
Singing Experience Influences RSST Scores

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
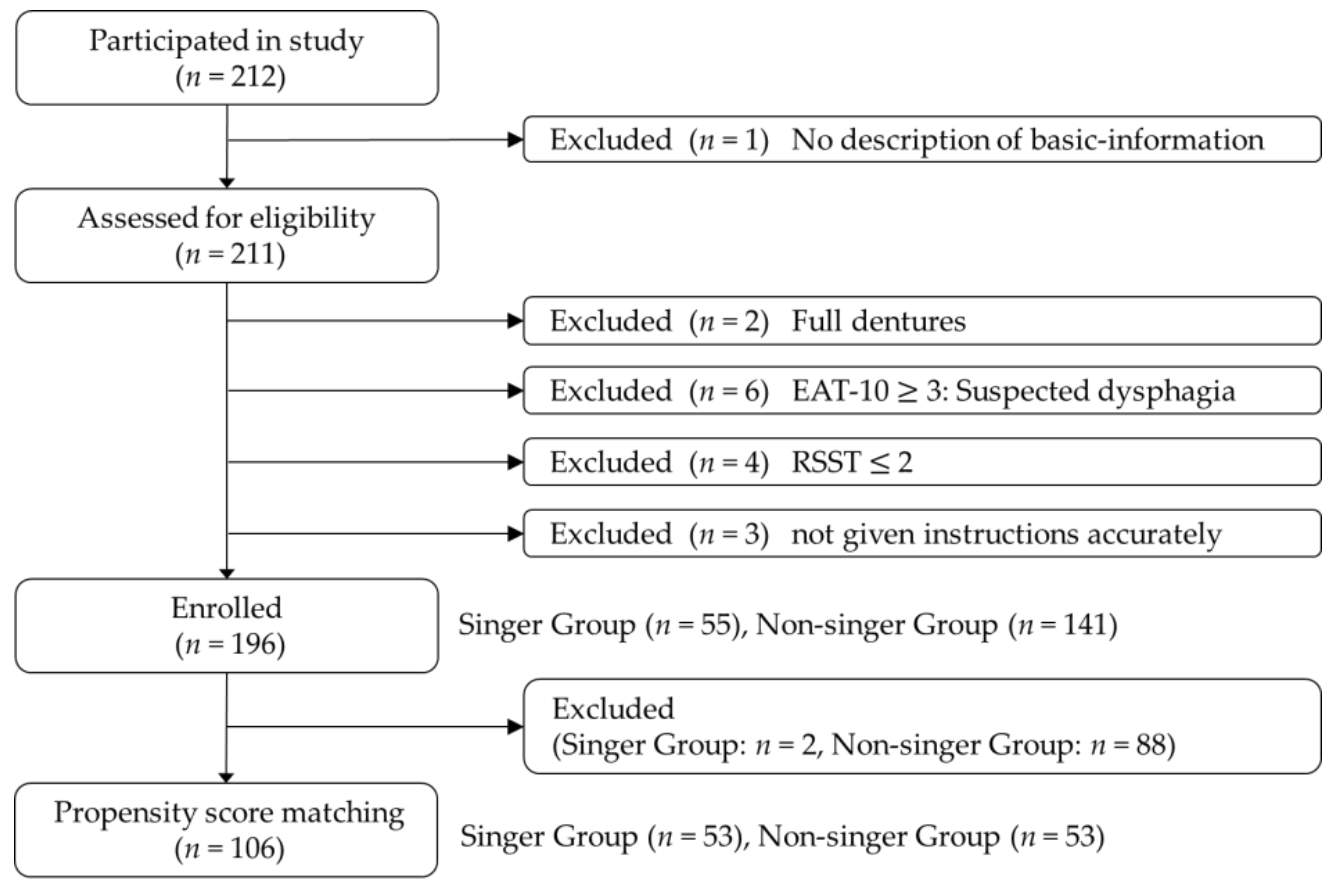
2.1. Study Design and Oversight
2.2. Procedure
2.2.1. RSST
2.2.2. MPT
2.2.3. Grip Strength
2.3. Statistical Analysis
- The continuous variable covariate case is represented by:where is the mean of the singer group, is the mean of the non-singer group, is the standard deviation of the singer group and is the standard deviation of the non-singer group.
- The nominal variable covariate case is represented by:where is the rate of the singer group and is the rate of the non-singer group.
3. Results
3.1. Characteristics of the Subjects
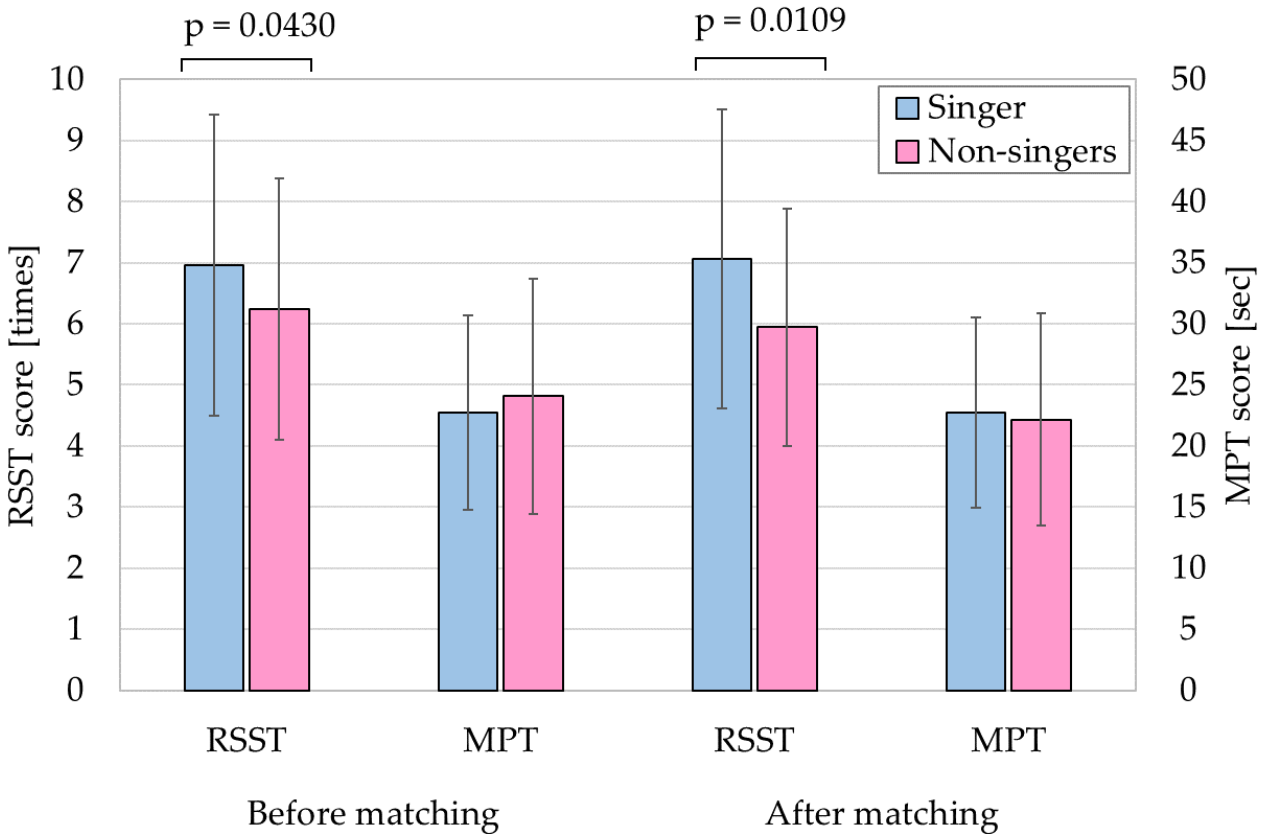
3.2. Analysis of Propensity Score Matching
4. Discussion
4.1. Comparison between Singers and Non-Singers
4.2. Dysphagia Treatment of Swallowing Therapy
4.3. Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gas Hepatol. 2015, 12, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Roy, N.; Stemple, J.; Merrill, M.R.; Thomas, L. Dysphagia in the elderly: Preliminary evidence of prevalence, risk factors, and socioemotional effects. Ann. Otol. Rhinol. Laryngol. 2007, 116, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Hirata, M.; Takahashi, K.; Kameda, S.; Katsuta, Y.; Yoshida, F.; Hattori, N.; Yanagisawa, T.; Palmer, J.; Oshino, S.; et al. Non-invasive quantification of human swallowing using a simple motion tracking system. Sci. Rep. 2018, 8, 5095. [Google Scholar] [CrossRef] [PubMed]
- Jayatilake, D.; Ueno, T.; Teramoto, Y.; Nakai, K.; Hidaka, K.; Ayuzawa, S.; Eguchi, K.; Matsumura, A.; Suzuki, K. Smartphone-Based Real-time Assessment of Swallowing Ability From the Swallowing Sound. IEEE J. Transl. Eng. Health Med. 2015, 3, 2900310. [Google Scholar] [CrossRef]
- Yagi, N.; Nagami, S.; Lin, M.; Yabe, T.; Itoda, M.; Imai, T.; Oku, Y. A noninvasive swallowing measurement system using a combination of respiratory flow, swallowing sound, and laryngeal motion. Med. Biol. Eng. Comput. 2017, 55, 1001–1017. [Google Scholar] [CrossRef]
- Oguchi, K.; Saitoh, E.; Baba, M.; Kusudo, S.; Tanaka, T.; Onogi, K. The repetitive saliva swallowing test (RSST) as a screening test of functional dysphagia (1) Normal Values of RSST. Jpn. J. Rehabil. Med. 2000, 37, 375–382. [Google Scholar] [CrossRef]
- Schwartz, S.R.; Francis, O.D.; Schwartz, R.S.; Damask, C.C.; Digoy, P.G.; Krouse, J.H.; McMurray, J.S.; Medina, S.; Ouellette, D.R.; Messinger-Rapport, B.J.; et al. Clinical practice guideline: Hoarseness (dysphonia). Otolaryngol. Head Neck Surg. 2018, 143, 175–180. [Google Scholar] [CrossRef]
- Logemann, J.A. Evaluation and Treatment of Swallowing Disorders. Am. J. Speech-Lang. Pathol. 1994, 3, 41–44. [Google Scholar] [CrossRef]
- Yagi, N.; Oku, Y.; Nagami, S.; Yamagata, Y.; Kayashita, J.; Ishikawa, A.; Domen, K.; Takahashi, R. Inappropriate timing of swallow in the respiratory cycle causes breathing-swallowing discoordination. Front. Physiol. 2017, 8, 676. [Google Scholar] [CrossRef] [Green Version]
- Nagami, S.; Oku, Y.; Yagi, N.; Sato, S.; Uozumi, R.; Morita, S.; Yamagata, Y.; Kayashita, J.; Tanimura, K.; Sato, A.; et al. Breathing-swallowing discoordination is associated with frequent exacerbations of COPD. BMJ Open Respir. Res. 2017, 4, e000202. [Google Scholar] [CrossRef]
- Maezawa, H.; Vicario, M.C.; Kuo, M.; Hirata, M.; Mima, T.; Ntsche, A.M. Effects of bilateral anodal transcranial direct current stimulation over the tongue primary motor cortex on cortical excitability of the tongue and tongue motor functions. Brain Stimul. 2020, 13, 270–272. [Google Scholar] [CrossRef] [Green Version]
- Maezawa, H.; Mima, M.; Yazawa, S.; Matsuhashi, M.; Shiraishi, H.; Hirai, Y.; Funahashi, M. Contralateral dominance of corticomuscular coherence for both sides of the tongue during human tongue protrusion: An MEG study. NeuroImage 2014, 101, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Lortie, L.C.; Rivard, J.; Thibeault, M.; Tremblay, P. The moderating effect of frequent singing on voice aging. J. Voice 2017, 31, 112.e1–112.e12. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT- 10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- Oguchi, K.; Saitoh, E.; Baba, M.; Kusudo, S.; Tanaka, T.; Onogi, K. The repetitive saliva swallowing test (RSST) as a screening test of functional dysphagia (2) Validity of RSST. Jpn. J. Rehabil. Med. 2000, 37, 383–388. [Google Scholar] [CrossRef]
- Maslan, J.; Leng, X.; Rees, C.; Blalock, D.; Butler, S.G. Maximum phonation time in healthy older adults. J. Voice 2011, 25, 709–713. [Google Scholar] [CrossRef] [Green Version]
- Umeno, H. A summary of the clinical practice guidelines for the diagnosis and management of voice disorders, 2018 in Japan. Auris Nasus Larynx 2020, 47, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Statistics notes: Matching. BMJ 1994, 309, 1128. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am. Stat. 1985, 39, 33–38. [Google Scholar]
- Yang, D.; Dalton, J. A unified approach to measuring the effect size between two groups using SAS. Mathematics 2012. Available online: http://support.sas.com/resources/papers/proceedings12/335-2012.pdf (accessed on 1 December 2021).
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Guo, S.Y.; Fraser, M.W. Propensity Score Analysis: Statistical Methods and Applications; SAGE Publications: Newbury Park, CA, USA, 2010; Volume 11. [Google Scholar]
- Yamaguchi, S.; Ishida, M.; Hidaka, K.; Gomi, S.; Takayama, S.; Sato, K.; Yoshioka, Y.; Wakayama, N.; Sekine, K.; Matsune, S.; et al. Relationship between swallowing function and breathing/phonation. Auris Nasus Larynx 2018, 45, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011, 10, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, S.; Hata, Y.; Yagi, N.; Kawamura, N.; Kashioka, H.; Yanagida, T.; Hirata, M.; Maezawa, H.; Sakai, Y. Relationship between Singing Experience and Laryngeal Movement Obtained by DeepLabCut. In Proceedings of the 2021 5th IEEE International Conference on Cybernetics (CYBCONF), Sendai, Japan, 8–10 June 2021; pp. 73–78. [Google Scholar]
- The Oto-Rhino-Laryngological Society of Japan. In Clinical Practice Guidelines for the Diagnosis and Management of Dysphagia 2018; Kanehara & Co., LTD.: Tokyo, Japan, 2018.
- Wheeler-Hegland, K.; Frymark, T.; Schooling, T.; McCabe, D.; Ashford, J.; Mullen, R.; Hammond, S.C.; Musson, N. Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part V—Applications for clinicians and researchers. J. Rehabil. Res. Dev. 2009, 46, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Shaker, R.; Kern, M.; Bardan, E.; Taylor, A.; Stewart, E.T.; Hoffmann, R.G.; Arndorfer, R.C.; Hofmann, C.; Bonnevier, J. Augmentation of deglutitive upper esophageal sphincter opening in the elderly by exercise. Am. J. Physiol. 1997, 272, G1518–G1522. [Google Scholar] [CrossRef] [PubMed]
- Shaker, R.; Easterling, C.; Kern, M.; Nitschke, T.; Massey, B.; Daniels, S.; Grande, B.; Kazandjian, M.; Dikeman, K. Rehabilitation of swallowing by exercise in tube-fed patients with pharyngeal dysphagia secondary to abnormal UES opening. Gastroenterology 2002, 122, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Belkacem, A.N.; Nishio, S.; Suzuki, T.; Ishiguro, H.; Hirata, M. Neuromagnetic Decoding of Simultaneous Bilateral Hand Movements for Multidimensional Brain-Machine Interfaces. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1301–1310. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Subjects | |||
|---|---|---|---|
| N | 196 | ||
| Male | Female | ||
| Group | Singers | 6 | 49 |
| Non-singers | 51 | 90 | |
| SD | range | ||
| Age | [years] | 11.7 | 40–93 |
| BMI | [kg/m2] | 3.2 | 16.2–38.8 |
| Grip strength | [kg] | 8.9 | 15.7–55.3 |
| RSST | [times] | 2.2 | 3–16 |
| MPT | [sec] | 9.2 | 6–62 |
| RSST | Age | BMI | Grip Strength | MPT | ||
|---|---|---|---|---|---|---|
| Singers | RSST | 1.0000 | −0.1815 | −0.2037 | 0.2219 | 0.2605 |
| Age | −0.1815 | 1.0000 | 0.2306 | −0.3093 * | −0.0192 | |
| BMI | −0.2037 | 0.2306 | 1.0000 | 0.1317 | −0.1448 | |
| Grip strength | 0.2219 | −0.3093 * | 0.1317 | 1.0000 | 0.2402 | |
| MPT | 0.2605 | −0.0192 | −0.1448 | 0.2402 | 1.0000 | |
| Non-singers | RSST | 1.0000 | −0.2344 ** | −0.0335 | 0.2446 # | 0.1778 * |
| Age | −0.2344 ** | 1.0000 | −0.1096 | −0.3150 ## | −0.2043 * | |
| BMI | −0.0335 | −0.1096 | 1.0000 | 0.3299 ## | −0.0284 | |
| Grip strength | 0.2446 # | −0.3150 ## | 0.3299 ## | 1.0000 | 0.2829 ## | |
| MPT | 0.1778 * | −0.2043 * | −0.0284 | 0.2829 ## | 1.0000 | |
| Both | RSST | 1.0000 | −0.2042 # | −0.0884 | 0.1815 * | 0.1859 ** |
| Age | −0.2042 # | 1.0000 | −0.0382 | −0.3196 ## | −0.1696 * | |
| BMI | −0.0884 | −0.0382 | 1.0000 | 0.2965 ## | −0.0501 | |
| Grip strength | 0.1815 * | −0.3196 ## | 0.2965 ## | 1.0000 | 0.2811 ## | |
| MPT | 0.1859 ** | −0.1696 * | −0.0501 | 0.2811 ## | 1.0000 |
| (A): Before matching | ||||||
| Matching Factor | Singers | Non-Singers | p-Value | Standardized | ||
| N | 55 | 141 | ||||
| Used | Gender | 0.0005 | 0.6237 | |||
| Male | ([%]) | 6 (10.9) | 51 (36.2) | |||
| Female | ([%]) | 49 (89.1) | 90 (63.8) | |||
| Age | [years] | 61.5 ± 10.2 | 59.6 ± 12.2 | 0.3039 | 0.1704 | |
| (range) | (40–82) | (40–93) | ||||
| BMI | [kg/m2] | 22.2 ± 2.9 | 22.6 ± 3.3 | 0.4302 | 0.1289 | |
| (range) | (16.9–29.8) | (16.2–38.8) | ||||
| Grip Strength | [kg] | 26.0 ± 5.8 | 31.4 ± 9.5 | 0.0001 | 0.6843 | |
| (range) | (15.7–44.3) | (15.9–55.3) | ||||
| Non-used | RSST | [times] | 7.0 ± 2.5 | 6.2 ± 2.1 | 0.0430 | 0.3134 |
| (range) | (3–16) | (3–13) | ||||
| MPT | [sec] | 22.7 ± 7.9 | 24.1 ± 9.7 | 0.3651 | 0.1504 | |
| (range) | (8–45) | (6–62) | ||||
| (B): After matching | ||||||
| Matching Factor | Singers | Non-Singers | p-Value | Standardized | ||
| N | 53 | 53 | ||||
| Used | Gender | 1.0000 | 0.0000 | |||
| Male | ([%]) | 5 (9.4) | 5 (9.4) | |||
| Female | ([%]) | 48 (90.6) | 48 (90.6) | |||
| Age | [years] | 61.4 ± 10.3 | 61.2 ± 13.5 | 0.9292 | 0.0173 | |
| (range) | (40–82) | (40–93) | ||||
| BMI | [kg/m2] | 22.1 ± 3.0 | 22.5 ± 3.6 | 0.5175 | 0.1262 | |
| (range) | (16.9–29.8) | (16.8–38.8) | ||||
| Grip Strength | [kg] | 26.2 ± 5.8 | 26.4 ± 5.9 | 0.9149 | 0.0208 | |
| (range) | (15.7–44.3) | (15.9–43.0) | ||||
| Non-used | RSST | [times] | 7.1 ± 2.4 | 5.9 ± 1.9 | 0.0109 | 0.5039 |
| (range) | (3–16) | (3–11) | ||||
| MPT | [sec] | 22.7 ± 7.8 | 22.1 ± 8.7 | 0.7162 | 0.0708 | |
| (range) | (8–45) | (10–52) | ||||
| Singers | Non-Singers | |||||
|---|---|---|---|---|---|---|
| Factor | r | 95% CI | p-Value | r | 95% CI | p-Value |
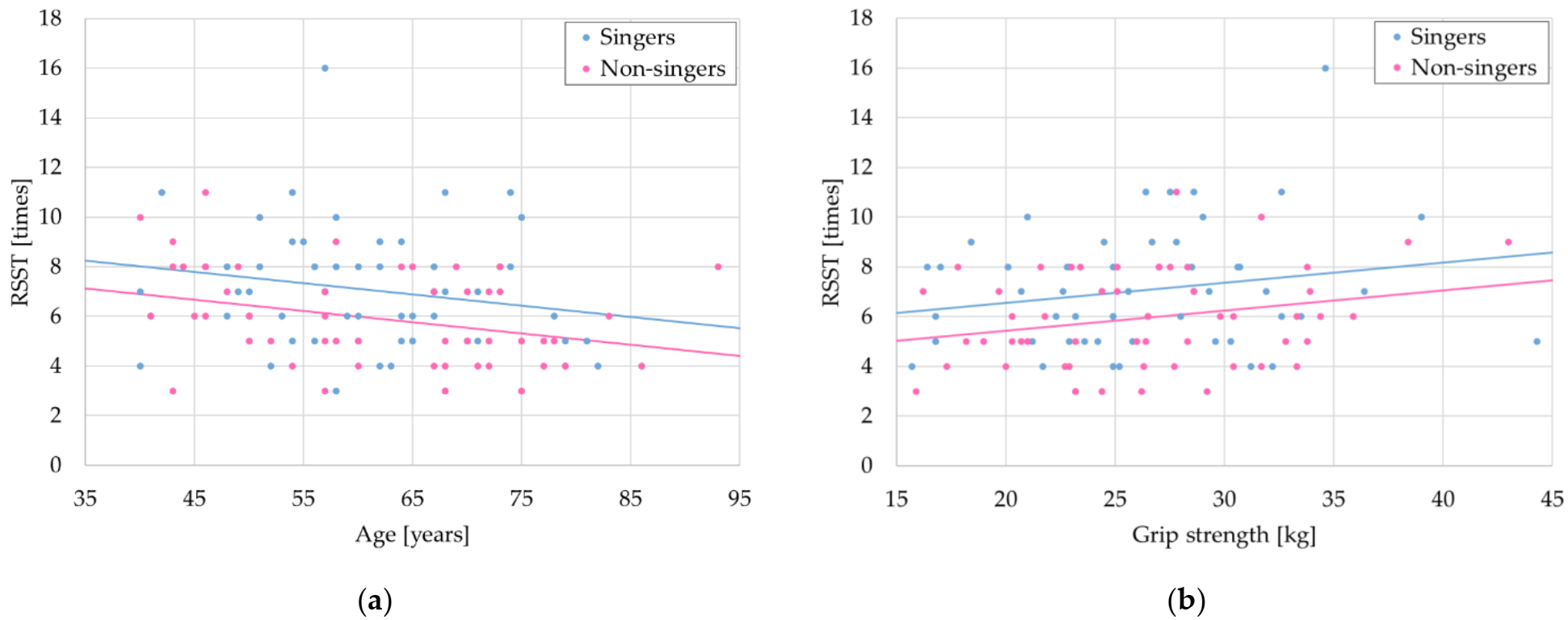
| Age | −0.1590 | −0.4116–0.1163 | 0.2554 | −0.3447 | −0.5626–−0.0821 | 0.0115 |
| BMI | −0.1930 | −0.4404–0.0815 | 0.1661 | −0.1442 | −0.3989–0.1312 | 0.3030 |
| Grip strength | 0.1859 | −0.0889–0.4344 | 0.1826 | 0.2576 | −0.0137–0.4935 | 0.0626 |
| MPT | 0.2458 | −0.0263–0.4839 | 0.0761 | 0.3258 | 0.0609–0.5478 | 0.0173 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagi, N.; Sakai, Y.; Kawamura, N.; Maezawa, H.; Hata, Y.; Hirata, M.; Kashioka, H.; Yanagida, T. Singing Experience Influences RSST Scores. Healthcare 2022, 10, 377. https://doi.org/10.3390/healthcare10020377
Yagi N, Sakai Y, Kawamura N, Maezawa H, Hata Y, Hirata M, Kashioka H, Yanagida T. Singing Experience Influences RSST Scores. Healthcare. 2022; 10(2):377. https://doi.org/10.3390/healthcare10020377
Chicago/Turabian StyleYagi, Naomi, Yoshitada Sakai, Naoko Kawamura, Hitoshi Maezawa, Yutaka Hata, Masayuki Hirata, Hideki Kashioka, and Toshio Yanagida. 2022. "Singing Experience Influences RSST Scores" Healthcare 10, no. 2: 377. https://doi.org/10.3390/healthcare10020377
APA StyleYagi, N., Sakai, Y., Kawamura, N., Maezawa, H., Hata, Y., Hirata, M., Kashioka, H., & Yanagida, T. (2022). Singing Experience Influences RSST Scores. Healthcare, 10(2), 377. https://doi.org/10.3390/healthcare10020377