
Can Lung Ultrasound Be the Ideal Monitoring Tool to Predict the Clinical Outcome of Mechanically Ventilated COVID-19 Patients? An Observational Study

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Study Population
2.3. Lung Ultrasound Examination
2.4. Recorded Data
2.5. Study Outcome
2.6. Statistical Analysis
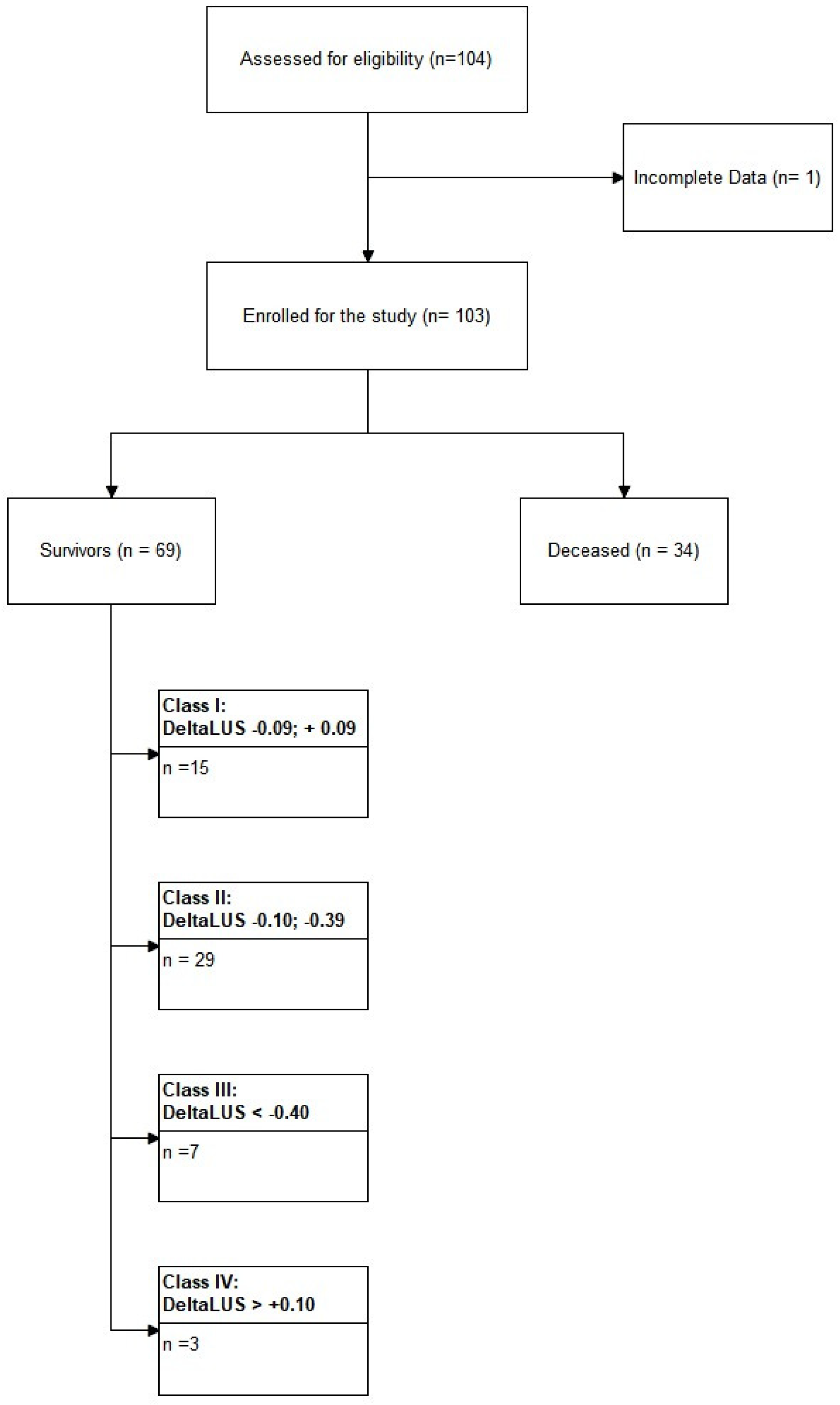
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy: Early Experience and Forecast during an Emergency Response. JAMA 2020, 323, 1545–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovács, A.; Palásti, P.; Veréb, D.; Bozsik, B.; Palkó, A.; Kincses, Z.T. The sensitivity and specificity of chest CT in the diagnosis of COVID-19. Eur. Radiol. 2021, 31, 2819–2824. [Google Scholar] [CrossRef]
- Buonsenso, D.; Pata, D.; Chiaretti, A. COVID-19 outbreak: Less stethoscope, more ultrasound. Lancet Respir. Med. 2020, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Portale, G.; Ciolina, F.; Arcari, L.; Giraldi, G.D.L.; Danti, M.; Pietropaolo, L.; Camastra, G.; Cordischi, C.; Urbani, L.; Proietti, L.; et al. Lung Ultrasound in COVID-19: Clinical Correlates and Comparison with Chest Computed Tomography. SN Compr. Clin. Med. 2021, 3, 2075–2081. [Google Scholar] [CrossRef] [PubMed]
- Meroi, F.; Orso, D.; Vetrugno, L.; Bove, T. Lung Ultrasound Score in Critically Ill COVID-19 Patients: A Waste of Time or a Time-Saving Tool? Acad. Radiol. 2021, 28, 1323–1324. [Google Scholar] [CrossRef] [PubMed]
- Bouhemad, B.; Mongodi, S.; Via, G.; Rouquette, I. Ultrasound for "lung monitoring" of ventilated patients. Anesthesiology 2015, 122, 437–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpicelli, G.; Gargani, L.; Perlini, S.; Spinelli, S.; Barbieri, G.; Lanotte, A.; Casasola, G.G.; Nogué-Bou, R.; Lamorte, A.; Agricola, E.; et al. Lung ultrasound for the early diagnosis of COVID-19 pneumonia: An international multicenter study. Intensive Care Med. 2021, 47, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Persona, P.; Valeri, I.; Zarantonello, F.; Forin, E.; Sella, N.; Andreatta, G.; Correale, C.; Serra, E.; Boscolo, A.; Volpicelli, G.; et al. Patients in intensive care unit for COVID-19 pneumonia: The lung ultrasound patterns at admission and discharge. An observational pilot study. Ultrasound J. 2021, 13, 1–7. [Google Scholar] [CrossRef]
- Stecher, S.S.; Anton, S.; Fraccaroli, A.; Götschke, J.; Stemmler, H.J.; Barnikel, M. Lung ultrasound predicts clinical course but not outcome in COVID-19 ICU patients: A retrospective single-center analysis. BMC Anesthesiol. 2021, 21, 178. [Google Scholar] [CrossRef]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, G.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensive Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Vetrugno, L.; Mojoli, F.; Boero, E.; Berchialla, P.; Bignami, E.G.; Orso, D.; Cortegiani, A.; Forfori, F.; Corradi, F.; Cammarota, G.; et al. Level of Diffusion and Training of Lung Ultrasound during the COVID-19 Pandemic—A National Online Italian Survey (ITALUS) from the Lung Ultrasound Working Group of the Italian Society of Anesthesia, Analgesia, Resuscitation, and Intensive Care (SIAARTI). Ultraschall Med. 2022. [Google Scholar] [CrossRef]
- Dargent, A.; Chatelain, E.; Kreitmann, L.; Quenot, J.P.; Cour, M.; Argaud, L.; COVID-LUS study group. Lung ultrasound score to monitor COVID-19 pneumonia progression in patients with ARDS. PLoS ONE 2020, 15, e0236312. [Google Scholar] [CrossRef]
- Ji, L.; Cao, C.; Gao, Y.; Zhang, W.; Xie, Y.; Duan, Y.; Kong, S.; You, M.; Ma, R.; Jiang, L.; et al. Prognostic value of bedside lung ultrasound score in patients with COVID-19. Crit Care. 2020, 24, 700. [Google Scholar] [CrossRef]
- de Alencar, J.C.G.; Marchini, J.F.M.; Marino, L.O.; da Costa Ribeiro, S.C.; Bueno, C.G.; da Cunha, V.P.; Lazar Neto, F.; Brandão Neto, R.A.; Souza, H.P.; COVID U. S. P. Registry Team. Lung ultrasound score predicts outcomes in COVID-19 patients admitted to the emergency department. Ann. Intensive Care 2021, 11, 6. [Google Scholar] [CrossRef]
- Gil-Rodríguez, J.; Pérez de Rojas, J.; Aranda-Laserna, P.; Benavente-Fernández, A.; Martos-Ruiz, M.; Peregrina-Rivas, J.A.; Guirao-Arrabal, E. Ultrasound findings of lung ultrasonography in COVID-19: A systematic review. Eur. J. Radiol. 2020, 148, 110156. [Google Scholar] [CrossRef]
- Volpicelli, G.; Gargani, L. Sonographic signs and patterns of COVID-19 pneumonia. Ultrasound J. 2020, 12, 22. [Google Scholar] [CrossRef]
- Vetrugno, L.; Bove, T.; Orso, D.; Bassi, F.; Boero, E.; Ferrari, G. Lung Ultrasound and the COVID-19 “Pattern”: Not All That Glitters Today Is Gold Tomorrow. J. Ultrasound Med. 2020, 39, 2281–2282. [Google Scholar] [CrossRef]
- Copetti, R.; Amore, G.; Di Gioia, C.C.; Orso, D. First comes the A, then the B: What we learned from the COVID-19 outbreak. Eur. J. Intern. Med. 2020, 80, 108–110. [Google Scholar] [CrossRef]
- Volpicelli, G.; Cardinale, L.; Fraccalini, T. Are Lung Ultrasound Findings in COVID-19 Pneumonia Typical or Specific? Praxis 2021, 110, 421–425. [Google Scholar] [CrossRef]
- Razazi, K.; Boissier, F.; Neuville, M.; Jochmans, S.; Tchir, M.; May, F.; de Prost, N.; Brun-Buisson, C.; Carteaux, G.; Mekontso Dessap, A. Pleural effusion during weaning from mechanical ventilation: A prospective observational multicenter study. Ann. Intensive Care 2018, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.S.; Wang, X.; Ye, L.L.; Niu, Y.R.; Peng, W.B.; Wang, Z.H.; Zhang, J.C.; Zhou, Q. Pleural effusion as an indicator for the poor prognosis of COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14123. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, L.; Baciarello, M.; Bignami, E.; Bonetti, A.; Saturno, F.; Orso, D.; Girometti, R.; Cereser, L.; Bove, T. The “pandemic” increase in lung ultrasound use in response to COVID-19: Can we complement computed tomography findings? A narrative review. Ultrasound J. 2020, 12, 39. [Google Scholar] [CrossRef] [PubMed]
- McDermott, C.; Daly, J.; Carley, S. Combatting COVID-19: Is ultrasound an important piece in the diagnostic puzzle? Emerg. Med. J. 2020, 37, 644–649. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Survived | Deceased | p-Value | |
|---|---|---|---|---|
| n = 103 | n = 69 | n = 34 | ||
| Age (years) | 67.0 (10.9) | 65.4 (12.0) | 70.3 (7.46) | 0.013 |
| Sex (male) | 81 (78.6%) | 54 (78.3%) | 27 (79.4%) | NS |
| BMI | 23.0 (14.3) | 22.3 (14.4) | 24.5 (14.1) | NS |
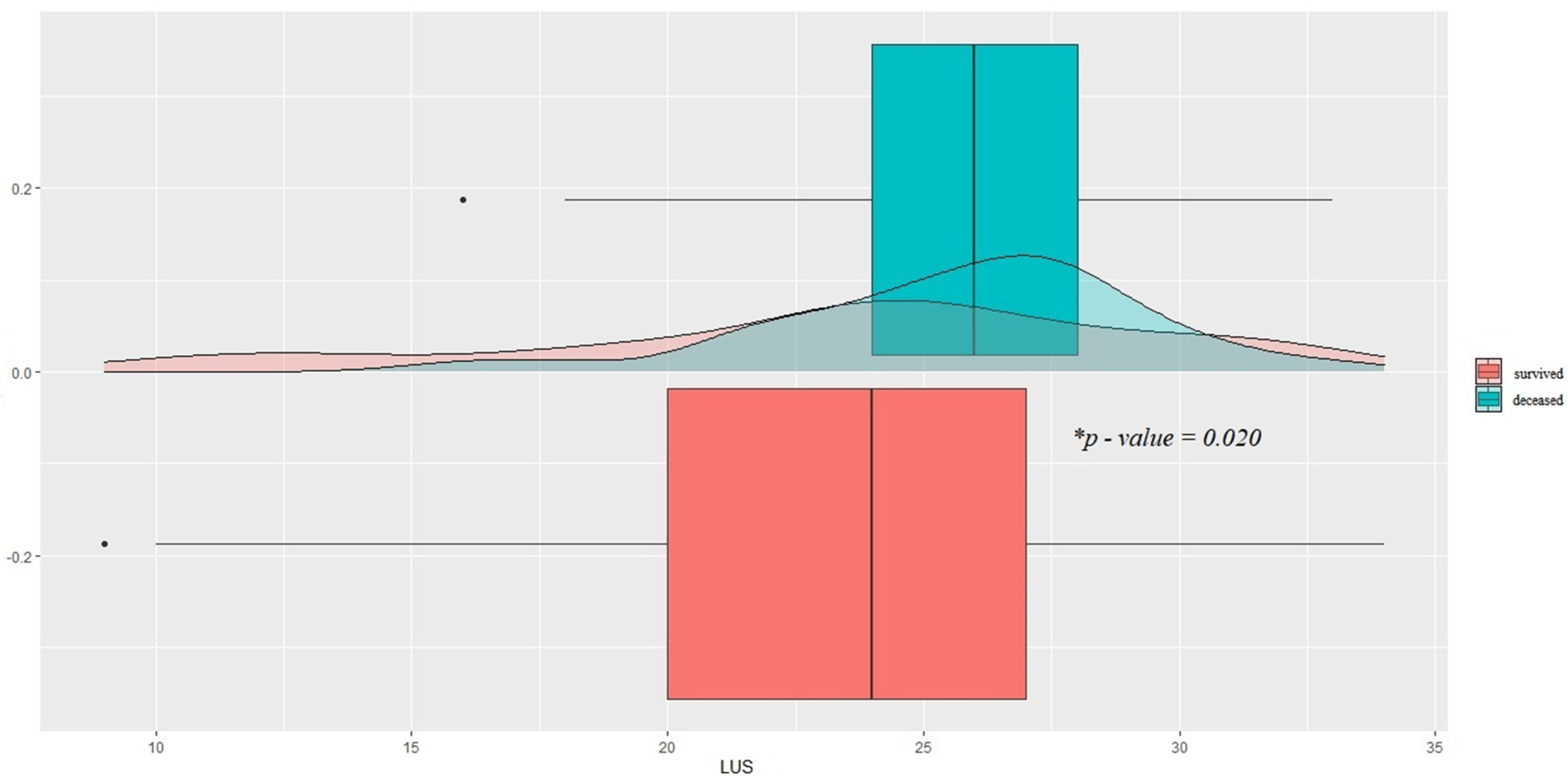
| LUS (t0) | 24.2 (5.44) | 23.5 (6.06) | 25.7 (3.54) | 0.020 |
| CPR (t0) | 11.8 (31.4) | 12.7 (35.3) | 9.91 (21.8) | NS |
| Il-6 (t0) | 100 (192) | 110 (217) | 69.6 (62.8) | NS |
| D-dimer (t0) FEUng/mL | 6337 (17,825) | 3039 (5958) | 13,030 (28,984) | NS |
| CPR (t1) | 6.44 (13.1) | 5.97 (15.7) | 7.40 (4.97) | NS |
| Il-6 (t1) | 55.2 (77.0) | 37.4 (34.3) | 111 (133) | NS |
| D-dimer (t1) FEUng/mL | 2310 (3764) | 1719 (1966) | 3510 (5798) | NS |
| Spon Breath (days) | 2.17 (2.55) | 3.12 (2.58) | 0.24 (0.85) | <0.001 |
| Controlled Mech. Vent. (days) | 6.04 (5.77) | 4.84 (6.28) | 8.47 (3.54) | <0.001 |
| Assisted Mech. Vent. (days) | 3.80 (5.06) | 3.97 (5.42) | 3.44 (4.30) | NS |
| Inhaled NO2 (days) | 0.91 (3.10) | 0.96 (3.57) | 0.82 (1.88) | NS |
| Hypertension | 63 (61.2%) | 41 (59.4%) | 22 (64.7%) | NS |
| Prev. Myocard. Infarction | 5 (4.85%) | 3 (4.35%) | 2 (5.88%) | NS |
| Chr. Heart failure | 5 (4.85%) | 3 (4.35%) | 2 (5.88%) | NS |
| Periph. Vascular disease | 11 (10.7%) | 6 (8.70%) | 5 (14.7%) | NS |
| Cerebrovascular disease | 5 (4.85%) | 3 (4.35%) | 2 (5.88%) | NS |
| Cognitive Impairment | 1 (0.97%) | 1 (1.45%) | 0 | NS |
| COPD | 17 (16.5%) | 9 (13.0%) | 8 (23.5%) | NS |
| Connective tissue diseases | 3 (2.91%) | 1 (1.45%) | 2 (5.88%) | NS |
| Gastric diseases | 1 (0.97%) | 0 | 1 (2.94%) | NS |
| Mild liver disease | 3 (2.91%) | 3 (4.35%) | 0 | NS |
| Moderate to severe liver disease | 1 (0.97%) | 1 (1.45%) | 0 | NS |
| Diabetes | 16 (15.5%) | 12 (17.4%) | 4 (11.8%) | NS |
| Diabetes with organ dysfunction | 7 (6.80%) | 4 (5.80%) | 3 (8.82%) | NS |
| Chronic renal failure | 8 (7.77%) | 2 (2.90%) | 6 (17.6%) | 0.015 |
| Solid neoplasm | 3 (2.91%) | 3 (4.35%) | 0 | NS |
| Leukemia | 3 (2.91%) | 1 (1.45%) | 2 (5.88%) | NS |
| Lymphoma | 2 (1.94%) | 1 (1.45%) | 1 (2.94%) | NS |
| Autoimmune Diseases | 4 (3.88%) | 2 (2.90%) | 2 (5.88%) | NS |
| Smoking | 14 (13.6%) | 9 (13.0%) | 5 (14.7%) | NS |
| Substance Use Disorder | 2 (1.94%) | 0 | 2 (5.88%) | NS |
| Chronic immunosuppressive therapy | 6 (5.83%) | 3 (4.35%) | 3 (8.82%) | NS |
| Chronic corticosteroid therapy | 2 (1.94%) | 1 (1.45%) | 1 (2.94%) | NS |
| Home oxygen therapy | 3 (2.91%) | 3 (4.35%) | 0 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vetrugno, L.; Meroi, F.; Orso, D.; D’Andrea, N.; Marin, M.; Cammarota, G.; Mattuzzi, L.; Delrio, S.; Furlan, D.; Foschiani, J.; et al. Can Lung Ultrasound Be the Ideal Monitoring Tool to Predict the Clinical Outcome of Mechanically Ventilated COVID-19 Patients? An Observational Study. Healthcare 2022, 10, 568. https://doi.org/10.3390/healthcare10030568
Vetrugno L, Meroi F, Orso D, D’Andrea N, Marin M, Cammarota G, Mattuzzi L, Delrio S, Furlan D, Foschiani J, et al. Can Lung Ultrasound Be the Ideal Monitoring Tool to Predict the Clinical Outcome of Mechanically Ventilated COVID-19 Patients? An Observational Study. Healthcare. 2022; 10(3):568. https://doi.org/10.3390/healthcare10030568
Chicago/Turabian StyleVetrugno, Luigi, Francesco Meroi, Daniele Orso, Natascia D’Andrea, Matteo Marin, Gianmaria Cammarota, Lisa Mattuzzi, Silvia Delrio, Davide Furlan, Jonathan Foschiani, and et al. 2022. "Can Lung Ultrasound Be the Ideal Monitoring Tool to Predict the Clinical Outcome of Mechanically Ventilated COVID-19 Patients? An Observational Study" Healthcare 10, no. 3: 568. https://doi.org/10.3390/healthcare10030568
APA StyleVetrugno, L., Meroi, F., Orso, D., D’Andrea, N., Marin, M., Cammarota, G., Mattuzzi, L., Delrio, S., Furlan, D., Foschiani, J., Valent, F., & Bove, T. (2022). Can Lung Ultrasound Be the Ideal Monitoring Tool to Predict the Clinical Outcome of Mechanically Ventilated COVID-19 Patients? An Observational Study. Healthcare, 10(3), 568. https://doi.org/10.3390/healthcare10030568