
Evidence of the Association between Nurse Staffing Levels and Patient and Nurses’ Outcomes in Acute Care Hospitals across Japan: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Study Selection
2.4. Assessment of the Risk of Bias
2.5. Data Extraction and Synthesis
3. Results
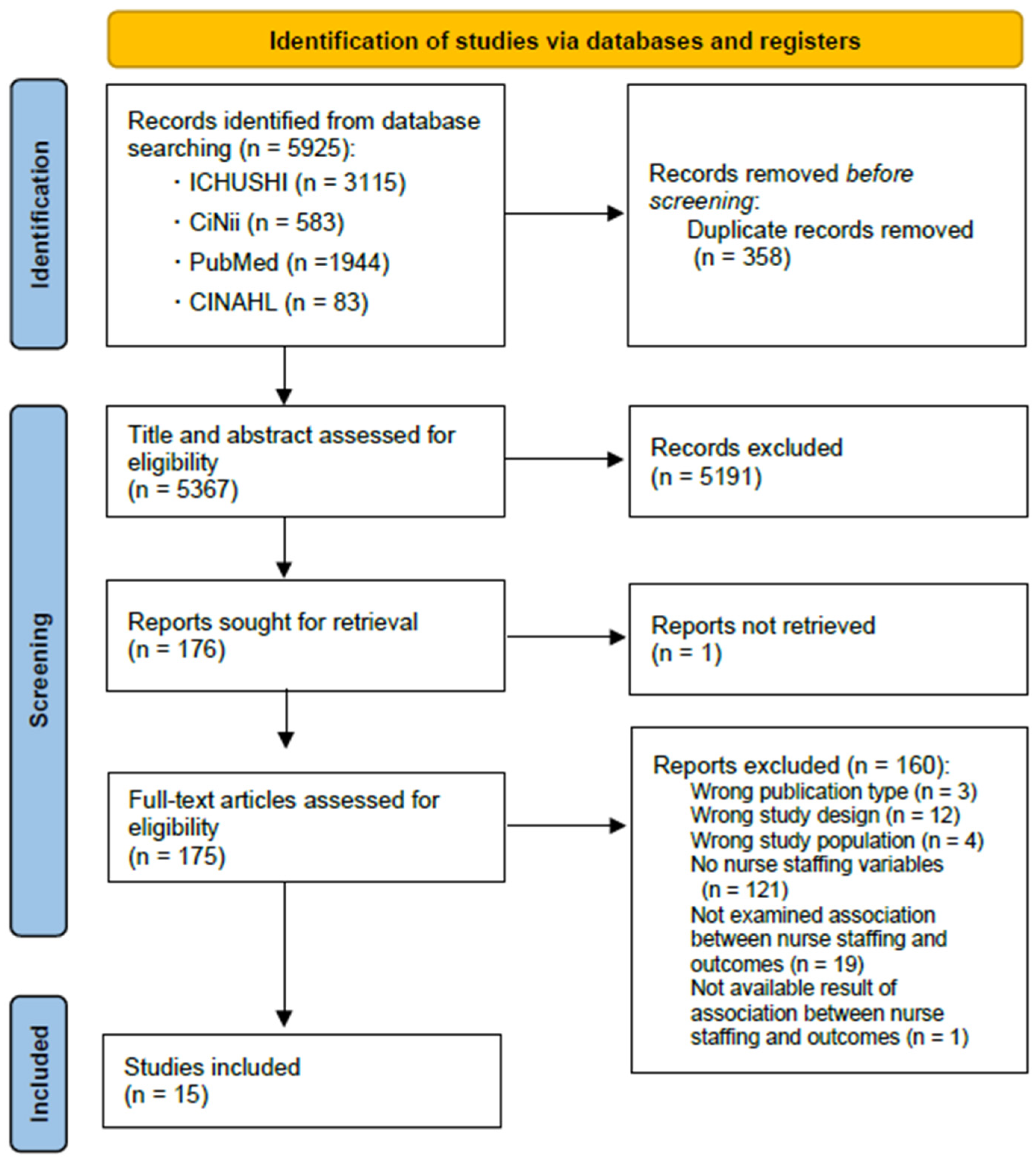
3.1. Search Results
3.2. Study Characteristics
3.3. Nurse Staffing Level Measures
3.4. Outcome Measures
3.5. Evidence of the Association between Nurse Staffing Level and Outcomes
4. Discussion
4.1. Nurse Staffing Level Measures
4.2. Outcome Measures
4.3. Evidence of the Association between Nurse Staffing Level and Outcomes in Japanese Hospitals
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aiken, L.H.; Clarke, S.P.; Sloane, D.M.; Sochalski, J.; Silber, J.H. Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA 2002, 288, 1987–1993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needleman, J.; Buerhaus, P.; Mattke, S.; Stewart, M.; Zelevinsky, K. Nurse-staffing Levels and the Quality of Care in Hospitals. N. Engl. J. Med. 2002, 346, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Blume, K.S.; Dietermann, K.; Kirchner-Heklau, U.; Winter, V.; Fleischer, S.; Kreidl, L.M.; Meyer, G.; Schreyögg, J. Staffing Levels and Nursing-sensitive Patient Outcomes: Umbrella Review and Qualitative Study. Health Serv. Res. 2021, 56, 885–907. [Google Scholar] [CrossRef] [PubMed]
- Morioka, N.; Tomio, J.; Seto, T.; Kobayashi, Y. The Association between Higher Nurse Staffing Standards in the Fee Schedules and the Geographic Distribution of Hospital Nurses: A Cross-Sectional Study Using Nationwide Administrative Data. BMC Nurs. 2017, 16, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanda, K. Research on Economic Evaluation of Nursing Service [Kango Sabis No Keizaiteki Hyouka ni Kansuru Kennkyu]; Ministry of Health, Labour, and Welfare Grants System: Tokyo, Japan, 1998. (In Japanese)
- Takase, M.; Imai, T. The Effects of Patient-to-nurse Ratios in Health Care: A Review of International Literature. Jpn. J. Occup. Med. Traumatol. 2017, 65, 53–60. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Dall’Ora, C.; Saville, C.; Rubbo, B.; Turner, L.Y.; Jones, J.; Griffiths, P. Nurse Staffing Levels and Patient Outcomes: A Systematic Review of Longitudinal Studies. medRxiv 2021. [Google Scholar] [CrossRef]
- Ito, K.; Kawano, K.; Hatanaka, J.; Goto, Y. Factors Influencing Work Engagement of Night Shift Work Nurses in a Group Hospitals. J. Yokkaichi Nurs. Med. Care Univ. 2018, 11, 1–12. (In Japanese) [Google Scholar]
- Kaneko, S.; Koinuma, N.; Ito, M. Relationship between Risk Factors Related Medical Errors and Working Conditions of Nurses in Acute Care Settings. J. Jpn. Acad. Nurs. Adm. Policies 2008, 12, 5–15. (In Japanese) [Google Scholar] [CrossRef]
- Namba, H.; Wakabayashi, T.; Koike, A. Relationship between Nurse-patient Ratio and Job Satisfaction and Intention to Continue Working in the Organization. J. Mie Prefect. Coll. Nurs. 2014, 17, 7–16. (In Japanese) [Google Scholar]
- Anzai, E.; Douglas, C.; Bonner, A. Nursing Practice Environment, Quality of Care, and Morale of Hospital Nurses in Japan. Nurs. Health Sci. 2014, 16, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimura, Y.; Tanii, H.; Saijoh, K. Inpatient Satisfaction and Job Satisfaction/stress of Medical Workers in a Hospital with the 7:1 Nursing Care System (in Which 1 Nurse Cares for 7 Patients at a Time). Environ. Health Prev. Med. 2011, 16, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukasawa, M.; Miyake, M.; Suzuki, Y.; Fukuda, Y.; Yamanouchi, Y. Relationship between the Use of Seclusion and Mechanical Restraint and the Nurse-bed Ratio in Psychiatric Wards in Japan. Int. J. Law Psychiatry 2018, 60, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Hirose, N.; Morita, K.; Matsui, H.; Fushimi, K.; Yasunaga, H. Dose-response Association between Nurse Staffing and Patient Outcomes Following Major Cancer Surgeries Using a Nationwide Inpatient Database in Japan. J. Clin. Nurs. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ibe, T.; Ishizaki, T.; Oku, H.; Ota, K.; Takabatake, Y.; Iseda, A.; Ishikawa, Y.; Ueda, A. Predictors of Pressure Ulcer and Physical Restraint Prevalence in Japanese Acute Care Units. Jpn. J. Nurs. Sci. 2008, 5, 91–98. [Google Scholar] [CrossRef]
- Morioka, N.; Moriwaki, M.; Tomio, J.; Kashiwagi, M.; Fushimi, K.; Ogata, Y. Structure and Process of Dementia Care and Patient Outcomes after Hip Surgery in Elderly People with Dementia: A Retrospective Observational Study in Japan. Int. J. Nurs. Stud. 2020, 102, 103470. [Google Scholar] [CrossRef]
- Morioka, N.; Moriwaki, M.; Tomio, J.; Fushimi, K.; Ogata, Y. Dementia and Patient Outcomes after Hip Surgery in Older Patients: A Retrospective Observational Study Using Nationwide Administrative Data in Japan. PLoS ONE 2021, 16, e0249364. [Google Scholar] [CrossRef]
- Morita, K.; Matsui, H.; Fushimi, K.; Yasunaga, H. Association between Nurse Staffing and In-Hospital Bone Fractures: A Retrospective Cohort Study. Health Serv. Res. 2017, 52, 1005–1023. [Google Scholar] [CrossRef]
- Nawata, S.; Yamauchi, K.; Ikegami, N. Do Staffing Levels Determine Outcome in Psychiatric Inpatient Care?: Factors Related to the Ratio of Period Hospitalized in Japan. Psychiatry Clin. Neurosci. 2006, 60, 709–717. [Google Scholar] [CrossRef]
- Tei-Tominaga, M. Factors Related to the Intention to Leave and the Decision to Resign among Newly Graduated Nurses: A Complete Survey in a Selected Prefecture in Japan. Environ. Health Prev. Med. 2013, 18, 293–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasunaga, H.; Hashimoto, H.; Horiguchi, H.; Miyata, H.; Matsuda, S. Variation in Cancer Surgical Outcomes Associated with Physician and Nurse Staffing: A Retrospective Observational Study Using the Japanese Diagnosis Procedure Combination Database. BMC Health Serv. Res. 2012, 12, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, E.; Itomine, I.; Kanoya, Y.; Katsuki, T.; Horii, S.; Sato, C. Factors Affecting Rapid Turnover of Novice Nurses in University Hospitals. J. Occup. Health 2006, 48, 49–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and Profile of Diagnosis Procedure Combination (DPC): Development of a Real Data Collection System for Acute Inpatient Care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Calculation of Patient-to-Nurse Ratio per Shift in the Fee Schedule [Nyuiniryo no Hyouka No Arikata ni Tuite]; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2005.
- Spetz, J.; Donaldson, N.; Aydin, C.; Brown, D.S. How Many Nurses per Patient? Measurements of Nurse Staffing in Health Services Research. Health Serv. Res. 2008, 43, 1674–1692. [Google Scholar] [CrossRef] [Green Version]
- Sermeus, W.; Aiken, L.H.; van den Heede, K.; Rafferty, A.M.; Griffiths, P.; Moreno-Casbas, M.T.; Busse, R.; Lindqvist, R.; Scott, A.P.; Bruyneel, L.; et al. Nurse Forecasting in Europe (RN4CAST): Rationale, Design and Methodology. BMC Nurs. 2011, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- National Quality Forum National Voluntary Consensus Standards for Nursing-Sensitive Care: An Initial Performance Measure Set. Available online: https://www.qualityforum.org/Publications/2004/10/National_Voluntary_Consensus_Standards_for_Nursing-Sensitive_Care__An_Initial_Performance_Measure_Set.aspx (accessed on 3 March 2022).
- Lake, E.T. Development of the Practice Environment Scale of the Nursing Work Index. Res. Nurs. Health 2002, 25, 176–188. [Google Scholar] [CrossRef]
- Pearson, A.; Pallas, L.O.; Thomson, D.; Doucette, E.; Tucker, D.; Wiechula, R.; Long, L.; Porritt, K.; Jordan, Z. Systematic Review of Evidence on the Impact of Nursing Workload and Staffing on Establishing Healthy Work Environments. Int. J. Evid.-Based Healthc. 2006, 4, 337–384. [Google Scholar] [CrossRef]
- Twigg, D.; McCullough, K. Nurse Retention: A Review of Strategies to Create and Enhance Positive Practice Environments in Clinical Settings. Int. J. Nurs. Stud. 2014, 51, 85–92. [Google Scholar] [CrossRef]
- Kane, R.L.; Shamliyan, T.A.; Mueller, C.; Duval, S.; Wilt, T.J. The Association of Registered Nurse Staffing Levels and Patient Outcomes: Systematic Review and Meta-analysis. Med. Care 2007, 45, 1195–1204. [Google Scholar] [CrossRef]
- Di Giulio, P.; Clari, M.; Conti, A.; Campagna, S. The Problems in the Interpretation of the Studies on the Relationship between Staffing and Patients’ Outcomes: The Case of the RN4CAST Studies. Assist. Inferm. Ric. 2019, 38, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.; Maruotti, A.; Recio Saucedo, A.; Redfern, O.C.; Ball, J.E.; Briggs, J.; Dall’Ora, C.; Schmidt, P.E.; Smith, G.B. Nurse Staffing, Nursing Assistants and Hospital Mortality: Retrospective Longitudinal Cohort Study. BMJ Qual. Saf. 2019, 28, 609–617. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Design and Data Source | Setting, Participants, and Sample Size | Measurement of Staffing | Outcome Measures | Analysis and Potential Confounders Measured and Included in the Analysis | Main Findings |
|---|---|---|---|---|---|---|
| Nawata et al. [21] | Two-wave questionnaire survey (October 1993 and October 1999) | Patients (first survey) = 2386; Patients (second survey) = 1131, Psychiatric hospitals = 18 | Patient-to-nurse ratio per shift (wards average at hospital level) | Percentage of followed-up period hospitalized | Bivariate analysis | No statistically significant association |
| Suzuki et al. [24] | Longitudinal questionnaire survey from June 2003 to December 2003 | Novice full-time nurses in 2003 = 1203, University hospitals = 20 | Patient-to-nurse ratio requirement in the fee schedule (hospital level) 7:1 vs. 10:1 | Rapid turnover among novice nurses | Bivariate analysis | No statistically significant association |
| Ibe et al. [17] | Longitudinal questionnaire survey from 1 November 2005 to 31 January 2006 | Hospital nursing unit managers = 98, Hospitals = 42 | Registered nurse hours per patient day (ward level) Associate nurse hours per patient day (ward level) | Pressure ulcer, physical restraint | Multiple regression analysis Conf.: a patient-level variable, work environment variables | More associated nurse hours per patient (daily) related to lower number of pressure ulcer |
| Kaneko et al. [11] | Cross-sectional questionnaire survey during November and December 2005 | Nurses = 787 (candidates = 1339), Hospitals = 6 | Patient-to-nurse ratio on day/ night shift (nurse individual level) | Medical error, medical mistakes | Univariate logistic regressionConf.: age | No statistically significant association |
| Fujimura et al. [14] | Questionnaire survey from January 2008 to December 2008 | Inpatient survey: Inpatients = 202, Hospital = 1 | Patient-to-nurse ratio requirement in the fee schedule (hospital level) 7:1 vs. 10:1 | Inpatient satisfaction with nursing care | Bivariate analysis | 7:1 system showed statistically greater satisfaction than that in the 10:1 system |
| Medical workers survey: First survey: Physicians = 36, Nurses = 14 Second survey: Physicians = 33, Nurses = 25 Hospital = 1 | Job satisfaction, effects of the DPC, stress of medical workers | Bivariate analysis | Nurses under the 7:1 system judged that their working hours were shortened compared to those under the 10:1 system No statistically significant association with nurse-reported nursing care and stress | |||
| Yasunaga et al. [23] | Retrospective observational study Data: DPC, the Survey of Medical Institutions data | Patients = 131,394 (underwent elective cancer surgery between 2007 and 2008) | Number of physicians per 100 occupied beds, number of nurses per 100 occupied beds (hospital level) | Post-operative complications, in-hospital mortality, failure to rescue | Logistic regression analysis Conf.: patient-level variables, hospital volume | Higher number of patients and nurses per occupied bed associated with lower failure to rescue but not associated with post-operative complications and in-hospital mortality |
| Namba et al. [12] | Cross-sectional questionnaire survey from 22 April to 28 May 2009 | Full-time nurses of = 919 (candidates = 2213), Hospitals = 15 | Number-of-patients-to-nurse ratio (hospital level) 7:1 vs. 10:1 | Job satisfaction, retention potential | Bivariate analysis | Job satisfaction in 7:1 system was higher than that in 10:1 |
| Tei-Tominaga [22] | Cross-sectional questionnaire survey in December 2009 | Newly graduated nurses = 493 (candidates = 1477), Hospitals = 353 | Patient-to-nurse ratio requirement in the fee schedule (hospital level) | Intention to leave, decision to resign | Multivariate logistic regression analysis Conf.: employment and organizational characteristics, individual factors | No statistically significant association |
| Anzai et al. [13] | Cross-sectional questionnaire survey | Nurses = 223 (candidates = 341), Acute care inpatient wards = 12, Hospital = 1 | Patient-to-nurse ratio in usual day shift (nurse individual level) | Ability to provide quality nursing care, quality of care, ward morale | Multiple regression analyses Conf.: demographic characteristics, work characteristics, work environment, management | Higher patient-to-nurse ratio in usual day shift was associated with lower ward morale but not associated with ability to provide quality nursing care |
| Morita et al. [20] | Retrospective cohort study Data: DPC, the Surveys for Medical Institution | Patients = 770,373 (50 years or older and underwent planned major cancer or cardiovascular surgery from July 2010 to March 2014), Hospitals = 1074 | Nurse-to-occupied-bed ratio (hospital level) | The occurrence of in-hospital bone fractures | Logistic regression analysis Conf.: patient-level variables | The higher nurses-to-occupied-bed ratio was associated with lower risk of in-hospital bone fractures |
| Fukasawa et al. [15] | Secondary analysis of clinical database, the Psychiatric Electronic Clinical Observation (PECO) system from April 2015 to March 2017 | Admissions = 10,013, Hospitals = 23 | Nurse to 10 beds in each psychiatric ward (ward level) | Use of seclusion or mechanical restraint during the first 90 days of admission | Multilevel logistic regression analysis Conf.: patient-level variables, hospital(ward)-level variables | The higher number of nurses per bed was associated with higher risk of seclusion and mechanical restraint |
| Ito et al. [10] | Cross-sectional questionnaire survey from 5 December 2013 to 25 December 2013 | Shift-work nurses = 1275 Hospitals = 13 | Patient-to-nurse ratio requirement in the fee schedule (hospital level) | Work engagement | Bivariate analysis | No statistically significant association |
| Morioka et al. [18] | Retrospective observational study Data: DPC, reporting on medical functions of hospital beds data | Patients = 20,393 (dementia, 65 years or older, underwent hip surgeries and discharged from April 2016 to March 2017), Hospitals = 405 | Patient-to-nurse ratio per shift (wards average at hospital level) | In-hospital mortality, readmission within 30 days, length of hospital stay | Logistic regression analysis (for in-hospital mortality and readmission within 30 days), regression analysis (for length of hospital stay) Conf.: patient-level variables, hospital-level variables | Higher number of patient-to-nurse ratio associated with extended length of hospital stay but not associated with other outcomes |
| Morioka et al. [19] | Retrospective observational study Data: DPC, reporting on medical functions of hospital beds data | Patients = 48,797 (65 years or older, underwent hip surgeries and discharged from April 2016 to March 2017), Acute care hospitals = 404 | Patient-to-nurse ratio per shift (wards average at hospital level) | In-hospital mortality, in-hospital pneumonia, in-hospital fracture, length of hospital stay | Multilevel logistic regression analysis Conf.: patient-level variables, hospital-level variables | Higher number of patient-to-nurse ratio associated with extended length of hospital stay but not associated with other outcomes |
| Hirose et al. [16] | Retrospective observational study Data: DPC, the Annual Report for Functions of Medical Institution | Patients = 645687 (aged 20–99 years, underwent major cancer surgeries from July 2010 to March 2018), Hospitals = 787 | Patient-to-nurse ratio per shift (wards average at hospital level) | 30-day in-hospital mortality, failure to rescue, post-operative complications | Restricted cubic spline regression analyses Conf.: patient-level variables, hospital-level variables | Higher number of patient-to-nurse ratio was associated with post-operative complication (J-shaped association) but not associated with other outcomes |
| Patient-to-Nurse Ratio | Nursing Hours per Patient Day | Nurse-to-Bed Ratio | ||||||
|---|---|---|---|---|---|---|---|---|
| Patient-to-Nurse Ratio Requirement in the Fee Schedule | Patient-to-Nurse Ratio per Shift | Registered Nurse Hours per Patient Day | Associate Nurse Hours per Patient Day | |||||
| Hospital Level | Average Wards at Hospital Level | Nurse at Individual Level | Ward Level | Ward Level | Hospital Level | Ward Level | ||
| Patient outcome | Readmission | N.S. [18] | ||||||
| Hospitalization | N.S.§ [21] | |||||||
| In-hospital mortality | N.S. [16,18,19,23] | N.S.† [23] | ||||||
| Failure to rescue | N.S. [16] | △† [23] | ||||||
| Length of hospital stay | ▲ [18,19] | |||||||
| In-hospital fracture | N.S. [19] | △ [20] | ||||||
| In-hospital pneumonia | N.S. [19] | |||||||
| Post-operative complications | ▲‡ [16] | N.S.† [23] | ||||||
| Seclusion | ▽ [15] | |||||||
| Pressure ulcer | N.S. [17] | △ [17] | ||||||
| Physical restraint | N.S. [17] | N.S. [17] | ▽ [15] | |||||
| Error and/or near miss | N.S.§ [11] | |||||||
| Patient satisfaction with nursing care | △§ [14] | |||||||
| Nursing care quality | Nurse-reported quality of care | N.S.§ [14] | N.S. [13] | |||||
| Ability to provide quality nursing care | N.S. [13] | |||||||
| Nurse outcome | Work engagement | N.S. § [10] | ||||||
| Job satisfaction | △§ [12] | |||||||
| Stressor of work | N.S.§ [14] | |||||||
| Response to stress (mental, physical) | N.S.§ [14] | |||||||
| Intention to leave | N.S.§ [22] | |||||||
| Decision to leave | N.S.§ [22, 24] | |||||||
| Nurse-reported better working environment | △§ [14] | |||||||
| Ward morale | ▲ [13] | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morioka, N.; Okubo, S.; Moriwaki, M.; Hayashida, K. Evidence of the Association between Nurse Staffing Levels and Patient and Nurses’ Outcomes in Acute Care Hospitals across Japan: A Scoping Review. Healthcare 2022, 10, 1052. https://doi.org/10.3390/healthcare10061052
Morioka N, Okubo S, Moriwaki M, Hayashida K. Evidence of the Association between Nurse Staffing Levels and Patient and Nurses’ Outcomes in Acute Care Hospitals across Japan: A Scoping Review. Healthcare. 2022; 10(6):1052. https://doi.org/10.3390/healthcare10061052
Chicago/Turabian StyleMorioka, Noriko, Suguru Okubo, Mutsuko Moriwaki, and Kenshi Hayashida. 2022. "Evidence of the Association between Nurse Staffing Levels and Patient and Nurses’ Outcomes in Acute Care Hospitals across Japan: A Scoping Review" Healthcare 10, no. 6: 1052. https://doi.org/10.3390/healthcare10061052
APA StyleMorioka, N., Okubo, S., Moriwaki, M., & Hayashida, K. (2022). Evidence of the Association between Nurse Staffing Levels and Patient and Nurses’ Outcomes in Acute Care Hospitals across Japan: A Scoping Review. Healthcare, 10(6), 1052. https://doi.org/10.3390/healthcare10061052