
Association between Walking Habit and Physical Frailty among Community-Dwelling Older Adults


Abstract
:1. Introduction
2. Materials and Methods
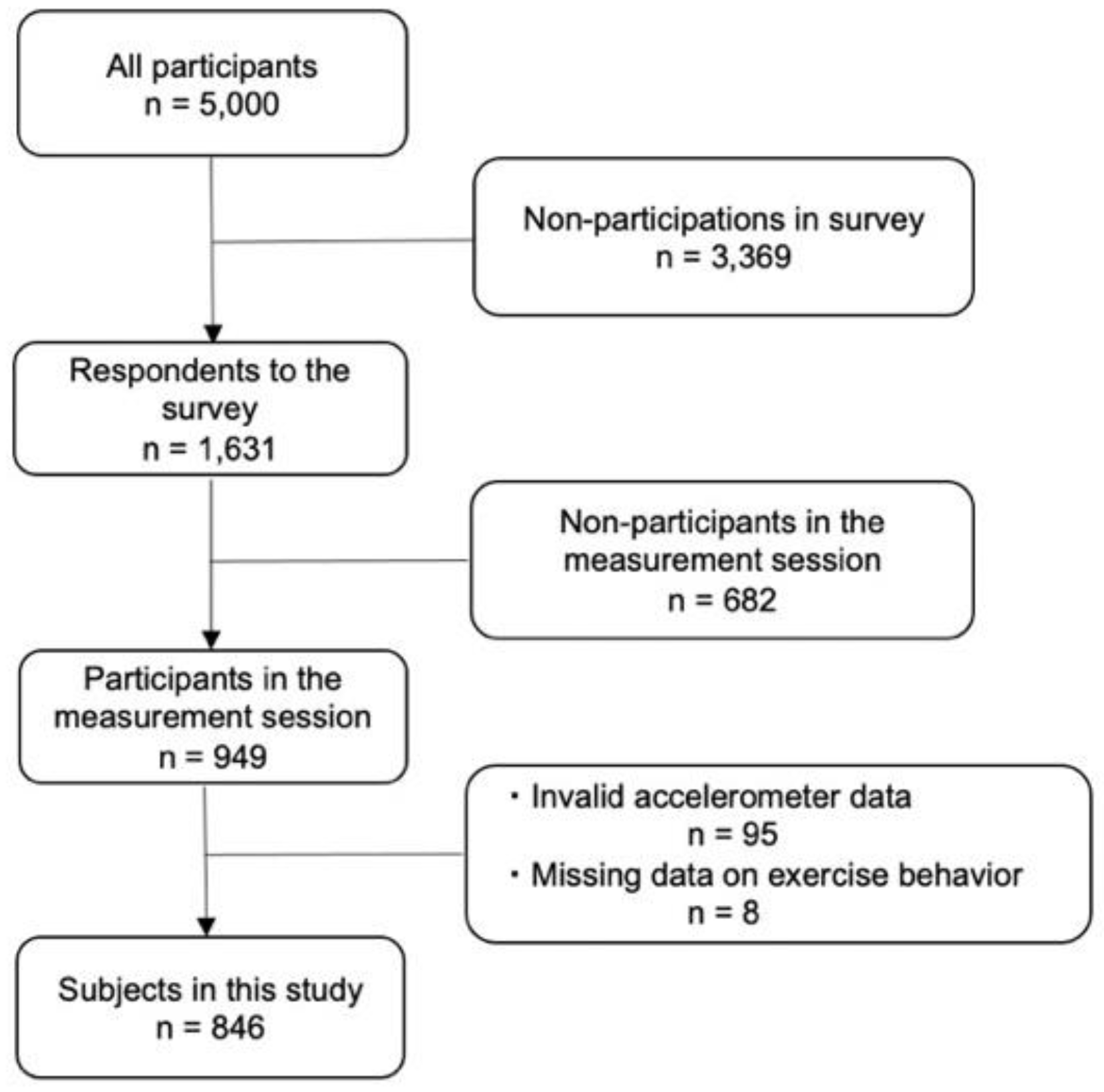
2.1. Study Design and Subjects
2.2. Measures
2.2.1. Physical Frailty
2.2.2. Walking Assessment
2.2.3. Other Assessment
2.2.4. Statistical Analyses
3. Results
3.1. The Caracteristics of Exercise Behavior Groups
3.2. Association between Exericise Behavior and Physical Frailty or Pre-Frailty
3.3. Distribution of Exercise Types Other Than Walking
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabinet Office. Impact of Aging on Social Security Benefits. 2015. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2019/html/zenbun/s1_1_6.html (accessed on 20 May 2021).
- Social Security Council. Future Social Security Reform. 2018. Available online: https://www.mhlw.go.jp/content/12601000/000474989.pdf (accessed on 1 January 2022).
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Iijima, K., VII. Community-dwelling Elderly and Frailty Prevention (Including Oral Frailty). Nihon Naika Gakkai Zasshi 2018, 107, 2469–2477. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Honda, T.; Narazaki, K.; Chen, T.; Kishimoto, H.; Kumagai, S. Physical Frailty and Risk of Needing Long-Term Care in Community-Dwelling Older Adults: A 6-Year Prospective Study in Japan. J. Nutr. Health Aging 2019, 23, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Report of the Study Group on the Revision of Exercise Standards and Guidelines. 2012. Available online: https://www.mhlw.go.jp/stf/shingi/other-kenkou_128596.html (accessed on 1 May 2021).
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.who.int/publications/i/item/9789240015111 (accessed on 10 January 2021).
- Negm, A.M.; Kennedy, C.C.; Thabane, L.; Veroniki, A.-A.; Adachi, J.D.; Richardson, J.; Cameron, I.D.; Giangregorio, A.; Petropoulou, M.; Alsaad, S.M.; et al. Management of Frailty: A Systematic Review and Network Meta-analysis of Randomized Controlled Trials. J. Am. Med Dir. Assoc. 2019, 20, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Russo, A.; Cesari, M.; Pahor, M.; Liperoti, R.; Danese, P.; Bernabei, R.; Onder, G. Walking one hour or more per day prevented mortality among older persons: Results from ilSIRENTE study. Prev. Med. 2008, 47, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, T.; Miyaki, A.; Akazawa, N.; Choi, Y.; Ra, S.-G.; Tanahashi, K.; Kumagai, H.; Oikawa, S.; Maeda, S. Aerobic exercise training increases plasma Klotho levels and reduces arterial stiffness in postmenopausal women. Am. J. Physiol. Circ. Physiol. 2014, 306, H348–H355. [Google Scholar] [CrossRef] [Green Version]
- Yokote, T.; Kishimoto, H. Association between walking exercise and physical function: In community-dwelling older people. Int. J. Phys. Med. Rehabil. 2021, 9, 1–12. [Google Scholar] [CrossRef]
- Chen, S.; Chen, T.; Kishimoto, H.; Susaki, Y.; Kumagai, S. Development of a Fried Frailty Phenotype Questionnaire for Use in Screening Community-Dwelling Older Adults. J. Am. Med. Dir. Assoc. 2019, 21, 272–276. [Google Scholar] [CrossRef]
- Yatsugi, H.; Chen, T.; Chen, S.; Liu, X.; Kishimoto, H. The Associations between Objectively Measured Physical Activity and Physical Function in Community-Dwelling Older Japanese Men and Women. Int. J. Environ. Res. Public Health 2021, 19, 369. [Google Scholar] [CrossRef]
- Chen, S.; Honda, T.; Chen, T.; Narazaki, K.; Haeuchi, Y.; Supartini, A.; Kumagai, S. Screening for frailty phenotype with objectively-measured physical activity in a west Japanese suburban community: Evidence from the Sasaguri Genkimon Study. BMC Geriatr. 2015, 15, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Arai, T.; Kuwabara, K.; Meguro, T.; Watanabe, S.; Fujita, H. The Relationship between Walking Frequency and Physical Function in Community-Dwelling Elderly People. Rigakuryoho Kagaku 2011, 26, 655–659. [Google Scholar] [CrossRef] [Green Version]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Alphen Aan Den Rijn, The Netherlands, 2017; pp. 142–166. [Google Scholar]
- Nose, H. Interval Walking Ttaining for Middle-Aged and Older People: The Effects and the Evidence. J. Jpn. Soc. Stomatognath. Funct. 2012, 19, 1–9. [Google Scholar] [CrossRef]
- Kelly, P.; Williamson, C.; Niven, A.; Hunter, R.; Mutrie, N.; Richards, J. Walking on sunshine: Scoping review of the evidence for walking and mental health. Br. J. Sports Med. 2018, 52, 800–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallgren, M.; Kandola, A.; Stubbs, B.; Nguyen, T.-T.; Wallin, P.; Andersson, G.; Ekblom-Bak, E. Associations of exercise frequency and cardiorespiratory fitness with symptoms of depression and anxiety—A cross-sectional study of 36595 adults. Ment. Health Phys. Act. 2020, 19, 100351. [Google Scholar] [CrossRef]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of Resistance Training Frequency on Gains in Muscular Strength: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef]
- Kemmler, W.; von Stengel, S. Exercise Frequency, Health Risk Factors, and Diseases of the Elderly. Arch. Phys. Med. Rehabil. 2013, 94, 2046–2053. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Lucas, M.; Mekary, R.; Pan, A.; Mirzaei, F.; O’Reilly, É.J.; Willett, W.C.; Koenen, K.; Okereke, O.I.; Ascherio, A. Relation between Clinical Depression Risk and Physical Activity and Time Spent Watching Television in Older Women: A 10-Year Prospective Follow-up Study. Am. J. Epidemiol. 2011, 174, 1017–1027. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-Y.; Yu, C.-P.; Wu, C.-D.; Pan, W.-C. The Effect of Leisure Activity Diversity and Exercise Time on the Prevention of Depression in the Middle-Aged and Elderly Residents of Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nes, B.M.; Janszky, I.; Aspenes, S.T.; Bertheussen, G.F.; Vatten, L.J.; Wisløff, U. Exercise Patterns and Peak Oxygen Uptake in a Healthy Population. Med. Sci. Sports Exerc. 2012, 44, 1881–1889. [Google Scholar] [CrossRef] [Green Version]
- Bennie, J.A.; Teychenne, M.J.; De Cocker, K.; Biddle, S.J. Associations between aerobic and muscle-strengthening exercise with depressive symptom severity among 17839 U.S. adults. Prev. Med. 2019, 121, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Tsujishita, S.; Wakui, T. Impact of a Monthly 3-Month Preventive Exercise Program on the Quality of Life, Ikigai (meaning for life) and Positive Attitudes of Older Women with Different Levels of Life Purpose. Rigakuryoho Kagaku 2021, 36, 337–343. [Google Scholar] [CrossRef]
- Matsumoto, H.; Osaka, H.; Inoue, K.; Park, D.; Hagino, H. Relationship between exercise, self-efficacy for exercise, and grade of frailty in community dwelling older adults—A cross-sectional observation study. Rigakuryohogaku 2019, 46, 429–436. [Google Scholar] [CrossRef]
- McCartney, N.; Hicks, A.L.; Martin, J.; Webber, C.E. Long-term Resistance Training in the Elderly: Effects on Dynamic Strength, Exercise Capacity, Muscle, and Bone. J. Gerontol. Ser. A 1995, 50, B97–B1041. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, E.-J.; Kim, H.-O. Effects of a Physical Exercise Program on Physiological, Psychological, and Physical Function of Older Adults in Rural Areas. Int. J. Environ. Res. Public Health 2021, 18, 8487. [Google Scholar] [CrossRef]


{kind=link}
| Shrinking | Unintentional weight loss > 2–3 kg in the prior 6 months |
| Weakness | Grip strength stratified by gender and BMI (kg/m2) |
| Men | ≤25.00 kg for BMI < 18.5, ≤30.00 kg for 18.5 ≤ BMI < 25, ≤31.50 kg for 25 ≤ BMI < 30, ≤33.00 kg for BMI ≥ 30 |
| Women | ≤17.50 kg for BMI < 18.5, ≤19.50 kg for 18.5 ≤ BMI < 25, ≤20.50 kg for BMI 25 ≤ BMI < 30, ≤19.75 kg for BMI ≥ 30 |
| Exhaustion | Positive answer to either of two self-reported questions. Participants were asked how they felt during the past 30 days: “Did you feel that everything you did was an effort?” and “Did you feel exhausted without any reason?” |
| Slowness | Time of 5 m walk test at one’s maximum waking speed stratified by gender and standing height (gender-specific cutoff: a medium height). |
| Men | Time ≥ 3.56 s for height < 162.0 cm or Time ≥ 3.21 s for height ≥ 162.0 cm |
| Women | Time ≥ 4.25 s for height < 148.7 cm or Time ≥ 3.61 s for height ≥ 148.7 cm |
| Low physical activity | Energy expenditure of physical activity by a triaxial accelerometer; quantified as kilocalories/kg (body weight), stratified by gender. |
| Men | ≤6.20 kcal/kg/day |
| Women | ≤7.13 kcal/kg/day |
| Overall frailty status | Robust: 0 affected component. Pre-frailty: 1–2 affected components. Frailty ≥ 3 affected components. |
| N Group n = 212 (25.1%) | W Group n = 75 (8.9%) | W + O Group n = 204 (24.1%) | O Group n = 355 (42.0%) | |
|---|---|---|---|---|
| Age, y | 70.8 ± 3.1 | 70.9 ± 3.3 | 71.1 ± 3.2 | 70.9 ± 3.0 |
| Men | 95 (44.8) | 34 (45.3) | 101 (49.5) | 169 (20.0) |
| Residential district: | ||||
| Shima | 55 (25.9) | 12 (16.0) | 41 (20.1) | 86 (24.2) |
| Nijo | 57 (26.9) | 23 (30.7) | 51 (25.0) | 91 (25.6) |
| Maebaru | 100 (47.2) | 40 (53.3) | 112 (54.9) | 178 (50.1) |
| BMI, kg/m2 | 23.0 ± 3.3 | 23.0 ± 3.2 | 22.7 ± 2.9 | 22.9 ± 3.2 |
| Presence of disease | 99 (46.7) | 34 (45.3) | 104 (51.0) | 159 (44.8) |
| No. of pain sites | 1.9 ± 2.1 | 1.3 ± 1.6 | 1.4 ± 1.7 * | 1.7 ± 1.8 |
| Education, y | 12.5 ± 2.3 | 12.7 ± 2.2 | 13.3 ± 2.6 * | 13 ± 2.3 |
| ADL score | 10.1 ± 0.6 | 10.1 ± 0.6 | 10.1 ± 0.5 | 10.1 ± 0.3 |
| MMSE score | 27.5 ± 2.2 | 28.3 ± 1.7 * | 28.0 ± 2.1 | 27.8 ± 2.1 |
| Sedentary time (minutes/day) | 440.6 ± 121.2 | 454.5 ± 111.3 | 445.2 ± 102.4 | 445.0 ± 103.9 |
| Moderate and Vigorous physical activity, min/day | 44.6 ± 33.6 | 67.4 ± 33.5 * | 59.4 ± 30.0 * | 50.6 ± 31.0 |
| Light physical activity, min/day | 350.1 ± 96.8 | 339.9 ± 110.3 | 336.1 ± 88.8 | 343.3 ± 90.1 |
| Alcohol consumption, any level | 101 (47.6) | 33 (44.0) | 113 (55.4) | 180 (50.7) |
| Smoking habit, any level | 23 (10.9) | 4 (5.3) | 9 (4.4) | 25 (7.0) |
| Frequency of exercise, ×/week | 0 | 4.8 ± 2.4 | 7.9 ± 4.3 †,§ | 5.0 ± 3.6 |
| Duration of exercise, min/session | 0 | 73.7 ± 57.4 | 91.2 ± 54.5 | 106.3 ± 75.9 †,‡ |
| N Group | W Group | W + O Group | O Group | |
|---|---|---|---|---|
| Physical frailty or pre-frailty, n (%): | 114 (53.8) | 33 (44.0) | 71 (34.8) | 146 (41.1) |
| OR | 1.00 | 0.77 | 0.51 | 0.66 |
| 95%CI | Ref. | 0.44–1.33 | 0.33–0.77 | 0.46–0.94 |
| p-value | – | 0.35 | 0.0014 | 0.02 |
| Components of physical frailty: | ||||
| Shrinking, n (%): | 31 (14.6) | 7 (9.3) | 23 (11.3) | 35 (9.9) |
| OR | 1.00 | 0.63 | 0.84 | 0.67 |
| 95%CI | Ref. | 0.26–1.51 | 0.46–1.53 | 0.40–1.14 |
| p-value | – | 0.29 | 0.57 | 0.14 |
| Exhaustion, n (%): | 45 (21.2) | 8 (10.7) | 13 (6.4) | 40 (11.3) |
| OR | 1.00 | 0.51 | 0.30 | 0.51 |
| 95%CI | Ref. | 0.22–1.19 | 0.15–0.59 | 0.31–0.84 |
| p-value | – | 0.12 | 0.0005 | 0.008 |
| Weakness, n (%): | 40 (18.9) | 14 (18.7) | 31 (15.2) | 62 (17.5) |
| OR | 1.00 | 1.04 | 0.84 | 0.95 |
| 95%CI | Ref. | 0.52–2.10 | 0.49–1.46 | 0.59–1.51 |
| p-value | – | 0.91 | 0.54 | 0.82 |
| Slowness, n (%): | 18 (8.6) | 2 (2.7) | 3 (1.5) | 15 (4.3) |
| OR | 1.00 | 0.37 | 0.2 | 0.47 |
| 95%CI | Ref. | 0.08–1.70 | 0.06–0.71 | 0.22–1.01 |
| p-value | – | 0.20 | 0.01 | 0.054 |
| Low physical activity, n (%): | 29 (13.6) | 6 (8.0) | 16 (7.8) | 41 (11.6) |
| OR | 1.00 | 0.66 | 0.54 | 0.96 |
| 95%CI | Ref. | 0.24–1.78 | 0.26–1.12 | 0.55–1.69 |
| p-value | – | 0.41 | 0.10 | 0.89 |
| N Group | W Group | W + O Group | O Group | |
|---|---|---|---|---|
| Physical frailty or pre-frailty, n (%): | 114 (53.8) | 33 (44.0) | 71 (34.8) | 146 (41.1) |
| OR | 1.00 | 0.85 | 0.54 | 0.67 |
| 95%CI | Ref. | 0.48–1.49 | 0.36–0.83 | 0.47–0.97 |
| p-value | – | 0.57 | 0.005 | 0.03 |
| Components of physical frailty: | ||||
| Shrinking, n (%): | 31 (14.6) | 7 (9.3) | 23 (11.3) | 35 (9.9) |
| OR | 1.00 | 0.58 | 0.81 | 0.66 |
| 95%CI | Ref. | 0.24–1.44 | 0.44–1.48 | 0.39–1.13 |
| p-value | – | 0.24 | 0.48 | 0.13 |
| Exhaustion, n (%): | 45 (21.2) | 8 (10.7) | 13 (6.4) | 40 (11.3) |
| OR | 1.00 | 0.52 | 0.30 | 0.51 |
| 95%CI | Ref. | 0.22–1.23 | 0.15–0.59 | 0.31–0.85 |
| p-value | – | 0.14 | 0.0006 | 0.009 |
| Weakness, n (%): | 40 (18.9) | 14 (18.7) | 31 (15.2) | 62 (17.5) |
| OR | 1.00 | 1.25 | 0.92 | 0.99 |
| 95%CI | Ref. | 0.60–2.58 | 0.52–1.61 | 0.62–1.59 |
| p-value | – | 0.55 | 0.76 | 0.97 |
| Slowness, n (%): | 18 (8.6) | 2 (2.7) | 3 (1.5) | 15 (4.3) |
| OR | 1.00 | 0.55 | 0.28 | 0.54 |
| 95%CI | Ref. | 0.12–2.61 | 0.07–1.02 | 0.25–1.18 |
| p-value | – | 0.45 | 0.053 | 0.12 |
| Low physical activity, n (%): | 29 (13.6) | 6 (8.0) | 16 (7.8) | 41 (11.6) |
| OR | 1.00 | 2.91 | 2.22 | 1.83 |
| 95%CI | Ref. | 0.86–9.90 | 0.86–5.69 | 0.89–3.75 |
| p-value | – | 0.09 | 0.10 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yokote, T.; Yatsugi, H.; Chu, T.; Liu, X.; Kishimoto, H. Association between Walking Habit and Physical Frailty among Community-Dwelling Older Adults. Healthcare 2022, 10, 1396. https://doi.org/10.3390/healthcare10081396
Yokote T, Yatsugi H, Chu T, Liu X, Kishimoto H. Association between Walking Habit and Physical Frailty among Community-Dwelling Older Adults. Healthcare. 2022; 10(8):1396. https://doi.org/10.3390/healthcare10081396
Chicago/Turabian StyleYokote, Tsubasa, Harukaze Yatsugi, Tianshu Chu, Xin Liu, and Hiro Kishimoto. 2022. "Association between Walking Habit and Physical Frailty among Community-Dwelling Older Adults" Healthcare 10, no. 8: 1396. https://doi.org/10.3390/healthcare10081396
APA StyleYokote, T., Yatsugi, H., Chu, T., Liu, X., & Kishimoto, H. (2022). Association between Walking Habit and Physical Frailty among Community-Dwelling Older Adults. Healthcare, 10(8), 1396. https://doi.org/10.3390/healthcare10081396