
Changes in Maximum Mandibular Mobility Due to Splint Therapy in Patients with Temporomandibular Disorders

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Maximum Mouth Opening
3.2. Condyle Motion during Maximum Mouth Opening
3.3. Lateral and Retrusion Movements
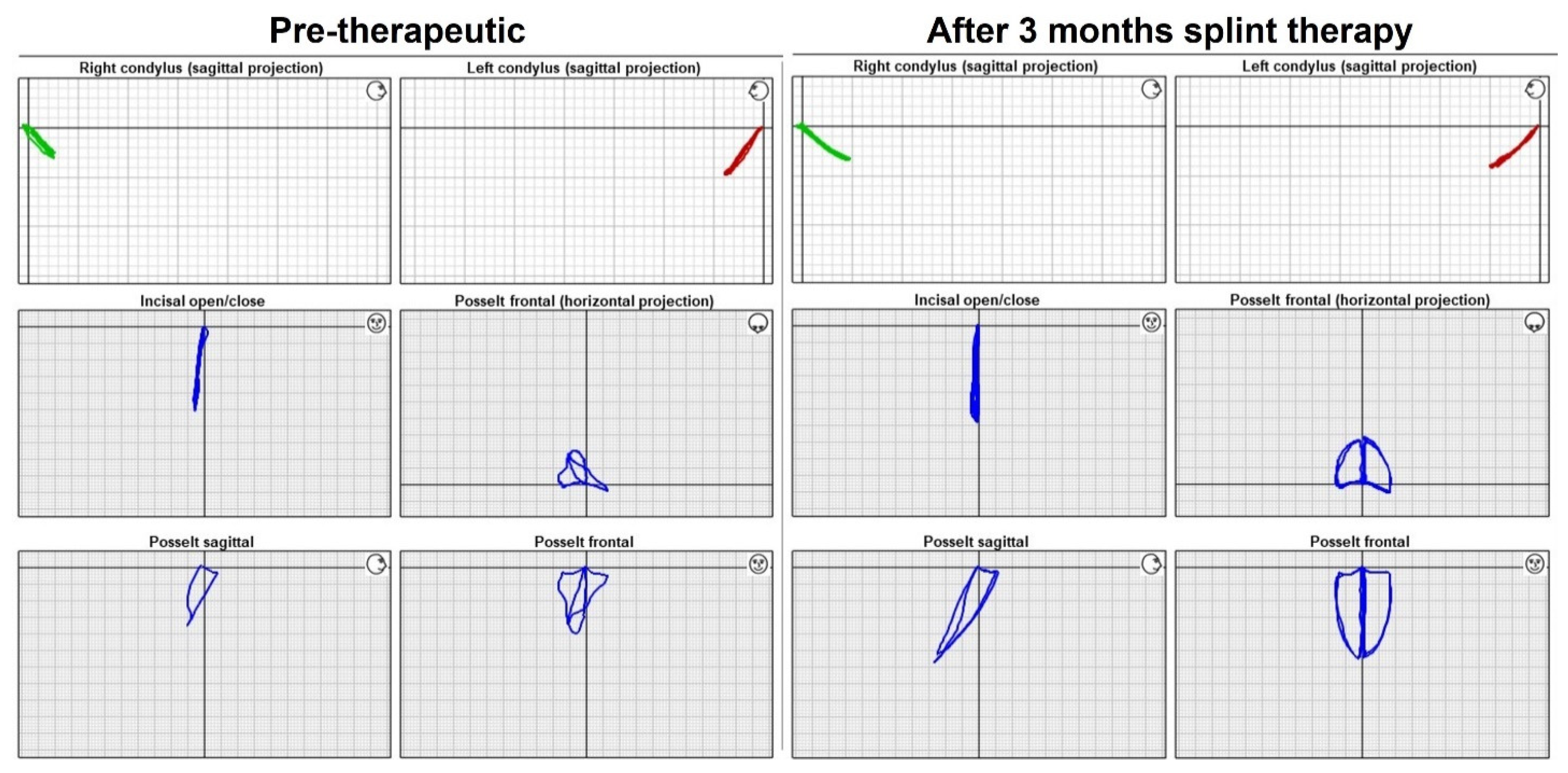
3.4. Pre-and Post-Therapeutic Qualitative Assessment of Movement Patterns
3.5. Post-Therapeutic Qualitative Assessment of Pain Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deregibus, A.; Ferrillo, M.; Grazia Piancino, M.; Chiara Domini, M.; de Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; DeNardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; De Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Aldemir, K.; Üstüner, E.; Erdem, E.; Demiralp, A.S.; Oztuna, D. Ultrasound evaluation of masseter muscle changes in stabilization splint treatment of myofascial type painful temporomandibular diseases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 377–383. [Google Scholar] [CrossRef] [PubMed]
- List, T.; Jensen, R.H. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef] [PubMed]
- Fleckenstein, J.; Zaps, D.; Rüger, L.J.; Lehmeyer, L.; Freiberg, F.; Lang, P.M.; Irnich, D. Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: Results of a cross-sectional, nationwide survey. BMC Musculoskelet. Disord. 2010, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Gerber, L.H.; Sikdar, S.; Armstrong, K.; Diao, G.; Heimur, J.; Kopecky, J.; Turo, D.; Otto, P.; Gebreab, T.; Shah, J. A Systematic Comparison Between Subjects with No Pain and Pain Associated With Active Myofascial Trigger Points. PMR 2013, 5, 931–938. [Google Scholar] [CrossRef] [Green Version]
- Pastore, G.P.; Goulart, D.R.; Pastore, P.R.; Prati, A.J.; De Moraes, M. Self-medication Among Myofascial Pain Patients: A Preliminary Study. Open Dent. J. 2018, 12, 347–353. [Google Scholar] [CrossRef] [Green Version]
- Bender, S.D. Temporomandibular disorders, facial pain, and headaches. Headache 2012, 52 (Suppl. 1), 22–25. [Google Scholar] [CrossRef]
- de Leeuw, R.; Klasser, G.D. Orofacial Pain Guidelines for Assessment, Diagnosis, and Management; Quintessence Publishing Co., Inc.: Chicago, IL, USA, 2013. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; Dworkin, S.F. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Al-Moraissi, E.; Farea, R.; Qasem, K.; Al-Wadeai, M.; Al-Sabahi, M.; Al-Iryani, G. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: Network meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2020, 49, 1042–1056. [Google Scholar] [CrossRef]
- Kuzmanovic Pficer, J.; Dodic, S.; Lazic, V.; Trajkovic, G.; Milic, N.; Milicic, B. Occlusal stabilization splint for patients with temporomandibular disorders: Meta-analysis of short and long term effects. PLoS ONE 2017, 12, e0171296. [Google Scholar] [CrossRef] [PubMed]
- Machado, D.; Martimbianco, A.L.C.; Bussadori, S.; Pacheco, R.L.; Riera, R.; Santos, E.M. Botulinum Toxin Type A for Painful Temporomandibular Disorders: Systematic Review and Meta-Analysis. J. Pain 2020, 21, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Keskin Tunç, S.; Ünalan Değirmenci, B.; Alpaslan Yaylı, N.; Aslan, Ş.; Akdeniz, M.Ş. Evaluation the effects of low-level laser therapy on disc displacement with reduction. Turk. J. Phys. Med. Rehabil. 2020, 66, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Aksu, Ö.; Pekin Doğan, Y.; Sayıner Çağlar, N.; Şener, B.M. Comparison of the efficacy of dry needling and trigger point injections with exercise in temporomandibular myofascial pain treatment. Turk. J. Phys. Med. Rehabil. 2019, 65, 228–235. [Google Scholar] [CrossRef]
- Liu, G.-F.; Gao, Z.; Liu, Z.-N.; Yang, M.; Zhang, S.; Tan, T.-P. Effects of Warm Needle Acupuncture on Temporomandibular Joint Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2021, 2021, 6868625. [Google Scholar] [CrossRef] [PubMed]
- Ferrillo, M.; Ammendolia, A.; Paduano, S.; Calafiore, D.; Marotta, N.; Migliario, M.; Fortunato, L.; Giudice, A.; Michelotti, A.; de Sire, A. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials. J. Back Musculoskelet. Rehabil. 2022, 1–16, Preprint. [Google Scholar] [CrossRef] [PubMed]
- Hou, C.-R.; Tsai, L.-C.; Cheng, K.-F.; Chung, K.-C.; Hong, C.-Z. Immediate effects of various physical therapeutic modalities on cervical myofascial pain and trigger-point sensitivity. Arch. Phys. Med. Rehabil. 2002, 83, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Ramfjord, S.; Ash, M.M. Reflections on the Michigan occlusal splint. J. Oral Rehabil. 1994, 21, 491–500. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Krügel, M.; Wesemann, C.; Pieralli, S.; Nold, J.; Spies, B.C.; Vach, K.; Kohal, R.-J. In Vitro Time Efficiency, Fit, and Wear of Conventionally- versus Digitally-Fabricated Occlusal Splints. Materials 2022, 15, 1085. [Google Scholar] [CrossRef]
- Posselt, U. Studies in the mobility of the human mandible. Acta Odontol. Scand. 1952, 10 (Suppl. 19), 1–160. [Google Scholar]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, ume 11, 851–856. [Google Scholar] [CrossRef] [Green Version]
- Daif, E.T. Correlation of splint therapy outcome with the electromyography of masticatory muscles in temporomandibular disorder with myofascial pain. Acta Odontol. Scand. 2011, 70, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Tetè, S.; D’Attilio, M.; Perillo, L.; Festa, F. Surface electromyographic patterns of masticatory, neck, and trunk muscles in temporomandibular joint dysfunction patients undergoing anterior repositioning splint therapy. Eur. J. Orthod. 2008, 30, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannakopoulos, N.N.; Rauer, A.; Hellmann, D.; Hugger, S.; Schmitter, M.; Hugger, A. Comparison of device-supported sensorimotor training and splint intervention for myofascial temporomandibular disorder pain patients. J. Oral Rehabil. 2018, 45, 669–676. [Google Scholar] [CrossRef]
- Zhang, F.-Y.; Wang, X.-G.; Dong, J.; Zhang, J.-F.; Lü, Y.-L. Effect of occlusal splints for the management of patients with myofascial pain: A randomized, controlled, double-blind study. Chin. Med. J. 2013, 126, 2270–2275. [Google Scholar]
- Berni, K.C.D.S.; Filho, A.V.D.; Pires, P.; Rodrigues-Bigaton, D. Accuracy of the surface electromyography RMS processing for the diagnosis of myogenous temporomandibular disorder. J. Electromyogr. Kinesiol. 2015, 25, 596–602. [Google Scholar] [CrossRef]
- Castroflorio, T.; Icardi, K.; Torsello, F.; Deregibus, A.P.; Debernardi, C.L.; Bracco, P. Reproducibility of Surface EMG in the Human Masseter and Anterior Temporalis Muscle Areas. Cranio J. Craniomandib. Pract. 2005, 23, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Szyszka-Sommerfeld, L.; Machoy, M.; Lipski, M.; Woźniak, K. The Diagnostic Value of Electromyography in Identifying Patients With Pain-Related Temporomandibular Disorders. Front. Neurol. 2019, 10, 180. [Google Scholar] [CrossRef]
- Santana-Mora, U.; López-Ratón, M.; Mora, M.J.; Cadarso-Suárez, C.; López-Cedrún, J.; Santana-Penín, U. Surface raw electromyography has a moderate discriminatory capacity for differentiating between healthy individuals and those with TMD: A diagnostic study. J. Electromyogr. Kinesiol. 2014, 24, 332–340. [Google Scholar] [CrossRef]
- Manfredini, D.; Cocilovo, F.; Favero, L.; Ferronato, G.; Tonello, S.; Guarda-Nardini, L. Surface electromyography of jaw muscles and kinesiographic recordings: Diagnostic accuracy for myofascial pain. J. Oral Rehabil. 2011, 38, 791–799. [Google Scholar] [CrossRef]
- Cooper, B.C.; Adib, F. An assessment of the usefulness of Kinesiograph as an aid in the diagnosis of TMD: A review of Manfredini et al.’s studies. Cranio J. Craniomandib. Pract. 2015, 33, 46–66. [Google Scholar] [CrossRef] [PubMed]
- Wieckiewicz, M.; Ziętek, M.; Nowakowska, D.; Więckiewicz, W. Comparison of Selected Kinematic Facebows Applied to Mandibular Tracing. BioMed Res. Int. 2014, 2014, 818694. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Fu, H.; Zeng, R.; Yang, X. Changes of Mandibular Movement Tracings After the Correction of Mandibular Protrusion by Bilateral Sagittal Split Ramus Osteotomy. J. Oral Maxillofac. Surg. 2009, 67, 2238–2244. [Google Scholar] [CrossRef] [PubMed]
- Stiesch-Scholz, M.; Demling, A.; Rossbach, A. Reproducibility of jaw movements in patients with craniomandibular disorders. J. Oral Rehabil. 2006, 33, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Kobs, G.; Didziulyte, A.; Kirlys, R.; Stacevicius, M. Reliability of ARCUSdigma (KaVo) in diagnosing temporomandibular joint pathology. Stomatologija 2007, 9, 47–55. [Google Scholar]
- Frisoli, M.; Edelhoff, J.M.; Gersdorff, N.; Nicolet, J.; Braidot, A.; Engelke, W. Comparative study using video analysis and an ultrasonic measurement system to quantify mandibular movement. Cranio J. Craniomandib. Pract. 2015, 35, 19–29. [Google Scholar] [CrossRef]
- Kaya, K.; Dulgeroglu, D.; Unsal-Delialioglu, S.; Babadag, M.; Tacal, T.; Barlak, A.; Ozel, S. Diagnostic value of ultrasonography in the evaluation of the temporomandibular joint anterior disc displacement. J. Cranio-Maxillofac. Surg. 2010, 38, 391–395. [Google Scholar] [CrossRef]


{kind=link}
| Difference of Variables in (mm) | Median | Min. | Max. | IQR | p-Value | Sign |
|---|---|---|---|---|---|---|
| Maximum opening | +6.15 | 0.20 | 17.01 | 7.95 | <0.001 | *** |
| Left condyle motion during maximum opening | +1.93 | −1.29 | 10.55 | 3.29 | 0.191 | n.s. |
| Right condyle motion during maximum opening | +2.73 | −0.75 | 18.00 | 4.64 | 0.045 | * |
| Left condyle motion during retrusion | +0.38 | −1.15 | 2.29 | 0.38 | 0.716 | n.s. |
| Right condyle motion during retrusion | +0.28 | −0.06 | 1.19 | 0.55 | 0.356 | n.s. |
| Left laterotrusion | +0.73 | −1.05 | 4.73 | 2.54 | 0.154 | n.s. |
| Right laterotrusion | +0.63 | −3.90 | 5.11 | 2.12 | 0.510 | n.s. |
| Patient | Right Condyle (Sagittal) | Left Condyle (Sagittal) | Maximum opening (Frontal) | Posselt (Frontal) | Posselt (Sagittal) | Posselt (Axial) |
|---|---|---|---|---|---|---|
| 001 | (+) | (+) | + | + | + | + |
| 002 | + | + | + | + | + | + |
| 003 | (+) | (+) | + | + | (+) | + |
| 004 | + | + | + | + | + | + |
| 005 | + | + | + | + | + | + |
| 006 | + | (+) | (+) | + | + | + |
| 007 | + | + | + | (+) | (+) | (+) |
| 008 | (+) | + | + | + | + | + |
| 009 | + | (+) | + | (+) | + | (+) |
| 010 | – | – | (+) | (+) | (+) | (+) |
| 011 | – | – | + | + | + | + |
| 012 | (+) | + | (+) | + | + | + |
| 013 | (+) | – | – | – | (+) | – |
| 014 | + | + | + | (+) | (+) | (+) |
| 015 | (+) | (+) | + | – | + | – |
| 016 | + | + | + | + | + | + |
| 017 | – | – | + | (+) | + | (+) |
| 018 | + | + | + | + | + | + |
| 019 | + | + | + | + | + | (+) |
| 020 | – | – | (+) | – | + | (+) |
| 021 | + | + | + | + | + | + |
| 022 | – | – | + | + | (+) | (+) |
| 023 | (+) | (+) | + | + | – | – |
| 024 | (+) | – | + | – | – | – |
| 025 | + | + | + | + | + | + |
| 026 | + | (+) | + | (+) | – | – |
| 027 | – | – | (+) | (+) | (+) | (+) |
| 028 | + | + | (+) | + | (+) | + |
| 029 | (+) | – | (+) | – | (+) | – |
| Number of Patients | No Change from Baseline | Improvement from Baseline | Complete Remission | Exacerbation from Baseline |
|---|---|---|---|---|
| 29 | 5 (17) | 24 (83) | 17 (59) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiechens, B.; Paschereit, S.; Hampe, T.; Wassmann, T.; Gersdorff, N.; Bürgers, R. Changes in Maximum Mandibular Mobility Due to Splint Therapy in Patients with Temporomandibular Disorders. Healthcare 2022, 10, 1070. https://doi.org/10.3390/healthcare10061070
Wiechens B, Paschereit S, Hampe T, Wassmann T, Gersdorff N, Bürgers R. Changes in Maximum Mandibular Mobility Due to Splint Therapy in Patients with Temporomandibular Disorders. Healthcare. 2022; 10(6):1070. https://doi.org/10.3390/healthcare10061070
Chicago/Turabian StyleWiechens, Bernhard, Svea Paschereit, Tristan Hampe, Torsten Wassmann, Nikolaus Gersdorff, and Ralf Bürgers. 2022. "Changes in Maximum Mandibular Mobility Due to Splint Therapy in Patients with Temporomandibular Disorders" Healthcare 10, no. 6: 1070. https://doi.org/10.3390/healthcare10061070
APA StyleWiechens, B., Paschereit, S., Hampe, T., Wassmann, T., Gersdorff, N., & Bürgers, R. (2022). Changes in Maximum Mandibular Mobility Due to Splint Therapy in Patients with Temporomandibular Disorders. Healthcare, 10(6), 1070. https://doi.org/10.3390/healthcare10061070