
Structural Model of Retention Intention of Nurses in Small- and Medium-Sized Hospitals: Based on Herzberg’s Motivation-Hygiene Theory


Abstract
:1. Introduction
Conceptual Basis and Hypothetical Model
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Measures
2.3.1. Calling
2.3.2. Resilience
2.3.3. Leader–Member Exchange
2.3.4. Workplace Bullying
2.3.5. Nursing Work Environment
2.3.6. Job Satisfaction
2.3.7. Intention to Stay
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. General Characteristics of the Subjects
3.2. Descriptive Statistics and Normality Test for the Measured Variable
3.3. Hypothesis Model Test
3.3.1. Goodness-of-Fit Test for the Hypothesis Model
3.3.2. Correlation between Measured Variables and Multicollinearity
3.3.3. Discriminant Validity
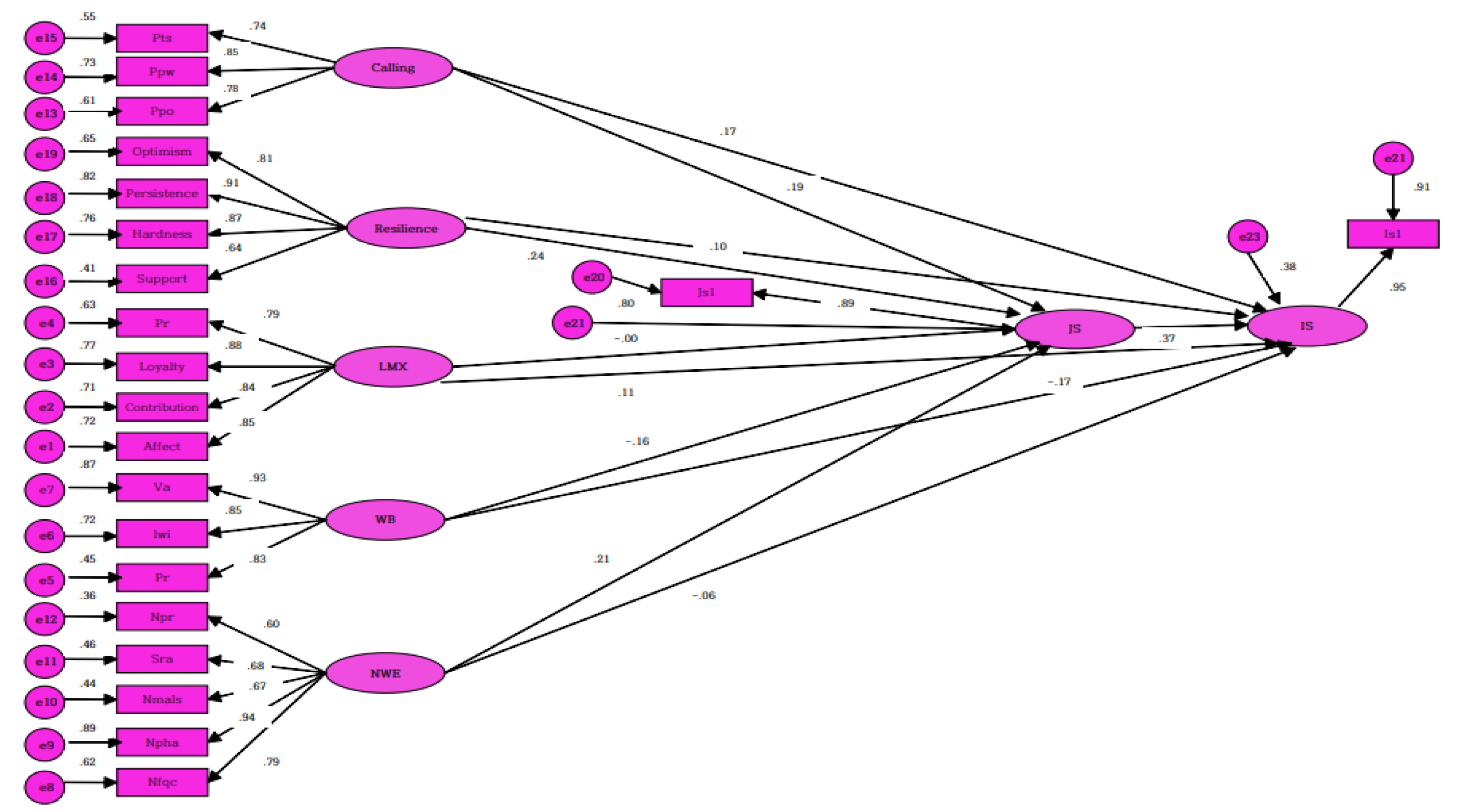
3.3.4. Verifying Effectiveness of the Hypothesis Model
3.3.5. Effectiveness Analysis of the Final Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hwang, N.M.; Kim, D.J. An overview of the nursing systems of france and germany. Health Welf. Policy Forum 2017, 217, 76–89. [Google Scholar]
- Korea Health Industry Development Institute. Statistics for Hospital Management [Internet]; Korea Health Industry Development Institute: Cheongju, Korea, 2016; [Updated 2018 April]; Available online: www.alio.go.kr/informationResearchView.do?seq=2375726 (accessed on 2 September 2021).
- Kwon, J.O.; Kim, E.Y. Impact of unit-level nurse practice environment on nurse turnover intention in the small and medium sized hospitals. Korean Acad. Nurs. Adm. 2012, 18, 414–423. [Google Scholar] [CrossRef] [Green Version]
- Bae, E.J.; Kim, K.Y. The effect of stress coping ability and recovery resilience on retention intention of nurses in medium-sized hospitals. J. Korea Acad. -Ind. Coop. Soc. 2018, 19, 662–671. [Google Scholar] [CrossRef]
- Baloch, Q.B.; Zaman, G.; Jamshed, J. Determinants of job satisfaction and employees turnover intentions. Abasyn J. Soc. Sci. 2014, 7, 118–136. [Google Scholar]
- Mark, B.A.; Harless, D.W.; McCue, M.; Xu, Y. A longitudinal examination of hospital registered nurse staffing and quality of care. Health Serv. Res. 2004, 39, 279–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, K.H.; Lim, Y.J. Influence of Professionalism, Role conflict and work environment in clinical nurses with expanded role on job embeddedness. J. Korean Acad. Nurs. Adm. 2016, 22, 424–436. [Google Scholar] [CrossRef]
- Howe, A.L.; King, D.S.; Ellis, J.M.; Wells, Y.D.; Wei, Z.; Teshuva, K.A. Stabilising the aged care workforce: An analysis of worker retention and intention. Aust. Health Rev. 2012, 36, 83–91. [Google Scholar] [CrossRef]
- Han, S.Y.; Lee, H.C. Intention to leave versus intention to stay, are they simply opposed concept?: Focused on comparison between flight attendants of full service carrier and low cost carrier. Korean J. Hosp. Tour. 2015, 24, 53–72. [Google Scholar]
- Lee, J.Y.; Lee, M.H. A study on calling, resilience, leader-member exchange and nursing work environment of nurses in small and medium sized hospital. J. Digit. Converg. 2020, 18, 313–321. [Google Scholar] [CrossRef]
- Herzberg, F. The motivation-hygiene concept & problem of manpower. Pers. Adm. 1964, 27, 3–7. [Google Scholar]
- Owe, H.O.; Kim, W.G.; Noh, E.K. The effects of nursing practice environment and peer group caring interaction on retention intention among small and medium-sized hospital nurses. J. Converg. Inf. Technol. 2019, 9, 83–92. [Google Scholar] [CrossRef]
- Kim, M.H.; Park, J.M. A study on the factor of retention intention on nurses in small and medium-sized hospitals. J. Korea Entertain. Ind. Assoc. 2020, 14, 195–203. [Google Scholar] [CrossRef]
- Lee, E.H.; Cho, K.S.; Son, H.M. A study of hospital nurse’s intention to keep nursing job. J. Korean Clin. Nurs. Res. 2014, 20, 15–27. [Google Scholar] [CrossRef]
- Dik, B.J.; Duffy, R.D. Calling and vocation at work: Definitions and prospects for research and practice. Couns. Psychol. 2008, 37, 424–450. [Google Scholar] [CrossRef]
- Park, J.O.; Jung, K.I. Effects of advanced beginner-stage nurses’ sense of calling, job satisfaction and organizational commitment on retention intention. J. Korean Acad. Nurs. Adm. 2016, 22, 137–147. [Google Scholar] [CrossRef] [Green Version]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The connor-davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Park, E.J.; Lee, Y.M. Effect of professinal autonomy, communication satisfaction, and resilience on the job satisfaction of intensive care unit nurses. J. Korean Crit. Care Nurs. 2018, 11, 63–74. [Google Scholar]
- Lee, J.G.; Park, J.H. The role of trust and value congruence as a mediator between superior‘s transformational, transactional leadership and outcomes. Korean Manag. Rev. 2003, 32, 925–954. [Google Scholar]
- Portoghese, I.; Galletta, M.; Battistlli, A.; Leiter, M.P. A multilevel investigation on nursing turnover intention: The cross-level role of leader-member exchange. J. Nurs. Manag. 2015, 23, 754–764. [Google Scholar] [CrossRef]
- Lee, Y.J.; Lee, M.H. Development and validity of workplace bullying in nursing-type inventory. J. Korean Acad. Nurs. 2014, 44, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.L.; Park, E.O. Comparison of organziational culture and organizational commitment based on experience of workplace bullying in clinical nurses. Korean J. Occup. Health Nurs. 2017, 26, 197–206. [Google Scholar] [CrossRef]
- Cho, E.H.; Choi, M.N.; Kim, E.Y.; Yoo, I.Y.; Lee, N.J. Construct validity and reliability of the korean version of the practice environment scale of nursing work index for korean nurses. J. Korean Acad. Nurs. 2011, 41, 325–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rafferty, A.M.; Ball, J.; Aiken, L.H. Are teamwork and professional autonomy compatible and do the result in improved hospital care? Qual. Health Care 2001, 10, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Bae, B.R. Structural Equation Modeling with AMOS 24; Chungrim Publishing: Seoul, Korea, 2017. [Google Scholar]
- Sim, Y.L.; Yoo, S.K. Development and validation of the korean version of the calling and vocation questionnaire(CVQ-K). Korean J. Couns. Psychother. 2012, 24, 847–872. [Google Scholar]
- Liden, R.C.; Maslyn, J.M. Multidimensionality of leader- member exchange: An empirical assessment through scale development. J. Manag. 2003, 24, 43–72. [Google Scholar] [CrossRef]
- Lake, E.T. Development of the practice environment scale of the nursing work index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef]
- Cowin, L.S. The effects of nurse’s job satisfaction on retention. J. Nurs. Assoc. 2002, 32, 283–291. [Google Scholar] [CrossRef]
- Kim, M.J. The Effect of Nursing Organizational Culture on Nurses’ Intention of Retention. Master’s Thesis, Hanyang University, Seoul, Korea, 2006. [Google Scholar]
- Yom, Y.H.; Yang, I.S.; Han, J.H. Effects of workplace bullying, job stress, self-esteem, and burnout on the intention of university hospital nurses to keep nursing job. J. Korean Acad. Nurs. Adm. 2017, 23, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Kang, K.J.; Yu, S.J.; Park, M. Factors affecting retention intention of male nurses working health care institution in korea. J. Korean Acad. Nurs. Adm. 2017, 23, 280–289. [Google Scholar] [CrossRef]
- Saunders, P.; Huynh, A.; Goodman, D.J. Defining workplace bullying behavior professional lay definitions of workplace bullying. Int. J. Law Psychiatry 2007, 30, 340–354. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Categories | n | % | Mean ± SD |
|---|---|---|---|---|
| Gender | Male | 30 | 8.6 | |
| Female | 318 | 91.4 | ||
| Age (year) | 20~29 | 153 | 44.0 | 33.47 ± 9.17 |
| 30~39 | 101 | 29.0 | ||
| 40~49 | 70 | 20.1 | ||
| ≥50 | 24 | 6.9 | ||
| Marital status | Married | 158 | 45.4 | |
| Single | 190 | 54.6 | ||
| Education level | Diploma | 140 | 40.2 | |
| Bachelor | 194 | 55.8 | ||
| ≥Graduate | 14 | 4.0 | ||
| Period working in the current department (years) | <1 | 70 | 20.1 | 6.54 ± 7.44 |
| 1~<3 | 96 | 27.6 | ||
| 3~<5 | 41 | 11.8 | ||
| 5~<10 | 49 | 14.1 | ||
| ≥10 | 92 | 26.4 | ||
| Clinical career (years) | <1 | 32 | 9.2 | 9.24 ± 8.17 |
| 1~<3 | 67 | 19.2 | ||
| 3~<5 | 43 | 12.4 | ||
| 5~<10 | 64 | 18.4 | ||
| ≥10 | 142 | 40.8 | ||
| Position | Staff nurse | 317 | 91.1 | |
| ≥Charge nurse | 31 | 8.9 | ||
| Type of unit | Medical ward | 96 | 27.6 | |
| Surgical ward | 95 | 27.3 | ||
| Special part | 86 | 24.7 | ||
| Comprehensive nursing care service ward | 62 | 17.8 | ||
| Outpatient | 9 | 2.6 | ||
| Work shift | Three shifts | 227 | 65.2 | |
| Two shifts | 28 | 8.1 | ||
| Full-time | 78 | 22.4 | ||
| Night shift | 15 | 4.3 |
| Latent Variable | Measured Variable | Min | Max | Mean ± SD | Skewness | Kurtosis | CR | AVE |
|---|---|---|---|---|---|---|---|---|
| Calling | 1.17 | 3.75 | 2.17 ± 0.49 | 0.55 | 0.48 | 0.94 | 0.63 | |
| Transcendental calling | 1.00 | 4.00 | 1.93 ± 0.63 | 0.44 | 0.05 | |||
| Purpose/Meaning | 1.00 | 4.00 | 2.34 ± 0.55 | 0.34 | 0.27 | |||
| Prosocial orientation | 1.00 | 4.00 | 2.25 ± 0.52 | 0.09 | 0.19 | |||
| Resilience | 0.81 | 3.97 | 2.58 ± 0.55 | −0.03 | 0.04 | 0.95 | 0.66 | |
| Hardness | 0.67 | 3.89 | 2.36 ± 0.59 | 0.09 | 0.19 | |||
| Patience | 0.88 | 4.00 | 2.54 ± 0.58 | 0.13 | 0.07 | |||
| Optimism | 0.25 | 4.00 | 2.47 ± 0.70 | −0.08 | 0.01 | |||
| Support | 1.00 | 4.00 | 2.93 ± 0.69 | −0.48 | −0.18 | |||
| Spirituality | 0.00 | 4.00 | 2.09 ± 0.77 | 0.07 | −0.14 | |||
| Leader–member exchange | 1.17 | 5.00 | 3.55 ± 0.61 | 0.01 | 0.29 | 0.95 | 0.71 | |
| Affect | 1.00 | 5.00 | 3.52 ± 0.68 | 0.04 | 0.27 | |||
| Loyalty | 1.67 | 5.00 | 3.52 ± 0.71 | 0.04 | −0.12 | |||
| Contribution | 1.00 | 5.00 | 3.46 ± 0.66 | −0.12 | 0.31 | |||
| Professional Respect | 1.00 | 5.00 | 3.71 ± 0.73 | −0.24 | 0.11 | |||
| Workplace Bulling | 1.00 | 3.42 | 2.57 ± 0.53 | 0.82 | 0.25 | 0.95 | 0.68 | |
| Verbal attacks | 1.00 | 4.00 | 1.87 ± 0.62 | 0.44 | −0.36 | |||
| Improper work instruction | 1.00 | 3.75 | 1.83 ± 0.62 | 0.46 | −0.37 | |||
| Physical treat | 1.00 | 3.50 | 1.37 ± 0.59 | 1.54 | 1.68 | |||
| Nursing Work Environment | 1.59 | 3.88 | 2.57 ± 0.42 | 0.16 | 0.02 | 0.95 | 0.56 | |
| Participation in hospital affairs | 1.00 | 3.89 | 2.49 ± 0.50 | −0.08 | 0.01 | |||
| Nursing foundation for quality of care | 1.44 | 4.00 | 2.65 ± 0.44 | −0.14 | 0.15 | |||
| Nursing manager ability, leader ship, and support | 1.50 | 4.00 | 2.91 ± 0.50 | −0.14 | −0.08 | |||
| Staffing and resource adequacy | 1.00 | 3.75 | 2.24 ± 0.65 | 0.08 | −0.67 | |||
| Nurse-physician relations | 1.00 | 4.00 | 2.58 ± 0.57 | −0.57 | 0.52 | |||
| Job satisfaction | 1.00 | 10.00 | 5.74 ± 1.90 | −0.12 | −0.52 | 0.82 | 0.80 | |
| Retention intention | 1.00 | 8.00 | 5.21 ± 1.43 | −0.21 | −0.07 | 0.84 | 0.91 | |
| Calling | Resilience | LMX | Workplace Bulling | NWE | JS | IS | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | |
| 1 | 1 | |||||||||||||||||||||
| 2 | 0.62 | 1 | ||||||||||||||||||||
| 3 | 0.64 | 0.65 | 1 | |||||||||||||||||||
| 4 | 0.28 | 0.45 | 0.33 | 1 | ||||||||||||||||||
| 5 | 0.32 | 0.54 | 0.39 | 0.79 | 1 | |||||||||||||||||
| 6 | 0.32 | 0.46 | 0.33 | 0.72 | 0.71 | 1 | ||||||||||||||||
| 7 | 0.11 | 0.28 | 0.17 | 0.54 | 0.60 | 0.53 | 1 | |||||||||||||||
| 8 | 0.45 | 0.29 | 0.26 | 0.41 | 0.38 | 0.47 | 0.24 | 1 | ||||||||||||||
| 9 | 0.17 | 0.23 | 0.17 | 0.19 | 0.22 | 0.19 | 0.21 | 0.15 | 1 | |||||||||||||
| 10 | 0.18 | 0.21 | 0.21 | 0.22 | 0.25 | 0.21 | 0.23 | 0.20 | 0.74 | 1 | ||||||||||||
| 11 | 0.18 | 0.26 | 0.19 | 0.31 | 0.32 | 0.26 | 0.23 | 0.17 | 0.71 | 0.74 | 1 | |||||||||||
| 12 | 0.08 | 0.14 | 0.12 | 0.17 | 0.23 | 0.15 | 0.17 | 0.10 | 0.68 | 0.69 | 0.67 | 1 | ||||||||||
| 13 | −0.04 | −0.08 | 0.07 | −0.11 | −0.16 | −0.11 | −0.26 | 0.05 | −0.25 | −0.23 | −0.24 | −0.14 | 1 | |||||||||
| 14 | 0.00 | −0.12 | 0.04 | −0.12 | −0.20 | −0.17 | −0.26 | 0.01 | −0.21 | −0.21 | −0.23 | −0.18 | 0.79 | 1 | ||||||||
| 15 | 0.08 | −0.09 | 0.01 | −0.13 | −0.17 | −0.13 | −0.29 | 0.06 | −0.13 | −0.14 | −0.14 | −0.14 | 0.63 | 0.56 | 1 | |||||||
| 16 | 0.14 | 0.16 | 0.16 | 0.17 | 0.18 | 0.15 | 0.13 | 0.46 | 0.50 | 0.46 | 0.47 | 0.47 | −0.15 | −0.19 | −0.10 | 1 | ||||||
| 17 | 0.18 | 0.15 | 0.21 | 0.13 | 0.13 | 0.15 | 0.07 | 0.19 | 0.03 | 0.13 | 0.11 | 0.06 | −0.05 | −0.17 | 0.09 | 0.41 | 1 | |||||
| 18 | 0.17 | 0.24 | 0.25 | 0.18 | 0.21 | 0.15 | 0.14 | 0.13 | 0.09 | 0.21 | 0.15 | 0.16 | −0.06 | −0.14 | −0.03 | 0.39 | 0.45 | 1 | ||||
| 19 | 0.23 | 0.21 | 0.22 | 0.17 | 0.21 | 0.19 | 0.07 | 0.21 | 0.23 | 0.32 | 0.26 | 0.25 | −0.04 | −0.13 | 0.09 | 0.61 | 0.66 | 0.57 | 1 | |||
| 20 | 0.16 | 0.15 | 0.16 | 0.11 | 0.14 | 0.14 | 0.09 | 0.18 | 0.22 | 0.24 | 0.19 | 0.25 | −0.03 | −0.05 | 0.03 | 0.58 | 0.49 | 0.45 | 0.75 | 1 | ||
| 21 | 0.23 | 0.37 | 0.19 | 0.31 | 0.34 | 0.36 | 0.27 | 0.23 | 0.20 | 0.16 | 0.26 | 0.13 | −0.17 | −0.23 | −0.12 | 0.25 | 0.32 | 0.21 | 0.27 | 0.20 | 1 | |
| 22 | 0.23 | 0.42 | 0.17 | 0.31 | 0.35 | 0.37 | 0.27 | 0.20 | 0.31 | 0.18 | 0.34 | 0.17 | −0.27 | −0.25 | −0.23 | 0.23 | 0.11 | 0.09 | 0.16 | 0.16 | 0.45 | 1 |
| Latent Variable | Calling | Resilience | LMX | WB | NWE | JS | IS |
|---|---|---|---|---|---|---|---|
| r | |||||||
| r2 | |||||||
| (p) | |||||||
| Calling | 0.63 † | ||||||
| resilience | 0.44 | 0.66 † | |||||
| 0.19 | |||||||
| (<0.001) | |||||||
| LMS | 0.23 | 0.29 | 0.71 † | ||||
| 0.05 | 0.08 | ||||||
| (<0.001) | (<0.001) | ||||||
| WB | −0.01 | −0.24 | −0.24 | 0.68 † | |||
| 0 | 0.08 | 0.06 | |||||
| –0.89 | (<0.001) | (<0.001) | |||||
| NWE | 0.27 | 0.21 | 0.33 | −0.09 | 0.56 † | ||
| 0.07 | 0.05 | 0.11 | 0.01 | ||||
| (<0.001) | (<0.001) | (<0.0014) | −0.085 | ||||
| JS | 0.31 | 0.37 | 0.21 | −0.20 | 0.32 | 0.80 † | |
| 0.09 | 0.14 | 0.04 | 0.04 | 0.1 | |||
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | (<0.001) | |||
| IS | 0.31 | 0.38 | 0.28 | −0.28 | 0.18 | 0.45 | 0.91 † |
| 0.1 | 0.14 | 0.08 | 0.24 | 0.03 | 0.2 | ||
| (<0.001) | (<0.001) | −0.001 | (<0.001) | (<0.001) | (<0.001) | ||
| Endogenous Variable | Exodoenous Variable | B | SE | β | CR (t) | p | Direct Effect (p) | Indirect Effect (p) | Total Effect (p) | SMC |
|---|---|---|---|---|---|---|---|---|---|---|
| Job satisfaction | Calling | 0.53 | 0.21 | 0.19 | 2.46 | 0.014 | 0.19 (0.039) | − | 0.19 (0.039) | 0.288 |
| Recovery resilience | 0.61 | 0.19 | 0.24 | 3.17 | 0.002 | 0.24 (0.007) | − | 0.24 (0.007) | ||
| Leader–member exchange relationship | −0.00 | 0.13 | −0.00 | −0.02 | 0.983 | −0.00 0.997 | − | −0.00 (0.997) | ||
| Workplace harassment | −0.46 | 0.17 | −0.16 | −2.64 | 0.008 | −0.16 (0.019) | − | −0.16 (0.019) | ||
| Nursing Work environment | 0.68 | 0.20 | 0.21 | 3.42 | <0.001 | 0.21 (0.018) | − | 0.21 (0.018) | ||
| Retention Intention | Calling | 0.44 | 0.18 | 0.17 | 2.43 | 0.015 | 0.17 (0.106) | 0.07 (0.039) | 0.24 (0.023) | 0.378 |
| Recovery resilience | 0.23 | 0.16 | 0.10 | 1.43 | 0.154 | 0.10 (0.225) | 0.09 (0.016) | 0.19 (0.034) | ||
| Leader–member exchange relationship | 0.20 | 0.11 | 0.11 | 1.88 | 0.060 | 0.11 (0.073) | −0.00 (0.996) | 0.11 (0.081) | ||
| Workplace harassment | −0.46 | 0.16 | −0.17 | −3.12 | 0.002 | −0.17 (0.011) | −0.06 (0.022) | −0.23 (0.016) | ||
| Nursing Work environment | −0.18 | 0.17 | −0.06 | −1.04 | 0.300 | −0.06 (0.381) | 0.08 (0.009) | 0.02 (0.689) | ||
| Job satisfaction | 0.35 | 0.06 | 0.37 | 5.66 | <0.001 | 0.37 (0.021) | − | 0.37 (0.021) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.Y.; Lee, M.H. Structural Model of Retention Intention of Nurses in Small- and Medium-Sized Hospitals: Based on Herzberg’s Motivation-Hygiene Theory. Healthcare 2022, 10, 502. https://doi.org/10.3390/healthcare10030502
Lee JY, Lee MH. Structural Model of Retention Intention of Nurses in Small- and Medium-Sized Hospitals: Based on Herzberg’s Motivation-Hygiene Theory. Healthcare. 2022; 10(3):502. https://doi.org/10.3390/healthcare10030502
Chicago/Turabian StyleLee, Joo Yeon, and Mi Hyang Lee. 2022. "Structural Model of Retention Intention of Nurses in Small- and Medium-Sized Hospitals: Based on Herzberg’s Motivation-Hygiene Theory" Healthcare 10, no. 3: 502. https://doi.org/10.3390/healthcare10030502