
Low-Pressure Laparoscopy Using the AirSeal System versus Standard Insufflation in Early-Stage Endometrial Cancer: A Multicenter, Retrospective Study (ARIEL Study)



 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Operative Procedure
2.2. Statistical Analysis
3. Results
3.1. Anesthesia Parameter Results
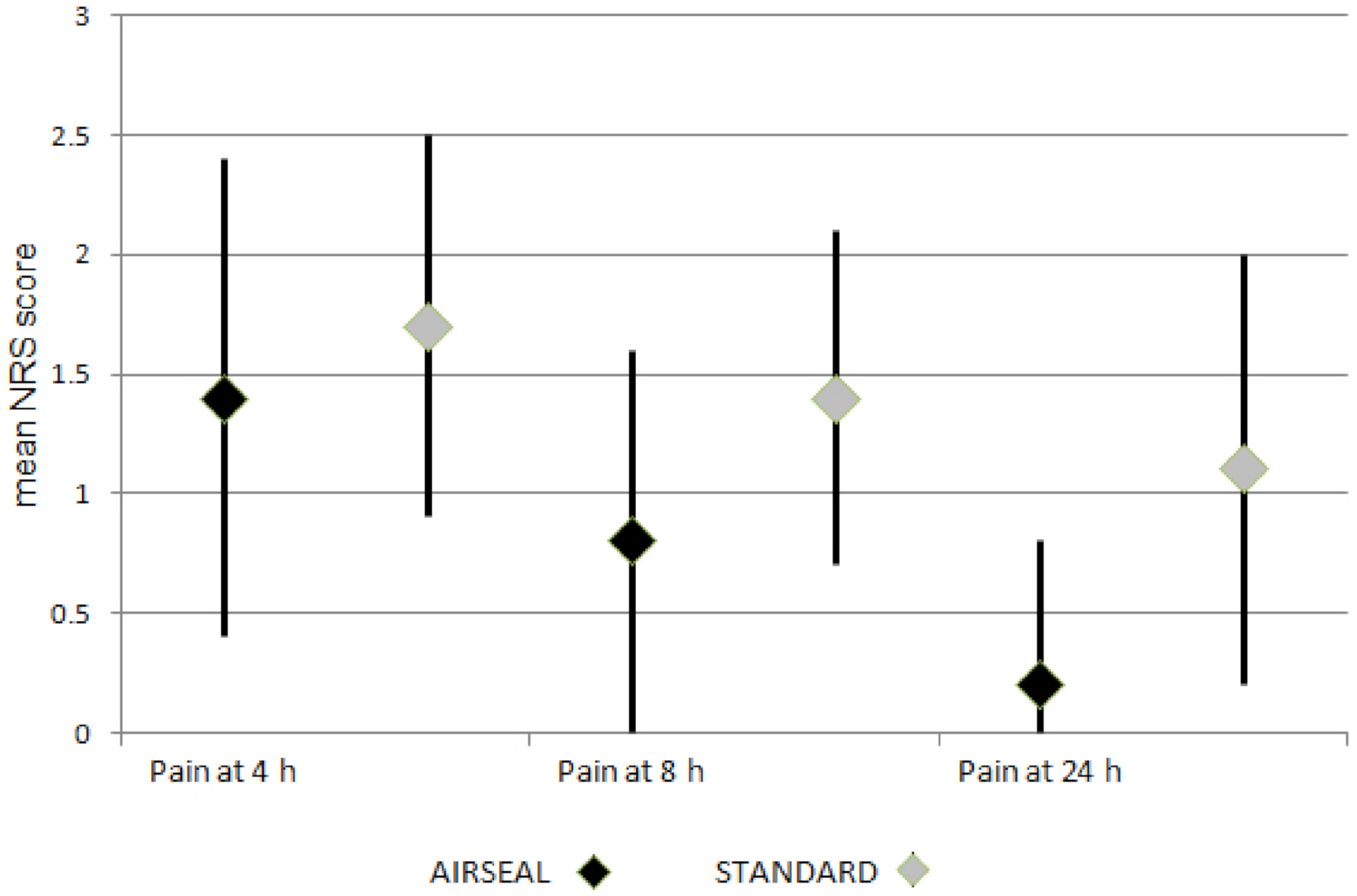
3.2. Pain Control Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Spiegel, G.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J. Clin. Oncol. 2009, 27, 5331–5336. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rustum, N.R.; Yashar, C.M.; Bean, S.; Bradley, K.; Campos, S.M.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; Damast, S.; et al. Uterine Neoplasms, Version 1.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.D. Laparoscopic Hysterectomy for Endometrial Cancer: A Procedure 25 Years in the Making. JAMA 2017, 317, 1215–1216. [Google Scholar] [CrossRef] [PubMed]
- Bouwman, F.; Smits, A.; Lopes, A.; Das, N.; Pollard, A.; Massuger, L.; Bekkers, R.; Galaal, K. The impact of BMI on surgical complications and outcomes in endometrial cancer surgery--an institutional study and systematic review of the literature. Gynecol. Oncol. 2015, 139, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Sroussi, J.; Elies, A.; Rigouzzo, A.; Louvet, N.; Mezzadri, M.; Fazel, A.; Benifla, J.L. Low pressure gynecological laparoscopy (7 mmHg) with AirSeal® System versus a standard insufflation (15 mmHg): A pilot study in 60 patients. J. Gynecol. Obstet. Hum. Reprod. 2017, 146, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.T.; Wolfe, B.M. The physiologic effects of pneumoperitoneum in the morbidly obese. Ann. Surg. 2005, 241, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Jardon, K.; Maleysson, E.; D’Arpiany, F.; Canis, M.; Botchorishvili, R. Impact of intraperitoneal pressure of a CO2 pneumoperitoneum on the surgical peritoneal environment. Hum. Reprod. 2012, 27, 1613–1623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyerges, A. Pain mechanisms in laparoscopic surgery. Semin. Laparosc. Surg. 1994, 1, 215–218. [Google Scholar]
- Luketina, R.R.; Knauer, M.; Köhler, G.; Koch, O.O.; Strasser, K.; Egger, M.; Emmanuel, K. Comparison of a standard CO2 pressure pneumoperitoneum insufflator versus AirSeal™: Study protocol of a randomized controlled trial. Trials 2014, 15, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herati, A.S.; Andonian, S.; Rais-Bahrami, S.; Atalla, M.A.; Srinivasan, A.K.; Richstone, L.; Kavoussi, L.R. Use of the valveless trocar system reduces carbon dioxide absorption during laparoscopy when compared with standard trocars. Urology 2011, 77, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Covotta, M.; Claroni, C.; Torregiani, G.; Naccarato, A.; Tribuzi, S.; Zinilli, A.; Forastiere, E. A prospective, randomized, clinical trial on the effects of a valveless trocar on respiratory mechanics during robotic radical cystectomy: A pilot study. Anesth. Analg. 2017, 124, 1794–1801. [Google Scholar] [CrossRef] [PubMed]
- Bucur, P.; Hofmann, M.; Menhadji, A.; Abedi, G.; Okhunov, Z.; Rinehart, J.; Landman, J. Comparison of pneumoperitoneum stability between a valveless trocar system and conventional insufflation: A prospective randomized trial. Urology 2016, 94, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Hagemann, A.R.; McCourt, C.K.; Varaday, S.S.; Moore, K.N. Defining and mitigating the challenges of an older and obese population in minimally invasive gynecologic cancer surgery. Gynecol. Oncol. 2018, 148, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Uccella, S.; Cromi, A.; Serati, M.; Casarin, I.; Pinelli, C.; Ghezzi, F. Low vs standard pneumoperitoneum pressure during laparoscopic hysterectomy: Prospective randomized trial. J. Minim. Invasive Gynecol. 2014, 21, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Madueke-Laveaux, O.S.; Advincula, A.; Grimes, C.L.; Walters, R.; Kim, J.H.; Simpson, K.; Truong, M.; Young, C.; Landau, R.; Ryntz, T. Comparison of Carbon Dioxide Absorption Rates in Gynecologic Laparoscopy with a Valveless versus Standard Insufflation System: Randomized Controlled Trial. J. Minim. Invasive Gynecol. 2020, 27, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Piedmonte, M.R.; Spirtos N.M. Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic oncology group LAP2 study. J. Clin. Oncol. 2012, 30, 695–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinkelspiel, H.E.; Wright, J.D.; Lewin, S.N.; Herzog, T.J. Contemporary clinical management of endometrial cancer. Obstet. Gynecol. Int. 2013, 2013, 583891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheib, S.A.; Tanner, E., 3rd; Green, I.C.; Fadre, A.N. Laparoscopy in the morbidly obese: Physiologic considerations and surgical techniques to optimize success. J. Minim. Invasive Gynecol. 2014, 21, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations-2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | AirSeal (N = 84) | Standard (N = 68) | p Value |
|---|---|---|---|
| Age | |||
| median (range) | 63 (52–73) | 65 (54–75) | |
| 0.275 | |||
| BMI, kg/m2, median (range) | 30.0 (23.7–36.4) | 27.9 (22.6–33.2) | 0.142 |
| FIGO stage, n (%) | 0.980 | ||
| IA | 54 (64.3) | 44 (65.7) | |
| IB | 14 (16.7) | 12 (17.9) | |
| II | 4 (4.8) | 3 (4.5) | |
| III | 12 (14.3) | 8 (11.9) | |
| Atypical Hyperplasia | - | 1 | |
| Grading, n (%) | 0.006 | ||
| G1 | 48 (57.1) | 20 (31.3) | |
| G2 | 24 (28.6) | 27 (42.2) | |
| G3 | 12 (14.3) | 17 (26.6) | |
| NA | 0 | 4 | |
| Histotype, n (%) | 0.013 | ||
| Complex hyperplasia | 0 | 1 (1.5) | |
| Endometrioid | 80 (95.2) | 58 (85.3) | |
| Serous | - | 6 (8.8) | |
| MMT & others | 4 (4.8) | 3 (4.4) | |
| LVSI, n (%) | 0.121 | ||
| Present | 23 (27.4) | 12 (17.7) | |
| Absent | 59 (72.6) | 56 (82.3) | |
| NA | 2 | 0 | |
| Previous surgery, n (%) | 28 (33.3) | 29 (42.7) | 0.174 |
| Smoke habit, n (%) | 29 (34.5) | 23 (33.8) | 0.507 |
| Pulmonary disease, n (%) | 11 (13.1) | 11 (16.2) | 0.393 |
| ASA score, n (%) | 0.433 | ||
| 1 | 12 (14.3) | 7 (10.3) | |
| 2 | 43 (51.2) | 42 (61.8) | |
| 3 | 29 (34.5) | 19 (27.9) |
| Variable | AirSeal (N = 84) | Standard (N = 68) | p Value |
|---|---|---|---|
| Estimated blood loss, mL | 0.880 | ||
| median (range) | 122.0 (77.6–166.4) | 121.0 (79.6–162.4) | |
| SLN detection, n (%) | 0.176 | ||
| Bilateral | 70 (83.3) | 52 (76.5) | |
| Monolateral | 9 (10.7) | 13 (19.1) | |
| Failed mapping | 5 (6) | 3 (4.4) | |
| Lymph nodes removed | 4 (0–9) | 7 (0–17) | 0.101 |
| median (range) | |||
| CO2 IAP, mmHg | |||
| median (range) | 8.5 (7.5–9.5) | 11.3 (10.2–12.4) | <0.0001 |
| Global pain at 4 h, | |||
| median (range) | 1.4 (0.4–2.4) | 1.7 (0.9–2.5) | 0.023 |
| Global pain at 8 h, | |||
| median (range) | 0.8 (0–1.6) | 1.4 (0.7–2.1) | <0.0001 |
| Global pain at 24 h, | 0.2 (0–0.8) | ||
| median (range) | 1.1 (0.2–2.0) | <0.0001 | |
| Shoulder pain, n (%) | |||
| Yes | 6 (7.1) | 20 (29.4) | |
| No | 78 (92.9) | 48 (70.6) | <0.0001 |
| Morphine consumption, n (%) | |||
| Yes | 4 (4.8) | 19 (27.9) | |
| No | 80 (95.2) | 49 (72.1) | <0.0001 |
| ETCO2, mmHg, | |||
| median (range) | 33.7 (31.4–36.0) | 35.8 (32.3–39.3) | <0.0001 |
| Peak airway pressure, cm H2O, median (range) | |||
| 21.8 (16.3–27.3) | 24.8 (21.5–28.1) | <0.0001 | |
| Max systolic arterial pressure, mmHg, median (range) | |||
| 111.7 (98.2–125.2) | 133.5 (119.7–147.3) | <0.0001 | |
| Total CO2 used, liters, | |||
| median (range) | 34.1 (29.9–38.3) | 47.9 (41.7–54.1) | <0.0001 |
| Duration of surgery, minutes, median (range) | . | ||
| 113 (91.8–134.2) | 119 (84.4–153.6) | 0.445 | |
| Length of stay, days, | 2.0 (1.4–2.6) | 2.2 (1.4–3.0) | 0.224 |
| median (range) | |||
| Major complications, n (%) | 0 | 2 (2.9) | - |
| Variables | AirSeal | Standard | p Value |
|---|---|---|---|
| (n° = 32) | (n° = 35) | ||
| Age | |||
| median (range) | 62 (58–69.3) | 65 (57–77) | 0.343 |
| Previous surgery | |||
| yes | 11 (34.4%) | 18 (51.4%) | 0.123 |
| Smoke habit | |||
| yes | 12 (37.5%) | 10 (28.6%) | 0.603 |
| Pulmonary disease | |||
| yes | 6 (18.8%) | 8 (22.9%) | 0.457 |
| ASA, n (%) | |||
| 1 | 5 (15.6%) | 1 (2.9%) | |
| 2 | 15 (46.9%) | 23 (65.7%) | 0.137 |
| 3 | 12 (37.5%) | 11 (31.4%) | |
| Et-CO2, | |||
| median (range) | 32 (31–33) | 34 (32.4–37) | 0.0004 |
| Peak airway pressure, median (range) | |||
| 19 (17–22.4) | 25 (20–25) | 0.0030 | |
| Max systolic pressure | |||
| median (range) | 105 (95–116.3) | 130 (120–137.2) | <0.0001 |
| Total CO2 used, liters | |||
| Median (range) | 30 (30–35) | 45 (40–50) | <0.0001 |
| Surgical time, minutes, | |||
| median (range) | 100 (90.120) | 101.9 (80–130) | 0.283 |
| Blood loss, mL, | |||
| median (range) | 100 (99.6–100) | 100 (100–120) | 0.497 |
| NRS pain at 4 h, median (range) | |||
| 1 (0–1) | 1 (1–2) | 0.062 | |
| NRS pain at 8 h | |||
| median (range) | 0 (0–1) | 1 (0–1) | 0.0034 |
| NRS pain at 24 h | |||
| median (range) | 0 (0–0) | 1 (0–1) | 0.0005 |
| Shoulder pain, n (%) | |||
| yes | 2 (6.3) | 10 (28.6) | 0.018 |
| Morphine consumption, n (%) | |||
| yes | |||
| 2 (6.3) | 14 (40.0) | 0.001 | |
| Length of stay, days | |||
| 1–2 | 28 (87.5) | 24 (68.6) | |
| 3 | 4 (12.5) | 11 (31.4) | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buda, A.; Di Martino, G.; Borghese, M.; Restaino, S.; Surace, A.; Puppo, A.; Paracchini, S.; Ferrari, D.; Perotto, S.; Novelli, A.; et al. Low-Pressure Laparoscopy Using the AirSeal System versus Standard Insufflation in Early-Stage Endometrial Cancer: A Multicenter, Retrospective Study (ARIEL Study). Healthcare 2022, 10, 531. https://doi.org/10.3390/healthcare10030531
Buda A, Di Martino G, Borghese M, Restaino S, Surace A, Puppo A, Paracchini S, Ferrari D, Perotto S, Novelli A, et al. Low-Pressure Laparoscopy Using the AirSeal System versus Standard Insufflation in Early-Stage Endometrial Cancer: A Multicenter, Retrospective Study (ARIEL Study). Healthcare. 2022; 10(3):531. https://doi.org/10.3390/healthcare10030531
Chicago/Turabian StyleBuda, Alessandro, Giampaolo Di Martino, Martina Borghese, Stefano Restaino, Alessandra Surace, Andrea Puppo, Sara Paracchini, Debora Ferrari, Stefania Perotto, Antonia Novelli, and et al. 2022. "Low-Pressure Laparoscopy Using the AirSeal System versus Standard Insufflation in Early-Stage Endometrial Cancer: A Multicenter, Retrospective Study (ARIEL Study)" Healthcare 10, no. 3: 531. https://doi.org/10.3390/healthcare10030531