
Cardiorespiratory Fitness and Health-Related Quality of Life in Secondary School Children Aged 14 to 18 Years: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Statistics
3. Results
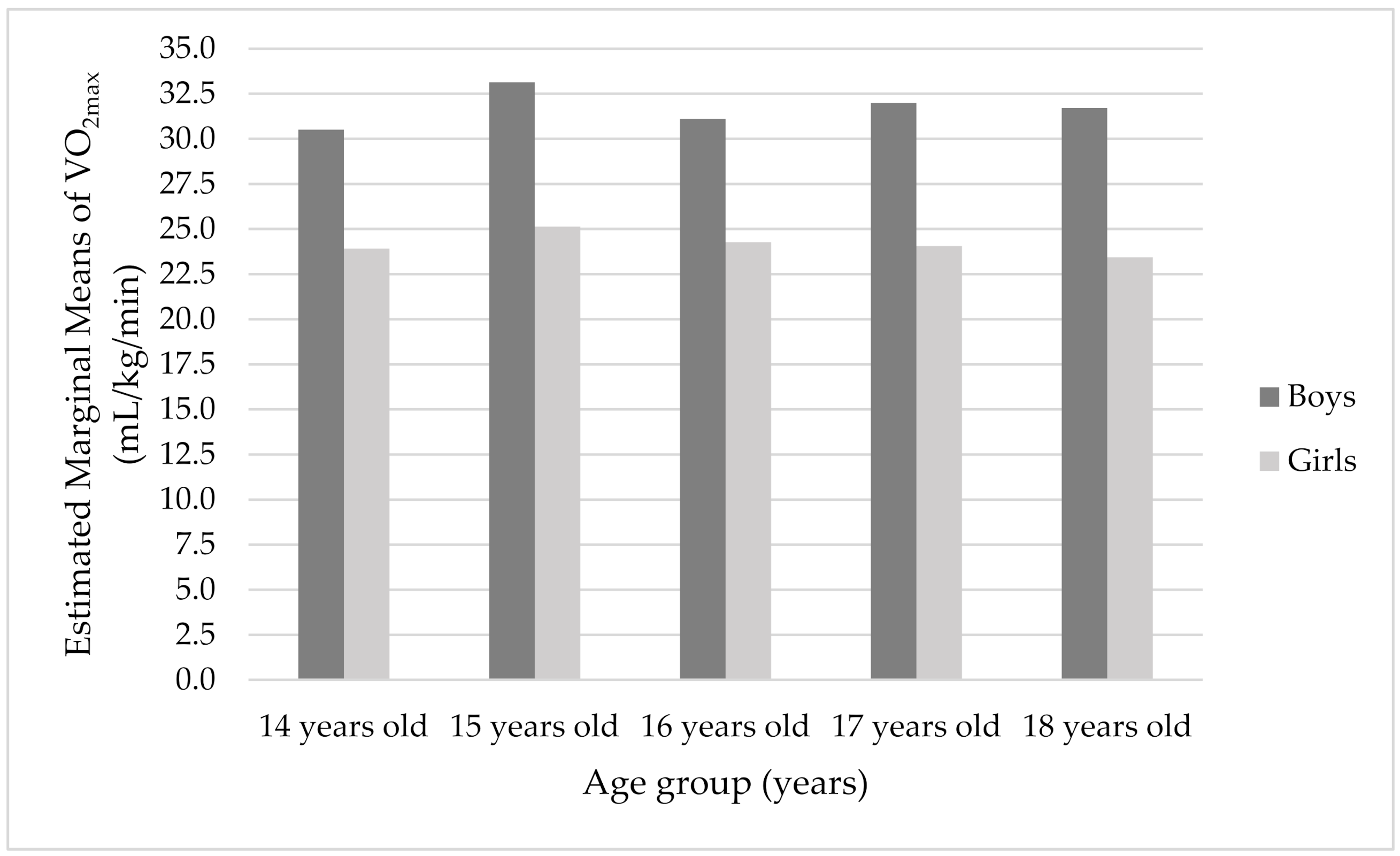
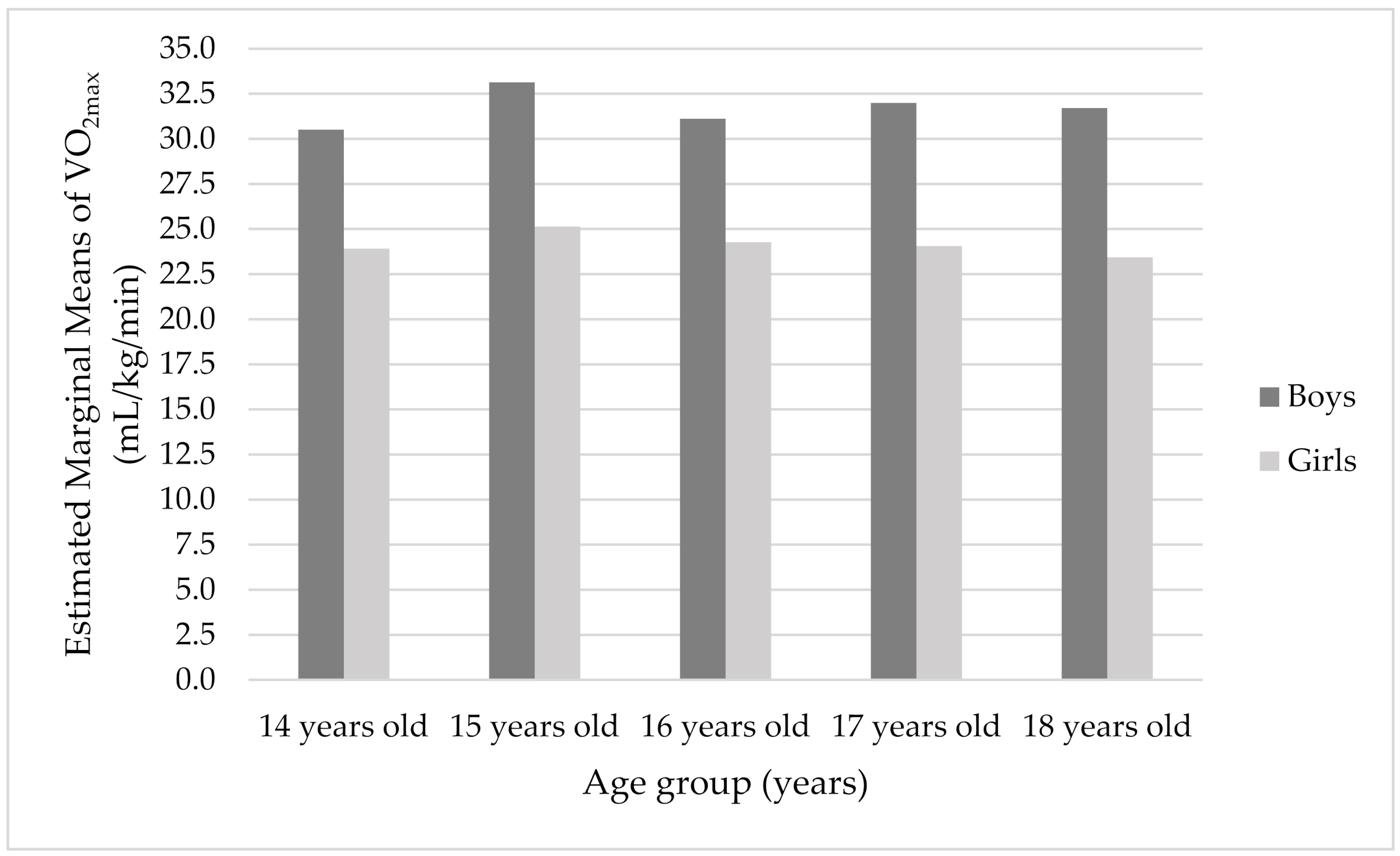
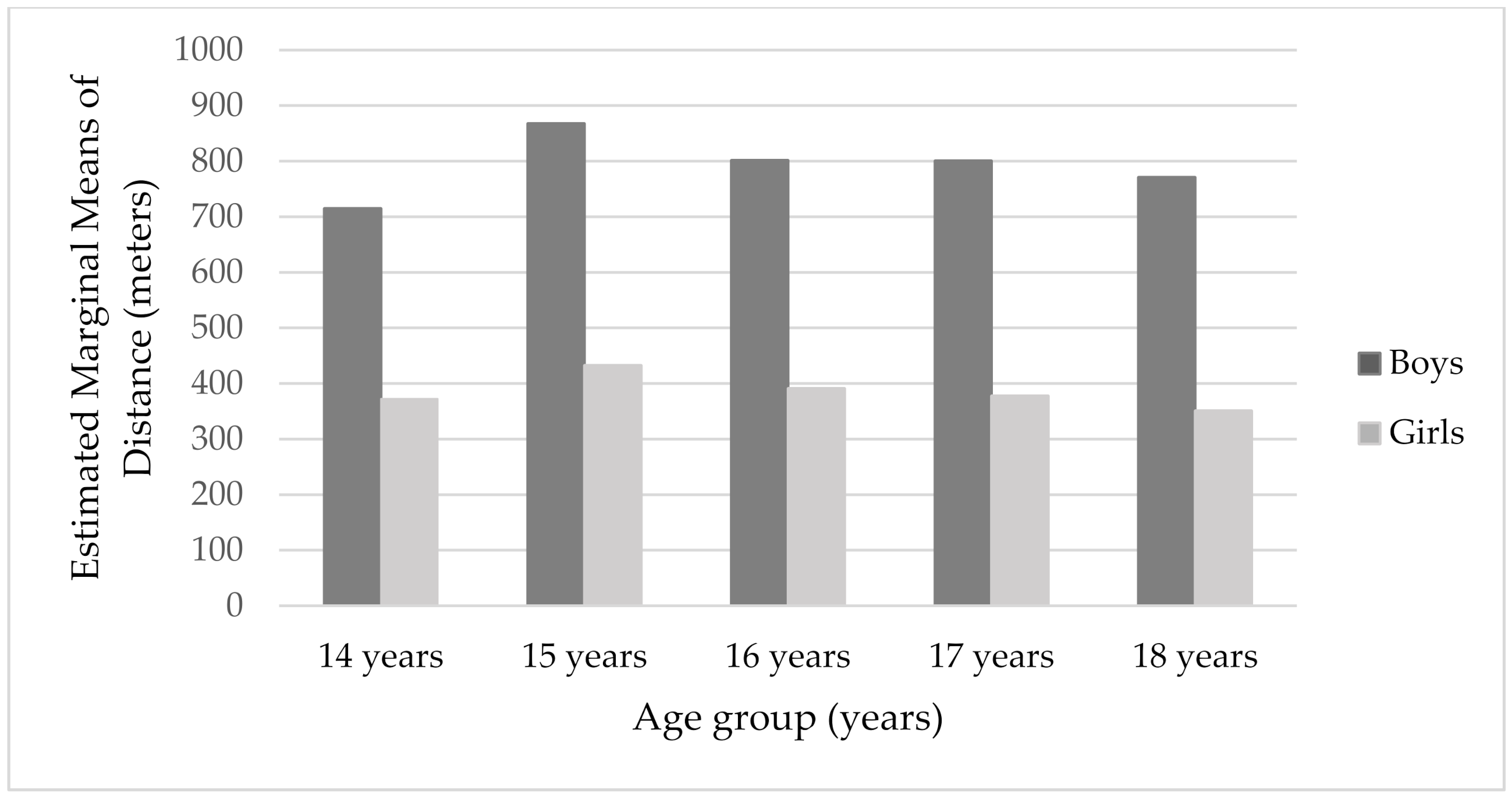
3.1. Gender Differences in CRF and Distance
3.2. Age Differences in CRF and Distance
3.3. Relations between CRF and HRQL in Adolescence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraser-Thomas, J.; Cote, J.; Deakin, J. Understanding dropout and prolonged engagement in adolescent competitive sport. Psychol. Sport Exerc. 2008, 9, 645–662. [Google Scholar] [CrossRef] [Green Version]
- Vella, S.A.; Schweickle, M.J.; Sutcliffe, J.T. Prevalence of dropout from organized extracurricular sports and associations with body fat percentage during childhood and adolescence. BMJ Open Sport Exerc. Med. 2020, 6, e000751. [Google Scholar] [CrossRef] [PubMed]
- Trbojević Jocić, J. Izazovi Omladinskog Sporta—Odustajanje od Bavljenja Sportom; Zadužbina Andrejević: Beograd, Serbia, 2021. [Google Scholar]
- Verloigne, M.; van Lippevelde, W.; Maes, L.; Yildirim, M.; Chinapaw, M.; Manios, Y. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 European countries using accelerometers: An observational study within the ENERGY-Project. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 34–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravens-Sieberer, U.; Herdman, M.; Devine, J.; Otto, C.; Bullinger, M.; Rose, M.; Klasen, F. The European KIDSCREEN approach to measure quality of life and well-being in children: Development, current application, and future advances. Qual. Life Res. 2014, 23, 791–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Božić, P.; Ostojić, S.M.; Berjan Bačvarević, B.; Radisavljević Janić, S.; Pažin, N.; Milanović, I.; Mirkov, D.; Čaprić, G. Vodič za Fizičku Aktivnost i Ishranu Mladih. Fizička Aktivnost i Ishrana Učenika Srednjih Škola; Zavod za Sport i Medicinu Republike Srbije: Beograd, Serbia, 2016.
- Castillo Garzón, M.J.; Ortega Porcel, F.B.; Ruiz Ruiz, J. Mejora de la forma física como terapia antienvejecimiento. Med. Clin. 2005, 124, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Eisenmann, J.C.; Laurson, K.R.; Welk, G.J. Aerobic fitness percentiles for U.S. adolescents. Am. J. Prev. Med. 2011, 41 (Suppl. 2), S106–S110. [Google Scholar] [CrossRef]
- Ekelund, U.; Poortvliet, E.; Nilsson, A.; Yngve, A.; Holmberg, A.; Sjöström, M. Physical activity in relation to aerobic fitness and body fat in 14- to 15-year-old boys and girls. Eur. J. Appl. Physiol. 2001, 85, 195–201. [Google Scholar] [CrossRef]
- Malina, R. Physical fitness of children and adolescents in the United States: Status and secular change. Med. Sport Sci. 2007, 50, 67–90. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise Capacity and Mortality among Men Referred for Exercise Testing. N. Engl. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Mendis, S.; Davis, S.; Norrving, B. Organizational update: The World Health Organization Global Status Report on Noncommunicable Diseases 2014; one more landmark step in the combat against stroke and vascular disease. Stroke 2015, 46, e121–e122. [Google Scholar] [CrossRef]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: Systematic review and meta-analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [Green Version]
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A. Childhood adiposity, adult adiposity, and cardiovascular risk factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar] [CrossRef] [Green Version]
- Laitinen, T.T.; Pahkala, K.; Venn, A.; Woo, J.G.; Oikonen, M.; Dwyer, T. Childhood lifestyle and clinical determinants of adult ideal cardiovascular health: The Cardiovascular Risk in Young Finns Study, the Childhood Determinants of Adult Health Study, the Princeton Follow-Up Study. Int. J. Cardiol. 2013, 169, 126–132. [Google Scholar] [CrossRef] [Green Version]
- Magnussen, C.G.; Smith, K.J.; Juonala, M. When to prevent cardiovascular disease? As early as possible: Lessons from prospective cohorts beginning in childhood. Curr. Opin. Cardiol. 2013, 28, 561–568. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L. European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts). Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Nielsen, G.A.; Andersen, L.B. The association between high blood pressure, physical fitness, and body mass index in adolescents. Prev. Med. 2003, 36, 229–234. [Google Scholar] [CrossRef]
- Theodore, R.F.; Broadbent, J.; Nagin, D.; Ambler, A.; Hogan, S.; Ramrakha, S. Childhood to early-midlife systolic blood pressure trajectories: Early-life predictors, effect modifiers, and adult cardiovascular outcomes. Hypertension 2015, 66, 1108–1115. [Google Scholar] [CrossRef] [Green Version]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women a meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Blair, S.N.; Kampert, J.B.; Kohl, H.W., III. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 1996, 276, 205–210. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Moreno, L.A.; González-Gross, M.; Wärnberg, J.; Gutiérrez, Á. Low Level of Physical Fitness in Spanish Adolescents. Relevance for Future Cardiovascular Health (AVENA Study). Rev. Española Cardiol. 2005, 58, 898–909. [Google Scholar] [CrossRef]
- Rowland, T. Evolution of maximal oxygen uptake in children. Med. Sport Sci. 2007, 50, 200–209. [Google Scholar] [CrossRef]
- Boreham, C.A.; Paliczka, V.J.; Nichols, A.K. A comparison of the PWC170 and 20-MST tests of aerobic fitness in adolescent schoolchildren. J. Sports Med. Phys. Fit. 1990, 30, 19–23. [Google Scholar]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 meter shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for adults: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.K.; Chi, L.; Etnier, J.L.; Wang, C.C.; Chu, C.H.; Zhou, C. Effect of acute aerobic exercise on cognitive performance: Role of cardiovascular fitness. Psychol. Sport Exerc. 2014, 15, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Jakšić, D.; Trbojević, J.; Majstorović, N. Fizička aktivnost kao facilitator kognitivnih sposobnosti kod dece. Tematski Zb. Rad. Međunarodnog Značaja 2017, 1, 111–125. [Google Scholar]
- Kirkcaldy, B.D.; Shephard, R.; Siefen, G. The relationship between physical activity and self-image and problem behavior among adolescents. Soc. Psychiatry Epidemiol. 2002, 37, 544–550. [Google Scholar] [CrossRef]
- Tubić, T.; Đorđić, V.; Poček, S. Dimenzije self-koncepta i bavljenje sportom u ranoj adolescenciji. Psihologija 2012, 45, 209–225. [Google Scholar]
- Gardner, L.A.; Magee, C.A.; Vella, S.A. Social climate profiles in adolescent sports: Associations with enjoyment and intention to continue. J. Adolesc. 2016, 52, 112–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabo, D.; Miller, K.E.; Melnick, M.J.; Farrell, M.P.; Barnes, G.M. High School Athletic Participation and Adolescent Suicide: A Nationwide US Study. Int. Rev. Sociol. Sport 2005, 40, 5–23. [Google Scholar] [CrossRef] [PubMed]
- Pires-Junior, R.; Coledam, D.H.C.; de Aguiar Greca, J.P.; de Arruda, G.A.; Teixeira, M.; de Oliveira, A.R. Physical fitness and health-related quality of life in Brazilian adolescents: A cross-sectional study. Hum. Mov. 2018, 19, 3–10. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Impaired health related quality of life in children and adolescents with chronic conditions: A comparative analysis of 10 disease clusters and 33 disease categories/severities utilizing the PedsQL™ 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 43. [Google Scholar] [CrossRef] [Green Version]
- Dumuid, D.; Olds, T.; Lewis, L.K.; Martin-Fernández, J.A.; Katzmarzyk, P.T.; Barreira, T. Health-Related Quality of Life and Lifestyle Behavior Clusters in School-Aged Children from 12 Countries. J. Pediatr. 2017, 183, 178–183. [Google Scholar] [CrossRef] [Green Version]
- Gu, X.; Chang, M.; Solmon, M.A. Physical activity, physical fitness, and health-related quality of life in school aged children. J. Teach. Phys. Educ. 2016, 35, 117–126. [Google Scholar] [CrossRef]
- Marques, A.; Mota, J.M.; Gaspar, T.; de Matos, M.G. Associations between self-reported fitness and self-rated health, life-satisfaction and health-related quality of life among adolescents. J. Exerc. Sci. Fit. 2017, 15, 8–11. [Google Scholar] [CrossRef]
- Belfer, M.L.; Saxena, S. WHO Child Atlas project. Lancet 2006, 367, 551–552. [Google Scholar] [CrossRef]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Ravens-Sieberer, U.; The KIDSCREEN Group Europe. The KIDSCREEN Questionnaires—Quality of Life Questionnaires for Children and Adolescents—Handbook; Pabst Science Publishers: Lengerich, Germany, 2006. [Google Scholar]
- Ravens-Sieberer, U.; Horka, H.; Illyes, A.; Rajmil, L.; Ottova-Jordan, V.; Erhart, M. Children’s Quality of Life in Europe: National Wealth and Familial Socioeconomic Position Explain Variations in Mental Health and Wellbeing—A Multilevel Analysis in 27 EU Countries. ISRN Public Health 2013, 2013, 419530. [Google Scholar] [CrossRef] [Green Version]
- Catley, M.J.; Tomkinson, G.R. Normative health-related fitness values for children: Analysis of 85347 test results on 9–17-year-old Australians since 1985. Br. J. Sports Med. 2013, 47, 98–108. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Parkinson, K.N.; Ravens-Sieberer, U.; Schirripa, G.; Thyen, U. Self-reported quality of life of 8–12-year-old children with cerebral palsy: A cross-sectional European study Already Registered? Please Login Already a Print Subscriber? Have a Free Trial Code? Lancet 2013, 369, 11–12. [Google Scholar] [CrossRef]
- Riiser, K.; Helseth, S.; Christophersen, K.A.; Haraldstad, K. Confirmatory factor analysis of the proxy version of Kidscreen-27 and relationships between health-related quality of life dimensions and body mass index and physical activity in young schoolchildren. Prev. Med. Rep. 2020, 20, 101210. [Google Scholar] [CrossRef]
- Armstrong, N.; Welsman, J.R. Assessment and interpretation of aerobic fitness in children and adolescents. Exerc. Sport Sci. Rev. 1994, 22, 435–476. [Google Scholar] [CrossRef]
- Romppanen, E.; Korhonen, M.; Salmelin, R.K.; Puura, K.; Luoma, I. The significance of adolescent social competence for mental health in young adulthood. Ment. Health Prev. 2021, 21, 200198. [Google Scholar] [CrossRef]
- Lyu, M.; Gill, D.L. Perceived physical competence and body image as predictors of perceived peer acceptance in adolescents. Asian J. Soc. Psychol. 2012, 15, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Bisegger, C.; Cloetta, B.; von Rueden, U.; Abel, T.; Ravens-Sieberer, U. Health-related quality of life: Gender differences in childhood and adolescence. Eur. Kidscreen Group Soz. Praventivmed. 2005, 50, 281–291. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Age | Boys (n = 285) | Girls (n = 294) |
|---|---|---|
| 14 (n = 67) | 33 | 34 |
| 15 (n = 136) | 72 | 64 |
| 16 (n = 135) | 57 | 78 |
| 17 (n = 139) | 67 | 72 |
| 18 (n = 102) | 56 | 46 |
| Height (cm) | 179.57 (7.38) | 166.29 (6.69) |
| Body weight (kg) | 71.78 (12.05) | 60.79 (10.09) |
| BMI | 22.22 (3.32) | 21.96 (3.43) |
| Mean | Std. Deviation | t-Test (df) | p | ||
| VO2max | Boys | 32.26 | 7.93 | 15.13 (455) | 0.001 |
| Girls | 24.06 | 4.64 | |||
| distance | Boys | 814.46 | 417.41 | 15.59 (437) | 0.001 |
| Girls | 376.53 | 228.70 |
| Mean | Std. Deviation | F (df) | p | ||
|---|---|---|---|---|---|
| VO2max | 14 | 27.04 | 7.139 | 1.382 (7578) | 0.239 |
| 15 | 29.45 | 8.104 | |||
| 16 | 27.66 | 7.708 | |||
| 17 | 27.99 | 7.556 | |||
| 18 | 27.70 | 7.347 | |||
| Distance | 14 | 533.73 | 373.49 | ||
| 15 | 666.62 | 420.04 | 1.639 (7578) | 0.163 | |
| 16 | 568.30 | 409.30 | |||
| 17 | 588.06 | 389.54 | |||
| 18 | 568.04 | 385.70 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. VO2max | * | 0.509 ** | 0.092 * | 0.031 | 0.005 | 0.013 | 0.198 ** | 0.434 ** | 0.199 ** | −0.560 ** | −0.017 | −0.086 * |
| 2. physical wellbeing | * | 0.318 ** | 0.225 ** | 0.170 ** | 0.239 ** | 0.572 ** | 0.223 ** | 0.082 * | −0.270 ** | −0.142 ** | −0.070 | |
| 3. psychological wellbeing | * | 0.474 ** | 0.403 ** | 0.422 ** | 0.792 ** | 0.031 | −0.027 | −0.061 | −0.084 * | −0.062 | ||
| 4. autonomy and parents | * | 0.409 ** | 0.438 ** | 0.748 ** | 0.052 | −0.016 | −0.082 * | −0.125 ** | −0.059 | |||
| 5. peers and social support | * | 0.234 ** | 0.577 ** | −0.002 | −0.012 | 0.010 | 0.029 | −0.004 | ||||
| 6. school environment | * | 0.654 ** | −0.072 | −0.117 ** | 0.050 | −0.192 ** | −0.098 * | |||||
| 7. HRQL | * | 0.072 | −0.021 | −0.111 ** | −0.160 ** | −0.082 * | ||||||
| 8. Height | * | 0.630 ** | −0.723 ** | 0.129 ** | 0.051 | |||||||
| 9. Weight | * | −0.477 ** | 0.170 ** | 0.781 ** | ||||||||
| 10. Gender | * | −0.025 | −0.062 | |||||||||
| 11. Age + | * | 0.119 ** | ||||||||||
| 12. BMI | * |
| Unstandardized Coefficients | Standardized Coefficients Beta | t | Sig. | Correlations | Collinearity Statistics | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Zero-Order | Partial | Part | Tolerance | VIF | ||||
| (Constant) | 119.167 | 8.289 | 14.377 | 0.001 | ||||||
| vo2max a | 0.297 | 0.081 | 0.175 | 3.650 | 0.001 | 0.186 | 0.150 | 0.148 | 0.712 | 1.405 |
| gender b | −0.338 | 1.245 | −0.013 | −0.272 | 0.786 | −0.104 | −0.011 | −0.011 | 0.712 | 1.405 |
| age *c | −1.560 | 0.437 | −0.145 | −3.568 | 0.001 | −0.148 | −0.147 | −0.145 | 0.998 | 1.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marković, L.; Trbojević Jocić, J.; Horvatin, M.; Pekas, D.; Trajković, N. Cardiorespiratory Fitness and Health-Related Quality of Life in Secondary School Children Aged 14 to 18 Years: A Cross-Sectional Study. Healthcare 2022, 10, 660. https://doi.org/10.3390/healthcare10040660
Marković L, Trbojević Jocić J, Horvatin M, Pekas D, Trajković N. Cardiorespiratory Fitness and Health-Related Quality of Life in Secondary School Children Aged 14 to 18 Years: A Cross-Sectional Study. Healthcare. 2022; 10(4):660. https://doi.org/10.3390/healthcare10040660
Chicago/Turabian StyleMarković, Lidija, Jovana Trbojević Jocić, Maja Horvatin, Damir Pekas, and Nebojša Trajković. 2022. "Cardiorespiratory Fitness and Health-Related Quality of Life in Secondary School Children Aged 14 to 18 Years: A Cross-Sectional Study" Healthcare 10, no. 4: 660. https://doi.org/10.3390/healthcare10040660