
STORK: Collaborative Online Monitoring of Pregnancies Complicated with Gestational Diabetes Mellitus

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
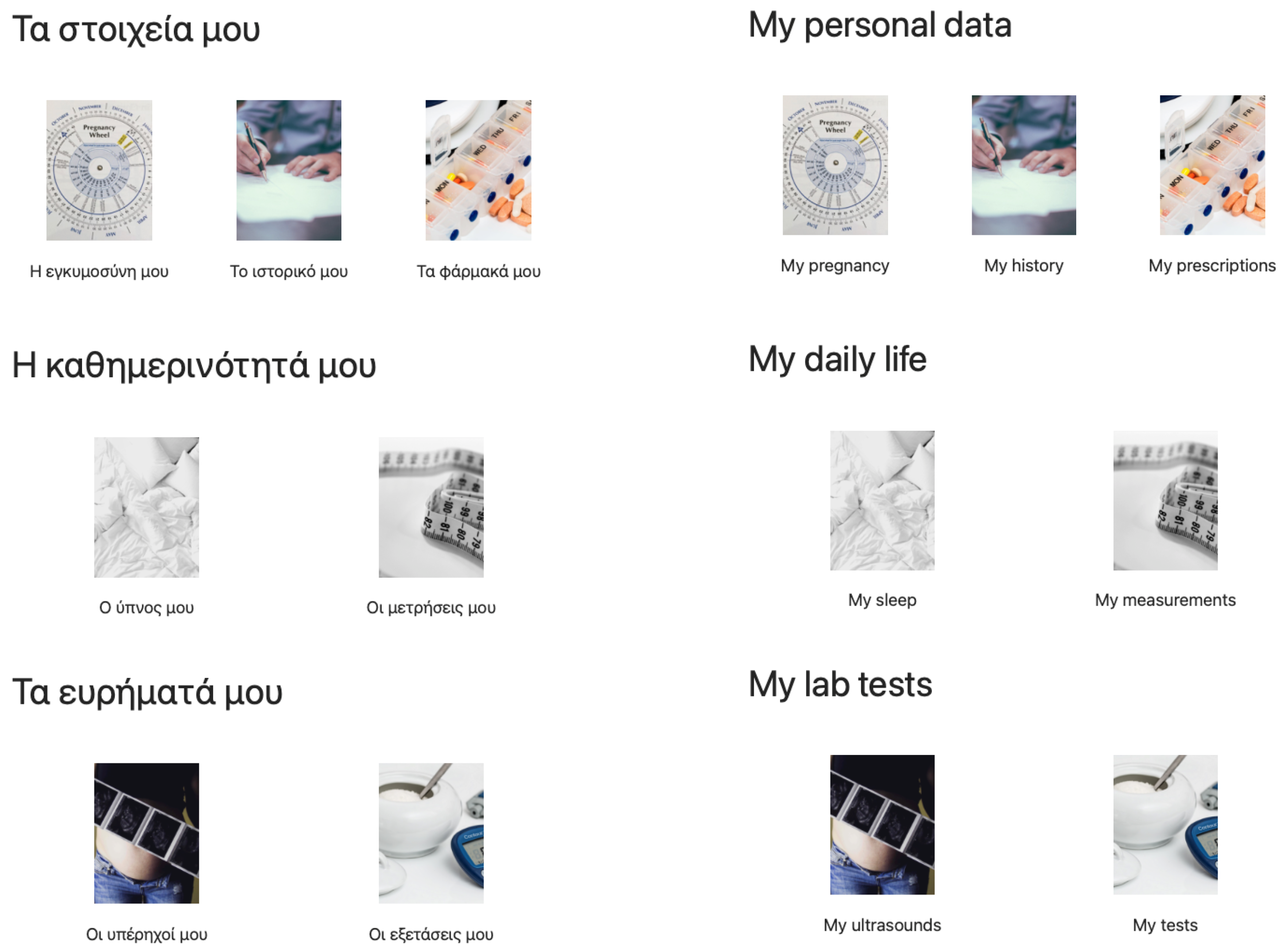
2.1. STORK Platform
2.2. Pilot Use of STORK
2.3. Historical Control Group
2.4. Variables
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Descriptive Data
3.3. Main Results
4. Discussion
4.1. Key Results
4.2. Limitations
4.3. Interpretation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ART | assisted reproduction techniques |
| BGC | blood glucose concentration |
| DIPS | data integrity, privacy and security |
| GDM | gestational diabetes mellitus |
| HGH | Hippokrateion General Hospital |
| IADPSG | International Association of Diabetes and Pregnancy Study Groups |
| OGTT | oral glucose tolerance test |
| SD | standard deviation |
| SMBG | self-monitoring blood glucose |
References
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational Diabetes Mellitus. Nat. Rev. Dis. Prim. 2019, 5, 47. [Google Scholar] [CrossRef]
- Coustan, D.R. Gestational Diabetes Mellitus. Clin. Chem. 2013, 59, 1310–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, T.A.; Xiang, A.H.; Page, K.A. Gestational Diabetes Mellitus: Risks and Management during and after Pregnancy. Nat. Rev. Endocrinol. 2012, 8, 639–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Q.; Aris, I.M.; Tan, K.H.; Li, L.J. Application and Utility of Continuous Glucose Monitoring in Pregnancy: A Systematic Review. Front. Endocrinol. 2019, 10, 697. [Google Scholar] [CrossRef] [PubMed]
- Bertini, A.; Gárate, B.; Pardo, F.; Pelicand, J.; Sobrevia, L.; Torres, R.; Chabert, S.; Salas, R. Impact of Remote Monitoring Technologies for Assisting Patients With Gestational Diabetes Mellitus: A Systematic Review. Front. Bioeng. Biotechnol. 2022, 10, 819697. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Dai, P.; Qin, Y.; Wu, M.; Yang, B.; Yu, X. Effectiveness of Telemedicine for Pregnant Women with Gestational Diabetes Mellitus: An Updated Meta-Analysis of 32 Randomized Controlled Trials with Trial Sequential Analysis. BMC Pregnancy Childbirth 2020, 20, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thouheed Ahmed, S.S.; Thanuja, K.; Guptha, N.S.; Narasimha, S. Telemedicine Approach for Remote Patient Monitoring System Using Smart Phones with an Economical Hardware Kit. In Proceedings of the 2016 International Conference on Computing Technologies and Intelligent Data Engineering (ICCTIDE’16), Kovilpatti, India, 7–9 January 2016; pp. 1–4. [Google Scholar] [CrossRef]
- O’Sullivan, J.B.; Gellis, S.S.; Dandrow, R.V.; Tenney, B.O. The Potential Diabetic and Her Treatment in Pregnancy. Obstet. Gynecol. 1966, 27, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Reece, E.; Coustan, D.R.; Hayslett, J.P.; Holford, T.; Coulehan, J.; O’Connor, T.Z.; Hobbins, J.C. Diabetic Nephropathy: Pregnancy Performance and Fetomaternal Outcome. Am. J. Obstet. Gynecol. 1988, 159, 56–66. [Google Scholar] [CrossRef]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guariguata, L.; Linnenkamp, U.; Beagley, J.; Whiting, D.; Cho, N. Global Estimates of the Prevalence of Hyperglycaemia in Pregnancy. Diabetes Res. Clin. Pract. 2014, 103, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zhao, Z.; Fu, D.; Gao, W.; Zhang, F. Maternal and Neonatal Outcomes after Energy-Restricted Diet for Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicine 2021, 100, e25279. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Dryden, D.M.; Guthrie, A.; Muise, M.; Vandermeer, B.; Donovan, L. Benefits and Harms of Treating Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis for the U.S. Preventive Services Task Force and the National Institutes of Health Office of Medical Applications of Research. Ann. Intern. Med. 2013, 159, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrison, A. Screening, Diagnosis, and Management of Gestational Diabetes Mellitus. Am. Fam. Physician 2015, 91, 460–467. [Google Scholar] [PubMed]
- Chatzakis, C.; Cavoretto, P.; Sotiriadis, A. Gestational Diabetes Mellitus Pharmacological Prevention and Treatment. Curr. Pharm. Des. 2021, 27, 3833–3840. [Google Scholar] [CrossRef]
- Myoga, M.; Tsuji, M.; Tanaka, R.; Shibata, E.; Askew, D.J.; Aiko, Y.; Senju, A.; Kawamoto, T.; Hachisuga, T.; Araki, S.; et al. Impact of Sleep Duration during Pregnancy on the Risk of Gestational Diabetes in the Japan Environmental and Children’s Study (JECS). BMC Pregnancy Childbirth 2019, 19, 483. [Google Scholar] [CrossRef] [PubMed]
- Adesina, N.; Dogan, H.; Green, S.; Tsofliou, F. Effectiveness and Usability of Digital Tools to Support Dietary Self-Management of Gestational Diabetes Mellitus: A Systematic Review. Nutrients 2022, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Miremberg, H.; Ben-Ari, T.; Betzer, T.; Raphaeli, H.; Gasnier, R.; Barda, G.; Bar, J.; Weiner, E. The Impact of a Daily Smartphone-Based Feedback System among Women with Gestational Diabetes on Compliance, Glycemic Control, Satisfaction, and Pregnancy Outcome: A Randomized Controlled Trial. Am. J. Obstet. Gynecol. 2018, 218, 453.e1–453.e7. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Tan, E.; Lum, E.; Sloot, P.; Boehm, B.O.; Car, J. A Smartphone App to Improve Medication Adherence in Patients with Type 2 Diabetes in Asia: Feasibility Randomized Controlled Trial. JMIR MHealth UHealth 2019, 7, e14914. [Google Scholar] [CrossRef]
- Bonoto, B.C.; de Araújo, V.E.; Godói, I.P.; de Lemos, L.L.P.; Godman, B.; Bennie, M.; Diniz, L.M.; Junior, A.A.G. Efficacy of Mobile Apps to Support the Care of Patients with Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR MHealth UHealth 2017, 5, e4. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Floros, D.; Papagianni, M.; Tsiroukidou, K.; Kosta, K.; Vamvakis, A.; Koletsos, N.; Hatziagorou, E.; Tsanakas, I.; Mastorakos, G. The Beneficial Effect of the Mobile Application Euglyca Child. Adolesc. Type 1 Diabetes Mellitus: A Randomized Control. Trial. Diabetes Technol. Ther. 2019, 21, 627–634. [Google Scholar] [CrossRef]
- DeNicola, N.; Grossman, D.; Marko, K.; Sonalkar, S.; Butler Tobah, Y.S.; Ganju, N.; Witkop, C.T.; Henderson, J.T.; Butler, J.L.; Lowery, C. Telehealth Interventions to Improve Obstetric and Gynecologic Health Outcomes: A Systematic Review. Obstet. Gynecol. 2020, 135, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Leblalta, B.; Kebaili, H.; Sim, R.; Lee, S.W.H. Digital Health Interventions for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. PLoS Digit. Health 2022, 1, e0000015. [Google Scholar] [CrossRef]
- Brørs, G.; Norman, C.D.; Norekvål, T.M. Accelerated Importance of eHealth Literacy in the COVID-19 Outbreak and Beyond. Eur. J. Cardiovasc. Nurs. 2020, 19, 458–461. [Google Scholar] [CrossRef]
- Alonso, S.G.; Marques, G.; Barrachina, I.; Garcia-Zapirain, B.; Arambarri, J.; Salvador, J.C.; de la Torre Díez, I. Telemedicine and E-Health Research Solutions in Literature for Combatting COVID-19: A Systematic Review. Health Technol. 2021, 11, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Arshad Ali, S.; Bin Arif, T.; Maab, H.; Baloch, M.; Manazir, S.; Jawed, F.; Ochani, R.K. Global Interest in Telehealth during COVID-19 Pandemic: An Analysis of Google Trends™. Cureus 2020, 12, e10487. [Google Scholar] [CrossRef] [PubMed]
- Fisk, M.; Livingstone, A.; Pit, S.W. Telehealth in the Context of COVID-19: Changing Perspectives in Australia, the United Kingdom, and the United States. J. Med. Internet Res. 2020, 22, e19264. [Google Scholar] [CrossRef]
- Bokolo, A.J. Application of Telemedicine and eHealth Technology for Clinical Services in Response to COVID-19 Pandemic. Health Technol. 2021, 11, 359–366. [Google Scholar] [CrossRef]
- Aziz, A.; Zork, N.; Aubey, J.J.; Baptiste, C.D.; D’Alton, M.E.; Emeruwa, U.N.; Fuchs, K.M.; Goffman, D.; Gyamfi-Bannerman, C.; Haythe, J.H.; et al. Telehealth for High-Risk Pregnancies in the Setting of the COVID-19 Pandemic. Am. J. Perinatol. 2020, 37, 800–808. [Google Scholar] [CrossRef]
- Stratton, P.; Gorodetsky, E.; Clayton, J. Pregnant in the United States in the COVID-19 Pandemic: A Collision of Crises We Cannot Ignore. J. Natl. Med. Assoc. 2021, 113, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Galle, A.; Semaan, A.; Huysmans, E.; Audet, C.; Asefa, A.; Delvaux, T.; Afolabi, B.B.; El Ayadi, A.M.; Benova, L. A Double-Edged Sword—Telemedicine for Maternal Care during COVID-19: Findings from a Global Mixed-Methods Study of Healthcare Providers. BMJ Glob. Health 2021, 6, e004575. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitton, C.; Dionne, F.; Masucci, L.; Wong, S.; Law, S. Innovations in Health Service Organization and Delivery in Northern Rural and Remote Regions: A Review of the Literature. Int. J. Circumpolar Health 2011, 70, 460–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajwani, A.; Qureshi, K.; Shaikh, T.; Sayani, S. eHealth for Remote Regions: Findings from Central Asia Health Systems Strengthening Project. Stud. Health Technol. Inform. 2015, 209, 128–134. [Google Scholar] [PubMed]
- Chang, T.; Li, H.; Zhang, N.; Jiang, X.; Yu, X.; Yang, Q.; Jin, Z.; Meng, H.; Chang, L. Highly Integrated Watch for Noninvasive Continual Glucose Monitoring. Microsyst. Nanoeng. 2022, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Ejdesjö, A.; Wentzel, P.; Eriksson, U.J. Influence of Maternal Metabolism and Parental Genetics on Fetal Maldevelopment in Diabetic Rat Pregnancy. Am. J. Physiol.-Endocrinol. Metab. 2012, 302, E1198–E1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Sundaram, R.; Maisog, J.; Calafat, A.M.; Barr, D.B.; Buck Louis, G.M. A Prospective Study of Prepregnancy Serum Concentrations of Perfluorochemicals and the Risk of Gestational Diabetes. Fertil. Steril. 2015, 103, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Tsai, M.Y.; Sun, Q.; Hinkle, S.N.; Rawal, S.; Mendola, P.; Ferrara, A.; Albert, P.S.; Zhang, C. A Prospective and Longitudinal Study of Plasma Phospholipid Saturated Fatty Acid Profile in Relation to Cardiometabolic Biomarkers and the Risk of Gestational Diabetes. Am. J. Clin. Nutr. 2018, 107, 1017–1026. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STORK Group | Control Group | |
|---|---|---|
| Mean (SD) | 31 in Total | 32 in Total |
| Maternal age (years) | 31.4 () | 32.1 () |
| Gestational age (weeks) | 28.1 () | 27.5 () |
| BMI before pregnancy | 25.4 () | 24.8 () |
| BMI at delivery | 30.7 () | 31.2 () |
| Weight gain (kg) | 14.5 () | 15.8 () |
| Total Number (Percentage) | ||
| Smoking | 3 (9.7%) | 5 (15.6%) |
| ART | 2 (6.5%) | 3 (9.4%) |
| Parity I | 16 (51.6%) | 14 (43.8%) |
| Parity II | 10 (32.2%) | 10 (31.2%) |
| Parity III | 3 (9.7%) | 5 (15.6%) |
| Parity IV | 2 (6.5%) | 3 (9.4%) |
| GDM in previous pregnancy | 5 (16.1%) | 6 (18.8%) |
| STORK Group | Control Group | |
|---|---|---|
| Non-Categorical Variables, Mean and Range (SD) | 31 in Total | 32 in Total |
| OGTT fasting value, mg/dL | 93.8 () | 91.7 () |
| OGTT 60-min value, mg/dL | 186.1 () | 178.0 () |
| OGTT 120-min value, mg/dL | 129.3 () | 142.1 () |
| Categorical Variables, Total Number and Percentage (%) | ||
| Insulin treatment | 5 (16.1%) | 5 (15.6%) |
| STORK Group | Control Group | |
|---|---|---|
| Non-Categorical Variables, Mean and Range (SD) | 31 in Total | 32 in Total |
| Gestational age at delivery, (weeks) | 38.5 () | 38.1 () |
| Birthweight (g) | 3298 () | 3167 () |
| Categorical Variables, Total Number and Percentage (%) | ||
| Antenatal corticosteroids | 0 | 0 |
| Caesarean delivery | 12 (38.7%) | 14 (43.8%) |
| COVID-19 positive | 0 | N/A |
| Episiotomy | 7 (22.6%) | 5 (15.6%) |
| Emergent cesarean delivery | 0 | 0 |
| Gestational hypertension | 0 | 1 (3.1%) |
| Hypoglycemia of newborn | 0 | 0 |
| Induction of labor | 0 | 0 |
| Instrumental delivery | 0 | 0 |
| Neonatal death | 0 | 0 |
| Neonatal macrosomia | 2 (6.5%) | 3 (9.4%) |
| NICU admission | 0 | 0 |
| Normal vaginal delivery | 0 | 0 |
| Phototherapy | 0 | 0 |
| Polyhydramnios | 1 (3.2%) | 1 (3.1%) |
| Preeclampsia | 0 | 0 |
| Respiratory morbidity | 0 | 0 |
| Shoulder dystocia | 0 | 0 |
| Third-/fourth-degree perineal tear | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatzakis, C.; Floros, D.; Liberis, A.; Gerede, A.; Dinas, K.; Pitsianis, N.; Sotiriadis, A. STORK: Collaborative Online Monitoring of Pregnancies Complicated with Gestational Diabetes Mellitus. Healthcare 2022, 10, 653. https://doi.org/10.3390/healthcare10040653
Chatzakis C, Floros D, Liberis A, Gerede A, Dinas K, Pitsianis N, Sotiriadis A. STORK: Collaborative Online Monitoring of Pregnancies Complicated with Gestational Diabetes Mellitus. Healthcare. 2022; 10(4):653. https://doi.org/10.3390/healthcare10040653
Chicago/Turabian StyleChatzakis, Christos, Dimitris Floros, Anastasios Liberis, Aggeliki Gerede, Konstantinos Dinas, Nikos Pitsianis, and Alexandros Sotiriadis. 2022. "STORK: Collaborative Online Monitoring of Pregnancies Complicated with Gestational Diabetes Mellitus" Healthcare 10, no. 4: 653. https://doi.org/10.3390/healthcare10040653