
A SARS-CoV-2 Infection High-Uptake Program on Healthcare Workers and Cancer Patients of the National Cancer Institute of Naples, Italy

 ,
,  , ,
, ,  , ,
, ,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
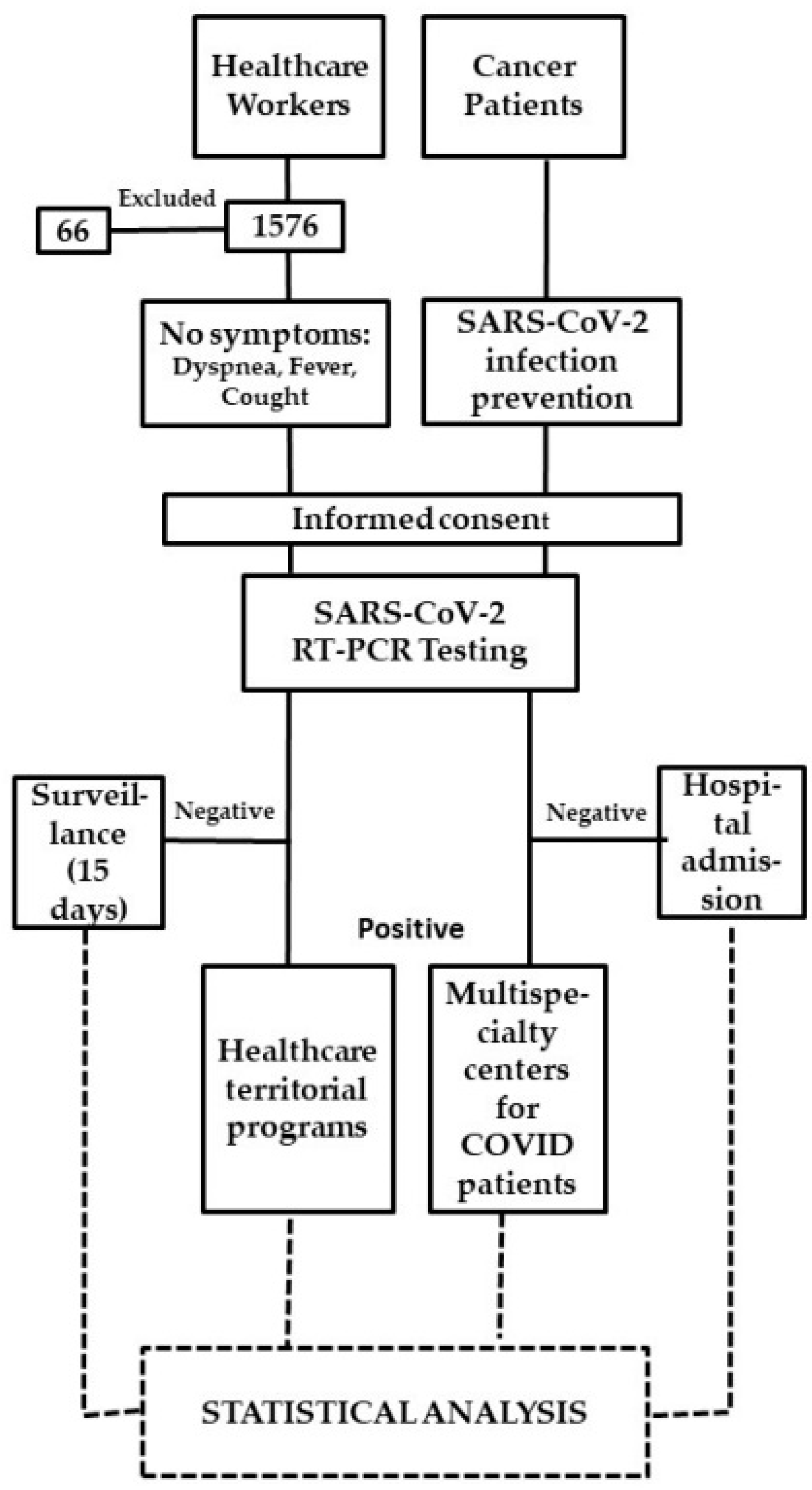
2.1. Study Design
- The first wave, from 4 March 2020, to 31 May 2020;
- A transition phase, from 1 June 2020, to 27 September 2020;
- The second wave from 28 September 2020, to 3 January 2021;
- The second transition phase from 4 January 2021, to 4 April 2021.
2.2. Sample
2.3. Tests Used for SARS-CoV-2
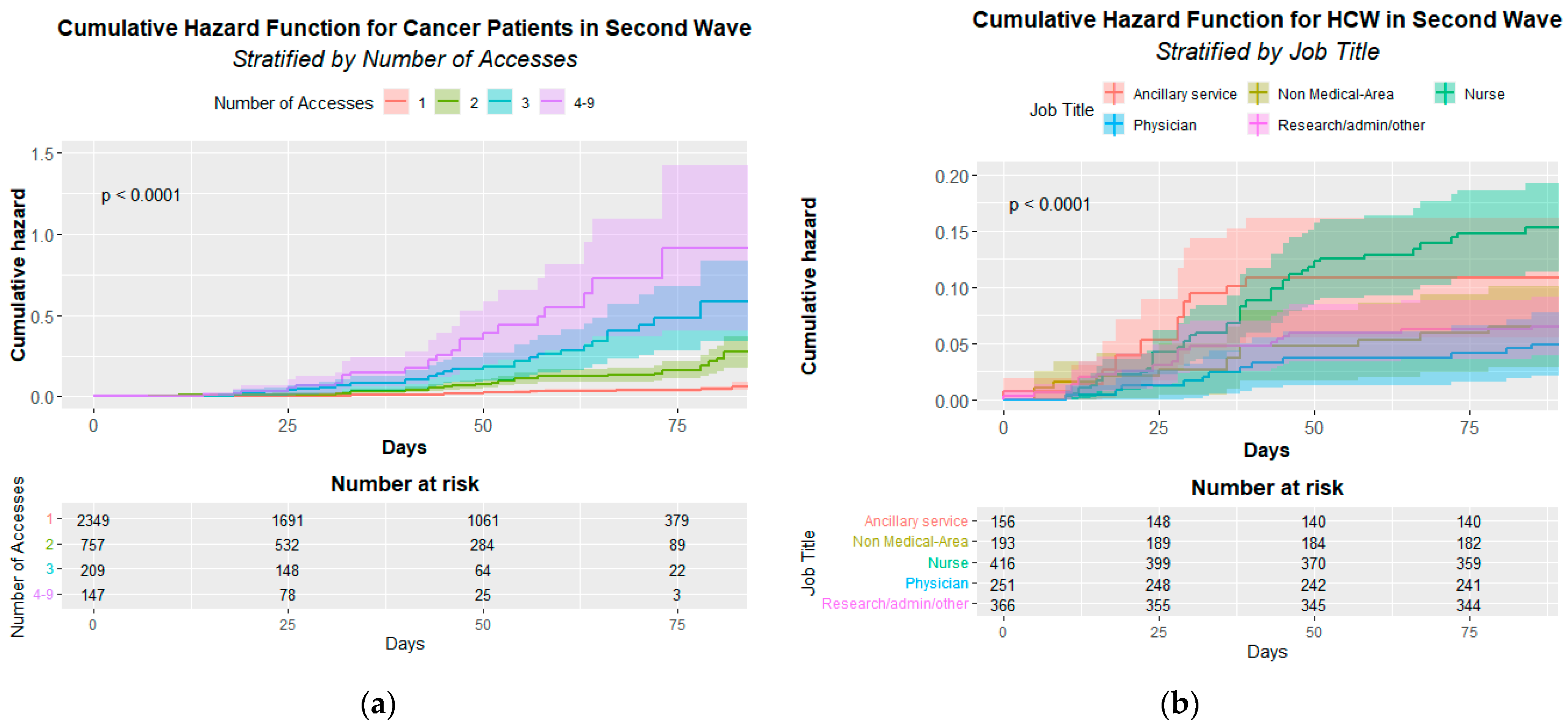
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gagliano, A.; Villani, P.G.; Co’, F.M.; Manelli, A.; Paglia, S.; Bisagni, P.A.G.; Perotti, G.; Storti, E.; Lombardo, M. COVID-19 Epidemic in the Middle Province of Northern Italy: Impact, Logistics, and Strategy in the First Line Hospital. Disaster Med. Public Health Prep. 2020, 14, 372–376. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Situazione Italia—Dati del Dipartimento della Protezione Civile 2021. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id=5351&lingua=italiano&menu=vuoto (accessed on 3 May 2021).
- Italian Ministry of Health. Coronavirus. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?lingua=italiano&id=5373&area=nuovoCoronavirus&menu=vuoto (accessed on 3 May 2021).
- Bielicki, J.A.; Duval, X.; Gobat, N.; Goossens, H.; Koopmans, M.; Tacconelli, E.; van der Werf, S. Monitoring approaches for health-care workers during the COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, e261–e267. [Google Scholar] [CrossRef]
- Moscola, J.; Sembajwe, G.; Jarrett, M.; Farber, B.; Chang, T.; McGinn, T.; Davidson, K.W. Northwell Health COVID-19 Research Consortium. Prevalence of SARS-CoV-2 Antibodies in Health Care Personnel in the New York City Area. JAMA 2020, 324, 893–895. [Google Scholar] [CrossRef]
- Liu, C.; Zhao, Y.; Okwan-Duodu, E.A.D.; Basho, R.; Cui, X. COVID-19 in cancer patients: Risk, clinical features, and management. Cancer Biol. Med. 2020, 17, 519–527. [Google Scholar] [CrossRef]
- Lee, K.A.; Ma, W.; Sikavi, D.R.; Drew, D.A.; Nguyen, L.H.; Bowyer, R.C.E.; Cardoso, M.J.; Fall, T.; Freidin, M.B.; Gomez, M.; et al. Cancer and Risk of COVID-19 Through a General Community Survey. Oncologist 2020, 26, e182–e185. [Google Scholar] [CrossRef]
- Iorio, G.C.; Ammendolia, A.; Marotta, N.; Ricardi, U.; de Sire, A. A bond between rheumatic diseases and cancer in the elderly: The interleukin-6 pathway. Int. J. Rheum. Dis. 2021, 24, 1317–1320. [Google Scholar] [CrossRef]
- Crispo, A.; Montagnese, C.; Perri, F.; Grimaldi, M.; Bimonte, S.; Augustin, L.S.; Amore, A.; Celentano, E.; Di Napoli, M.; Cascella, M.; et al. COVID-19 Emergency and Post-Emergency in Italian Cancer Patients: How Can Patients Be Assisted? Front. Oncol. 2020, 10, 1571. [Google Scholar] [CrossRef]
- Buonaguro, F.M.; Botti, G.; Ascierto, P.A.; Pignata, S.; Ionna, F.; Delrio, P.; Petrillo, A.; Cavalcanti, E.; Di Bonito, M.; Perdonà, S.; et al. The clinical and translational research activities at the INT—IRCCS “Fondazione Pascale” cancer center (Naples, Italy) during the COVID-19 pandemic. Infect. Agents Cancer 2020, 15, 69. [Google Scholar] [CrossRef]
- Laboratory testing strategy recommendations for COVID-19—Interim guidance 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331509/WHO-COVID-19-lab_testing-2020.1-eng.pdf?sequence=1&isAllowed=y (accessed on 3 May 2021).
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [Green Version]
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Huff, H.V.; Singh, A. Asymptomatic Transmission During the Coronavirus Disease 2019 Pandemic and Implications for Public Health Strategies. Clin. Infect. Dis. 2020, 71, 2752–2756. [Google Scholar] [CrossRef]
- Barranco, R.; Ventura, F. COVID-19 and infections in health care workers: An emerging problem. Med.-Leg. J. 2020, 88, 65–66. [Google Scholar] [CrossRef]
- Iavicoli, S.; Boccuni, F.; Buresti, G.; Gagliardi, D.; Persechino, B.; Valenti, A.; Rondinone, B.M. Risk assessment at work and prevention strategies on COVID-19 in Italy. PLoS ONE 2021, 16, e0248874. [Google Scholar] [CrossRef]
- Gosain, R.; Abdou, Y.; Singh, A.; Rana, N.; Puzanov, I.; Ernstoff, M.S. COVID-19 and Cancer: A Comprehensive Review. Curr. Oncol. Rep. 2020, 22, 53. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Sikavi, D.R.; Lo, C.H.; Kwon, S.; Song, M.; et al. Risk of COVID-19 among frontline healthcare workers and the general community: A prospective cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Barrett, E.S.; Horton, D.B.; Roy, J.; Gennaro, M.L.; Brooks, A.; Tischfield, J.; Greenberg, P.; Andrews, T.; Jagpal, S.; Reilly, N.; et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic. medRxiv 2020. [Google Scholar] [CrossRef]
- Houlihan, C.F.; Vora, N.; Byrne, T.; Lewer, D.; Kelly, G.; Heaney, J.; Gandhi, S.; Spyer, M.J.; Beale, R.; Cherepanov, P.; et al. Pandemic peak SARS-CoV-2 infection and seroconversion rates in London frontline health-care workers. Lancet 2020, 396, e6–e7. [Google Scholar] [CrossRef]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife 2020, 9, e58728. [Google Scholar] [CrossRef]
- Shields, A.; Faustini, S.E.; Perez-Toledo, M.; Jossi, S.; Aldera, E.; Allen, J.D.; Al-Taei, S.; Backhouse, C.; Bosworth, A.; Dunbar, L.A.; et al. SARS-CoV-2 seroprevalence and asymptomatic viral carriage in healthcare workers: A cross-sectional study. Thorax 2020, 75, 1089–1094. [Google Scholar] [CrossRef]
- Sahu, A.K.; Amrithanand, V.; Mathew, R.; Aggarwal, P.; Nayer, J.; Bhoi, S. COVID-19 in health care workers—A systematic review and meta-analysis. Am. J. Emerg. Med. 2020, 38, 1727–1731. [Google Scholar] [CrossRef]
- Ran, L.; Chen, X.; Wang, Y.; Wu, W.; Zhang, L.; Tan, X. Risk Factors of Healthcare Workers with Coronavirus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China. Clin. Infect. Dis. 2020, 71, 2218–2221. [Google Scholar] [CrossRef] [Green Version]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. [Google Scholar] [CrossRef]
- Eyre, D.W.; Lumley, S.; O’Donnell, D.; Campbell, M.; Sims, E.; Lawson, E.; Warren, F.; James, T.; Cox, S.; Howarth, A.; et al. Differential occupational risks to healthcare workers from SARS-CoV-2 observed during a prospective observational study. eLife 2020, 9, e60675. [Google Scholar] [CrossRef]
- Lombardi, A.; Consonni, D.; Carugno, M.; Bozzi, G.; Mangioni, D.; Muscatello, A.; Castelli, V.; Palomba, E.; Cantù, A.; Ceriotti, F.; et al. Characteristics of 1573 healthcare workers who underwent nasopharyngeal swab testing for SARS-CoV-2 in Milan, Lombardy, Italy. Clin. Microbiol. Infect. 2020, 26, 1413.e9–1413.e13. [Google Scholar] [CrossRef]
- de Sire, A.; Marotta, N.; Raimo, S.; Lippi, L.; Inzitari, M.T.; Tasselli, A.; Gimigliano, A.; Palermo, L.; Invernizzi, M.; Ammendolia, A. Psychological Distress and Work Environment Perception by Physical Therapists from Southern Italy during COVID-19 Pandemic: The C.A.L.A.B.R.I.A Study. Int. J. Environ. Res. Public Health 2021, 18, 9676. [Google Scholar] [CrossRef]
- Farì, G.; de Sire, A.; Giorgio, V.; Rizzo, L.; Bruni, A.; Bianchi, F.P.; Zonno, A.; Pierucci, P.; Ranieri, M.; Megna, M. Impact of COVID-19 on the mental health in a cohort of Italian rehabilitation healthcare workers. J. Med. Virol. 2021, 94, 110–118. [Google Scholar] [CrossRef]
- Calò, F.; Russo, A.; Camaioni, C.; De Pascalis, S.; Coppola, N. Burden, risk assessment, surveillance and management of SARS-CoV-2 infection in health workers: A scoping review. Infect. Dis. Poverty 2020, 9, 139. [Google Scholar] [CrossRef]
- Lahner, E.; Dilaghi, E.; Prestigiacomo, C.; Alessio, G.; Marcellini, L.; Simmaco, M.; Santino, I.; Orsi, G.B.; Anibaldi, P.; Marcolongo, A.; et al. Prevalence of SARS-CoV-2 Infection in Health Workers (HWs) and Diagnostic Test Performance: The Experience of a Teaching Hospital in Central Italy. Int. J. Environ. Res. Public Health 2020, 17, 4417. [Google Scholar] [CrossRef]
- Crispo, A.; Bimonte, S.; Porciello, G.; Forte, C.A.; Cuomo, G.; Montagnese, C.; Prete, M.; Grimaldi, M.; Celentano, E.; Amore, A.; et al. Strategies to evaluate outcomes in long-COVID-19 and post-COVID survivors. Infect. Agents Cancer 2021, 16, 62. [Google Scholar] [CrossRef]
- Jin, H.; Chen, Y.; Fu, Q.; Qu, Q. Occupational risk factors of contracting COVID-19 among health workers: A systematic review. Work 2021, 69, 721–734. [Google Scholar] [CrossRef]
- Cascella, M.; Marinangeli, F.; Vittori, A.; Scala, C.; Piccinini, M.; Braga, A.; Miceli, L.; Vellucci, R. Open Issues and Practical Suggestions for Telemedicine in Chronic Pain. Int. J. Environ. Res. Public Health 2021, 18, 12416. [Google Scholar] [CrossRef]
- Cascella, M.; Miceli, L.; Cutugno, F.; Di Lorenzo, G.; Morabito, A.; Oriente, A.; Massazza, G.; Magni, A.; Marinangeli, F.; Cuomo, A.; et al. A Delphi Consensus Approach for the Management of Chronic Pain during and after the COVID-19 Era. Int. J. Environ. Res. Public Health 2021, 18, 13372. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Roma, P.; Da Molin, G.; Diella, G.; Montagna, M.T.; Ferracuti, S.; Liguori, G.; Orsi, G.B.; Napoli, C. Acceptance of COVID-19 Vaccination in the Elderly: A Cross-Sectional Study in Southern Italy. Vaccines 2021, 9, 1222. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HCWs and CPs | First Wave: March–May 2020 | 1^ Transition Phase June–September 2020 | Second Wave October–December 2020 | 2^ Transition Phase January–March 2021 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HCWs | CPs | HCWs | CPs | HCWs | CPs | HCWs | CPs | |||||
| Total (%) 1 | 1204 (79.7%) | 2152 (24.6%) | 1268 (84.0%) | 1793 (20.5%) | 1385 (91.7%) | 3462 (39.6%) | 1249 (82.7%) | 3439 (39.4%) | ||||
| Positive (%) | 20 (1.7%) | 100 (4.6%) | 3 (0.2%) | 14 (0.8%) | 127 (9.2%) | 168 (4.9%) | 9 (0.7%) | 40 (1.2%) | ||||
| Positive/TOT (%) | p-Value 2 | Positive/TOT (%) | p-Value 2 | Posivtive/TOT (%) | p-Value 2 | Positive/TOT (%) | p-Value 2 | |||||
| Age | ||||||||||||
| ≤44 | 13/551 (2.4%) | 8/269 (3.0%) | 0.77 | 3/612 (0.5%) | 5/261 (1.9%) | 0.10 | 51/682 (7.5%) | 28/530 (5.3%) | 0.16 | 10/621 (1.6%) | 10/615 (1.6%) | 1 |
| >44 | 7/653 (1.1%) | 92/1883 (4.9%) | <0.001 | 0/656 | 9/1532 (0.6%) | 0.11 | 76/703 (10.8%) | 140/2932 (4.8%) | <0.001 | 2/625 (0.3%) | 30/2824 (1.1%) | 0.13 |
| Gender | ||||||||||||
| Male | 6/588 (1.0%) | 40/992 (4.0%) | 0.001 | 1/566 (0.2%) | 6/840 (0.7%) | 0.31 | 66/638 (10.3%) | 83/1683 (4.9%) | <0.001 | 8/556 (1.4%) | 24/1717 (1.4%) | 1 |
| Female | 14/616 (2.3%) | 60/1160 (5.2%) | 0.005 | 2/702 (0.3%) | 8/953 (0.8%) | 0.26 | 61/747 (8.2%) | 85/1779 (4.8%) | 0.001 | 4/693 (0.6%) | 16/1722 (0.9%) | 0.54 |
| Healthcare Workers (HCWs) | First Wave March–May 2020 | 1^ Transition Phase June–September 2020 2 | Second Wave October–December 2020 3 | 2^ Transition Phase January–March 2021 4 |
|---|---|---|---|---|
| Departments | ||||
| Clinical care | 8/403 (2.0%) | 0/432 | 46/444 (10.4%) | 2/418 (0.5%) |
| Surgery | 11/293 (3.8%) | 1/315 (0.3%) | 34/332 (10.2%) | 4/305 (1.3%) |
| Research | 0/206 | 1/240 (0.4%) | 16/248 (6.5%) | 2/234 (0.9%) |
| Administrative | 0/150 | 1/175 (0.6%) | 14/203 (6.9%) | 0/183 |
| Operational Services | 1/152 (0.7%) | 0/105 | 17/156 (10.9%) | 1/105 (1.0%) |
| Job Title | ||||
| Ancillary services 1 | 1/152 (0.7%) | 0/105 | 17/156 (10.9%) | 1/105 (1.0%) |
| Non medical-area | 1/173 (0.6%) | 0/185 | 13/193 (6.7%) | 2/189 (1.1%) |
| Nurse | 4/356 (1.1%) | 1/387 (0.3%) | 62/416 (14.9%) | 4/377 (1.1%) |
| Physician | 7/238 (2.9%) | 1/247 (0.4%) | 12/251 (4.8%) | 0/233 |
| Research staff | 7/205 (3.4%) | 0/242 | 19/252 (7.5%) | 2/236 (0.8%) |
| Techno/Administr. Staff/Other | 0/80 | 1/101 (1.0%) | 4/114 (3.5%) | 0/105 |
| Molecular Swabs | ||||
| Total (%) | 1877 (14.8%) | 2374 (18.7%) | 5951 (46.9%) | 2475 (19.5%) |
| Mean (SD) | 1.56 (1.09) | 1.87 (0.85) | 4.30 (1.70) | 1.98 (1.28) |
| Cancer Patients | First Wave: March–May 2020 | 1^ Transition Phase June–September 2020 | Second Wave October–December 2020 | 2^ Transition Phase January–March 2021 |
|---|---|---|---|---|
| Number of accesses | ||||
| One | 56/1562 (3.6%) | 7/1338 (0.5%) | 50/2349 (2.1%) | 22/2741 (0.8%) |
| Two | 33/494 (6.7%) | 3/344 (0.9%) | 57/757 (7.5%) | 10/500 (2.0%) |
| Three | 8/78 (10.3%) | 2/76 (2.6%) | 35/209 (16.7%) | 3/102 (2.9%) |
| Four or more | 3/18 (16.7%) | 2/35 (5.7%) | 26/147 (17.7%) | 5/96 (5.2%) |
| Molecular Swabs | ||||
| Total (%) | 2859 (18.9%) | 2405 (15.9%) | 5177 (34.2%) | 4714 (31.1%) |
| Mean for patient (SD) | 1.33 (0.59) | 1.34 (0.68) | 1.50 (0.92) | 1.37 (1.21) |
| Healthcare Workers | Second Wave October–December 2020 1 | |||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| Negative | Positive (%) | p-Value 2 | Effect-Size 4 | OR (95% CI) | p-Value 3 | |
| Age | 0.04 | 0.06 | 0.06 | |||
| ≤44 | 631 | 51 (7.5%) | 1† | |||
| >44 | 627 | 76 (10.8%) | 1.44 (0.98–2.12) | |||
| Gender | 0.6 | 0.01 | 0.2 | |||
| Male | 616 | 66 (9.7%) | 1† | |||
| Female | 642 | 61 (8.7%) | 0.80 (0.55–1.17) | |||
| Job Title | <0.001 | 0.07 | <0.001 | |||
| Research, administrative staff and other | 343 | 23 (6.3%) | 1† | |||
| Ancillary services | 139 | 17 (10.9%) | 1.68 (0.55–1.17) | |||
| Non medical-area | 180 | 13 (6.7%) | 0.96 (0.47–1.98) | |||
| Nurse | 354 | 62 (14.9%) | 2.24 (1.23–4.08) | |||
| Physician | 239 | 12 (4.8%) | 0.58 (0.26–1.27) | |||
| Departments | 0.3 | 0.03 | 0.6 | |||
| Research, administrative and operational services | 560 | 47 (7.7%) | 1† | |||
| Clinical care | 398 | 46 (10.4%) | 1.24 (0.71–2.17) | |||
| Surgery | 298 | 34 (10.2%) | 1.02 (0.54–1.91) | |||
| Cancer Patients (CPs) | Second Wave October–December 2020 | |||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| Negative | Positive (%) | p-Value 1 | Effect-Size 3 | OR (95% CI) | p-Value 2 | |
| Age | 0.7 | 0.06 | 0.39 | |||
| ≤44 | 502 | 28 (5.3%) | 1 † | |||
| >44 | 2792 | 140 (4.8%) | 0.83 (0.54–1.27) | |||
| Gender | 0.9 | 0.01 | 0.57 | |||
| Male | 1600 | 83 (4.9%) | 1 † | |||
| Female | 1694 | 85 (4.8%) | 1.10 (0.80–1.51) | |||
| Number of accesses | <0.001 | 0.1 | <0.001 | |||
| One | 2299 | 50 (2.1%) | 1 † | |||
| Two | 700 | 57 (7.5%) | 3.76 (2.55–5.55) | |||
| Three | 174 | 35 (16.7%) | 9.38 (5.92–14.86) | |||
| Four or more | 121 | 26 (17.7%) | 10.12 (6.07–16.86) | |||
| Cox-Model for Cancer Patients (CPs) | Second Wave October–December 2020 | |
|---|---|---|
| HR 1 (95% CI) | p-Value | |
| Number of accesses | ||
| One | 1 † | |
| Two | 4.13 (2.82–6.04) | <0.001 |
| Three | 10.80 (6.99–16.68) | <0.001 |
| Four or more | 21.04 (13.09–33.82) | <0.001 |
| Cox-Model for Healthcare Workers (HCWs) | Second Wave October–December 2020 | |
|---|---|---|
| HR 1 (95% CI) | p-Value | |
| Job Title | ||
| Research and admin, staff/other | 1 † | |
| Ancillary services | 1.70 (0.88–3.29) | 0.117 |
| Non medical-area | 0.95 (0.48–1.91) | 0.895 |
| Nurse | 2.05 (1.16–3.64) | 0.014 |
| Physician | 0.60 (0.28–1.29) | 0.189 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crispo, A.; Di Gennaro, P.; Coluccia, S.; Gandini, S.; Montagnese, C.; Porciello, G.; Nocerino, F.; Grimaldi, M.; Tafuri, M.; Luongo, A.; et al. A SARS-CoV-2 Infection High-Uptake Program on Healthcare Workers and Cancer Patients of the National Cancer Institute of Naples, Italy. Healthcare 2022, 10, 205. https://doi.org/10.3390/healthcare10020205
Crispo A, Di Gennaro P, Coluccia S, Gandini S, Montagnese C, Porciello G, Nocerino F, Grimaldi M, Tafuri M, Luongo A, et al. A SARS-CoV-2 Infection High-Uptake Program on Healthcare Workers and Cancer Patients of the National Cancer Institute of Naples, Italy. Healthcare. 2022; 10(2):205. https://doi.org/10.3390/healthcare10020205
Chicago/Turabian StyleCrispo, Anna, Piergiacomo Di Gennaro, Sergio Coluccia, Sara Gandini, Concetta Montagnese, Giuseppe Porciello, Flavia Nocerino, Maria Grimaldi, Mariangela Tafuri, Assunta Luongo, and et al. 2022. "A SARS-CoV-2 Infection High-Uptake Program on Healthcare Workers and Cancer Patients of the National Cancer Institute of Naples, Italy" Healthcare 10, no. 2: 205. https://doi.org/10.3390/healthcare10020205
APA StyleCrispo, A., Di Gennaro, P., Coluccia, S., Gandini, S., Montagnese, C., Porciello, G., Nocerino, F., Grimaldi, M., Tafuri, M., Luongo, A., Rotondo, E., Amore, A., Labonia, F., Meola, S., Marone, S., Pierro, G., Menegozzo, S., Miscio, L., Perri, F., ... Celentano, E. (2022). A SARS-CoV-2 Infection High-Uptake Program on Healthcare Workers and Cancer Patients of the National Cancer Institute of Naples, Italy. Healthcare, 10(2), 205. https://doi.org/10.3390/healthcare10020205