
“Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature


Abstract
:1. Introduction
2. Methods
2.1. Protocol Registration
2.2. Article Identification
2.2.1. PICOs Question and Eligibility Criteria
- –
- Participants (P): Patients with “Wire Syndrome” (WS), i.e., dental movements described as aberrant, unexpected, unexplained, unwanted, or excessive;
- –
- Interventions (I): Fixed orthodontic retainer bonded at the maxilla and/or mandible after orthodontic treatment;
- –
- Comparisons (C): Patients not affected by “Wire Syndrome” (only for studies including a control group);
- –
- Outcomes (O): Define the prevalence of “Wire Syndrome” and the characteristics associated with it.
- –
- Study designs (S): All prospective and retrospective clinical studies, including case reports or series, written in English or French, clearly reporting the description, detection, or management of “Wire Syndrome” or tooth movement described as aberrant, unexpected, unwanted, or unexplained in the presence of a bonded fixed retainer placed after orthodontic treatment were included, regardless of the length of the follow-up. In vitro studies, narrative reviews, author opinions, editorials, or commentaries were excluded.
2.2.2. Search Strategy
- ❖
- Electronic search
- ❖
- Manual search
- –
- From the bibliography of articles selected by the electronic search;
- –
- From the search engine of a selection of orthodontic and dental journals:
- ○
- American Journal of Orthodontics and Dentofacial Orthopedics;
- ○
- European Journal of Orthodontics;
- ○
- Journal of Orthodontics;
- ○
- Journal of Clinical Orthodontics;
- ○
- Orthodontic & Craniofacial Research;
- ○
- The Angle Orthodontist;
- ○
- Revue d’Orthopédie Dento-Faciale;
- ○
- L’information Dentaire.
2.3. Article Selection
2.3.1. Electronic Search
- –
- Reading of titles;
- –
- Reading of abstracts;
- –
- Reading of the full text.
2.3.2. Manual Search
2.4. Data Extraction
2.5. Risk of Bias Analysis
3. Results
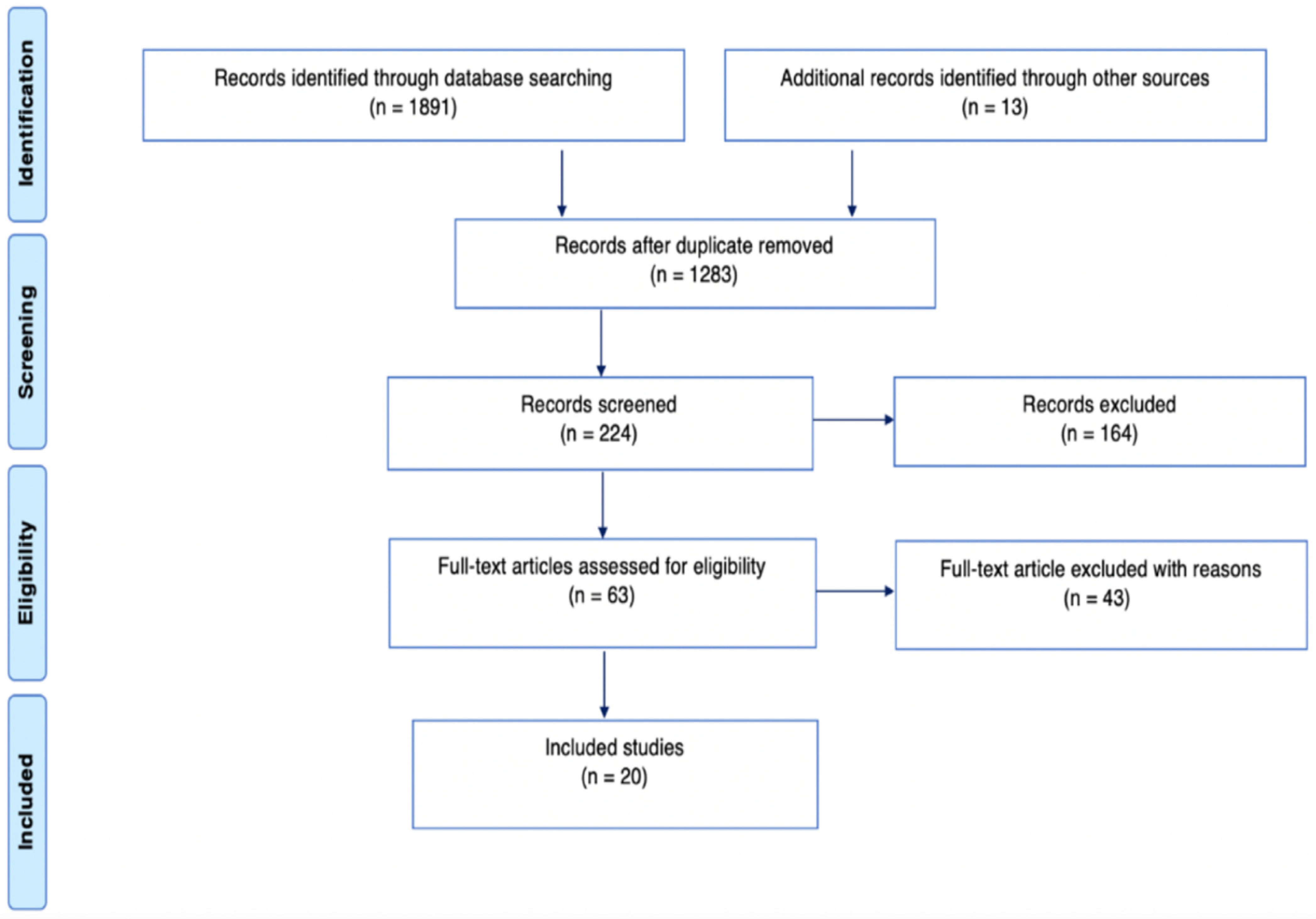
3.1. Article Selection
3.1.1. Electronic Search
3.1.2. Manual Search
3.2. Studies’ Characteristics

{kind=link}
| Authors | Publication Date | Wire Syndrome Definition |
|---|---|---|
| Katsaros et al. [1] | 2007 | Unexpected complications of bonded mandibular lingual retainers |
| Abudiak et al. [12] | 2011 | A complication with orthodontic fixed retainers |
| Renkema et al. [13] | 2011 | Unexpected posttreatment complications |
| Alessandri Bonetti et al. [14] | 2012 | Isolated-type recession defects with an abnormal buccolingual inclination |
| Pazera et al. [2] | 2012 | Severe complication of a bonded mandibular lingual retainer |
| Farret et al. [15] | 2015 | Extreme labial movement of the root |
| Roussarie et al. [3] | 2015 | Syndrome du fil |
| Kučera et al. [11,16] | 2016 | Unexpected complications/X effect, Twist effect, and non-specific complications |
| Laursen et al. [17] | 2016 | Complications after unintentional tooth displacement by active bonded retainers |
| Shaughnessy et al. [4] | 2016 | Inadvertent tooth movement with fixed lingual retainers |
| Wolf et al. [18] | 2016 | Undesired tooth movement |
| Egli et al. [10] | 2017 | Unexpected posttreatment changes |
| Jacobs et al. [19] | 2017 | Single tooth torque problems |
| Beitlitum et al. [20] | 2020 | Unwanted effects such as inadvertent tooth movement and torque changes |
| Kim et al. [21] | 2020 | Unexpected tooth movements |
| Klaus et al. [22] | 2020 | Unwanted tooth movements |
| Knaup et al. [23] | 2021 | Side effects of twistflex retainers |
| Singh et al. [5] | 2021 | Extreme complication of a fixed mandibular lingual retainer |
3.3. Bias Results
3.4. Studies’ Results
- ❖
- Flat, braided chains (Ortho FlexTech).
- ❖
- Single-stranded, round wire bonded on the canines only; diameter: 0.036 inch.
- ❖
- Round, twisted, stainless steel wire:
- Unknows strands with diameter: 0.0175 inch; 0.0215 inch; 0.0195 inch;
- Three strands with a diameter of 0.0155, 0.0195, or 0.0195 inches (heat treatment);
- Five strands with a diameter of 0.0215 inched (gold-plated);
- Six strands with a diameter of 0.0175 inches.
- ❖
- Round, coaxial, stainless steel wire:
- Six strands with a diameter of 0.018 inches.
- ❖
- Patient-related factors: Different parameters were found to be significant in WS patients, such as lower facial level increase (p < 0.0001) [11], vestibulo-position of mandibular incisors before orthodontic treatment (p = 0.029) [11], and presence of dysfunctions/parafunctions (p = 0.049) [22]. However, Klaus et al. [22] did not find any significant difference in WS patients regarding mandibular plane angle or initial vestibulo-version of the incisors.
- ❖
- Orthodontic treatment-related factors: Different parameters were found to be significant in WS patients, such as debonded at a young age (p = 0.03) [11], canine expansion and overjet reduction during treatment [18], and absence of inter-incisal contact at the end of treatment (p < 0.01) [22]. In contrast, Klaus et al. [22] found no significant difference in WS patients regarding expansion of the inter-canine distance and reduction in overjet. Kucera et al. [11] showed no significant difference regarding treatment duration (p = 0.270), inter-canine distance (p = 0.065), or change in incisor inclination (p = 0.151).
- ❖
- ❖
- Mild severity: The most common treatment was retainer removal. Some authors [10,23] observed significant improvement up to spontaneous repositioning. Stripping was recommended by Roussarie et al. [3] to facilitate teeth repositioning and avoid relapse. The correction of parafunctions was also recommended [14]. For two research teams [3,5], an observation period of six months to one year was performed after wire removal.
- ❖
- ❖
- Significant severity: Orthodontic retreatment combined with endodontic and/or periodontal treatment is indicated. Endodontic treatment is performed when the displacement of the tooth is so important that it has caused a rupture of the vascular–nervous bundle. Endodontic surgery may be associated if necessary [14,15]. In cases where periodontal surgery is indicated, the removal of retainers is beneficial [20]. In cases of extreme WS, dental avulsion is sometimes the only solution [5].
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katsaros, C.; Livas, C.; Renkema, A.M. Unexpected complications of bonded mandibular lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Pazera, P.; Fudalej, P.; Katsaros, C. Severe complication of a bonded mandibular lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Roussarie, F.; Douady, G. Effet indésirable des fils de contention collés: Le « syndrome du fil »: 1ère partie. Unwanted tooth movement produced by the bonded retention wires: The “wire syndrom”: First part. Rev. Orthop. Dento Faciale 2015, 49, 411–426. [Google Scholar] [CrossRef]
- Shaughnessy, T.G.; Proffit, W.R.; Samara, S.A. Inadvertent tooth movement with fixed lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Singh, P. Canine avulsion: An extreme complication of a fixed mandibular lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Rafflenbeul, F.; Hanriat, C.; Lefebvre, F.; Renkema, A.M.; Bolender, Y. How do general dental practitioners perceive and deal with orthodontic bonded retainers? Am. J. Orthod. Dentofac. Orthop. 2021, 160, e1–e8. [Google Scholar] [CrossRef]
- Habegger, M.; Renkema, A.M.; Bronkhorst, E.; Fudalej, P.S.; Katsaros, C. A survey of general dentists regarding orthodontic retention procedures. Eur. J. Orthod. 2017, 39, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Padmos, J.; Mei, L.; Wouters, C.; Renkema, A.M. Orthodontic retention procedures in New Zealand: A survey to benefit clinical practice guideline development. J. World Fed. Orthod. 2019, 8, 24–30. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Improving the content validity of the mixed methods appraisal tool: A modified e-Delphi study. J. Clin. Epidemiol. 2019, 111, 49–59.e41. [Google Scholar] [CrossRef] [Green Version]
- Egli, F.; Bovali, E.; Kiliaridis, S.; Cornelis, M.A. Indirect vs direct bonding of mandibular fixed retainers in orthodontic patients: Comparison of retainer failures and posttreatment stability. A 2-year follow-up of a single-center randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 15–27. [Google Scholar] [CrossRef]
- Kučera, J.; Marek, I. Unexpected complications associated with mandibular fixed retainers: A retrospective study. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Abudiak, H.; Shelton, A.; Spencer, R.J.; Burns, L.; Littlewood, S.J. A complication with orthodontic fixed retainers: A case report. Orthod. Update 2011, 4, 112–117. [Google Scholar] [CrossRef]
- Renkema, A.M.; Renkema, A.; Bronkhorst, E.; Katsaros, C. Long-term effectiveness of canine-to-canine bonded flexible spiral wire lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 614–621. [Google Scholar] [CrossRef]
- Alessandri Bonetti, G.; Incerti Parenti, S.; Zucchelli, G. Onychophagia and postorthodontic isolated gingival recession: Diagnosis and treatment. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Farret, M.M.; Farret, M.M.; da Luz Vieira, G.; Assaf, J.H.; de Lima, E.M. Orthodontic treatment of a mandibular incisor fenestration resulting from a broken retainer. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Kucera, J.; Streblov, J.; Marek, I.; Hanzelka, T. Treatment of Complications Associated with Lower Fixed Retainers. J. Clin. Orthod. 2016, 50, 54–59. [Google Scholar]
- Laursen, M.G.; Rylev, M.; Melsen, B. Treatment of Complications after Unintentional Tooth Displacement by Active Bonded Retainers. J. Clin. Orthod. 2016, 50, 290–297. [Google Scholar]
- Wolf, M.; Schulte, U.; Küpper, K.; Bourauel, C.; Keilig, L.; Papageorgiou, S.N.; Dirk, C.; Kirschneck, C.; Daratsianos, N.; Jäger, A. Post-treatment changes in permanent retention. J. Orofac. Orthop. 2016, 77, 446–453. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, C.; Katzorke, M.; Wiechmann, D.; Wehrbein, H.; Schwestka-Polly, R. Single tooth torque correction in the lower frontal area by a completely customized lingual appliance. Head Face Med. 2017, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Beitlitum, I.; Barzilay, V.; Rayyan, F.; Sebaoun, A.; Sarig, R. Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach. Int. J. Environ. Res. Public Health 2020, 17, 8060. [Google Scholar] [CrossRef]
- Kim, T.; Baek, S. Lingual bonded retainers: A case series of complications and resolutions. APOS Trends Orthod. 2020, 10, 3–11. [Google Scholar]
- Klaus, K.; Xirouchaki, F.; Ruf, S. 3D-analysis of unwanted tooth movements despite bonded orthodontic retainers: A pilot study. BMC Oral Health 2020, 20, 308. [Google Scholar] [CrossRef] [PubMed]
- Knaup, I.; Bartz, J.R.; Schulze-Späte, U.; Craveiro, R.B.; Kirschneck, C.; Wolf, M. Side effects of twistflex retainers-3D evaluation of tooth movement after retainer debonding. J. Orofac. Orthop. 2021, 82, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Roussarie, F.; Douady, G. Effet indésirable des fils de contention collés: Le « syndrome du fil »: Observations, théories, conséquences cliniques: 2e partie. Unwanted tooth movement produced by the bonded retention wire: The « wire syndrome », observations, theories, clinical consequences: Second part. Rev. Orthop. Dento Faciale 2018, 52, 327–341. [Google Scholar]
- Padmos, J.A.D.; Fudalej, P.S.; Renkema, A.M. Epidemiologic study of orthodontic retention procedures. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 496–504. [Google Scholar] [CrossRef]
- Andriekute, A.; Vasiliauskas, A.; Sidlauskas, A. A survey of protocols and trends in orthodontic retention. Prog. Orthod. 2017, 18, 31. [Google Scholar] [CrossRef] [Green Version]
- Schneider, E.; Ruf, S. Upper bonded retainers. Angle Orthod. 2011, 81, 1050–1056. [Google Scholar] [CrossRef]
- Zachrisson, B.U. Multistranded wire bonded retainers: From start to success. Am. J. Orthod Dentofac. Orthop. 2015, 148, 724–727. [Google Scholar] [CrossRef] [Green Version]
- Kučera, J.; Littlewood, S.J.; Marek, I. Fixed retention: Pitfalls and complications. Br. Dent. J. 2021, 230, 703–708. [Google Scholar] [CrossRef]
- Engeler, O.G.; Dalstra, M.; Arnold, D.T.; Steineck, M.; Verna, C. In vitro comparison of the torsional load transfer of various commercially available stainless-steel wires used for fixed retainers in orthodontics. J. Orthod. 2021, 48, 118–126. [Google Scholar] [CrossRef]
- Gelin, E.; Seidel, L.; Bruwier, A.; Albert, A.; Charavet, C. Innovative customized CAD/CAM nickel-titanium lingual retainer versus standard stainless-steel lingual retainer: A randomized controlled trial. Korean J. Orthod. 2020, 50, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. 1), S204–S213. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Data Base | Search Strategy |
|---|---|
| PubMed (MEDLINE) | (orthodontic retainer) AND (((complication OR movement OR post treatment changes OR version) AND (unexpected OR unwanted OR inadvertent)) OR (“orthodontic retainers/adverse effects” (MeSH Terms)) OR (Side effect) OR (Relapse) OR (Torque) OR (twist effect) OR (Active) |
| The Cochrane Library | (orthodontic retainer) AND (((complication OR movement OR post treatment changes OR version) AND (unexpected OR unwanted OR inadvertent)) OR (adverse event) OR (Side effect) OR (Relapse) OR (Torque) OR (twist effect) OR (Active) |
| Embase | (orthodontic retainer) AND (((complication OR movement OR post treatment changes OR version) AND (unexpected OR unwanted OR inadvertent)) OR (adverse event) OR (Side effect) OR (Relapse) OR (Torque) OR (twist effect) OR (Active) |
| Scopus | ((orthodontic AND retainer) AND (((complication OR movement OR “post treatment changes” OR version) AND (unexpected OR unwanted OR inadvertent)) OR (“adverse event”) OR (“Side effect”) OR (relapse) OR (torque) OR (“twist effect”) OR (active)) |
| Author (Year Published) Journal | Aim * | Study Design | Population | Main Results |
|---|---|---|---|---|
| Katsaros et al. [1] (2007) AJODO | Demonstrate unexpected labiolingual changes in the mandibular anterior region associated with orthodontic bonded retainers. | Case series | Patients were screened for unexpected posttreatment changes in the mandibular anterior region during a three-year period for regular posttreatment follow-up. | 21 patients presented unexpected movements, half of which required retreatment. Prevalence: 5%. Arch involved: Mandible. Observed movements: 18 patients had differences in torque between two adjacent mandibular incisors and 3 patients had significant buccal inclination and movement of one mandibular canine previously adapted on a working dental cast. Retainer: 0.0195 inch, three-strand, heat-treated twistflex wire bonded to the six mandibular anterior teeth. |
| Abudiak et al. [12] (2011) Orthodontic Update | Describe a case of severe unwanted movement, the cause of which is believed to be the activation of a multistrand bonded retainer. | Case report | 21-year-old patient completed a fixed appliance treatment five years ago and had a fixed maxilla and mandibular retainer bonded to all the teeth from canine to canine. She observed worsening displacement of teeth 12 and 13. | The patient presented unexpected movements. Arch involved: Maxilla. Observed movements: Open bite 13/43–44, height difference between the clinical crowns of 13 and adjacent teeth, excessive palatal root torque of 13, and excessive buccal root torque of 12 (apex palpable in the vestibule). Retainer: 0.0195-inch, three-strand, heat-treated twistflex wire bonded from canine to canine. Apparition delay: Two years. None of these unexpected movements were present at the end of the treatment and also did not correspond to the initial position of the teeth. Treatment: Wire removal; orthodontic retreatment; new 0.0195-inch, twisted, bonded passive retainer fabricated on a study model and placed using a jig. |
| Renkeman et al. [13] (2011) AJODO | Long-term effectiveness of flexible spiral wire canine-to-canine lingual retainers in maintaining alignment of mandibular anterior teeth. | Case series | 221 patients who received a flexible spiral wire canine-to-canine lingual retainer after active orthodontic treatment. | Of the 221 patients (75 boys and 146 girls), 6 patients presented unexpected movements, of which 3 required retreatment. Prevalence: 2.7%. Arch involved: Mandible. Observed movements: Five years after debonding, three patients had a torque difference between the two mandibular central incisors, two patients had an increased buccal inclination and movement of the mandibular left canine, and one patient had a torque difference between the two mandibular central incisors and increased buccal inclination and movement of the mandibular left canine. Retainer: 0.0195 inch, three-strand, heat-treated twist wire, bonded to the six mandibular anterior teeth. |
| Alessandri Bonetti et al. [14] (2012) AJODO | Describe the diagnosis and management of isolated-type recession defects of complex etiology. | Case series | Two post-orthodontic patients (18 and 22 years old) presented gingival recession limited to one mandibular incisor associated with abnormal buccolingual inclination despite six-unit lingual bonded retainer. | Patients presented unexpected movements. Observed movements: First patient: Labial gingival recession and excessive buccal and lingual root inclination of 41 and 31, respectively. Second patient: Gingival recession and buccal dislocation of the root on 42. Apparition delay: First patient: Five years. Second patient: Four years. Hypothetical etiology in both: Onychophagia. Retainer in both: Round, twisted, stainless steel wire bonded to the six mandibular anterior teeth. Treatment: First patient: Onychophagia managing; removal retainer; orthodontic retreatment; periodontal surgery. Second patient: As the patient refused the treatment, a worsening was observed one year later that finally induced an acceptance of treatment, as follows: Endodontic treatment on 42 (vitality loss); orthodontic retreatment; periodontal surgery; a new multibraided, rectangular, stainless steel wire was bonded from canine to canine. |
| Pazera et al. [2] (2012) AJODO | Present a severe complication of a lingual flexible spiral wire retainer. | Case report | 20-year-old patient who previously underwent an orthodontic treatment. He came to the clinic with a fracture of his wire retainer four years after debonding. | The patient presented a serious complication. Arch involved: Mandible. Observed movements: Excessive buccal root torque (35°) on 43 with significant lingual inclination of crown and buccal gingival recession. CBCT revealed that the root and its apex were almost out of the buccal bone on its buccal side. Pulp vitality was preserved. Apparition delay: Four years. Retainer: Soft, twisted wire bonded to the six anterior teeth with a fracture between 42 and 43. Treatment: Orthodontic retreatment; new 0.0215 × 0.027 inch rounded steel wire bonded to the canines only; recession was still present but the patient refused periodontal treatment. |
| Farret et al. [15] (2015) AJODO | Describe the case of a patient who underwent previous orthodontic treatment 21 years ago and had a fixed mandibular bonded retainer. | Case report | 36-year-old patient who completed orthodontic treatment 21 years previously but had his mandibular bonded retainer partially debonded and broken for four years. He came to the clinic with pain and gingival recession on 32. | The patient presented unexpected movements. Arch involved: Mandible. Observed movements: Localized open bite 33/12–13, excessive buccal crown torque of 33, and extreme labial movement of the root of 32, but the vitality test was negative. Apparition delay: 21 years. Retainer: Wire (no detail provided) bonded to the six anterior teeth and fractured between 42 and 43. The mandibular left lateral incisor stayed bonded to the retainer and received the entire load of the incisors. Treatment: Orthodontic retreatment; endodontic treatment followed by apectomy of 32; a slight residual recession remained; a new 0.016 × 0.022 inch stainless steel mandibular fixed retainer was bonded to the mandible. |
| Roussarie et al. [3] (2015) Revue d’Orthopédie Dento-Faciale | Describe Wire Syndrome associated with maxilla and mandibular bonded retainers. | Case series | 60 patients presenting Wire Syndrome. Patient’s documentation came from Dr. Roussarie’s office and from colleagues. | 60 patients presented Wire Syndrome (WS). Arches involved: Maxilla and mandible. Observed movements: Of the 40 cases observed in the mandible, 29 had a right canine with exaggerated vestibular crown torque, and 11 had a left canine with exaggerated lingual crown torque. Of the 20 cases observed in the maxilla, only 2 cases involved canines. Retainer: Three- or six-stranded twist round wires, flat braided chain, or 0.036 inch single-stranded wire bonded only on the canines. |
| Kučera et al. [11] (2016) AJODO | Describe different types of unexpected complications associated with mandibular-fixed retainers, assessing their prevalence and possible etiological causes. | Retrospective cohort study | 3500 consecutive patients (1423 men; 2077 women) who had a mandibular-fixed bonded retainer were screened for unexpected complications and then compared with a randomly selected control group of 105 patients (43 men; 62 women; 29.5 ± 9.7 years) without unexpected complications. | 38 patients (20.7 ± 8.9 years) presented unexpected complications. Prevalence: 1.1%. Arch involved: Mandible Observed movements: 21 patients had an opposite inclination of the contralateral canines = twist effect (89.5% of the left canines were tipped buccally). 12 patients had a torque difference between two adjacent incisors = X effect. Five patients had nonspecific complications. Apparition delay: 4 ± 2.8 years post-treatment. The number of intercepted unexpected complications was highest in the first five years after debonding, and then it declined with time. Retainer: 0.0215 inch, gold-plated, five-stranded spiral wire OR a 0.0175 inch, six-stranded, co-axial wire bonded to the six anterior teeth. Etiologies: Patients in the “unexpected complications” group were, at pretreatment, with a higher mandibular plane angle (p < 0.0001), as well as the position of the mandibular incisors relative to the Point A-pogonion line (p = 0.029), but no difference was observed for intercanine distance (p = 0.065) or mandibular incisor inclination to the mandibular plane (p = 0.151) between the two groups. Patients in the “unexpected complications” group were also significantly younger at debonding (p = 0.03), but there was no significant difference in treatment time (p = 0.270), wire type (p = 1.000), or failure rate (p = 0.562) between the two groups. |
| Kučera et al. [16] (2016) Journal of Clinical Orthodontics | Describe the interdisciplinary treatment of gingival recession secondary to an unexpected complication associated with a fixed mandibular retainer. | Case report | 28-year-old patient completed two orthodontic treatments, in which 14/24 and a mandibular central incisor were extracted. The patient observed 43 gradually worsening. | The patient presented an unexpected complication. Arch involved: Mandible. Observed movements: An anterior open bite, a difference in height of the clinical crowns in the anterior sector, left canine and incisor inclined buccally, and right canine and incisor inclined lingually (twist effect). On 42, a gingival recession of 4 mm with exaggerated root prominence was observed. Finally, on the panoramic, the roots of 32 and 33 were tipped. Retainer: 0.0155 inch, three-stranded twisted wire, debonded of the lower left incisor. Treatment: Orthodontic retreatment; periodontal treatment; a new fixed retainer with a five-stranded, gold-plated wire of a 0.0215 inch diameter bonded on the six anterior teeth and extended to the first premolars. |
| Laursen et al. [17] (2016) Journal of Clinical Orthodontics | Describe how to correct unwanted tooth movements with rational biomechanics. | Case series | Two patients (24 and 31 years old) completed orthodontic treatment and had a mandibular-fixed retainer. | The patients had unwanted movements. Arch involved: Mandible. Observed movements: First patient: 31 had an exaggerated labial root torque with a labial gingival recession. Second patient: 42 had exaggerated lingual root torque with a lingual gingival recession associated with lingual bone dehiscence. The tooth was still vital. Apparition delay: First patient: 10 years. Second patient: Five years. Type of wire: First patient: A flexible spiral wire. Second patient: A heat-treated, flexible spiral wire. Treatment: First patient: Retainer removal; orthodontic retreatment; periodontal treatment. Second patient: Retainer removal; orthodontic retreatment; periodontal treatment. In both cases, after retreatment, double retention: A three- (first patient) or six-stranded (second patient) spiral bonded wire associated with a vacuum-formed retainer for nighttime wear. |
| Shaughnessy et al. [4] (2016) AJODO | Illustrate inadvertent tooth movement associated with fixed retainer, debate possible causes, make recommendations, and discuss orthodontic–periodontic management. | Case report with illustrated discussion | 28-year-old patient that completed an orthodontic treatment 15 years prior and presented an intact fixed mandibular retainer. She had regular check-ups for the first year, but since then, no check-ups have been made. | The patient presented unwanted movements. Arches involved: Mandible. Observed movements: Gingival recessions, lingually on 42 and buccally on 41 with differential torque between 41 and 42. A difference in the height of the clinical crowns was observed on the anterior teeth. In the canines, the opposite inclination of 33 and 43 was noted. On the CBCT, bone fenestration was observed on 43 and 41 buccally and on 42 lingually. Apparition delay: 15 years. Retainer: 0.0195 inch twisted wire bonded to the six anterior teeth for the case report. Treatment: Retainer post-treatment; orthodontic retreatment; periodontal surgery; a removable retainer, according to the patient’s request. |
| Wolf et al. [18] (2016) Journal of Orofacial Orthopedics | Analyzed post-treatment changes in the anterior mandibular region. | Case series | 30 patients aged 24.52 ± 4.36 years completed orthodontic treatment (for at least one year of active treatment). | Prevalence of severe adverse movement: 13%, which required orthodontic retreatment. Observed movements: Superposition of each digitized and segmented tooth permitted to define the type of the movement to which each lower anterior tooth had been subjected, and in-depth analysis revealed that the canines underwent the most pronounced rotation and translation. Retainer: Dentaflex 0.45 mm, three-stranded twisted steel wire bonded to the six mandibular anterior teeth by the indirect method. |
| Egli et al. [10] (2017) AJODO | Compare direct and indirect bonded mandibular-fixed retainers and study post-treatment changes after two years. | Randomized controlled trial (RCT) | 64 consecutive patients were included in a two-arm RCT, according to an “indirect bonding group” versus a “direct bonding group”. | Of the 60 patients, five presented unexpected complications (all in the direct bonding group). Prevalence: 17%. Observed movements: Lingual crown inclination of 33. For one patient, the movement was considered clinically severe. Apparition delay: Two years. Retainer: 0.0215 inch, stainless steel, multistrand wire. Two bonding methods (direct and indirect) were employed. |
| Jacobs et al. [19] (2017) Head & Face Medicine | Analyze the efficacy and accuracy of a completely customized lingual appliance regarding the correction of the torque of a single tooth. | Case series | Three patients who completed orthodontic treatment. Patients had a torque problem on one tooth with gingival recession. | The patients had unwanted movements. Arch involved: Mandible. Observed movements: Exaggerated torque on one tooth associated with gingival recession. Retainer: A bonded retainer without further details. For two patients, the wire was partially debonded. Treatment: Orthodontic retreatment with a completely customized lingual appliance associated with a reduction in the gingival recession. |
| Roussarie et al. [24] (2018) Revue d’Orthopédie Dento-Faciale | Propose a mechanical theory to explain the apparition of Wire Syndrome. | Case series | 115 cases. Patients’ documentation came from Dr. Roussarie’s office and from colleagues. | Etiological hypotheses: The bonded retention wire is “active” due to errors during bonding, during rebonding (repair), or due to an interposition of a hard foreign object; or, in presence of a fracture at the wire/bonding interface and when a force is applied, tooth can move/rotate around the wire. Recommendation: Wires should be passive and accurately rebonded if necessary. Retainer should be performed with the utmost care. Strengthening the wire/bonding interface (avoiding wire contamination before bonding, using a metal primer after degreasing the wire, sanding the wire surface to be bonded) should take place. In the case of Wire Syndrome (WS), the wire has to be removed, and a period of monitoring is recommended to achieve spontaneous repositioning. Patients should also be aware of the risk of unwanted movement associated with the presence of a fixed retainer. |
| Beitlitum et al. [20] (2020) International Journal of Environmental Research and Public Health | Explore the benefits of a combined periodontic–orthodontic approach to resolve Miller class III gingival recession in post-orthodontic patients. | Prospective study | 15 patients presented unexpected movements, despite the presence of a bonded retainer, associated with class III gingival recession were divided into two different groups. | Two groups: (1) Bonded lingual retainer removal prior to periodontal surgery plus removable retainer at night three months after surgery; (2) periodontal surgery only (without retainer removal). Arch involved: Mandible. Retainer: All patients had a lingual bonded retainer without further details. Results: For group (1), the improvement in the average recession depth was significantly greater (4.0 ± 0.83 mm; improvement: 87.2%) compared with group (2), who showed an improvement of 43.8% (1.88 ± 1.29 mm) (p = 0.008). Retainer removal prior to the surgery was beneficial in correcting Miller class III recessions. |
| Kim et al. [21] (2020) APOS Trends in Orthodontics | Describe the types, causes, and recommendations for preventing/managing complications associated with bonded lingual retainers. | Case series | Nine patients who presented an intact fixed maxilla/mandibular retainer (no failure; no fracture). | Patients had unexpected tooth movements and gingival problems. Arches involved: Mandible and maxilla. Retainer: Maxillary or mandibular 0.0175 inch, multistrand wire bonded from canine to canine with a Duralay resin transfer method and a removable retainer (both arches) for night wearing. Observed movements: Several types of complications were described: Change in the transverse position, angulation, or torque of the crown, gingival recession, and non-specific complications such as space openings, misalignment, and appearance of black triangle. |
| Klaus et al. [22] (2020) BMC Oral Health | Analyze the prevalence of undesirable tooth movement despite an intact fixed bonded retainer and identify possible predisposing factors. | Retrospective cohort study | Patients had completed previous orthodontic treatment and had a bonded canine-to-canine retainer. Patients with a removable retainer were excluded. | Of the 163 patients, 44 patients had adverse movements. Prevalence: 27%. Arches involved: Maxilla and mandible. Retainer: 0.018 inch, six-stranded coaxial wire. Movement observed: Maxillary retainers (20.9%) were more concerned than mandibular retainers (14%). Median amount of tooth movement: 0–0.66 mm with a large interindividual variation of up to 2.58 mm. Risk factors: These risk factors, associated with the occurrence of adverse movements, were dysfunction or parafunction (p = 0.049) and lacked inter-incisal contact (p < 0.01). No significant differences were found for the mandibular plane angle before treatment, amount of incisor proclination, expansion of the inter-canine distance, and overjet reduction during treatment. |
| Knaup et al. [23] (2021) Journal of Orofacial Orthopedics | Measure tooth movement after retainer removal in cases of misalignment associated with a bonded retainer. | Case series (pilot study) | Patients completed orthodontic treatment, presented a fixed lingual retainer in the upper/lower jaw, and presented visible overcrowding. The existing retainers were removed to discontinue the present forces. | 23 teeth were analyzed (12 upper teeth: 10 incisors, two canines; 11 lower teeth: 7 incisors, 4 canines). Arches concerned: Maxillary and mandibular. Retainer: Flexible, round spiral wire. Observed movements: Several types of movements were described and also measured. Misaligned teeth bonded to fixed retainers demonstrated movement when those retainers were debonded. These observations also highlight the impression that retainers might be able to provoke active force, which could be responsible for iatrogenic tooth movements. |
| Singh et al. [5] (2021) AJODO | Describe a serious complication (canine completely avulsed) with a mandible bonded retainer | Case report | The patient (26 years old) completed orthodontic treatment with four premolar extractions 10 years earlier. The patient had received a mandibular bonded wire from canine to canine and removable retainers on both jaws. The removable retainers were prescribed the first year. | The patient had a severe complication that required the avulsion of the right mandibular canine. Involved arch: Mandible. Observed movements: 43 had torqued 70° labially, the apex was short and totally exposed. 42 presented lingual root torque. 32 was localized labially, and the apex was nearly exposed. An anterior and right lateral open bite was present. Generalized root resorptions from 20% to 40% were observed on the panoramic radiograph. The patient did not report any significant pain. Retainer: Supposition: Multistrand, twisted, fractured between 42 and 43. Apparition delay: 10 years. Treatment: Avulsion 43; retainer removal; nonsurgical periodontal therapy; six-month latency period. No further orthodontic intervention was advised because of the periodontal health and the presence of root resorptions. |
| Movement Families Associated with WS |
|---|
| X effect Torque differential between two adjacent incisors |
| Twist effect Opposite inclination between the two contralateral canines |
| Excessive crown and/or root torque Incisors or canines, which presents an exaggerated modification of the torque |
| Non-specific complications Diastema openings, differences in incisor heights, etc. |
| Associated movements “X effect” AND Torque modification; “X effect” AND “twist effect” Or any other possible combination |
| Practitioner-Related Etiologies [1,2,4,5,10,11,12,16,18,20,21,22] |
| - Insufficient passivity |
| - Wire iatrogenic deformation during bonding |
| Wire-related etiologies [1,2,4,5,10,11,12,14,16,18,19,20,21,22,24] |
| - Wire deformation (chewing force or hard foods, traumatic application after dental floss, other harmful habits, or by parafunctions such as onychophagia) |
| - Modification or instability of the mechanical properties of wires: Wire fatigue, wire activation, and “despiralization” of the wire strands |
| - Adhesive failure at the adhesive/wire interface with the application of an external force |
| - Undetected wire debonded |
| - Fracture of the wire (remaining bonded to one or more teeth) |
| Patient-related etiologies [18,19] |
| - Physiological changes |
| Recommendations to Bond the Retainer |
|---|
| - Careful manufacture of a passive wire on a dental model (precise adaptation, avoid any stress) [4,19,21] |
| - Indirect bonding method is indicated to avoid wire deformation by finger or instrument pressure [4,21] |
| - Bonding canines and central incisors only to improve patient sensitivity in the case of debonding [4] |
| - Strengthen the wire/adhesive liaison (avoid wire contamination before bonding, using a metal primer after degreasing the wire and sanding the wire surface to be bonded [24]) |
| - Prescribe a removable retainer, in addition to the fixed retainer, for nighttime wear [4,5,18,21] |
| Recommendations for follow-up after retainer placement |
| - Regular check-ups [4,5,13,15,19] |
| - Early detection with systematic search for all signs of WS during retainer visits [1,2,4,5,11,13,14,15,21] |
| - Educate and inform patients about WS [1,2,11,13,15,21,24] |
| - Educate and inform all dental practitioners (general practitioners, periodontists, and orthodontists) about WS [2,3,5,13,21] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charavet, C.; Vives, F.; Aroca, S.; Dridi, S.-M. “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare 2022, 10, 379. https://doi.org/10.3390/healthcare10020379
Charavet C, Vives F, Aroca S, Dridi S-M. “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare. 2022; 10(2):379. https://doi.org/10.3390/healthcare10020379
Chicago/Turabian StyleCharavet, Carole, France Vives, Sofia Aroca, and Sophie-Myriam Dridi. 2022. "“Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature" Healthcare 10, no. 2: 379. https://doi.org/10.3390/healthcare10020379
APA StyleCharavet, C., Vives, F., Aroca, S., & Dridi, S.-M. (2022). “Wire Syndrome” Following Bonded Orthodontic Retainers: A Systematic Review of the Literature. Healthcare, 10(2), 379. https://doi.org/10.3390/healthcare10020379