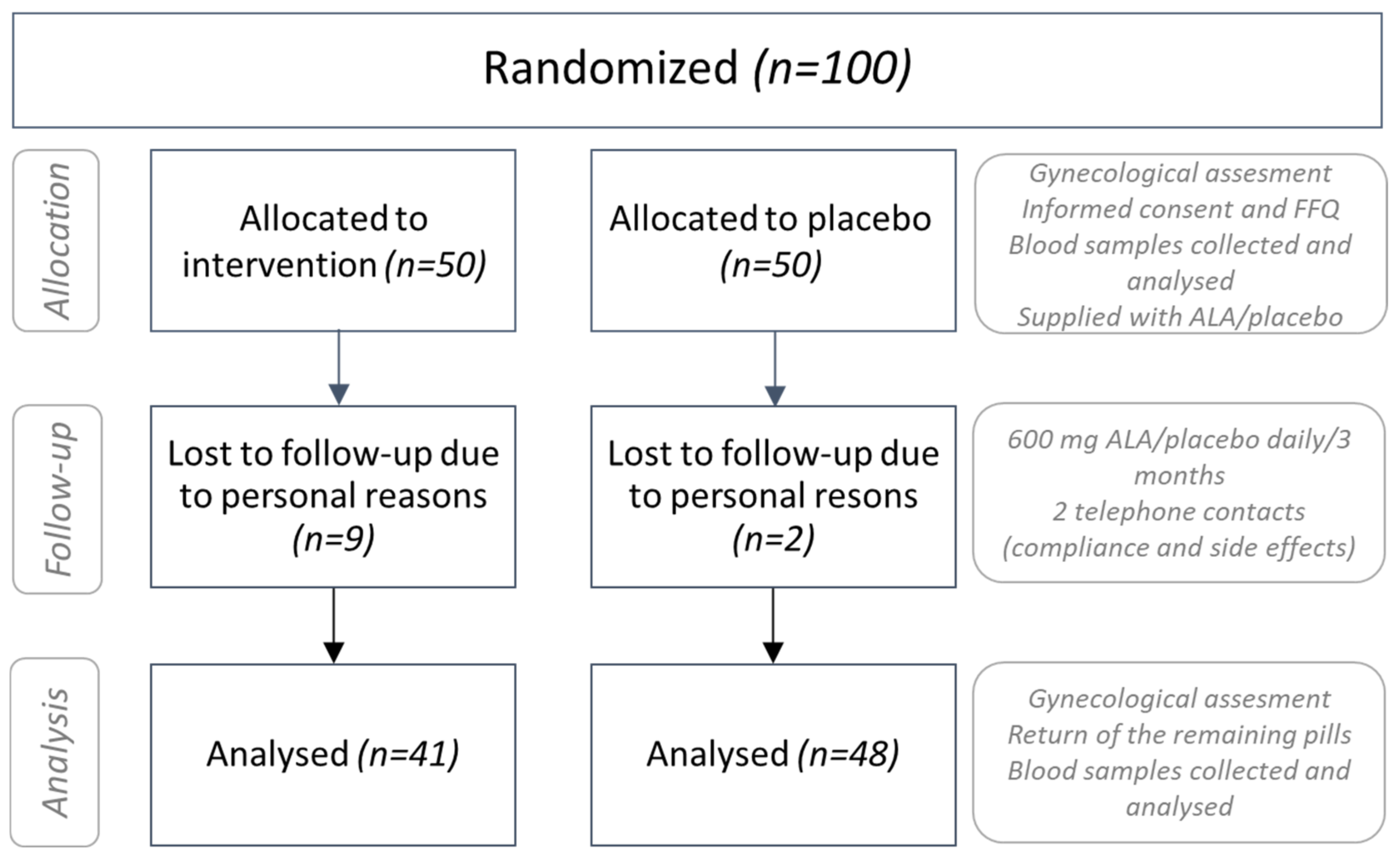
2.1. Participants and the Study Design
2.2. Data Collection
2.3. Assessment of Primary Outcomes
2.4. Assessment of Secondary Outcomes
2.5. Analysis of Diet Characteristics
2.6. Sample Size Assessment and Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richart, R.M. A modified terminology for cervical intraepithelial neoplasia. Obstet. Gynecol. 1990, 75, 131–133. [Google Scholar]
- Silveira, F.A.; Almeida, G.; Furtado, Y.L.; Cavalcanti, S.; Silva, K.S.; Maldonado, P.; Carvalho, M.G. The association of HPV genotype with the regression, persistence or progression of low-grade squamous intraepithelial lesions. Exp. Mol. Pathol. 2015, 99, 702–706. [Google Scholar] [CrossRef]
- Koshiyama, M.; Nakagawa, M.; Ono, A. The Preventive Effect of Dietary Antioxidants Against Cervical Cancer Versus the Promotive Effect of Tobacco Smoking. Healthcare 2019, 7, 162. [Google Scholar] [CrossRef] [Green Version]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Agrifoglio, O.; Scalisi, A.; Agodi, A. The association of dietary patterns with high-risk human papillomavirus infection and cervical cancer: A cross-sectional study in Italy. Nutrients 2018, 10, 469. [Google Scholar] [CrossRef] [Green Version]
- Hui, J.C.; Andy, H.L.; Linda, C.; Colin, W.B.; Daniel, X. A Review of Dietary Prevention of Human Papillomavirus-Related Infection of the Cervix and Cervical Intraepithelial Neoplasia. Nutr. Cancer 2013, 65, 317–328. [Google Scholar] [CrossRef]
- Erin, M.S.; Jason, L.S.; Luisa, L.V.; Alex, F.; Eduardo, L.F.; Anna, R.G. Dietary consumption of antioxidant nutrients and risk of incident cervical intraepithelial neoplasia. Gynecol. Oncol. 2010, 118, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Feng, C.Y.; Lin, M.; Lakhaney, D.; Sun, H.K.; Dai, X.B.; Zhao, F.H.; Qiao, Y.L. The association between dietary intake and cervical intraepithelial neoplasia grade 2 or higher among women in a high-risk rural area of China. Arch. Gynecol. Obstet. 2011, 284, 973–980. [Google Scholar] [CrossRef]
- Jiang, B.; Xiao, S.; Khan, M.A.; Xue, M. Defective antioxidant systems in cervical cancer. Tumor Biol. 2013, 34, 2003–2009. [Google Scholar] [CrossRef]
- Keefe, K.A.; Schell, M.J.; Brewer, C.; McHale, M.; Brewster, W.; Chapman, J.A.; Rose, G.S.; McMeeken, D.S.; Lagerberg, W.; Peng, Y.M.; et al. A randomized, double blind, Phase III trial using oral beta-carotene supplementation for women with high-grade cervical intraepithelial neoplasia. Cancer Epidemiol. Biomark. Prev. 2001, 10, 1029–1035. [Google Scholar]
- Butterworth, C.E., Jr.; Hatch, K.D.; Soong, S.J.; Cole, P.; Tamura, T.; Sauberlich, H.E.; Borst, M.; Macaluso, M.; Baker, V. Oral folic acid supplementation for cervical dysplasia: A clinical intervention trial. Am. J. Obstet. Gynecol. 1992, 166, 803–809. [Google Scholar] [CrossRef]
- Karamali, M.; Nourgostar, S.; Zamani, A.; Vahedpoor, Z.; Asemi, Z. The favourable effects of long-term selenium supplementation on regression of cervical tissues and metabolic profiles of patients with cervical intraepithelial neoplasia: A randomised, double-blind, placebo-controlled trial. Br. J. Nutr. 2015, 114, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asemi, Z.; Vahedpoor, Z.; Jamilian, M.; Bahmani, F.; Esmaillzadeh, A. Effects of long-term folate supplementation on metabolic status and regression of cervical intraepithelial neoplasia: A randomized, double-blind, placebo-controlled trial. Nutrition 2016, 32, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Vahedpoor, Z.; Mahmoodi, S.; Samimi, M.; Gilasi, H.R.; Bahmani, F.; Soltani, A.; Sharifi, E.M.; Asemi, Z. Long-Term Vitamin D Supplementation and the Effects on Recurrence and Metabolic Status of Cervical Intraepithelial Neoplasia Grade 2 or 3: A Randomized, Double-Blind, Placebo-Controlled Trial. Ann. Nutr. Metab. 2018, 72, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Tibullo, D.; Li Volti, G.; Giallongo, C.; Grasso, S.; Tomassoni, D.; Anfuso, C.D.; Lupo, G.; Amenta, F.; Avola, R.; Bramanti, V. Biochemical and clinical relevance of alpha lipoic acid: Antioxidant and anti-inflammatory activity, molecular pathways and therapeutic potential. Inflamm. Res. 2017, 66, 947–959. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.V.; Rideout, T.C.; Jones, P.J. Evidence for using alpha-lipoic acid in reducing lipoprotein and inflammatory related atherosclerotic risk. J. Diet. Suppl. 2012, 9, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.B.; Negrato, C.A. Alpha-lipoic acid as a pleiotropic compound with potential therapeutic use in diabetes and other chronic diseases. Diabetol. Metab. Syndr. 2014, 6, 80. [Google Scholar] [CrossRef] [Green Version]
- Šabanović, M.; Jašić, M.; Odobašić, A.; Aleksovska, E.S.; Pavljašević, S.; Bajraktarević, A.; Čepo, D.V. Alpha Lipoic Acid Reduces Symptoms and Inflammation Biomarkers in Patients with Chronic Hemorrhoidal Illness. Int. J. Vitam. Nutr. Res. 2018, 88, 281–290. [Google Scholar] [CrossRef]
- Salehi, B.; Berkay, Y.Y.; Antika, G.; Boyunegmez, T.T.; Fawzi, M.M.; Lobine, D.; Akram, M.; Riaz, M.; Capanoglu, E.; Sharopov, F.; et al. Insights on the Use of α-Lipoic Acid for Therapeutic Purposes. Biomolecules 2019, 9, 356. [Google Scholar] [CrossRef] [Green Version]
- Babić, D.; Sindik, J.; Missoni, S. Development and validation of a self-administered food frequency questionnaire to assess habitual dietary intake and quality of diet in healthy adults in the Republic of Croatia. Coll. Antropol. 2014, 38, 1017–1026. [Google Scholar]
- Ovanin-Rakić, A.; Pajtler, M.; Stanković, T.; Audy-Jurković, S.; Ljubojević, N. Klasifikacija citoloških nalaza vrata maternice »ZAGREB 2002« Modifikacija klasifikacija »Zagreb 1990« i »NCI Bethesda system 2001«. Gynaecol. Perinatol. 2003, 12, 148–153. [Google Scholar]
- Female Genital Tumors. Available online: https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Female-Genital-Tumours-2020 (accessed on 11 November 2022).
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Kaić, R.A.; Antonić, K. Tablice o Sastavu Namirnica i Pica; Zavod za Zaštitu Zdravlja SR Hrvatske: Zagreb, Croatia, 1990. [Google Scholar]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans. Available online: https://health.gov/our-work/nutrition-physical-activity/dietary-guidelines/current-dietary-guidelines (accessed on 11 November 2022).
- Harry, W.; Haverkos, G.S.; Stacey, L.; Steckley, W.P. Cigarette smoking and cervical cancer: Part I: A meta-analysis. Biomed. Pharmacother. 2003, 57, 67–77. [Google Scholar]
- Vinodhini, K.; Shanmughapriya, S.; Das, B.C.; Natarajaseenivasan, K. Prevalence and risk factors of HPV infection among women from various provinces of the world. Arch. Gynecol. Obstet. 2012, 285, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Koshiyama, M. The Effects of the Dietary and Nutrient Intake on Gynecologic Cancers. Healthcare 2019, 7, 88. [Google Scholar] [CrossRef] [Green Version]
- Stefani, C.C.A.; Liverani, V.; Bianco, C.; Penna, T.; Guarnieri, C.; Comparetto, E.; Monti, I.; Valente, A.L.; Pieralli, C.; Fiaschi, M.; et al. Spontaneous regression of low-grade cervical intraepithelial lesions is positively improved by topical bovine colostrum preparations (GINEDIE®). A multicentre, observational, italian pilot study. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 728–733. [Google Scholar]
- Bekos, C.; Schwameis, R.; Heinze, G.; Gärner, M.; Grimm, C.; Joura, E.; Horvat, R.; Polterauer, S.; Polterauer, M. Influence of age on histologic outcome of cervical intraepithelial neoplasia during observational management: Results from large cohort, systematic review, meta-analysis. Sci. Rep. 2018, 8, 6383. [Google Scholar] [CrossRef]
- Zappavigna, S.; Cossu, A.M.; Grimaldi, A.; Bocchetti, M.; Ferraro, G.A.; Nicoletti, G.F.; Filosa, R.; Caraglia, M. Anti-Inflammatory Drugs as Anticancer Agents. Int. J. Mol. Sci. 2020, 21, 2605. [Google Scholar] [CrossRef] [Green Version]
- Sangjeong, A.; Gi, J.K.; Sung, I.D.; Kyunge, K.; Hyunjoo, L.; In, G.D.; Dong, H.K.; Seoung, W.C.; Seungho, R.; Jin, H.S. High-sensitivity C-reactive Protein and Regression of Low-grade Squamous Intraepithelial Lesion: The Role of Low-grade Inflammation in Cervical Carcinogenesis. J. Epidemiol. 2021, 31, 615–620. [Google Scholar] [CrossRef]
- Akbari, M.; Ostadmohammadi, V.; Tabrizi, R.; Mobini, M.; Lankarani, K.B.; Moosazadeh, M.; Heydari, S.T.; Chamani, M.; Kolahdooz, F.; Asemi, Z. The effects of alpha-lipoic acid supplementation on inflammatory markers among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Nutr. Metab. 2018, 5, 15–39. [Google Scholar] [CrossRef] [Green Version]
- Feuerecker, B.; Pirsig, S.; Seidl, C.; Aichler, M.; Feuchtinger, A.; Bruchelt, G.; Senekowitsch, S.R. Lipoic acid inhibits cell proliferation of tumor cells in vitro and in vivo. Cancer Biol. Ther. 2012, 13, 1425–1435. [Google Scholar] [CrossRef] [Green Version]
- Jeon, M.J.; Kim, W.G.; Lim, S.; Choi, H.J.; Sim, S.; Kim, T.Y.; Shong, Y.K.; Kim, W.B. Alpha lipoic acid inhibits proliferation and epithelial mesenchymal transition of thyroid cancer cells. Mol. Cell. Endocrinol. 2016, 419, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Wen, Y.; Lv, G.; Lin, Y.; Tang, J.; Lu, J.; Zhang, M.; Liu, W.; Sun, X. α-Lipoic acid inhibits human lung cancer cell proliferation through Grb2-mediated EGFR down regulation. Biochem. Biophys. Res. Commun. 2017, 494, 325–331. [Google Scholar] [CrossRef]
- Moungjaroen, J.; Nimmannit, U.; Callery, P.S.; Wang, L.; Azad, N.; Lipipun, V.; Chanvorachote, P.; Rojanasakul, Y. Reactive oxygen species mediate caspase activation and apoptosis induced by lipoic acid in human lung epithelial cancer cells through Bcl-2 down-regulation. J. Pharmacol. Exp. Ther. 2006, 319, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Cure, E.; Cumhur, C.M. Alpha-lipoic acid may protect patients with diabetes against COVID-19 infection. Med. Hypotheses 2020, 143, 110–185. [Google Scholar] [CrossRef] [PubMed]
- Castañon, A.; Tristram, A.; Mesher, D.; Powell, N.; Beer, H.; Ashman, S.; Rieck, G.; Fielder, H.; Fiander, A.; Sasieni, P. Effect of diindolylmethane supplementation on low-grade cervical cytological abnormalities: Double-blind, randomised, controlled trial. Br. J. Cancer 2012, 106, 45–52. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Placebo n = 48 | Treated n = 41 | p | Placebo n = 48 | Treated n = 41 | p | |
|---|---|---|---|---|---|---|
| Initial Visit | 3-Month Follow-Up Visit | |||||
| 1 LSIL number of patients | 48 | 41 | 1.000 | 44 | 2 | <0.0001 |
| 1 HPV number of patients | 18 (37.5%) | 19 (46.3%) | 0.5178 | 18 (37.5%) | 19 (46.3%) | 0.5178 |
| 2 hsCRP (mg/L) | 0.86 (0.47–1.32) | 1.77 (0.82–2.44) | 0.0344 | 1.11 (0.61–1.98) | 0.89 (0.39–1.68) | 0.2408 |
| 2 FI (g/L) | 3.30 (2.4–3.9) | 3.9 (3.1–4.4) | 0.0130 | 3.7 (2.7–4.5) | 3.3 (2.6–3.8) | 0.0437 |
| 2 SE (mm/h) | 16 (12–23) | 20 (15–26) | 0.0785 | 20 (16–26) | 16 (12–22) | 0.0046 |
| Placebo | Treated | |||||
|---|---|---|---|---|---|---|
| Initial | 3-Month Follow-Up | p | Initial | 3-Month Follow-Up | p | |
| 1 LSIL number of patients | 48 | 44 | 0.1171 | 41 | 2 | <0.001 |
| 1 HPV number of patients | 18 | 18 | 1.000 | 19 | 19 | 1.000 |
| 2 hsCRP (mg/L) | 0.86 (0.47–1.32) | 1.11 (0.61–1.98) | <0.001 | 1.77 (0.82–2.44) | 0.89 (0.39–1.68) | <0.001 |
| 2 FI (g/L) | 3.30 (2.4–3.9) | 3.7 (2.7–4.5) | <0.001 | 3.9 (3.1–4.4) | 3.3 (2.6–3.8) | <0.001 |
| 2 SE (mm/h) | 16 (12–23) | 20 (16–26) | <0.001 | 20 (15–26) | 16 (12–22) | <0.001 |
| Placebo n = 48 (Final Visit) | Treated n = 41 (Final Visit) | Odds Ratio | 95% Cl | p | |
|---|---|---|---|---|---|
| Recovery (n) | 4 | 39 | 0.004662 | 0.0008091–0.02686 | <0.0001 |
| LSIL (n) | 44 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Divković, A.; Radić, K.; Sabitović, D.; Golub, N.; Rajković, M.G.; Rumora Samarin, I.; Karasalihović, Z.; Šerak, A.; Trnačević, E.; Turčić, P.; et al. Effect of Alpha-Lipoic Acid Supplementation on Low-Grade Squamous Intraepithelial Lesions—Double-Blind, Randomized, Placebo-Controlled Trial. Healthcare 2022, 10, 2434. https://doi.org/10.3390/healthcare10122434
Divković A, Radić K, Sabitović D, Golub N, Rajković MG, Rumora Samarin I, Karasalihović Z, Šerak A, Trnačević E, Turčić P, et al. Effect of Alpha-Lipoic Acid Supplementation on Low-Grade Squamous Intraepithelial Lesions—Double-Blind, Randomized, Placebo-Controlled Trial. Healthcare. 2022; 10(12):2434. https://doi.org/10.3390/healthcare10122434
Chicago/Turabian StyleDivković, Anja, Kristina Radić, Damir Sabitović, Nikolina Golub, Marija Grdić Rajković, Ivana Rumora Samarin, Zinaida Karasalihović, Adnan Šerak, Emir Trnačević, Petra Turčić, and et al. 2022. "Effect of Alpha-Lipoic Acid Supplementation on Low-Grade Squamous Intraepithelial Lesions—Double-Blind, Randomized, Placebo-Controlled Trial" Healthcare 10, no. 12: 2434. https://doi.org/10.3390/healthcare10122434