
The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
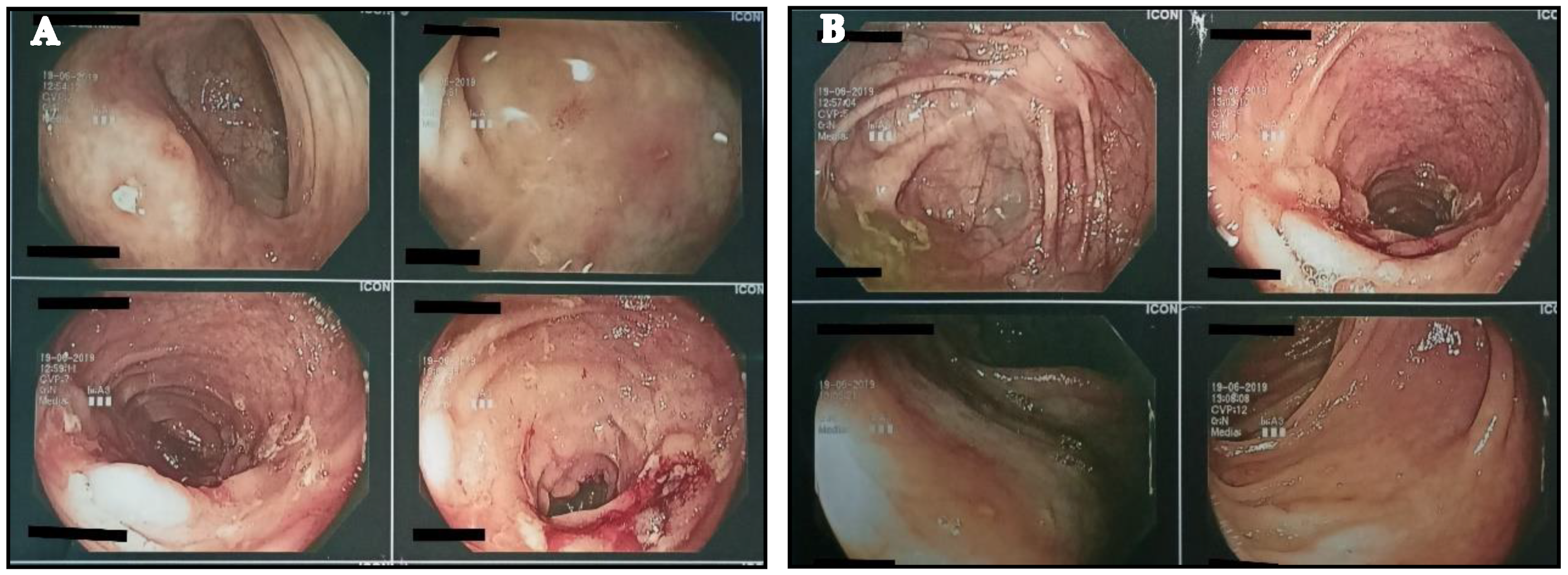
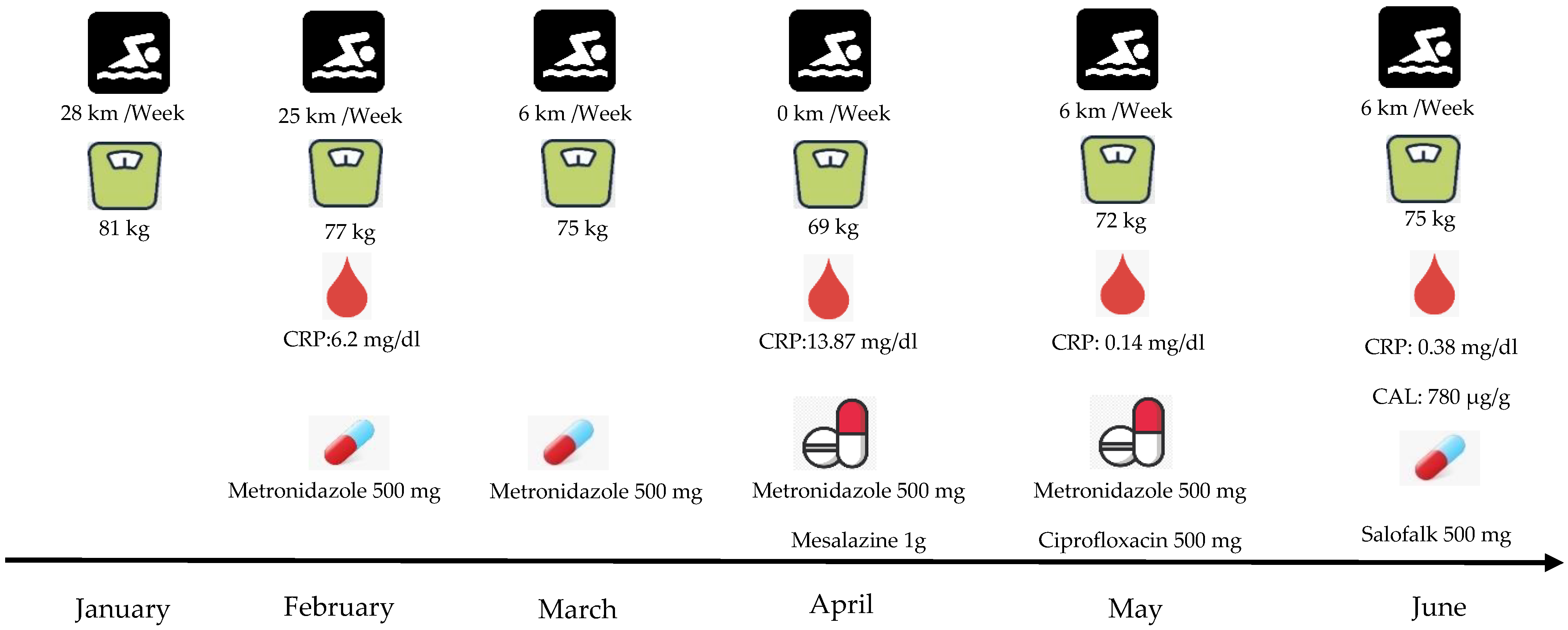
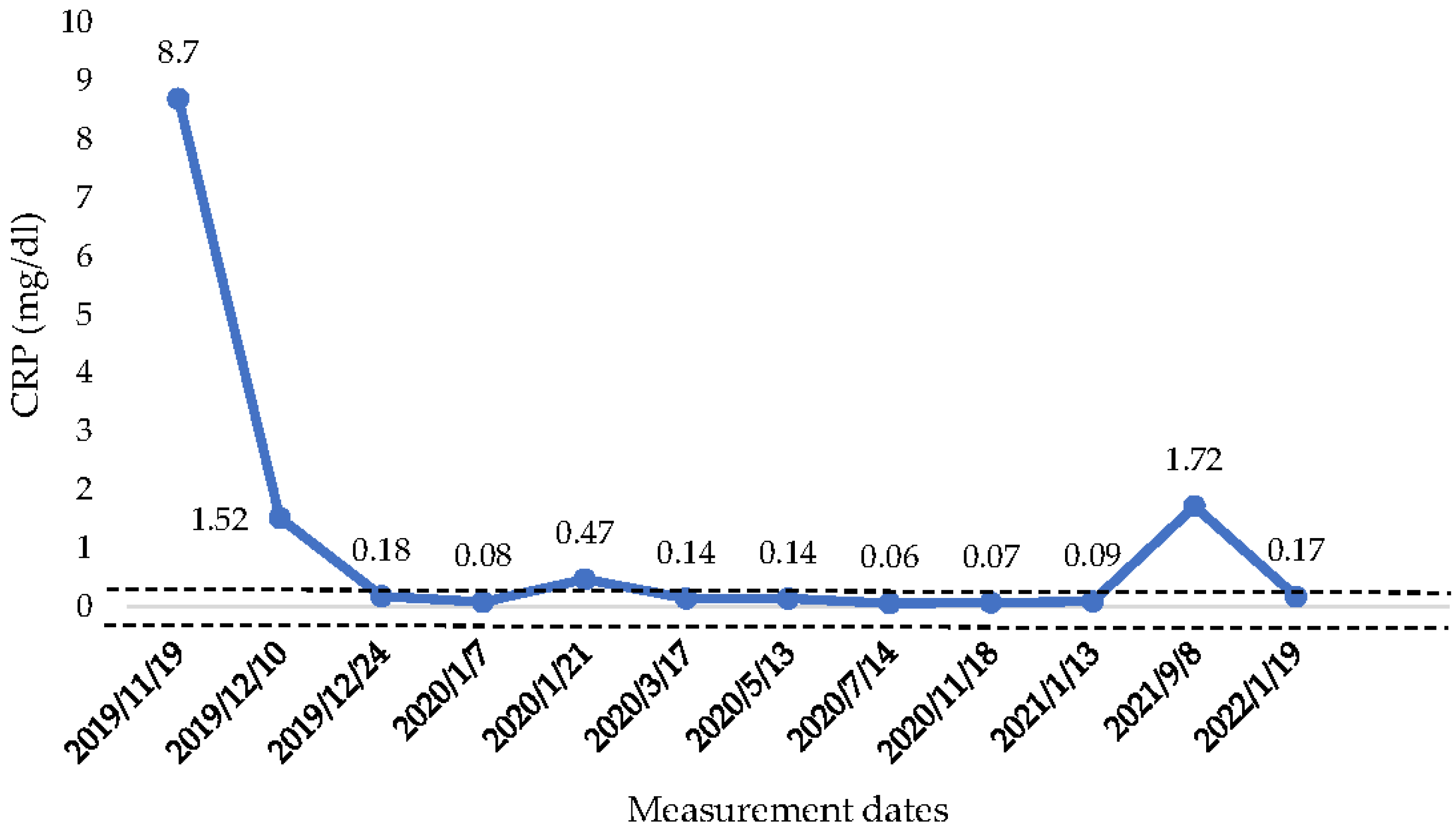
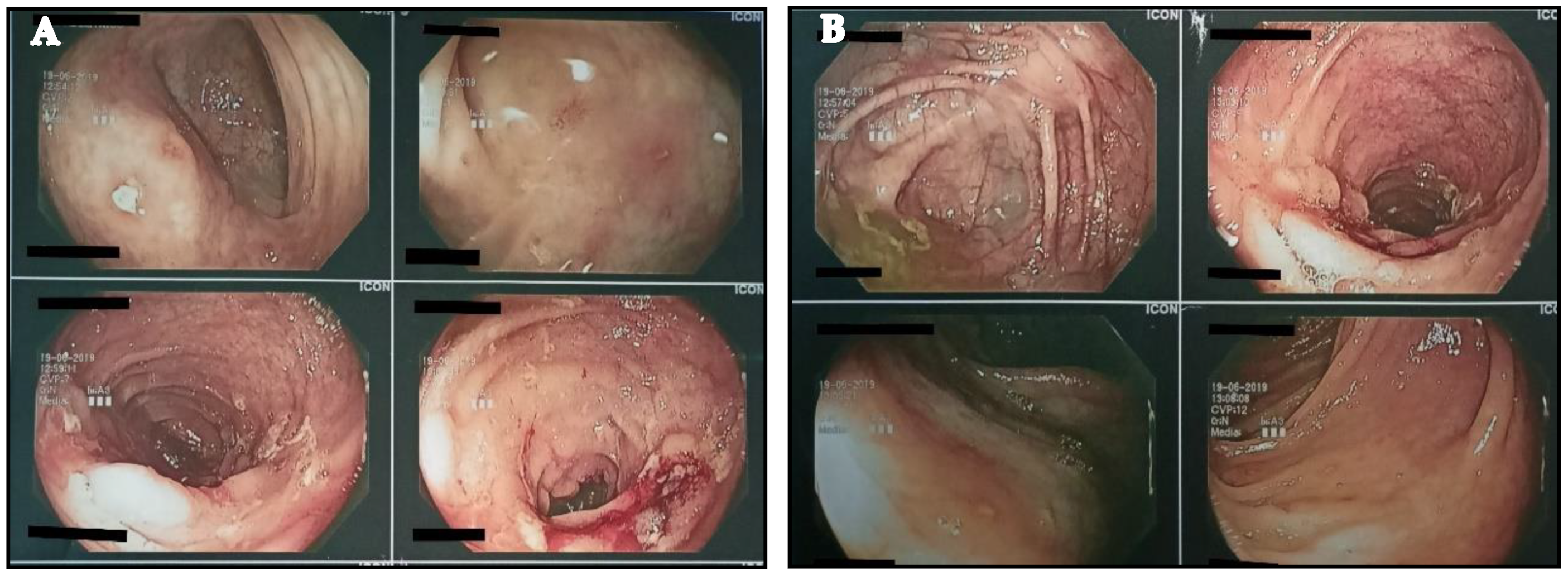
2. Case Report
3. Discussion
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aniwan, S.; Harmsen, W.S.; Tremaine, W.J.; Loftus, E.V., Jr. Incidence of inflammatory bowel disease by race and ethnicity in a population-based inception cohort from 1970 through 2010. Therap. Adv. Gastroenterol. 2019, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legeret, C.; Mählmann, L.; Gerber, M.; Kalak, N.; Köhler, H.; Holsboer-Trachsler, E.; Brand, S.; Furlano, R. Favorable impact of long-term exercise on disease symptoms in pediatric patients with inflammatory bowel disease. BMC Pediatr. 2019, 19, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilski, J.; Mazur-Bialy, A.I.; Brzozowski, B.; Magierowski, M.; Jasnos, K.; Krzysiek-Maczka, G.; Urbanczyk, K.; Ptak-Belowska, A.; Zwolinska-Wcislo, M.; Mach, T.; et al. Moderate exercise training attenuates the severity of experimental rodent colitis: The importance of crosstalk between adipose tissue and skeletal muscles. Mediat. Inflamm. 2015, 2015, 605071. [Google Scholar] [CrossRef] [PubMed]
- Elia, J.; Kane, S. Adult inflammatory bowel disease, physical rehabilitation, and structured exercise. Inflamm. Bowel. Dis. 2018, 24, 12. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou, K. Effect of resistance exercise training on Crohn’s disease patients. Intest. Res. 2021, 19, 275. [Google Scholar] [CrossRef] [PubMed]
- Wiroth, J.B.; Filippi, J.; Schneider, S.M.; Al-Jaouni, R.; Horvais, N.; Gavarry, O.; Bermon, S.; Hébuterne, X. Muscle performance in patients with Crohn’s disease in clinical remission. Inflamm. Bowel. Dis. 2005, 11, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Cabalzar, A.L.; Oliveira, D.J.F.; Reboredo, M.M.; Lucca, F.A.; Chebli, J.M.F.; Malaguti, C. Muscle function and quality of life in the Crohn’s disease. Fisioter. Mov. Curitiba. 2017, 30, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Robinson, R.J.; Krzywicki, T.; Almond, L.; Al-Azzawi, F.; Abrams, K.; Iqbal, S.J.; Mayberry, J.F. Effect of a low-impact exercise program on bone mineral density in Crohn’s disease: A randomized controlled trial. Gastroenterology 1998, 115, 36–41. [Google Scholar] [CrossRef]
- Candow, D.; Rizzi, A.; Chillibeck, P.; Worobetz, L. Effect of resistance training on Crohn’s disease. Can. J. Appl. Physiol. 2002, 27, S7–S8. [Google Scholar]
- Pérez, C.A. Prescription of physical exercise in Crohn’s disease. J. Crohn’s Colitis 2009, 3, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Souza Tajiri, G.J.; de Castro, C.L.; Zaltman, C. Progressive resistance training improves muscle strength in women with inflammatory bowel disease and quadriceps weakness. J. Crohn’s Colitis 2014, 8, 1749–1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cronin, O.; Barton, W.; Moran, C.; Sheehan, D.; Whiston, R.; Nugent, H.; McCarthy, Y.; Molloy, C.B.; O’Sullivan, O.; Cotter, P.D.; et al. Moderate-intensity aerobic and resistance exercise is safe and favorably influences body composition in patients with quiescent inflammatory bowel disease: A randomized controlled cross-over trial. BMC Gastroenterol. 2019, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Potempa, L.A.; El Kebir, D.; Filep, J.G. C-reactive protein and inflammation: Conformational changes affect function. Biol. Chem. 2015, 396, 1181–1197. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Mak, W.Y.; Andersen, M.J.; Lei, D.; Pekow, J.R.; Cohen, R.D.; Pereira, B.; Rubin, D.T. Fecal calprotectin is highly effective to detect endoscopic ulcerations in Crohn’s disease regardless of disease location. BMC Gastroenterol. 2018, 154, 6. [Google Scholar] [CrossRef]
- Nehring, S.M.; Goyal, A.; Patel, B.C. C Reactive protein. In Stat Pearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441843/ (accessed on 1 January 2022).
- Peyrin-Biroulet, L.; Sandborn, W.J.; Panaccione, R.; Domènech, E.; Pouillon, L.; Siegmund, B.; Danese, S.; Ghosh, S. Tumour necrosis factor inhibitors in inflammatory bowel disease: The story continues. Therap. Adv. Gastroenterol. 2021, 14. [Google Scholar] [CrossRef] [PubMed]

 : Range of normal values 0–0.50 mg/dL.
: Range of normal values 0–0.50 mg/dL.
: Range of normal values 0–0.50 mg/dL.
: Range of normal values 0–0.50 mg/dL.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadimitriou, K. The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete. Healthcare 2022, 10, 713. https://doi.org/10.3390/healthcare10040713
Papadimitriou K. The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete. Healthcare. 2022; 10(4):713. https://doi.org/10.3390/healthcare10040713
Chicago/Turabian StylePapadimitriou, Konstantinos. 2022. "The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete" Healthcare 10, no. 4: 713. https://doi.org/10.3390/healthcare10040713
APA StylePapadimitriou, K. (2022). The Influence of Aerobic Type Exercise on Active Crohn’s Disease Patients: The Incidence of an Elite Athlete. Healthcare, 10(4), 713. https://doi.org/10.3390/healthcare10040713