
Hepatitis of Unknown Origin and Etiology (Acute Non HepA-E Hepatitis) among Children in 2021/2022: Review of the Current Findings

 ,
, 
Abstract
:1. Introduction
2. Case Definition for Acute Non HepA-E Hepatitis
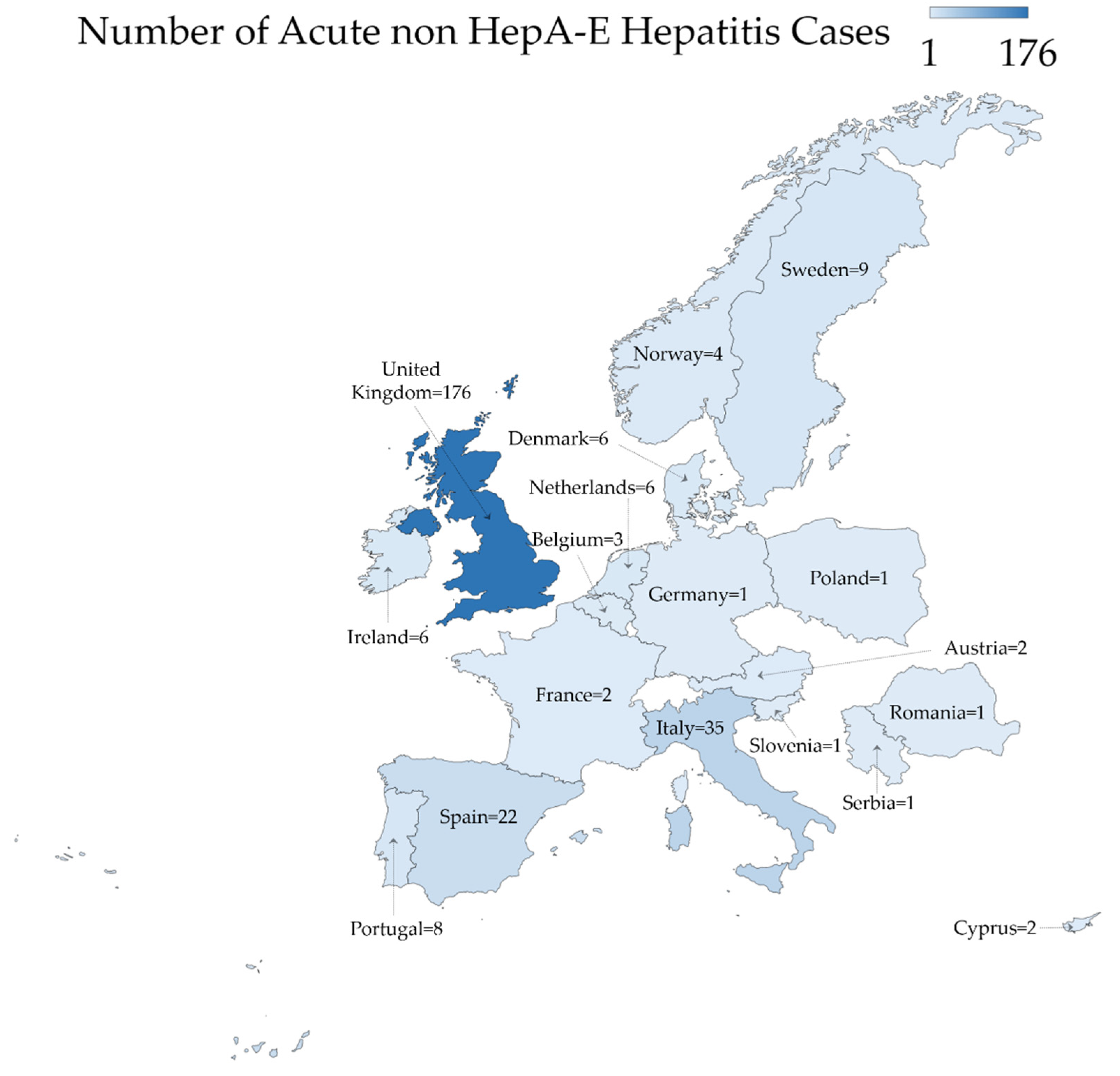
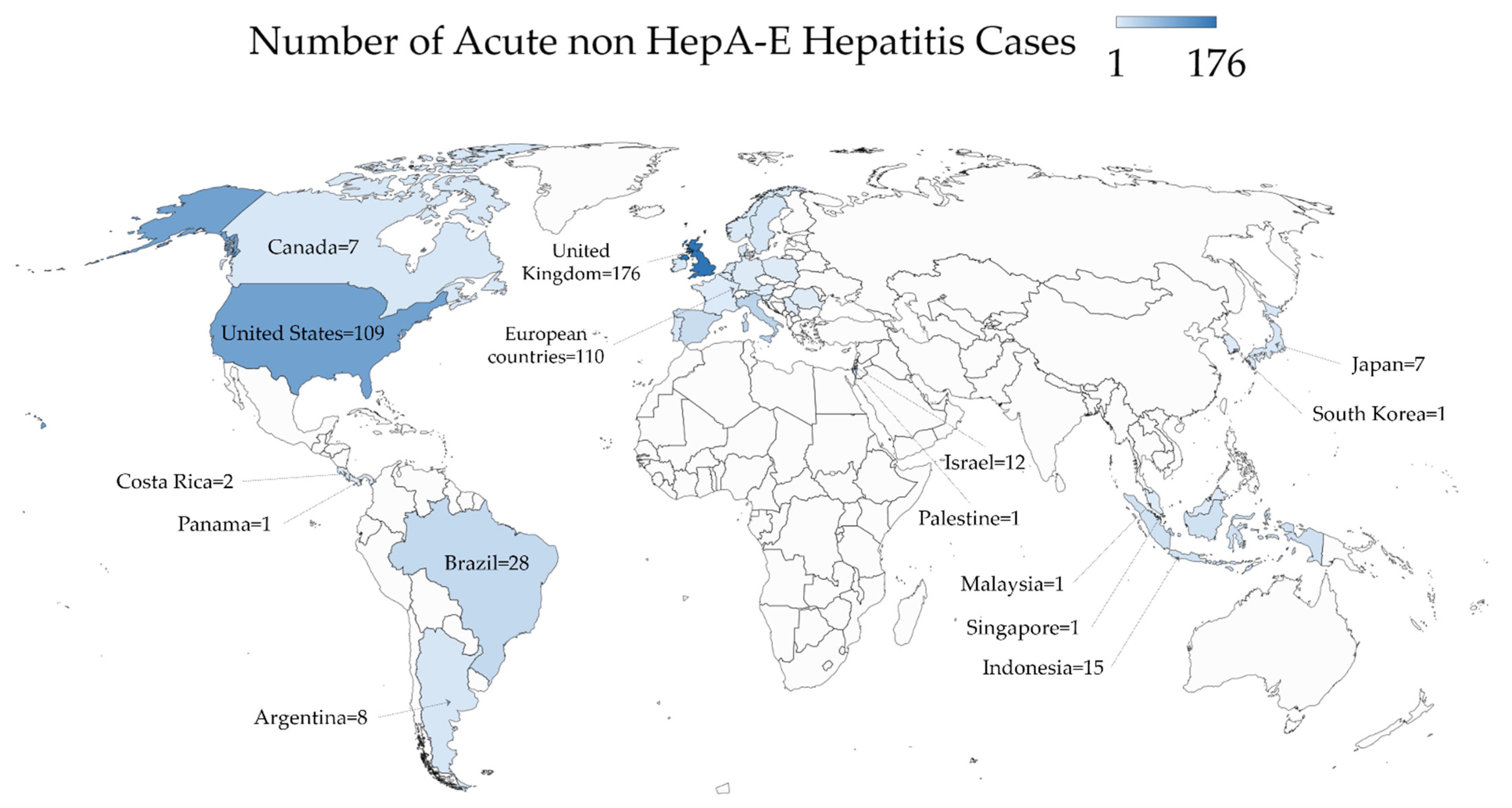
3. Current Geographic Distribution of the Reported Acute Non HepA-E Hepatitis Cases

{kind=link}
{kind=link}
{kind=link}
| Region/Country | Number of Acute Non HepA-E Hepatitis Cases | Notes |
|---|---|---|
| North America | ||
| United States | 109 | Five cases of death were reported. Sources in [11,37] |
| Canada | 7 | Source in [21] |
| Europe * | ||
| United Kingdom | 176 | Source in [22] |
| Italy | 35 | Source in [24] |
| Spain | 22 | Source in [24] |
| Sweden | 9 | Source in [24] |
| Portugal | 8 | Source in [24] |
| Denmark | 6 | Source in [24] |
| Ireland | 6 | Age range was 1–12 year, one died and once received liver transplantation. Source in [12] |
| Netherlands | 6 | Source in [24] |
| Norway | 4 | Source in [24] |
| Belgium | 3 | Source in [24] |
| Austria | 2 | Source in [24] |
| Cyprus | 2 | Source in [24] |
| France | 2 | Source in [24] |
| Germany | 1 | Source in [4] |
| Poland | 1 | Source in [24] |
| Romania | 1 | Source in [24] |
| Serbia | 1 | Source in [24] |
| Slovenia | 1 | Source in [38] |
| Central & South America | ||
| Brazil | 28 | Source in [32] |
| Argentina | 8 | Source in [35] |
| Costa Rica | 2 | Source in [33] |
| Panama | 1 | Source in [34] |
| Asia | ||
| Indonesia | 15 | Three cases of death were reported in children aged 2, 8 and 11. Source in [13] |
| Japan | 7 | |
| Malaysia | 1 | Source in [31] |
| Singapore | 1 | Source in [29] |
| South Korea | 1 | Source in [30] |
| Middle East | ||
| Israel | 12 | Source in [36] |
| Palestine | 1 | One case of death in a child aged 8 years in Gaza. Source in [14] |
4. Clinical Presentation and Severity
5. Hypotheses of Possible Etiology
5.1. Adenovirus Role
5.2. COVID-19
5.3. COVID-19 Vaccination
5.4. Novel Infectious Agent Etiology
5.5. Toxic Agent
5.6. Foodborne Etiology
6. Laboratory Investigation
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HAdV-F41 | Human Adenovirus Group F Serotype 41 |
| ALT | Alanine aminotransferase |
| ASO | Anti-streptolysin O |
| AST | Aspartate aminotransferase |
| CMV | Cytomegalovirus |
| COVID-19 | Coronavirus disease 2019 |
| EBV | Epstein Barr virus |
| ECDC | European Centre for Disease Prevention and Control |
| ESCMID | European Society of Clinical Microbiology and Infectious Diseases |
| ESGVH | ESCMID Study Group for Viral Hepatitis |
| HAV | Hepatitis A virus |
| HBV | Hepatitis B virus |
| HCV | Hepatitis C virus |
| HDV | Hepatitis delta virus |
| HEV | Hepatitis E virus |
| IgM | Immunoglobulin M |
| IU | International unit |
| n | Number |
| PCR | Polymerase chain reaction |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| UK | United Kingdom |
| US | United States |
| WHO | World Health Organization |
References
- Christie, B. Scientists Search for Cause of Hepatitis Cases in Children. BMJ 2022, 377, o982. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Acute Hepatitis of Unknown Aetiology—The United Kingdom of Great Britain and Northern Ireland. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/acute-hepatitis-of-unknown-aetiology---the-united-kingdom-of-great-britain-and-northern-ireland (accessed on 29 April 2022).
- Centers for Disease Control and Prevention (CDC). Recommendations for Adenovirus Testing and Reporting of Children with Acute Hepatitis of Unknown Etiology—Distributed via the CDC Health Alert Network. Available online: https://emergency.cdc.gov/han/2022/han00462.asp (accessed on 28 April 2022).
- European Centre for Disease Prevention and Control. Increase in Severe Acute Hepatitis Cases of Unknown Aetiology in Children—28 April 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/increase-severe-acute-hepatitis-cases-unknown-aetiology-children (accessed on 28 April 2022).
- Marsh, K.; Tayler, R.; Pollock, L.; Roy, K.; Lakha, F.; Ho, A.; Henderson, D.; Divala, T.; Currie, S.; Yirrell, D.; et al. Investigation into Cases of Hepatitis of Unknown Aetiology among Young Children, Scotland, 1 January 2022 to 12 April 2022. Eurosurveillance 2022, 27, 2200318. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Multi-Country—Acute, Severe Hepatitis of Unknown Origin in Children. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON376 (accessed on 28 April 2022).
- Baker, J.M.; Buchfellner, M.; Britt, W.; Sanchez, V.; Potter, J.L.; Ingram, L.A.; Shiau, H.; Sanchez, L.H.G.; Saaybi, S.; Kelly, D.; et al. Acute Hepatitis and Adenovirus Infection Among Children—Alabama, October 2021–February 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 638–640. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. Acute Hepatitis: Technical Briefing. Available online: https://www.gov.uk/government/publications/acute-hepatitis-technical-briefing (accessed on 29 April 2022).
- UK Health Security Agency. Investigation into Acute Hepatitis of Unknown Aetiology in Children in England: Technical Briefing 2. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1073704/acute-hepatitis-technical-briefing-2.pdf (accessed on 29 April 2022).
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Who Press Conference—26 April 2022. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-who-press-conference-26-April-2022 (accessed on 30 April 2022).
- Butler, J.; Parashar, U. Centers for Disease Control and Prevention (CDC). CDC Media Telebriefing: Update on Acute Hepatitis of Unknown Cause. Available online: https://www.cdc.gov/media/releases/2022/a0505-hepatitis.html (accessed on 29 April 2022).
- O’lLeary, K.; Pitts, S. CheshireLive. Child Dies of Acute Hepatitis as Others Hospitalised. Available online: https://www.cheshire-live.co.uk/news/uk-world-news/child-dies-acute-hepatitis-others-23945859 (accessed on 29 April 2022).
- Janti, N. The Jakarta Post. Health Ministry Investigates Mysterious Hepatitis That Killed Three Children in Jakarta. Available online: https://www.thejakartapost.com/indonesia/2022/05/04/health-ministry-investigates-mysterious-hepatitis-that-killed-three-children-in-jakarta.html (accessed on 29 April 2022).
- Xinhua News Agency in, Arabic. A Child Dies of Hepatitis of Unknown Origin in the Gaza Strip. Available online: http://arabic.news.cn/2022-05/04/c_1310582790.htm (accessed on 29 April 2022).
- Davies, J. for Mailonline; Shaheen, M. U.S. Deputy Health Editor for Dailymail.com. Hepatitis Cases in Children May Just Be the ‘Tip of the Iceberg’, UK Expert Claims as Fears over the Mysterious Global Outbreak Which Has Officially Killed One Youngster and Sickened 169 Begin to Grow. Available online: https://www.dailymail.co.uk/health/article-10752181/Hepatitis-numbers-children-just-tip-iceberg-UK-expert-claims.html (accessed on 29 April 2022).
- Ozbay Hoşnut, F.; Canan, O.; Ozçay, F.; Bilezikçi, B. Adenovirus Infection as Possible Cause of Acute Liver Failure in a Healthy Child: A Case Report. Turk. J. Gastroenterol. 2008, 19, 281–283. [Google Scholar] [PubMed]
- Shike, H.; Shimizu, C.; Kanegaye, J.; Foley, J.L.; Burns, J.C. Quantitation of Adenovirus Genome during Acute Infection in Normal Children. Pediatric Infect. Dis. J. 2005, 24, 29–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peled, N.; Nakar, C.; Huberman, H.; Scherf, E.; Samra, Z.; Finkelstein, Y.; Hoffer, V.; Garty, B.Z. Adenovirus Infection in Hospitalized Immunocompetent Children. Clin. Pediatr. 2004, 43, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Kojaoghlanian, T.; Flomenberg, P.; Horwitz, M.S. The Impact of Adenovirus Infection on the Immunocompromised Host. Rev. Med. Virol. 2003, 13, 155–171. [Google Scholar] [CrossRef] [PubMed]
- Koneru, B.; Atchison, R.; Jaffe, R.; Cassavilla, A.; Van Thiel, D.H.; Starzl, T.E. Serological Studies of Adenoviral Hepatitis Following Pediatric Liver Transplantation. Transplant. Proc. 1990, 22, 1547–1548. [Google Scholar] [PubMed]
- Pelley, L. CBC News. 7 Cases of Severe Acute Hepatitis Reported at Toronto Children’s Hospital. Available online: https://www.cbc.ca/news/health/7-cases-of-severe-acute-hepatitis-reported-at-toronto-children-s-hospital-1.6447257 (accessed on 29 April 2022).
- UK Health Security Agency. Increase in Hepatitis (Liver Inflammation) Cases in Children under Investigation. Available online: https://www.gov.uk/government/news/increase-in-hepatitis-liver-inflammation-cases-in-children-under-investigation#full-publication-update-history (accessed on 29 April 2022).
- Public Heath Scotland. Cases of Non A to E Hepatitis. Available online: https://publichealthscotland.scot/news/2022/april/cases-of-non-a-to-e-hepatitis/ (accessed on 29 April 2022).
- European Centre for Disease Prevention and Control. Epidemiological update: Hepatitis of Unknown Aetiology in Children. Epidemiological Update 11 May 2022. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-hepatitis-unknown-aetiology-children (accessed on 29 April 2022).
- Mahase, E. Hepatitis in Children: What’s behind the Outbreaks? BMJ 2022, 377, o1067. [Google Scholar] [CrossRef] [PubMed]
- Otake, T. The Japan Times. Possible Case of Mysterious Acute Child Hepatitis Found in Japan. Available online: https://www.japantimes.co.jp/news/2022/04/25/national/science-health/mysterious-child-hepatitis-japan/ (accessed on 30 April 2022).
- NHK World-Japan. Two More Children in Japan Are Hospitalized with Unidentified Acute Hepatitis. Available online: https://www3.nhk.or.jp/nhkworld/en/news/20220428_40/ (accessed on 29 April 2022).
- Sun, D. The Straits Times. Infant with Acute Hepatitis of Unknown Cause Hospitalised at KKH; MOH Investigating. Available online: https://www.straitstimes.com/singapore/infant-with-acute-hepatitis-of-unknown-cause-warded-at-kkh-moh-investigating (accessed on 30 April 2022).
- Wei, L.D.; Keatinge, C. Bloomberg. Singapore Confirms Case of Acute Hepatitis in 10-Month Old Baby. Available online: https://www.bloomberg.com/news/articles/2022-04-30/singapore-confirms-case-of-acute-hepatitis-in-10-month-old-baby (accessed on 29 April 2022).
- Yonhap News Agency. S. Korea Reports 1st Suspected Case of Acute Child Hepatitis of Unknown Origin. Available online: https://en.yna.co.kr/view/AEN20220510007900320 (accessed on 29 April 2022).
- CodeBlue. Malaysia Suspects Hepatitis Case of Unknown Origin in Sabah Child. Available online: https://codeblue.galencentre.org/2022/05/06/malaysia-suspects-hepatitis-case-of-unknown-origin-in-sabah-child/ (accessed on 29 April 2022).
- Bocchini, B. Agência Brasil. Brasil Tem 28 Casos Suspeitos de Hepatite de Causa Desconhecida. Available online: https://agenciabrasil.ebc.com.br/saude/noticia/2022-05/brasil-tem-28-casos-suspeitos-de-hepatite-de-causa-desconhecida (accessed on 29 April 2022).
- Ministerio de Salud Costa Rica. Salud Investiga Caso de Hepatitis Severa en Niña de Dos Años. Available online: https://www.ministeriodesalud.go.cr/index.php/prensa/52-noticias-2022/1280-salud-investiga-caso-de-hepatitis-severa-en-nina-de-dos-anos?fbclid=IwAR1aGd8p9zPdfNg-o_iCcopPTt-https://www.ministeriodesalud.go.cr/index.php/prensa/52-noticias-2022/1280-salud-investiga-caso-de-hepatitis-severa-en-nina-de-dos-anos?fbclid=IwAR1aGd8p9zPdfNg-o_iCcopPTt-b3byCyNVkiEBMiYVa_bWYlv2h4XhkRiI (accessed on 29 April 2022).
- Ministerio de Salud Costa Rica. Instituto Conmemorativo Gorgas Confirma Caso CSspechoso de Hepatitis Aguda. Available online: https://www.minsa.gob.pa/noticia/instituto-conmemorativo-gorgas-confirma-caso-sospechoso-de-hepatitis-aguda (accessed on 29 April 2022).
- Ministerio de Salud Argentina. Información Relevante del Ministerio de Salud de la Nación Ante Casos Sospechosos de Hepatitis Aguda Grave de Origen Desconocido en Población Pediátrica. Available online: https://www.argentina.gob.ar/noticias/informacion-relevante-del-ministerio-de-salud-de-la-nacion-ante-casos-sospechosos-de (accessed on 29 April 2022).
- Ministry of Health of Israel. The Ministry of Health Informed of 12 Cases of Children with Acute Hepatitis without Clear Background—Press Releases. Available online: https://www.gov.il/en/Departments/news/19042022-01 (accessed on 29 April 2022).
- Hohman, M.; Universal, T.N. Mystery Hepatitis Outbreak in Kids: Which States Are Investigating Cases? Available online: https://www.today.com/health/health/pediatric-hepatitis-america-states-reported-cases-rcna27546 (accessed on 29 April 2022).
- Total Slovenia News. Morning Headlines for Slovenia: Tuesday, 26 April 2022. Available online: https://www.total-slovenia-news.com/news/9924-morning-headlines-for-slovenia (accessed on 30 April 2022).
- Joint ECDC-WHO Regional Office for Europe Hepatitis of Unknown Origin in Children Surveillance, Bulletin. Surveillance summary. Available online: https://cdn.ecdc.europa.eu/novhep-surveillance/ (accessed on 29 April 2022).
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 Nonpharmaceutical Interventions on Influenza and Other Respiratory Viral Infections in New Zealand. Nat. Commun. 2021, 12, 1001. [Google Scholar] [CrossRef] [PubMed]
- de Kleine, R.H.; Lexmond, W.S.; Buescher, G.; Sturm, E.; Kelly, D.; Lohse, A.W.; Lenz, D.; Hørby Jørgensen, M. On Behalf of the Contributors to the Survey. Severe Acute Hepatitis and Acute Liver Failure of Unknown Origin in Children: A Questionnaire-Based Study within 34 Paediatric Liver Centres in 22 European Countries and Israel, April 2022. Eurosurveillance 2022, 27, 2200369. [Google Scholar] [CrossRef] [PubMed]
- Brisca, G.; Mallamaci, M.; Tardini, G.; Martino, L.; Chianucci, B.; Ricci, M.; Buffoni, I.; Romanengo, M. SARS-CoV-2 Infection May Present as Acute Hepatitis in Children. Pediatr. Infect. Dis. J. 2021, 40, e214–e215. [Google Scholar] [CrossRef] [PubMed]
- WHO | World Health Organization. Enhancing Response to Omicron SARS-CoV-2 Variant. Available online: https://www.who.int/publications/m/item/enhancing-readiness-for-omicron-(b.1.1.529)-technical-brief-and-priority-actions-for-member-states (accessed on 29 April 2022).
- Mücke, M.M.; Zeuzem, S. The Recent Outbreak of Acute Severe Hepatitis in Children of Unknown Origin—What Is Known So Far. J. Hepatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-(covid-19)-vaccines (accessed on 29 April 2022).
- Parrish, C.R.; Holmes, E.C.; Morens, D.M.; Park, E.-C.; Burke, D.S.; Calisher, C.H.; Laughlin, C.A.; Saif, L.J.; Daszak, P. Cross-Species Virus Transmission and the Emergence of New Epidemic Diseases. Microbiol. Mol. Biol. Rev. MMBR 2008, 72, 457–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Valdoleiros, S.R.; Cunha, F.; Beeching, N.; di Caro, A.; Petrosillo, N.; Ergonul, O.; Petersen, E. Hepatitis in Children—Could It Be Aflatoxins? Available online: https://www.escmid.org/fileadmin/src/media/PDFs/3Research_Projects/EITaF/EITaf_2022_04_28.pdf (accessed on 29 April 2022).
- Etzel, R.A. Mycotoxins. JAMA 2002, 287, 425–427. [Google Scholar] [CrossRef]
- UK Health Security Agency. Guidance: Increase in Acute Hepatitis Cases of Unknown Aetiology in Children. Available online: https://www.gov.uk/government/publications/hepatitis-increase-in-acute-cases-of-unknown-aetiology-in-children/increase-in-acute-hepatitis-cases-of-unknown-aetiology-in-children (accessed on 29 April 2022).
- Mattner, F.; Sykora, K.W.; Meissner, B.; Heim, A. An Adenovirus Type F41 Outbreak in a Pediatric Bone Marrow Transplant Unit: Analysis of Clinical Impact and Preventive Strategies. Pediatr. Infect. Dis. J. 2008, 27, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Lynch, J.P., 3rd; Kajon, A.E. Adenovirus: Epidemiology, Global Spread of Novel Serotypes, and Advances in Treatment and Prevention. Semin. Respir. Crit. Care Med. 2016, 37, 586–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Source | Case Definition |
|---|---|
| WHO/ECDC | |
| Confirmed acute non HepA-E hepatitis | Not applicable |
| Probable acute non HepA-E hepatitis | The presence of acute hepatitis with elevated level(s) of ALT or AST higher than 500 IU/L, and negativity for viral hepatitis (A–E) in children aged 16 years or younger, since 1 October 2021 |
| Epi-linked acute non HepA-E hepatitis | The presence of acute hepatitis in a person who has been in close contact with a probable case of acute non HepA-E hepatitis, since 1 October 2021 |
| UK Health Security Agency | |
| Confirmed acute non HepA-E hepatitis | The presence of acute hepatitis with elevated level(s) of ALT or AST higher than 500 IU/L, and negativity for viral hepatitis (A–E) in children aged 10 years or less any time from 1 January 2022 |
| Possible acute non HepA-E hepatitis | The presence of acute hepatitis with elevated level(s) of ALT or AST higher than 500 IU/L, and negativity for viral hepatitis (A-E) in those aged between 11 and 16 years any time from 1 January 2022 |
| Epi-linked acute non HepA-E hepatitis | The presence of acute hepatitis in a person who has been in close contact with a probable case of acute non HepA-E hepatitis, any time from 1 January 2022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sallam, M.; Mahafzah, A.; Şahin, G.Ö.; on behalf of ESCMID Study Group for Viral Hepatitis—(ESGVH). Hepatitis of Unknown Origin and Etiology (Acute Non HepA-E Hepatitis) among Children in 2021/2022: Review of the Current Findings. Healthcare 2022, 10, 973. https://doi.org/10.3390/healthcare10060973
Sallam M, Mahafzah A, Şahin GÖ, on behalf of ESCMID Study Group for Viral Hepatitis—(ESGVH). Hepatitis of Unknown Origin and Etiology (Acute Non HepA-E Hepatitis) among Children in 2021/2022: Review of the Current Findings. Healthcare. 2022; 10(6):973. https://doi.org/10.3390/healthcare10060973
Chicago/Turabian StyleSallam, Malik, Azmi Mahafzah, Gülşen Özkaya Şahin, and on behalf of ESCMID Study Group for Viral Hepatitis—(ESGVH). 2022. "Hepatitis of Unknown Origin and Etiology (Acute Non HepA-E Hepatitis) among Children in 2021/2022: Review of the Current Findings" Healthcare 10, no. 6: 973. https://doi.org/10.3390/healthcare10060973