
Machine Learning for Predicting Risk of Early Dropout in a Recovery Program for Opioid Use Disorder


Abstract
:1. Introduction
2. Materials and Methods
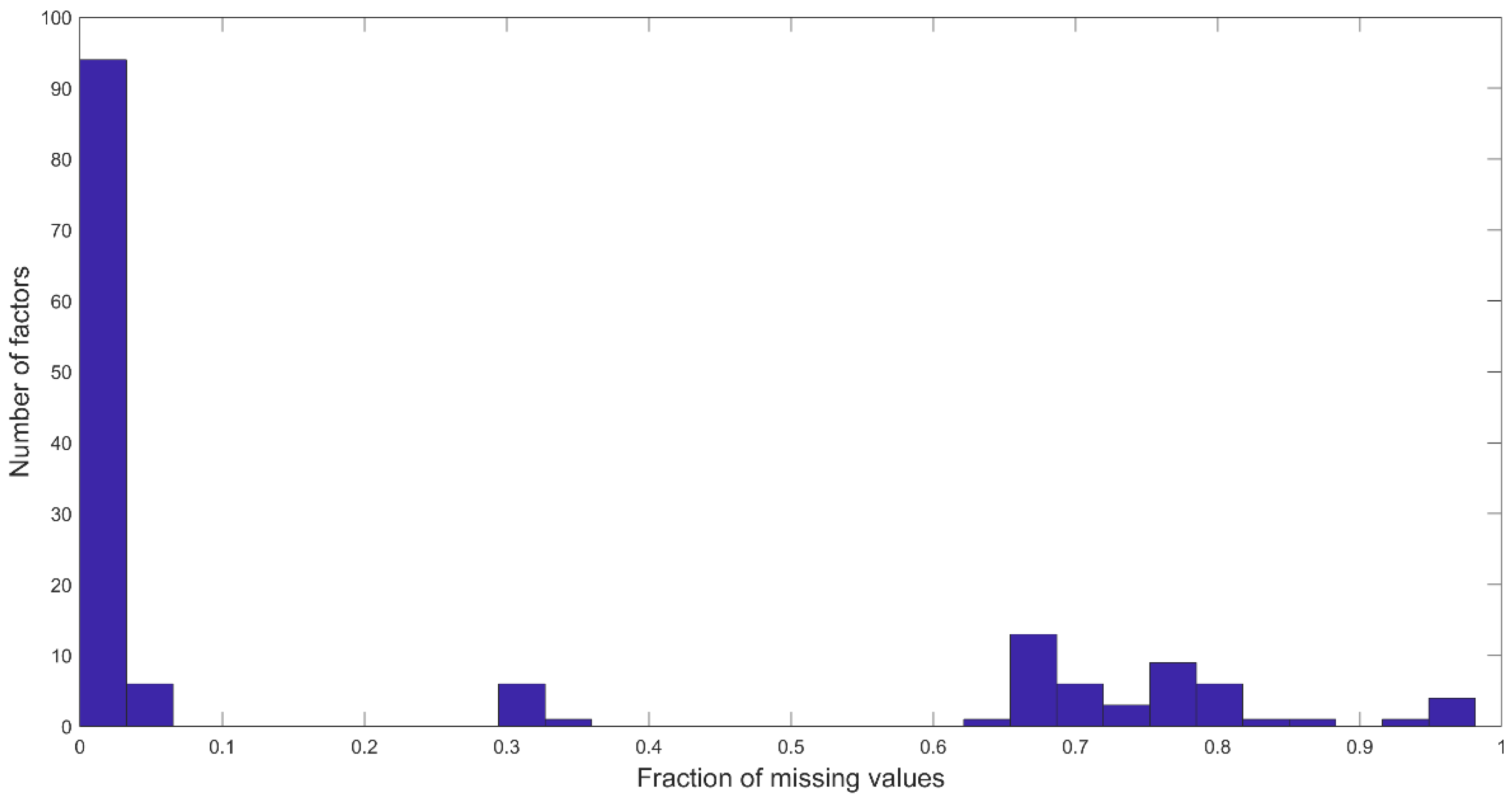
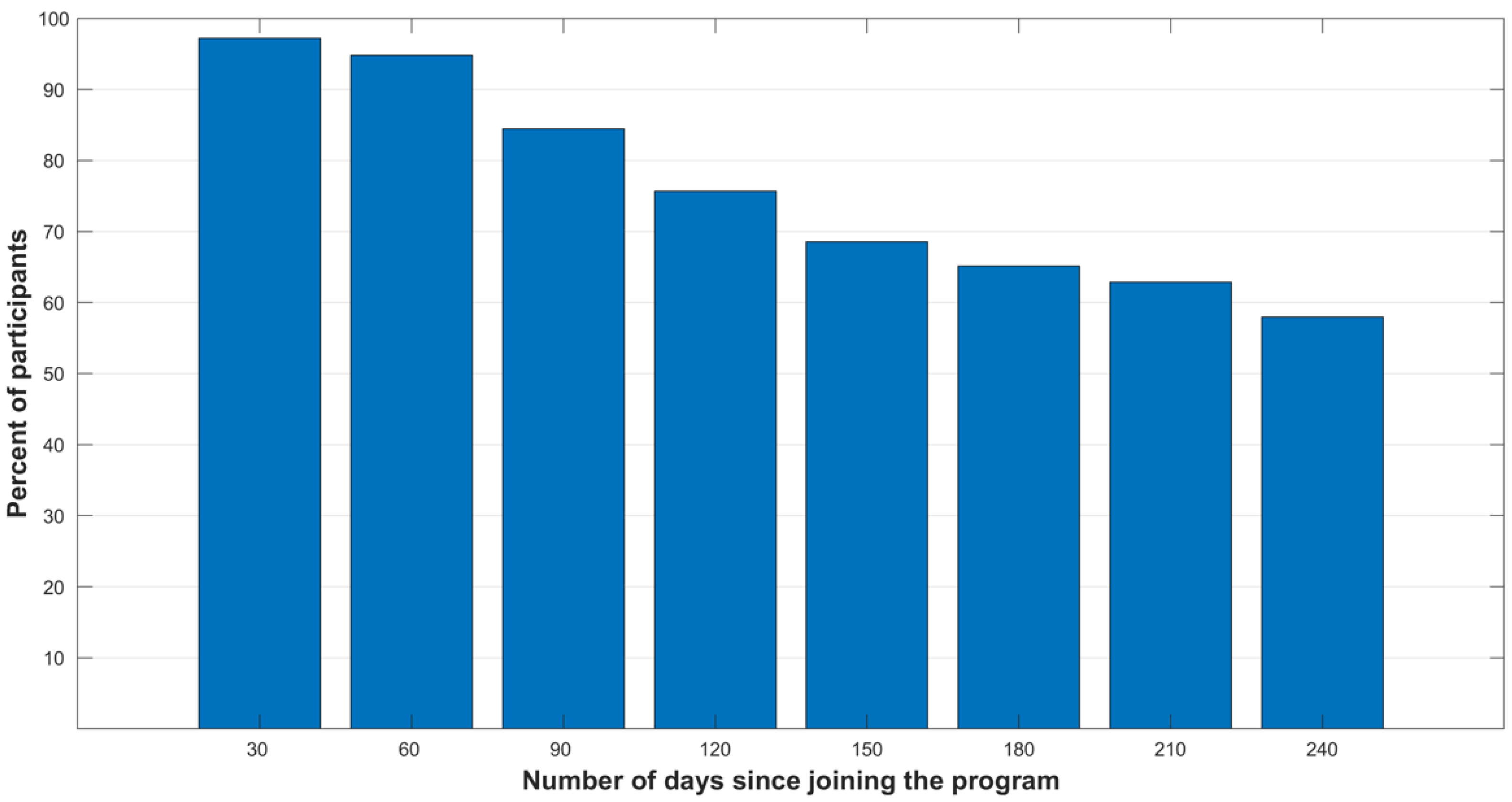
2.1. Data
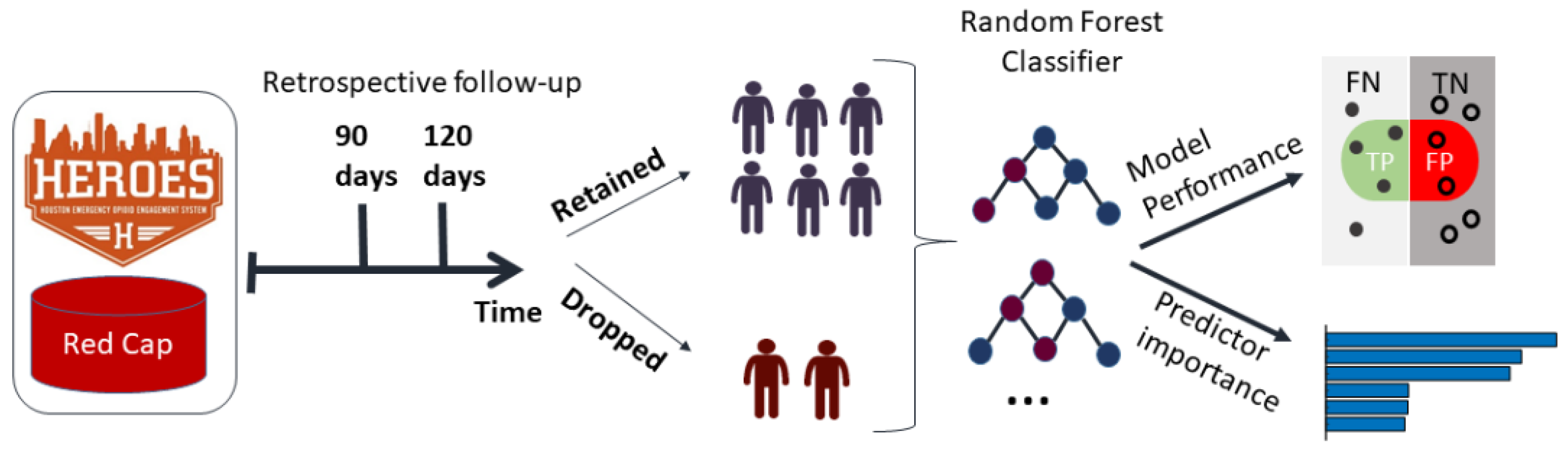
2.2. Prediction Scheme
2.3. Factor Ranking
3. Results
3.1. Machine Learning Framework to Identify Program Dropout
3.2. Risk Factors Associated with Program Dropout
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AdaBoost | Adaptive Boosting |
| AUC | Area Under the Curve |
| FDR | False Discovery Rate |
| HEROES | Houston Emergency Opioid Engagement System |
| OUD | Opioid Use Disorder |
References
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2019 National Survey on Drug Use and Health (HHS Publication No. PEP20-07-01-001, NSDUH Series H-55); Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2020. Available online: https://www.samhsa.gov/data/ (accessed on 2 January 2022).
- Langabeer, J.R.; Champagne-Langabeer, T.; Yatsco, A.J.; O’Neal, M.M.; Cardenas-Turanzas, M.; Prater, S.; Luber, S.; Stotts, A.; Fadial, T.; Khraish, G.; et al. Feasibility and outcomes from an integrated bridge treatment program for opioid use disorder. J Am. Coll. Emerg. Physicians Open 2021, 2, e12417. [Google Scholar] [CrossRef] [PubMed]
- Hser, Y.-I.; Evans, E.; Grella, C.; Ling, W.; Anglin, D. Long-term course of opioid addiction. Harv. Rev. Psychiatry 2015, 23, 76–89. [Google Scholar] [CrossRef] [PubMed]
- McHugh, R.K.; Murray, H.W.; Hearon, B.A.; Pratt, E.M.; Pollack, M.H.; Safren, S.A.; Otto, M.W. Predictors of dropout from psychosocial treatment in opioid-dependent outpatients. Am. J. Addict. 2013, 22, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, N.; Mojtabai, R.; Stuart, E.A.; Fingerhood, M.; Agus, D.; Lyons, B.C.; Weiner, J.P.; Saloner, B. Opioid agonist treatment and fatal overdose risk in a state-wide US population receiving opioid use disorder services. Addiction 2020, 115, 1683–1694. [Google Scholar] [CrossRef]
- National Institute on Drug Abuse (NIDA). Principles of Effective Treatment; National Institute on Drug Abuse Website. Available online: https://www.drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/principles-effective-treatment (accessed on 2 January 2022).
- Marcovitz, D.E.; McHugh, R.K.; Volpe, J.; Votaw, V.; Connery, H.S. Predictors of early dropout in outpatient buprenorphine/naloxone treatment. Am. J. Addict. 2016, 25, 472–477. [Google Scholar] [CrossRef] [Green Version]
- Panlilio, L.V.; Stull, S.W.; Kowalczyk, W.J.; Phillips, K.A.; Schroeder, J.R.; Bertz, J.W.; Vahabzadeh, M.; Lin, J.L.; Mezghanni, M.; Nunes, E.V.; et al. Stress, craving and mood as predictors of early dropout from opioid agonist therapy. Drug Alcohol Depend 2019, 202, 200–208. [Google Scholar] [CrossRef]
- Weinstein, Z.M.; Kim, H.W.; Cheng, D.M.; Quinn, E.; Hui, D.; Labelle, C.T.; Drainoni, M.-L.; Bachman, S.S.; Samet, J.H. Long-term retention in office based opioid treatment with buprenorphine. J. Subst. Abus. Treat. 2017, 74, 65–70. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, A.M.; Cousins, G.; Durand, L.; Barry, J.; Boland, F. Retention of patients in opioid substitution treatment: A systematic review. PLoS ONE 2020, 15, e0232086. [Google Scholar] [CrossRef]
- Bharat, C.; Hickman, M.; Barbieri, S.; Degenhardt, L. Big data and predictive modelling for the opioid crisis: Existing research and future potential. Lancet Digit Health 2021, 3, e397–e407. [Google Scholar] [CrossRef]
- Acion, L.; Kelmansky, D.; van der Laan, M.; Sahker, E.; Jones, D.; Arndt, S. Use of a machine learning framework to predict substance use disorder treatment success. PLoS ONE 2017, 12, e0175383. [Google Scholar] [CrossRef]
- Hasan, M.M.; Young, G.J.; Shi, J.; Mohite, P.; Young, L.D.; Weiner, S.G. A machine learning based two-stage clinical decision support system for predicting patients’ discontinuation from opioid use disorder treatment: Retrospective observational study. BMC Med. Inform. Decis. Mak. 2021, 21, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Patridge, E.F.; Bardyn, T.P. Research electronic data capture (REDCap). J. Med. Libr. Assoc. JMLA 2018, 106, 142. [Google Scholar] [CrossRef] [Green Version]
- Freund, Y.; Schapire, R.; Abe, N. A short introduction to boosting. J.-Jpn. Soc. Artif. Intell. 1999, 14, 1612. [Google Scholar]
- Friedman, J.; Hastie, T.; Tibshirani, R. Additive logistic regression: A statistical view of boosting (with discussion and a rejoinder by the authors). Ann. Stat. 2000, 28, 337–407. [Google Scholar] [CrossRef]
- Freund, Y. A more robust boosting algorithm. arXiv 2009, arXiv:0905.2138. [Google Scholar]
- Warmuth, M.K.; Liao, J.; Rätsch, G. Totally corrective boosting algorithms that maximize the margin. In Proceedings of the 23rd International Conference on Machine Learning, Pittsburgh, PA, USA, 25–29 June 2006; pp. 1001–1008. [Google Scholar]
- Lappan, S.N.; Brown, A.W.; Hendricks, P.S. Dropout rates of in-person psychosocial substance use disorder treatments: A systematic review and meta-analysis. Addiction 2020, 115, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, S.; Stopka, T.J.; Hughto, J.M.W.; Case, P.; Palacios, W.R.; Reilly, B.; Green, T.C. Prevalence and correlates of non-fatal overdose among people who use drugs: Findings from rapid assessments in Massachusetts, 2017-2019. Harm Reduct. J. 2021, 18, 93. [Google Scholar] [CrossRef] [PubMed]
- Au, V.Y.O.; Rosic, T.; Sanger, N.; Hillmer, A.; Chawar, C.; Worster, A.; Marsh, D.C.; Thabane, L.; Samaan, Z. Factors associated with opioid overdose during medication-assisted treatment: How can we identify individuals at risk? Harm Reduct. J. 2021, 18, 71. [Google Scholar] [CrossRef]
- Hasin, D.S.; Grant, B.F. The National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Waves 1 and 2: Review and summary of findings. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1609–1640. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, A.; Violato, C. Knowledge of and attitudes towards depression and adherence to treatment: The Antidepressant Adherence Scale (AAS). J. Affect. Disord. 2010, 126, 388–394. [Google Scholar] [CrossRef]
- De Maeyer, J.; van Nieuwenhuizen, C.; Bongers, I.L.; Broekaert, E.; Vanderplasschen, W. Profiles of quality of life in opiate-dependent individuals after starting methadone treatment: A latent class analysis. Int. J. Drug Policy 2013, 24, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Nosyk, B.; Guh, D.P.; Sun, H.; Oviedo-Joekes, E.; Brissette, S.; Marsh, D.C.; Schechter, M.T.; Anis, A.H. Health related quality of life trajectories of patients in opioid substitution treatment. Drug Alcohol Depend. 2011, 118, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Nosyk, B.; Bray, J.W.; Wittenberg, E.; Aden, B.; Eggman, A.A.; Weiss, R.D.; Potter, J.; Ang, A.; Hser, Y.I.; Ling, W.; et al. Short term health-related quality of life improvement during opioid agonist treatment. Drug Alcohol Depend. 2015, 157, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.F.; Greene, M.C.; Bergman, B.G. Beyond Abstinence: Changes in Indices of Quality of Life with Time in Recovery in a Nationally Representative Sample of U.S. Adults. Alcohol. Clin. Exp. Res. 2018, 42, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.G.; Gryczynski, J.; Schwartz, R.P.; Myers, C.P.; O’Grady, K.E.; Olsen, Y.K.; Jaffe, J.H. Changes in Quality of Life following Buprenorphine Treatment: Relationship with Treatment Retention and Illicit Opioid Use. J. Psychoact. Drugs 2015, 47, 149–157. [Google Scholar] [CrossRef]
- Bray, J.W.; Aden, B.; Eggman, A.A.; Hellerstein, L.; Wittenberg, E.; Nosyk, B.; Stribling, J.C.; Schackman, B.R. Quality of life as an outcome of opioid use disorder treatment: A systematic review. J. Subst. Abus. Treat. 2017, 76, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Strada, L.; Vanderplasschen, W.; Buchholz, A.; Schulte, B.; Muller, A.E.; Verthein, U.; Reimer, J. Measuring quality of life in opioid-dependent people: A systematic review of assessment instruments. Qual. Life Res. 2017, 26, 3187–3200. [Google Scholar] [CrossRef] [Green Version]
- Center for Substance Abuse Treatment. Substance Abuse: Clinical Issues in Intensive Outpatient Treatment; Treatment Improvement Protocol (TIP) Series 47. DHHS Publication No. (SMA) 06-4182; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2006.
- Strang, J.; Volkow, N.D.; Degenhardt, L.; Hickman, M.; Johnson, K.; Koob, G.F.; Marshall, B.D.L.; Tyndall, M.; Walsh, S.L. Opioid use disorder. Nat. Rev. Dis. Primers 2020, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Smyth, B.P.; Barry, J.; Keenan, E.; Ducray, K. Lapse and relapse following inpatient treatment of opiate dependence. Ir. Med. J. 2010, 103, 176–179. [Google Scholar]
- Chopra, N.; Marasa, L.H. The opioid epidemic: Challenges of sustained remission. Int. J. Psychiatry Med. 2017, 52, 196–201. [Google Scholar] [CrossRef]
- Ma, J.; Bao, Y.P.; Wang, R.J.; Su, M.F.; Liu, M.X.; Li, J.Q.; Degenhardt, L.; Farrell, M.; Blow, F.C.; Ilgen, M.; et al. Effects of medication-assisted treatment on mortality among opioids users: A systematic review and meta-analysis. Mol. Psychiatry 2019, 24, 1868–1883. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R. New findings on biological factors predicting addiction relapse vulnerability. Curr. Psychiatry Rep. 2011, 13, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson Silver Wolf, D.A.; Gold, M. Treatment resistant opioid use disorder (TROUD): Definition, rationale, and recommendations. J. Neurol. Sci. 2020, 411, 116718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Casale, A.; Sorice, S.; Padovano, A.; Simmaco, M.; Ferracuti, S.; Lamis, D.A.; Rapinesi, C.; Sani, G.; Girardi, P.; Kotzalidis, G.D.; et al. Psychopharmacological Treatment of Obsessive-Compulsive Disorder (OCD). Curr. Neuropharmacol. 2019, 17, 710–736. [Google Scholar] [CrossRef]
- Bergfeld, I.O.; Mantione, M.; Figee, M.; Schuurman, P.R.; Lok, A.; Denys, D. Treatment-resistant depression and suicidality. J. Affect. Disord. 2018, 235, 362–367. [Google Scholar] [CrossRef]
- Blum, K.A. Treatment-Resistant Hodgkin Lymphoma: Defining the Role of Autologous Transplantation. Cancer J. 2018, 24, 244–248. [Google Scholar] [CrossRef]
- Bozinoff, N.; Anderson, B.J.; Bailey, G.L.; Stein, M.D. Correlates of Stigma Severity among Persons Seeking Opioid Detoxification. J. Addict. Med. 2018, 12, 19–23. [Google Scholar] [CrossRef]
- Champagne-Langabeer, T.; Swank, M.W.; Langabeer, J.R. Routes of non-traditional entry into buprenorphine treatment programs. Subst. Abus. Treat Prev. Policy 2020, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Volkow, N.D.; Jones, E.B.; Einstein, E.B.; Wargo, E.M. Prevention and Treatment of Opioid Misuse and Addiction: A Review. JAMA Psychiatry 2019, 76, 208–216. [Google Scholar] [CrossRef]
- Oquendo, M.A.; Volkow, N.D. Suicide: A Silent Contributor to Opioid-Overdose Deaths. N. Engl. J. Med. 2018, 378, 1567–1569. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 90 Days | 120 Days | |||
|---|---|---|---|---|
| Method | Specificity | Sensitivity | Specificity | Sensitivity |
| Logistic Regression | 0.22 ± 0.3 | 0.9 ± 0.13 | 0.44 ± 0.27 | 0.81 ± 0.12 |
| Radial Basis Support Vector Machines | 0.54 ± 0.02 | 0.63 ± 0.04 | 0.57 ± 0.03 | 0.66 ± 0.03 |
| AdaBoost | 0.62 ± 0.05 | 0.82 ± 0.07 | 0.66 ± 0.01 | 0.83 ± 0.03 |
| Gentle Boost | 0.63 ± 0.05 | 0.81 ± 0.02 | 0.67 ± 0.04 | 0.79 ± 0.03 |
| Logit Boost | 0.64 ± 0.05 | 0.79 ± 0.04 | 0.68 ± 0.02 | 0.81 ± 0.04 |
| Robust Boost | 0.62 ± 0.06 | 0.79 ± 0.02 | 0.69 ± 0.06 | 0.8 ± 0.05 |
| Total Boost | 0.61 ± 0.03 | 0.81 ± 0.02 | 0.66 ± 0.03 | 0.84 ± 0.02 |
| Random Forest | 0.65 ± 0.05 | 0.81 ± 0.02 | 0.66 ± 0.02 | 0.86 ± 0.03 |
| Factor | Individuals Who Dropped 90 Days (%) | Individuals Retained 90 Days (%) | Individuals Who Dropped 120 Days (%) | Individuals Retained 120 Days (%) | FDR-Adjusted p-Values (90 Days, 120 Days) |
|---|---|---|---|---|---|
| Have you overdosed? | 58 (56%) | 91 (17%) | 84 (52.2%) | 49 (11.0%) | e−15, 2e−26 |
| QoL improvement | 100 (95%) | 347 (64%) | 155 (93.9%) | 269 (59.0%) | 4e−15, 4e−25 |
| Have you relapsed since joining? | 58 (55%) | 169 (31%) | 90 (54.5%) | 126 (27.6%) | 3e−6, 2e−11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gottlieb, A.; Yatsco, A.; Bakos-Block, C.; Langabeer, J.R.; Champagne-Langabeer, T. Machine Learning for Predicting Risk of Early Dropout in a Recovery Program for Opioid Use Disorder. Healthcare 2022, 10, 223. https://doi.org/10.3390/healthcare10020223
Gottlieb A, Yatsco A, Bakos-Block C, Langabeer JR, Champagne-Langabeer T. Machine Learning for Predicting Risk of Early Dropout in a Recovery Program for Opioid Use Disorder. Healthcare. 2022; 10(2):223. https://doi.org/10.3390/healthcare10020223
Chicago/Turabian StyleGottlieb, Assaf, Andrea Yatsco, Christine Bakos-Block, James R. Langabeer, and Tiffany Champagne-Langabeer. 2022. "Machine Learning for Predicting Risk of Early Dropout in a Recovery Program for Opioid Use Disorder" Healthcare 10, no. 2: 223. https://doi.org/10.3390/healthcare10020223