
Modelling Granular Process Flow Information to Reduce Bottlenecks in the Emergency Department


Abstract
1. Introduction
1.1. Review of the Literature
1.2. Need for Granular Understanding of ED Process Flow

{kind=link}
{kind=link}
{kind=link}
| Capabilities | Classify complex system into processes | Process mapping and modelling | ||||||||
| Methodology | Show start and end of a process | Show sequential flow and steps in a process | Show sub-processes | Show decision questions & possible outcome | Show simultaneous processes | Show roles performing activities within a process | Show interactions between roles | Predictive system performance | ||
| SIPOC [87,88] | Yes | NA | ||||||||
| Data flow diagram [59,60,61] |  | Yes | Yes | No | No | No | No | No | ||
| Value Stream Mapping [23,64,65,66] | Yes | Yes | Yes | No | No | No | No | |||
| Flow chart [21,71,72,73] | Yes | Yes | Yes | Yes | No | No | No | |||
| Role Activity Diagram (proposed in the paper) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| Simulation approaches * | Process mapping provided through flow chart, textual description or activity list [89] | Yes | ||||||||
2. Materials and Methods
2.1. Data Collection
2.2. Analysis
3. Results
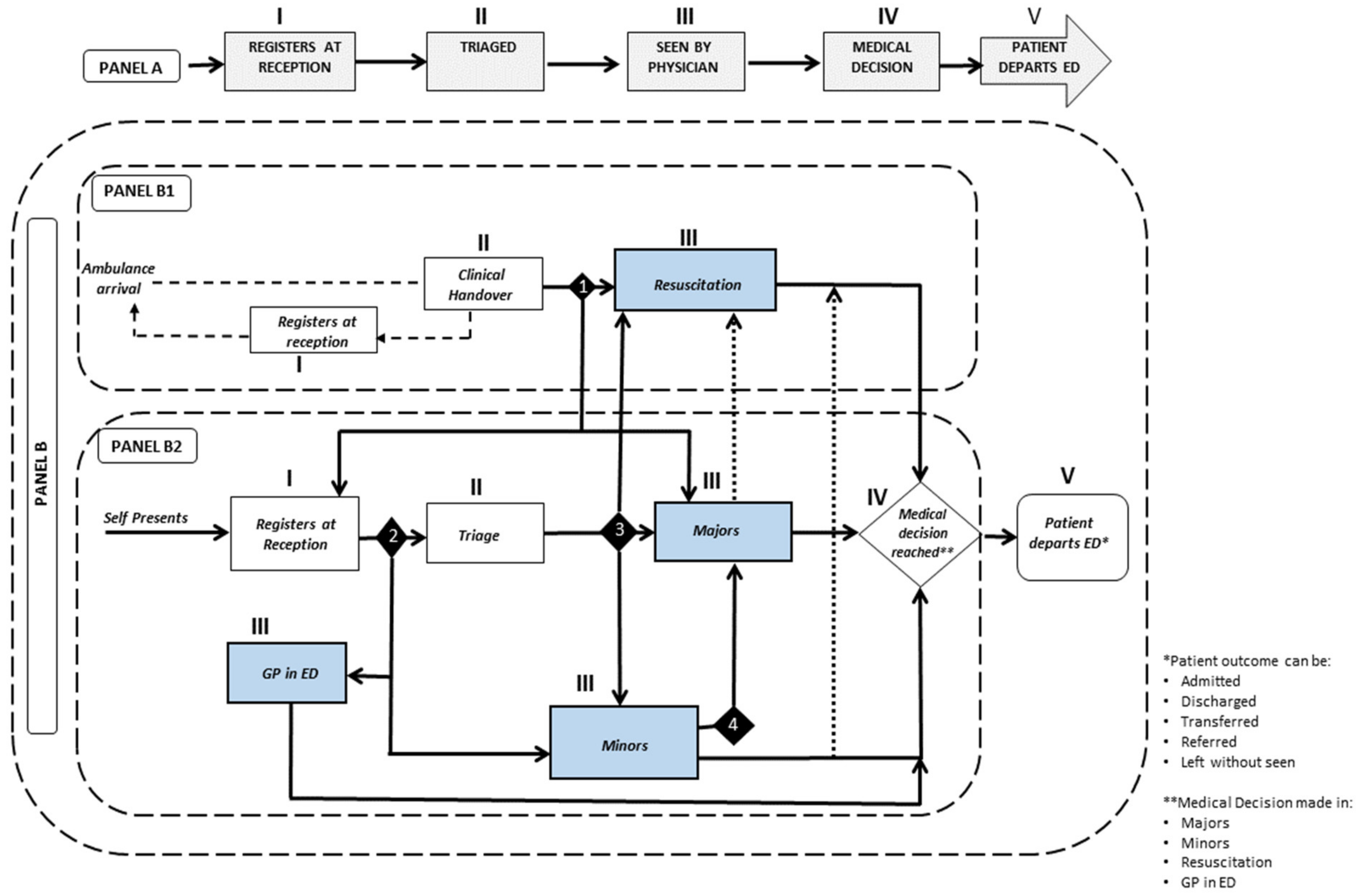
3.1. General Protocol Followed in the ED
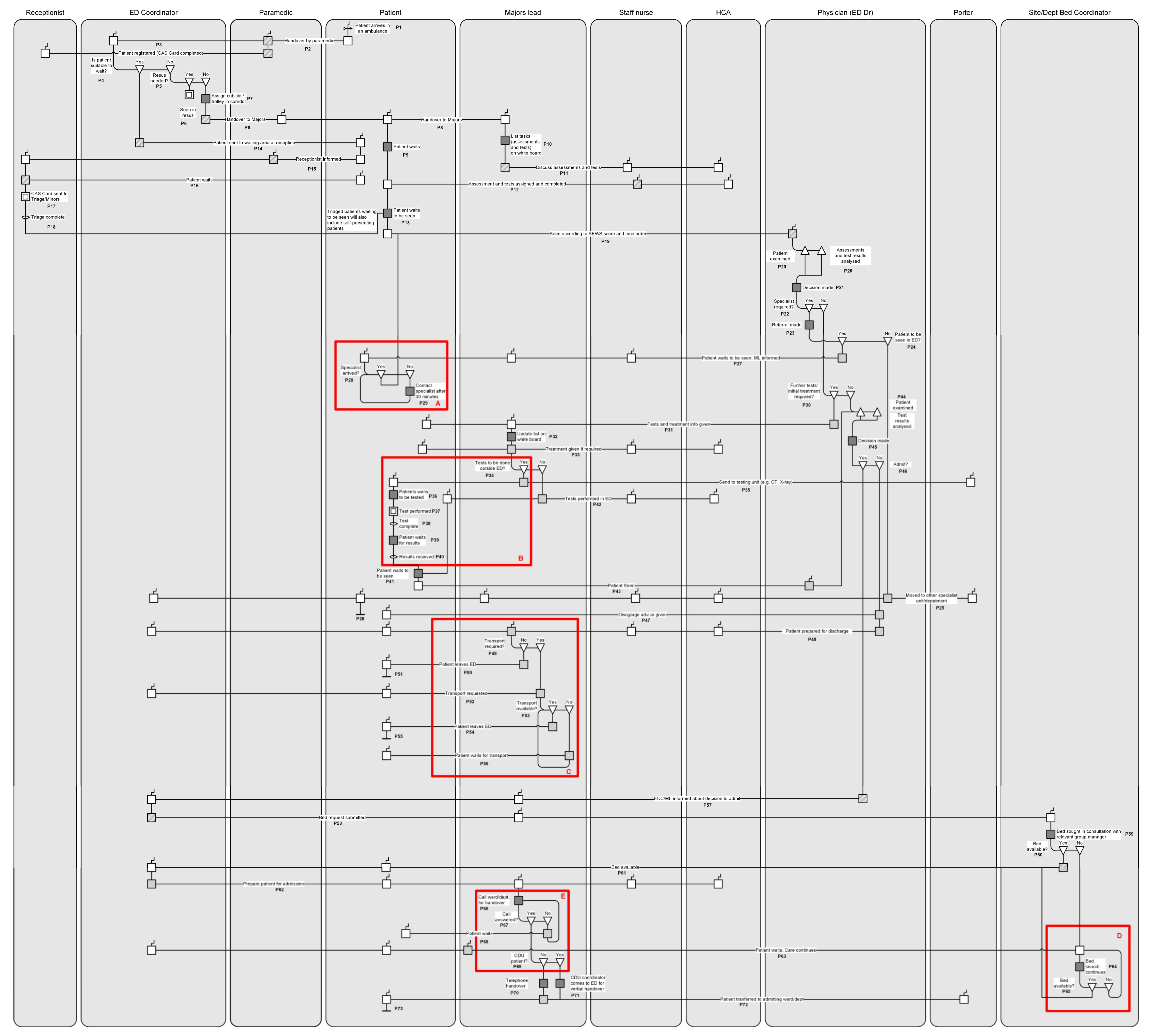
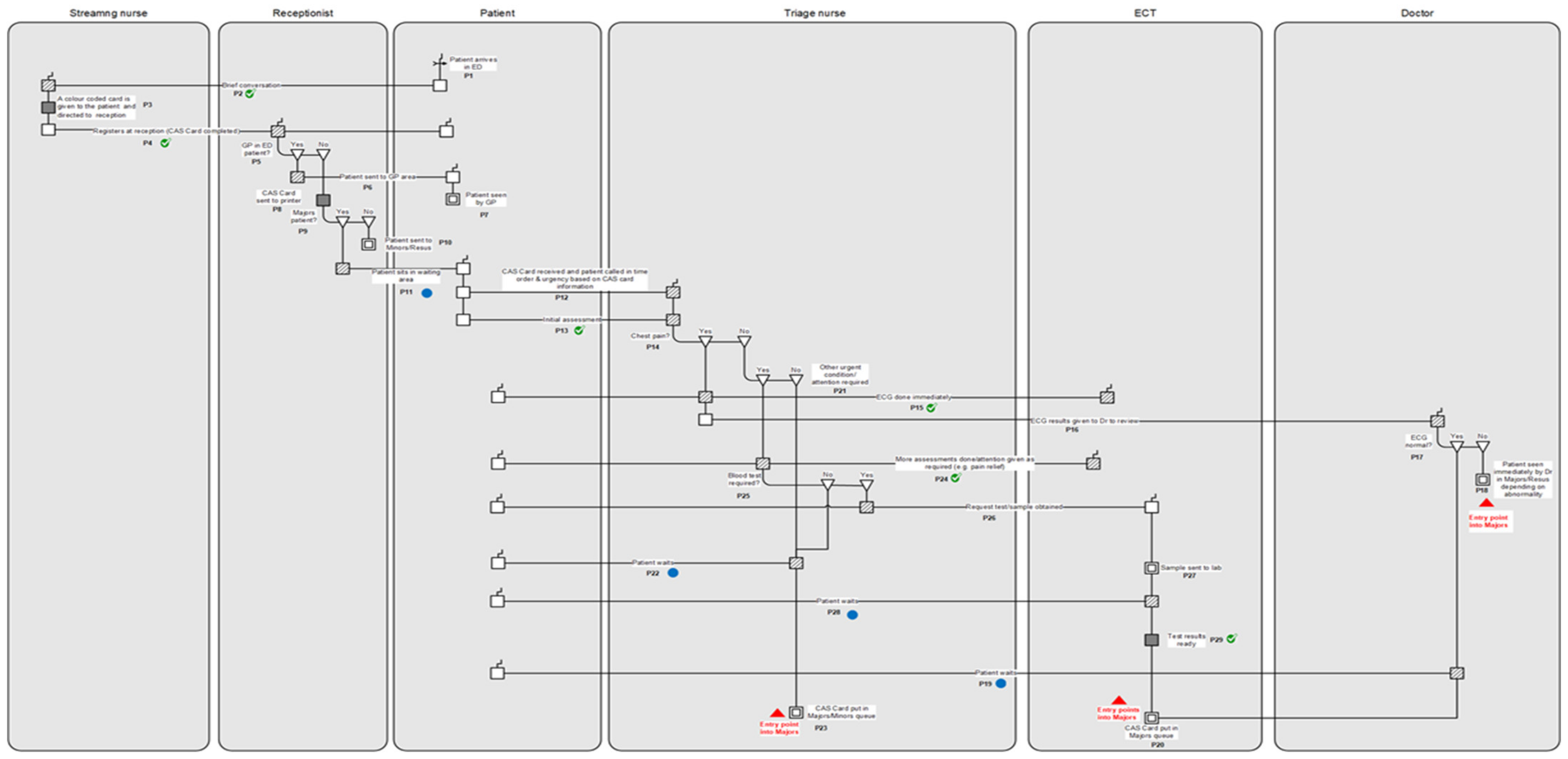
3.2. Granular Process Modelling of Care in the Majors Unit
3.3. Suggestions to Address the Identified Bottlenecks in Majors Derived from Process Mapping
3.3.1. Use of Precedence Information to Reduce Repeat Tests
3.3.2. Developing an Informed Alert System to Alleviate Waiting Time Pressure
3.3.3. Understanding Variation in the Context of Time-Based Quality Indicator in ED
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| No. | RAD Concept | General Description | Example (from Figure 2) | Graphical Notation |
|---|---|---|---|---|
| 1. | Role | A role performs a set of activities to achieve a particular goal. A role can be an individual, a group of people, or equipment. | ED coordinator, paramedic, and staff nurse. |  |
| 2. | Activity | A unit of work performed by a role is an activity. | List jobs on board, call ward/dept. |  |
| 3. | Interaction | Interaction represents a collaboration between roles to achieve the objective of the process. The role with the shaded box is the driver or the interaction, and the plain box is the receiver. There can be multiple drivers and receivers for an interaction. | Handover by a paramedic to ED coordinator, Major leads discuss tests and assessments with staff nurse and HCA. |  |
| 4. | Case Refinement | A case refinement represents a decision question and the possible outcomes. | Decision question: Bed available? Outcome: Yes or No. |  |
| 5. | Part refinement | The part refinement symbol represents activities done simultaneously by a role. | Patient examined, assessments and test results analysed simultaneously. |  |
| 6. | Trigger | A trigger represents an event that starts the activity thread. | A patient arrives in an ambulance. |  |
| 7. | Encapsulated process | An encapsulated process symbol represents a subprocess on the main diagram. The subprocess is then expanded on a separate diagram. | Tests outside ED. |  |
| 8. | Loop | A loop symbol is used to represents a part of the process that repeats itself | Is transport available? If ‘no’ then patient waits, and the question is repeated until the answer is ‘yes’. |  |
| 9. | Stop | The stop symbol marks the end of a process by ending a thread. | After the patient leaves the ED, the thread ends. |  |
| 10. | State | The state symbol is used to describe what is true before or after an action. | Test complete. |  |
References
- Campbell, P.; Boyle, A.; Higginson, I. Should we scrap the target of a maximum four hour wait in emergency departments? BMJ-Br. Med. J. 2017, 359, j4857. [Google Scholar] [CrossRef]
- Higginson, I.; Boyle, A.; Ahmad, S.; Macnamara, A.; Wilson, R.; Williamson, D. Tackling Emergency Department Crowding; The Royal College of Emergency Medicine: London, UK, 2015. [Google Scholar]
- Boyle, A.; Beniuk, K.; Higginson, I.; Atkinson, P. Emergency department crowding: Time for interventions and policy evaluations. Emerg. Med. Int. 2012, 2012, 838610. [Google Scholar] [CrossRef]
- Mason, S.; Weber, E.J.; Coster, J.; Freeman, J.; Locker, T. Time Patients Spend in the Emergency Department: England’s 4-Hour Rule—A Case of Hitting the Target but Missing the Point? Ann. Emerg. Med. 2012, 59, 341–349. [Google Scholar] [CrossRef]
- Letham, K.; Gray, A.; Edinburgh, E. The four-hour target in the NHS emergency departments: A critical comment. Emergencias 2012, 24, 69–72. [Google Scholar]
- Pines, J.M.; Hilton, J.A.; Weber, E.J.; Alkemade, A.J.; Al Shabanah, H.; Anderson, P.D.; Bernhard, M.; Bertini, A.; Gries, A.; Ferrandiz, S.; et al. International Perspectives on Emergency Department Crowding. Acad. Emerg. Med. 2011, 18, 1358–1370. [Google Scholar] [CrossRef]
- PHCC. Improving Access to Emergency Care: Addressing System Issues; Ontario Hospital Association: Torronto, ON, Canada, 2006. [Google Scholar]
- Schoen, C.; Osborn, R.; Huynh, P.T.; Doty, M.; Davis, K.; Zapert, K.; Peugh, J.; Peugh, J. Primary care and health system performance: Adults’ experiences in five countries. Health Aff. 2004, 23, W4487–W4503. [Google Scholar] [CrossRef]
- Elder, E.; Johnston, A.N.B.; Crilly, J. Improving emergency department throughput: An outcomes evaluation of two additional models of care. Int. Emerg. Nurs. 2016, 25, 19–26. [Google Scholar] [CrossRef]
- Zeinali, F.; Mahootchi, M.; Sepehri, M.M. Resource planning in the emergency departments: A simulation-based metamodeling approach. Simul. Model. Pract. Theory 2015, 53, 123–138. [Google Scholar] [CrossRef]
- Verelst, S.; Wouters, P.; Gillet, J.B.; Van den Berghe, G. Emergency department crowding in relation to in-hospital adverse medical events: A large prospective observational cohort study. J. Emerg. Med. 2015, 49, 949–961. [Google Scholar] [CrossRef]
- Sun, B.C.; Hsia, R.Y.; Weiss, R.E.; Zingmond, D.; Liang, L.-J.; Han, W.; McCreath, H.; Asch, S.M. Effect of Emergency Department Crowding on Outcomes of Admitted Patients. Ann. Emerg. Med. 2013, 61, 605–611. [Google Scholar] [CrossRef]
- Hoot, N.R.; LeBlanc, L.J.; Jones, I.; Levin, S.R.; Zhou, C.; Gadd, C.S.; Aronsky, D. Forecasting emergency department crowding: A discrete event simulation. Ann. Emerg. Med. 2008, 52, 116–125. [Google Scholar] [CrossRef]
- Duguay, C.; Chetouane, F. Modeling and improving emergency department systems using discrete event simulation. Simul.-Trans. Soc. Model. Simul. Int. 2007, 83, 311–320. [Google Scholar] [CrossRef]
- Schull, M.J.; Szalai, J.P.; Schwartz, B.; Redelmeier, D.A. Emergency department overcrowding following systematic hospital restructuring: Trends at twenty hospitals over ten years. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2001, 8, 1037–1043. [Google Scholar] [CrossRef]
- Uthman, O.A.; Walker, C.; Lahiri, S.; Jenkinson, D.; Adekanmbi, V.; Robertson, W.; Clarke, A. Genera practitioners providing non-urgent care in emergency department a natural experiment. Bmj Open 2018, 8, e019736. [Google Scholar] [CrossRef]
- Saghafian, S.; Austin, G.; Traub, S.J. Operations research/management contributions to emergency department patient flow optimization: Review and research prospects. IIE Trans. Health Syst. Eng. 2015, 5, 101–123. [Google Scholar] [CrossRef]
- Ortíz-Barrios, M.A.; Coba-Blanco, D.M.; Alfaro-Saíz, J.J.; Stand-González, D. Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8814. [Google Scholar] [CrossRef]
- Mallitt, K.A.; McNab, J.; Hughes, R.; Fernyhough, J.; Paterson, J.; O’Halloran, D. Reducing emergency department presentations among chronically ill patients in Western Sydney: A key role for coordinated primary care. Aust. J. Prim. Health 2017, 23, 140–146. [Google Scholar] [CrossRef]
- Hwang, U.; Shah, M.N.; Han, J.H.; Carpenter, C.R.; Siu, A.L.; Adams, J.G. Transforming Emergency Care For Older Adults. Health Aff. 2013, 32, 2116–2121. [Google Scholar] [CrossRef]
- Durand, A.-C.; Palazzolo, S.; Tanti-Hardouin, N.; Gerbeaux, P.; Sambuc, R.; Gentile, S. Nonurgent patients in emergency departments: Rational or irresponsible consumers? Perceptions of professionals and patients. BMC Res. Notes 2012, 5, 525. [Google Scholar] [CrossRef]
- Weber, E.J.; Mason, S.; Carter, A.; Hew, R.L. Emptying the Corridors of Shame: Organizational Lessons From England’s 4-Hour Emergency Throughput Target. Ann. Emerg. Med. 2011, 57, 79–88.e1. [Google Scholar] [CrossRef]
- Zhao, Y.C.; Peng, Q.J.; Strome, T.; Weldon, E.; Zhang, M.; Chochinov, A. Bottleneck detection for improvement of Emergency Department efficiency. Bus. Process Manag. J. 2015, 21, 564–585. [Google Scholar] [CrossRef]
- Zhao, X.; Bai, X. The Application of FMEA method in the risk management of medical device during the lifecycle. In Proceedings of the 2010 2nd International Conference on E-Business and Information System Security (Ebiss 2010), Wuhan, China, 22–13 May 2010; pp. 455–458. [Google Scholar]
- Swancutt, D.; Joel-Edgar, S.; Allen, M.; Thomas, D.; Brant, H.; Benger, J.; Byng, R.; Pinkney, J. Not all waits are equal: An exploratory investigation of emergency care patient pathways. BMC Health Serv. Res. 2017, 17, 436. [Google Scholar] [CrossRef]
- Martin, M.; Champion, R.; Kinsman, L.; Masman, K. Mapping patient flow in a regional Australian emergency department: A model driven approach. Int. Emerg. Nurs. 2011, 19, 75–85. [Google Scholar] [CrossRef]
- Finamore, S.R.; Turris, S.A. Shortening the wait: A strategy to reduce waiting times in the emergency department. J. Emerg. Nurs. 2009, 35, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Bowers, J.; Ghattas, M.; Mould, G. Success and failure in the simulation of an Accident and Emergency department. J. Simul. 2009, 3, 171–178. [Google Scholar] [CrossRef][Green Version]
- Asaro, P.V.; Lewis, L.M.; Boxerman, S.B. Emergency department overcrowding: Analysis of the factors of renege rate. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2007, 14, 157–162. [Google Scholar] [CrossRef]
- Asplin, B.R.; Magid, D.J.; Rhodes, K.V.; Solberg, L.I.; Lurie, N.; Camargo, C.A. A conceptual model of emergency department crowding. Ann. Emerg. Med. 2003, 42, 173–180. [Google Scholar] [CrossRef]
- Derlet, R.W.; Richards, J.R. Overcrowding in the nation’s emergency departments: Complex causes and disturbing effects. Ann. Emerg. Med. 2000, 35, 63–68. [Google Scholar] [CrossRef]
- Boyle, A.; Higginson, I.; Smith, S.; Henderson, K. Crowding in Emergency Departments; The Royal College of Emergency Medicine: London, UK, 2014. [Google Scholar]
- Oueida, S.; Kotb, Y.; Kadry, S.; Ionescu, S. Healthcare Operation Improvement Based on Simulation of Cooperative Resource Preservation Nets for None-Consumable Resources. Complexity 2018, 2018, 4102968. [Google Scholar] [CrossRef]
- Jarvis, P.R. Improving emergency department patient flow. Clin. Exp. Emerg. Med. 2016, 3, 63–68. [Google Scholar] [CrossRef]
- Ortiz-Barrios, M.A.; Alfaro-Saiz, J.J. Methodological Approaches to Support Process Improvement in Emergency Departments: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2664. [Google Scholar] [CrossRef] [PubMed]
- Higginson, I.; Boyle, A. What should we do about crowding in emergency departments? Br. J. Hosp. Med. 2018, 79, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Vanbrabant, L.; Braekers, K.; Ramaekers, K.; Van Nieuwenhuyse, I. Simulation of emergency department operations: A comprehensive review of KPIs and operational improvements. Comput. Ind. Eng. 2019, 131, 356–381. [Google Scholar] [CrossRef]
- Yarmohammadian, M.H.; Rezaei, F.; Haghshenas, A.; Tavakoli, N. Overcrowding in emergency departments: A review of strategies to decrease future challenges. J. Res.Med Sci. 2017, 22, 23. [Google Scholar] [CrossRef]
- DH. The NHS Plan: A plan for investment, a plan for reform. In Health Do; NHS: London, UK, 2000. [Google Scholar]
- Day, A.; Oldroyd, C. Attempting to reduce the maximum emergency waiting time to 4 h in England: Was the initiative successful? J. Emerg. Nurs. 2012, 38, 383–385. [Google Scholar] [CrossRef]
- ICF. Evidence Scan: The Impact of Performance Targets Within the NHS and Internationally; Atherton, H., Ed.; The Health Foundation: London, UK, 2015. [Google Scholar]
- DH. Clinical exceptions to the 4 h emergency care target. In Health Do; NHS: London, UK, 2003. [Google Scholar]
- Murray, R.; Jabbal, J.; Thompson, J.; Baird, B.; Maguire, D. The Kings Fund Quarterly Monitoring Report 2016/2017; 23rd Report; The King’s Fund: London, UK, 2017. [Google Scholar]
- Blunt, I.; Edwards, N.; Merry, L. What’s behind the A&E ”Crisis”? Policy Briefing #3; Nuffield Trust: London, UK, 2015. [Google Scholar]
- NHS Improvement. Part of Improving patient flow through urgent and emergency care. In Good Practice Guide: Focus on Improving Patient Flow; NHS Improvement: Leeds, UK, 2017. [Google Scholar]
- Smith, E.; Higginson, I.; Cleaver, B.; Smith, M.; Morris, A.M. Initial Assessment of Emergency Department Patients; Delivery, TRCoEMSDa; The Royal College of Emergency Medicine: London, UK, 2017. [Google Scholar]
- Goodacre, S.; Webster, A. Who waits longest in the emergency department and who leaves without being seen? Emerg. Med. J. 2005, 22, 93–96. [Google Scholar] [CrossRef]
- Khanna, S.; Boyle, J.; Good, N.; Bell, A.; Lind, J. Analysing the emergency department patient journey: Discovery of bottlenecks to emergency department patient flow. Emerg. Med. Australas. 2017, 29, 18–23. [Google Scholar] [CrossRef]
- Van der Veen, D.; Remeijer, C.; Fogteloo, A.J.; Heringhaus, C.; De Groot, B. Independent determinants of prolonged emergency department length of stay in a tertiary care centre: A prospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 81. [Google Scholar] [CrossRef]
- Brick, C.; Lowes, J.; Lovstrom, L.; Kokotilo, A.; Villa-Roel, C.; Lee, P.; Lang, E.; Rowe, B.H. The impact of consultation on length of stay in tertiary care emergency departments. Emerg. Med. J. 2014, 31, 134–138. [Google Scholar] [CrossRef]
- Paul, J.A.; Lin, L. Models For Improving Patient Throughput And Waiting At Hospital Emergency Departments. J. Emerg. Med. 2012, 43, 1119–1126. [Google Scholar] [CrossRef]
- Qureshi, N.U.; Ghawanni, A.O.; Bakhider, G.O.; AlDarrab, A. Consultation Impacts on Patients’ Length of Stay In the Emergency Department. Ann. Emerg. Med. 2010, 56, S110–S111. [Google Scholar] [CrossRef]
- Tomar, A.; Ganesh, S.S.; Richards, J.R. Transportation Preferences of Patients Discharged from the Emergency Department in the Era of Ridesharing Apps. West. J. Emerg. Med. 2019, 20, 672–680. [Google Scholar] [CrossRef]
- Smith, M.; Feied, C. The Emergency Department as a Complex System; The George Washington University: Washington, DC, USA, 1999. [Google Scholar]
- Clarkson, P.; Bogle, D.; Dean, J.; Tooley, M.; Trewby, J.; Vaughan, L.; Adams, E.; Dudgeon, P.; Platt, N.; Shelton, P. Engineering Better Care: A Systems Approach to Health and Care Design and Continuous Improvement; Royal Academy of Engineering: London, UK, 2017. [Google Scholar]
- Morley, C.; Unwin, M.; Peterson, G.M.; Stankovich, J.; Kinsman, L. Emergency department crowding: A systematic review of causes, consequences and solutions. PLoS ONE 2018, 13, e0203316. [Google Scholar] [CrossRef]
- Peng, Q.; Yang, J.; Strome, T.; Weldon, E.; Chochinov, A. Bottleneck Detection and Reduction Using Simulation Modeling to Reduce Overcrowding of Hospital Emergency Department. J. Model. Optim. 2020, 12, 100–109. [Google Scholar] [CrossRef]
- O’Neill, S.M.; Miake-Lye, I.; Childers, C.; Mak, S.; Beroes, J.M.; Maggard-Gibbons, M.; Shekelle, P.G. Effectiveness of interventions to improve the efficiency of emergency department operations: An evidence map. Am. J. Emerg. Med. 2018, 36, 2314–2317. [Google Scholar] [CrossRef] [PubMed]
- Souza, D.; Korzenowski, A.; Alvarado, M.; Sperafico, J.; Ackermann, A.; Mareth, T.; Scavarda, A. A Systematic Review on Lean Applications’ in Emergency Departments. Healthcare 2021, 9, 763. [Google Scholar] [CrossRef]
- Barrios, M.A.O.; Jimenez, H.F. Use of Six Sigma Methodology to Reduce Appointment Lead-Time in Obstetrics Outpatient Department. J. Med. Syst. 2016, 40, 220. [Google Scholar] [CrossRef]
- Kaushal, A.; Zhao, Y.; Peng, Q.; Strome, T.; Weldon, E.; Zhang, M.; Chochinov, A. Evaluation of fast track strategies using agent-based simulation modeling to reduce waiting time in a hospital emergency department. Socio-Econ. Plan. Sci. 2015, 50, 18–31. [Google Scholar] [CrossRef]
- Castanheira-Pinto, A.; Goncalves, B.S.; Lima, R.M.; Dinis-Carvalho, J. Modeling, Assessment and Design of an Emergency Department of a Public Hospital through Discrete-Event Simulation. Appl. Sci. 2021, 11, 805. [Google Scholar] [CrossRef]
- Mohiuddin, S.; Busby, J.; Savović, J.; Richards, A.; Northstone, K.; Hollingworth, W.; Donovan, J.L.; Vasilakis, C. Patient flow within UK emergency departments: A systematic review of the use of computer simulation modelling methods. BMJ Open 2017, 7, e015007. [Google Scholar] [CrossRef]
- Morgan, J., Howick, S., Belton, V., Eds.; Designs for the complementary use of System Dynamics and Discrete-Event Simulation. In Proceedings of the 2011 Winer Simulation Conference (WSC), Phoenix, AZ, USA, 11–14 December 2011. [Google Scholar]
- Karnon, J.; Stahl, J.; Brennan, A.; Caro, J.J.; Mar, J.; Möller, J. Modeling using Discrete Event Simulation: A Report of the ISPOR-SMDM Modeling Good Research Practices Task Force-4. Value Health 2012, 15, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Vanderby, S.; Carter, M.W. An evaluation of the applicability of system dynamics to patient flowmodelling. J. Oper. Res. Soc. 2010, 61, 1572–1581. [Google Scholar] [CrossRef]
- Zeinalnezhad, M.; Chofreh, A.G.; Goni, F.A.; Klemeš, J.J.; Sari, E. Simulation and Improvement of Patients’ Workflow in Heart Clinics during COVID-19 Pandemic Using Timed Coloured Petri Nets. Int. J. Environ. Res. Public Health 2020, 17, 8577. [Google Scholar] [CrossRef] [PubMed]
- Salimifard, K., Hosseini, S.Y., Moradi, M.S., Eds.; Improving Emergency Department Processes Using Coloured Petri Nets. In Proceedings of the PNSE+ ModPE Joint International Workshop on Petri Nets and Software Engineering (PNSE’13) and the International Workshop on Modeling and Business Environments (ModBE’13), Milan, Italy, 24–25 June 2013. [Google Scholar]
- Maier, J.F.; Eckert, C.M.; Clarkson, P.J. Model granularity in engineering design-concepts and framework. Des. Sci. 2017, 3, e1. [Google Scholar] [CrossRef]
- Eatock, J.; Clarke, M.; Picton, C.; Young, T. Meeting the four-hour deadline in an A&E department. J. Health Organ. Manag. 2011, 25, 606–624. [Google Scholar]
- Proudlove, N.C.; Black, S.; Fletcher, A. OR and the challenge to improve the NHS: Modelling for insight and improvement in in-patient flows. J. Oper. Res. Soc. 2007, 58, 145–158. [Google Scholar] [CrossRef]
- Jahangirian, M.; Naseer, A.; Stergioulas, L.; Young, T.; Eldabi, T.; Brailsford, S.; Patel, B.; Harper, P. Simulation in health-care: Lessons from other sectors. Oper. Res. 2012, 12, 45–55. [Google Scholar] [CrossRef]
- Katsaliaki, K.; Mustafee, N. Applications of simulation within the healthcare context. J. Oper. Res. Soc. 2011, 62, 1431–1451. [Google Scholar] [CrossRef]
- Eldabi, T., Ed.; Implementation issues of modeling healthcare problems: Misconceptions and lessons. In Proceedings of the Winter Simulation Conference 2009, Austin, TX, USA, 13–16 December 2009. [Google Scholar]
- Shukla, N.; Keast, J.; Ceglarek, D. Role activity diagram-based discrete event simulation model for healthcare service delivery processes. Int. J. Syst. Sci. Oper. Logist. 2015, 4, 68–83. [Google Scholar] [CrossRef][Green Version]
- Shukla, N.; Keast, J.E.; Ceglarek, D. Improved workflow modelling using role activity diagram-based modelling with application to a radiology service case study. Comput. Methods Programs Biomed. 2014, 116, 274–298. [Google Scholar] [CrossRef]
- Hunt, V.D. Process Mapping How to Re-Engineer Your Business Process; John Wiley & Sons: New York, NY, USA, 1996. [Google Scholar]
- Aguilar-Saven, R.S. Business process modelling: Review and framework. Int. J. Prod. Econ. 2004, 90, 129–149. [Google Scholar] [CrossRef]
- Crabbe, J.; Frank, C.; Nye, W. Improving report turnaround time: An integrated method using data from a radiology information system. AJR Am. J. Roentgenol. 1994, 163, 1503–1507. [Google Scholar] [CrossRef] [PubMed]
- Al-Balushi, S. The Value Stream Mapping in Hospital: The Case of Emergency Department. In Proceedings of the 29th International Business Information Management Association Conference-Education Excellence and Innovation Management through Vision 2020, Vienna, Austria, 3–4 May 2017; Volume I–VII, pp. 2844–2853. [Google Scholar]
- Gill, P.S. Application of value stream mapping to eliminate waste in an emergency room. Glob. J. Med. Res. 2012, 12, 51–56. [Google Scholar]
- Kaale, R.L.; Vega, D.D.; Messner, K.; Eitel, D.R.; Johnson, D.E.; McKniff, S. Time value stream mapping as a tool to measure patient flow through emergency department triage. Ann. Emerg. Med. 2005, 46, S108. [Google Scholar] [CrossRef]
- Ould, M.A. Business Process Management: A Rigorous Approach; BCS: Swindon, UK, 2007. [Google Scholar]
- Odeh, M.; Beeson, I.; Green, S.; Sa, J. Modelling Processes using RAD and UML Activity Diagrams: An Exploratory Study. In Proceedings of the Arab Conference on Information Technology (ACIT’2002) IACoIT, Doha, Qatar, 22–24 November 2002. [Google Scholar]
- Ould, M.A. An Introduction to Process Modelling Using RADs; IOPTCLUB Practical Process Modelling: London, UK, 1992. [Google Scholar]
- Zhao, W., Dai, W., Wang, A., Fang, X., Eds.; Role-Activity Diagrams Modeling Based on Workflow Mining. In Proceedings of the 2009 WRI World Congress on Computer Science and Information Engineering, Washington, DC, USA, 31 March–2 April 2009. [Google Scholar]
- NHS Digital. Hospital Accident and Emergency Activity, 2016–2017 Tables; NHS Digital: Leeds, UK, 2017. [Google Scholar]
- Ploeg, J. Identifying the best research design to fit the question. Part 2: Qualitative designs. Evid. Based Nurs. 1999, 2, 36–37. [Google Scholar] [CrossRef]
- Ross, A.J.; Murrells, T.; Kirby, T.; Jaye, P.; Anderson, J.E. An integrated statistical model of Emergency Department length of stay informed by Resilient Health Care principles. Saf. Sci. 2019, 120, 129–136. [Google Scholar] [CrossRef]
- Boddy, C.R. Sample size for qualitative research. Qual. Mark. Res. Int. J. 2016, 19, 426–432. [Google Scholar] [CrossRef]
- Saville, C.E.; Griffiths, P.; Ball, J.E.; Monks, T. How many nurses do we need? A review and discussion of operational research techniques applied to nurse staffing. Int. J. Nurs. Stud. 2019, 97, 7–13. [Google Scholar] [CrossRef]
- Shukla, N.; Lahiri, S.; Ceglarek, D. Pathway variation analysis (PVA): Modelling and simulations. Oper. Res. Health Care 2015, 6, 61–77. [Google Scholar] [CrossRef]
- Alexander, D.; Abbott, L.; Zhou, Q.P.; Staff, I. Can triage nurses accurately predict patient dispositions in the emergency department? J. Emerg. Nurs. 2016, 42, 513–518. [Google Scholar] [CrossRef]
- Xu, M.; Wong, T.C.; Wong, S.Y.; Chin, K.S.; Tsui, K.L.; Hsia, R.Y. Delays in Service for Non-Emergent Patients due to Arrival of Emergent Patients in the Emergency Department: A Case Study in Hong Kong. J. Emerg. Med. 2013, 45, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, P.; Joseph, D.; Bartlett, M.; Morris, A.; Mahajan, A.; McHugh, K.; Hillary, F.; O’Kelly, P. The ’who are all these people?’ study. Emerg. Med. J. 2015, 32, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, J.E.; Lee, J.A.; Lopiano, K.K.; McKinley, S.A.; Keesling, J.; Tyndall, J.A. A flexible simulation platform to quantify and manage emergency department crowding. BMC Med. Inform. Decis. Mak. 2014, 14, 50. [Google Scholar] [CrossRef] [PubMed]
- Gharahighehi, A.; Kheirkhah, A.S.; Bagheri, A.; Rashidi, E. Improving performances of the emergency department using discrete event simulation, DEA and the MADM methods. Digit. Health 2016, 2. [Google Scholar] [CrossRef]
- Moskop, J.C.; Geiderman, J.M.; Marshall, K.; McGreevy, J.; Derse, A.R.; Bookman, K.; McGrath, N.; Iserson, K.V. Another Look at the Persistent Moral Problem of Emergency Department Crowding. Ann. Emerg. Med. 2019, 74, 357–364. [Google Scholar] [CrossRef]
- Cho, S.J.; Jeong, J.; Han, S.; Yeom, S.; Park, S.W.; Kim, H.H.; Hwang, S.Y. Decreased Emergency Department Length of Stay by Application of a Computerized Consultation Management System. Acad. Emerg. Med. 2011, 18, 398–402. [Google Scholar] [CrossRef]
- Kim, M.J.; Park, J.M.; Je, S.M.; You, J.S.; Park, Y.S.; Chung, H.S.; Chung, S.P.; Lee, H.S. Effects of a short text message reminder system on emergency department length of stay. Int. J. Med. Inf. 2012, 81, 296–302. [Google Scholar] [CrossRef]
- Shin, S.; Lee, S.H.; Kim, D.H.; Kim, S.C.; Kim, T.Y.; Kang, C.; Jeong, J.H.; Lim, D.; Park, Y.J.; Lee, S.B. The impact of the improvement in internal medicine consultation process on ED length of stay. Am. J. Emerg. Med. 2018, 36, 620–624. [Google Scholar] [CrossRef]
- Chang, A.M.; Cohen, D.J.; Lin, A.; Augustine, J.; Handel, D.A.; Howell, E.; Kim, H.; Pines, J.M.; Schuur, J.D.; McConnell, K.J.; et al. Hospital Strategies for Reducing Emergency Department Crowding: A Mixed-Methods Study. Ann. Emerg. Med. 2018, 71, 497–505. [Google Scholar] [CrossRef]
- Woods, R.; Sandoval, R.; Vermillion, G.; Bates-Jackson, B.; Nwankwo, A.; Canamar, C.P.; Sarff, L. The Discharge Lounge A Patient Flow Process Solution. J. Nurs. Care Qual. 2020, 35, 240–244. [Google Scholar] [CrossRef]
- Franklin, B.J.; Vakili, S.; Huckman, R.S.; Hosein, S.; Falk, N.; Cheng, K.; Murray, M.; Harris, S.; Morris, C.A.; Goralnick, E. The Inpatient Discharge Lounge as a Potential Mechanism to Mitigate Emergency Department Boarding and Crowding. Ann. Emerg. Med. 2020, 75, 704–714. [Google Scholar] [CrossRef] [PubMed]
- Jenkin, A.; Abelson-Mitchell, N.; Cooper, S. Patient handover: Time for a change? Accid. Emerg. Nurs. 2007, 15, 141–147. [Google Scholar] [CrossRef]
- Altuwaijri, E.A.; Budgen, D.; Maxwell, S. Factors impeding the effective utilisation of an electronic patient report form during handover from an ambulance to an emergency department. Health Inform. J. 2019, 25, 1705–1721. [Google Scholar] [CrossRef] [PubMed]
- Snooks, H.; Wrigley, H.; George, S.; Thomas, E.; Smith, H.; Glasper, A. Appropriateness of use of emergency ambulances. J. Accid. Emerg. Med. 1998, 15, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Montán, K.L.; Riddez, L.; Lennquist, S.; Olsberg, A.C.; Lindberg, H.; Gryth, D.; Örtenwall, P. Assessment of hospital surge capacity using the MACSIM simulation system: A pilot study. Eur. J. Trauma Emerg. Surg. 2017, 43, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Goodacre, S.W.; Bradburn, M.; Cross, E.; Collinson, P.; Gray, A.; Hall, A.S.; RATPAC Research Team. The Randomised Assessment of Treatment using Panel Assay of Cardiac Markers (RATPAC) trial: A randomised controlled trial of point-of-care cardiac markers in the emergency department. Heart 2011, 97, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Harrison, G.; Speroni, K.G.; Dugan, L.; Daniel, M.G. A Comparison of the Quality of Blood Specimens Drawn in the Field by Ems Versus Specimens Obtained in the Emergency Department. J. Emerg. Nurs. 2010, 36, 16–20. [Google Scholar] [CrossRef]
- Goyder, C.; Tan, P.S.; Verbakel, J.; Ananthakumar, T.; Lee, J.J.; Hayward, G.; Turner, P.J.; Bruel, A.V.D. Impact of point-of-care panel tests in ambulatory care: A systematic review and meta-analysis. BMJ Open 2020, 10, e032132. [Google Scholar] [CrossRef]
- Delorenzo, A.; Meadley, B. Point-of-care ultrasound use in the pre-hospital setting. J. Paramed. Pract. 2018, 10, 326–332. [Google Scholar] [CrossRef]
- Roantree, R.; Furtado, C.; Welch, K.; Lambert, M.J. EMS Ultrasound Use; StatPearls Publishing: Treasure Island, FL, USA.
- Hand, P.J.; Kwan, J.; Lindley, R.I.; Dennis, M.S.; Wardlaw, J.M. Distinguishing between stroke and mimic at the bedside—The brain attack study. Stroke 2006, 37, 769–775. [Google Scholar] [CrossRef]
- Nor, A.M.; Davis, J.; Sen, B.; Shipsey, D.; Louw, S.J.; Dyker, A.G.; Davis, M.; Ford, G.A. The Recognition of Stroke in the Emergency Room (ROSIER) scale: Development and validation of a stroke recognition instrument. Lancet Neurol. 2005, 4, 727–734. [Google Scholar] [CrossRef]
- Greenfield, G.; Blair, M.; Aylin, P.P.; Saxena, S.; Majeed, A.; Hoffman, M.; Bottle, A. Frequent attendances at emergency departments in England. Emerg. Med. J. 2020, 37, 597. [Google Scholar] [CrossRef] [PubMed]
- Hilmer, S.N.; Perera, V.; Mitchell, S.; Murnion, B.P.; Dent, J.; Bajorek, B.; Matthews, S.; Rolfson, D.B. The assessment of frailty in older people in acute care. Australas. J. Ageing 2009, 28, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.C.; Cabrera, E.; Taboada, M.; Epelde, F.; Rexachs, D.; Luque, E. Quantitative Evaluation of Decision Effects in the Management of Emergency Department Problems. Procedia Comput. Sci. 2015, 51, 433–442. [Google Scholar] [CrossRef][Green Version]
- HEE. Advanced practice framework in Yorkshire and the Humber; England HEE: Leeds, UK, 2017. [Google Scholar]
- Gunal, M.M.; Pidd, M. Discrete event simulation for performance modelling in health care: A review of the literature. J. Simul. 2010, 4, 42–51. [Google Scholar] [CrossRef]
- Vanbrabant, L.; Martin, N.; Ramaekers, K.; Braekers, K. Quality of input data in emergency department simulations: Framework and assessment techniques. Simul. Model. Pract. Theory 2019, 91, 83–101. [Google Scholar] [CrossRef]
- Roberts, D.; Taylor, S.; Bodell, W.; Gostick, G.; Silkstone, J.; Smith, L.; Phippen, A.; Lyons, B.; Penny, D.; Norris, A.; et al. Development of a holistic admission assessment: An integrated care pathway for the hospice setting. Int. J. Palliat. Nurs. 2005, 11, 322–323. [Google Scholar] [CrossRef]
- Anjard, R.P. Process mapping: One of three, new, special quality tools for management, quality and all other professionals. Microelectron. Reliab. 1996, 36, 223–225. [Google Scholar] [CrossRef]
- McDonald, P.S.; Whittle, C.L.; Dunn, L.; De Luc, K. Shortfalls in Integrated Care Pathways. Part 1: What Don’t they Contain? J. Integr. Care Pathw. 2006, 10, 17–22. [Google Scholar]
- NHS Digital; S.C.A.T. Hospital Accident & Emergency Activity 2020–21; Gair RsD; NHS Digital: Leeds, UK, 2021. [Google Scholar]
- Chou, Y.C.; Yen, Y.F.; Chu, D.C.; Hu, H.Y. Impact of the COVID-19 Pandemic on Healthcare-Seeking Behaviors among Frequent Emergency Department Users: A Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 6351. [Google Scholar] [CrossRef] [PubMed]
- Ould, M.A.; Roberts, C. (Eds.) Modelling Iteration in the Software Process; ISPW: Calgary, AB, Canada, 1986. [Google Scholar]



| ED Unit | LoS < 4 h | LoS ≥ 4 h | Total n (%) | ||
|---|---|---|---|---|---|
| n (%) | Mean (SD) | n (%) | Mean (SD) | ||
| GP-in-ED | 4617(5.25%) | 129 (53) | 122 (0.53%) | 318 (78) | 4739 (4.28%) |
| Minors | 53,300 (60.84%) | 144 (57) | 4832(20.98%) | 342 (92) | 58,132 (52.54%) |
| Majors | 25,448 (29.05%) | 184 (51) | 14,551 (63.17%) | 433 (171) | 39,999 (36.15%) |
| Resuscitation | 4248 (4.85%) | 185 (53) | 3530 (15.32%) | 447 (160) | 7778 (7.03%) |
| Grand Total | 87,613 | 23,035 | 110,648 | ||
| Bottlenecks Identified | Improvement Suggestions to Alleviate the Bottleneck | Trade-Off | |
|---|---|---|---|
| Positive | Negative | ||
| Reallocate resources to bottleneck area | |||
| Clinicians from inpatient specialties can be freed up from elective and non-clinical activities to facilitate quicker responses to the ED. Automated reminders [99,100] can be sent to the specialties in addition to the ability for specialties to review results of investigations through electronic means, hence, only needing to visit the ED in person if a physical evaluation is required [101]. | Quicker patient processing in the ED, thus helping to meet waiting times. | Inpatients may be affected by having to wait longer to be seen by specialists. |
| Move tests upstream | |||
| Facilitate front loading tests [36]. Service level agreements can ensure faster turnarounds for tests by prioritising ED requests and POCT [2,102]. There are agreements at the site for a maximum 2-h turnaround for blood tests; this can be explored for other tests. | Quicker patient processing in ED, thus helping to meet waiting times. | Resources needed to meet service level agreements. Non-ED patients might have to wait longer for tests. |
| Create buffer zone | |||
| Use a discharge lounge to facilitate quicker discharges from the ED [103,104]. | Timely patient discharge from ED. Fewer problems with boarding | Increased use of the discharge lounge will require extra resources. |
| Evidence on inpatient boarding suggests that admitted patients awaiting a bed can wait in the inpatient ward [2,45,102]. | Can be initiated early in the patient stay. Reduce boarding. Free up staff time to see other patients. | Bed availability could be dependent on factors that are outside the control of the hospital. |
| Better data and information handling | |||
| Integrated electronic notes and handover reports can expedite processes [102], thus reducing the need for verbal handover. Better documentation of admission processes could reduce duplication [2]. | Patients will egress the ED on time. | The cost involved in implementing an integrated electronic system. |
| Variables of Interest | Patient Report Form 1 | Casualty Card 2 |
|---|---|---|
| Demography (age, gender) | x | x |
| Incident date and time | x | - |
| Date and time of arrival | x | x |
| Date of birth | x | x |
| Specialty | - | x |
| Source of referral | - | x |
| Number of previous attendances | - | x |
| GP detail | x | x |
| Patient transported with an alert | x | x |
| Risk of fall risks | - | x |
| Health history | x | x |
| Vital signs and observations | x | x |
| Pre-hospital blood test | x | - |
| Pre-hospital ultrasound | x | - |
| Cardiac health and ECG reading | x | - |
| Cerebrovascular events, such as suspected stroke | x | - |
| Any history of medication | x | x |
| Mental health among others | x | - |
| Presenting complaints | - | x |
| Signs of infection | - | x |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amissah, M.; Lahiri, S. Modelling Granular Process Flow Information to Reduce Bottlenecks in the Emergency Department. Healthcare 2022, 10, 942. https://doi.org/10.3390/healthcare10050942
Amissah M, Lahiri S. Modelling Granular Process Flow Information to Reduce Bottlenecks in the Emergency Department. Healthcare. 2022; 10(5):942. https://doi.org/10.3390/healthcare10050942
Chicago/Turabian StyleAmissah, Marian, and Sudakshina Lahiri. 2022. "Modelling Granular Process Flow Information to Reduce Bottlenecks in the Emergency Department" Healthcare 10, no. 5: 942. https://doi.org/10.3390/healthcare10050942
APA StyleAmissah, M., & Lahiri, S. (2022). Modelling Granular Process Flow Information to Reduce Bottlenecks in the Emergency Department. Healthcare, 10(5), 942. https://doi.org/10.3390/healthcare10050942