
The Effects of Pain, Agitation, Delirium, Immobility, and Sleep Disruption Education on Novice Nurses in Adult Intensive Care Units


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Measurements
2.3. The PADIS Education Intervention
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Description of Demographic Characteristics
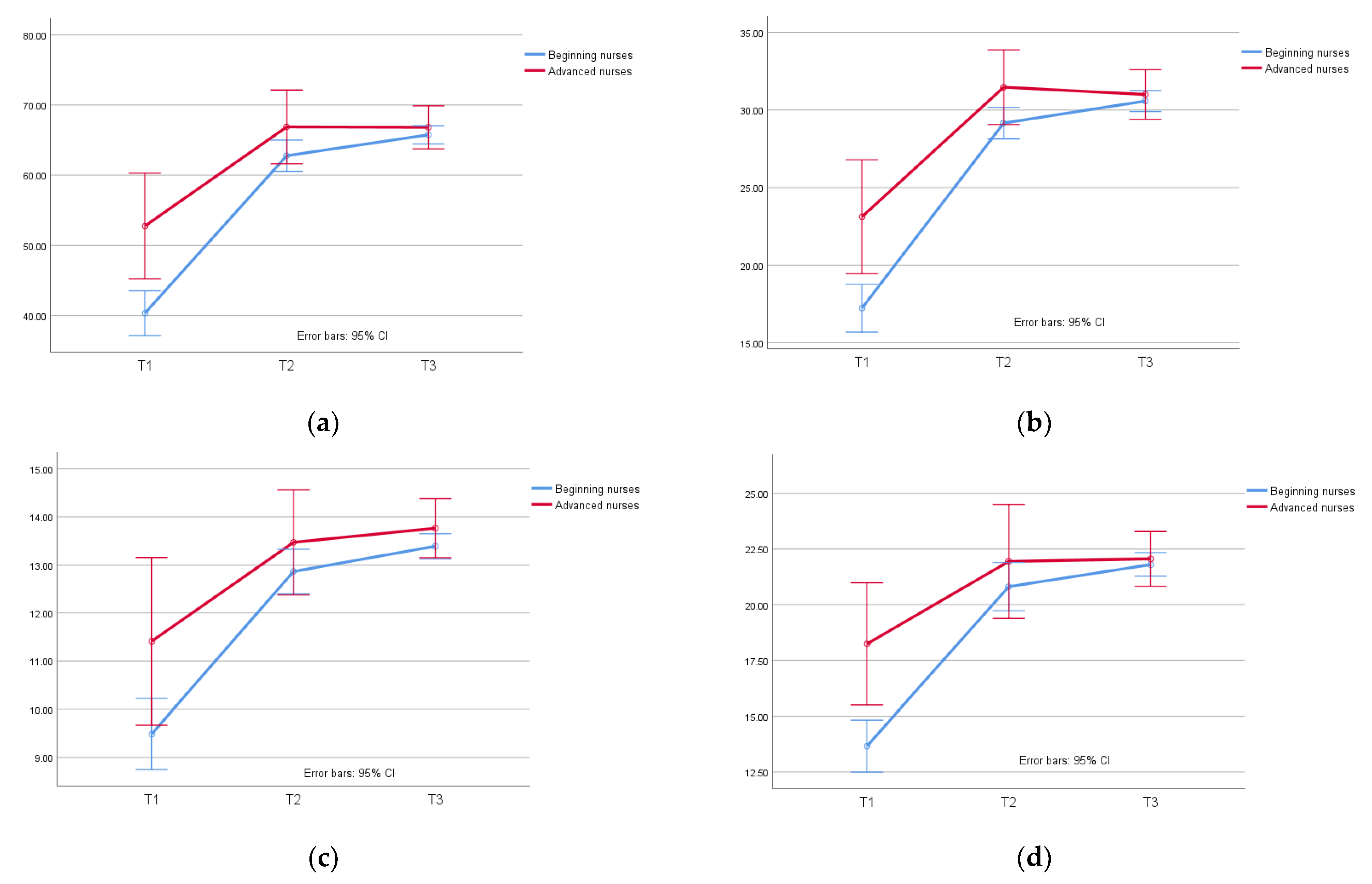
3.2. The Effects of the PADIS Education Program
4. Discussion
4.1. Demographic Characteristics
4.2. The Effects of the PADIS Education Program
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smithburger, P.L.; Patel, M.K. Pharmacologic considerations surrounding sedation, delirium, and sleep in critically Ill adults: A narrative review. J. Pharm. Pract. 2019, 32, 271–291. [Google Scholar] [CrossRef]
- Pandharipande, P.P.; Patel, M.B.; Barr, J. Management of pain, agitation, and delirium in critically ill patients. Pol. Arch. Med. Wewn. 2014, 124, 114–123. [Google Scholar] [CrossRef]
- Rowley-Conwy, G. Critical care nurses’ knowledge and practice of delirium assessment. Br. J. Nurs. 2017, 26, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Alsulami, G.; Marie Rice, A.; Kidd, L. Prospective repeated assessment of self-reported sleep quality and sleep disruptive factors in the intensive care unit: Acceptability of daily assessment of sleep quality. BMJ Open 2019, 9, e029957. [Google Scholar] [CrossRef]
- Wu, C.M.; Lai, F.-C.; Chaou, C.-H.; Tung, H.-H.; Maio, N.-F. An exploration of the pain management knowledge of emergency room staffs and factors of influence. J. Nurs. 2016, 63, 99–109. [Google Scholar] [CrossRef]
- Eskandari, F.; Abdullah, K.L.; Zainal, N.Z.; Wong, L.P. Use of physical restraint: Nurses’ knowledge, attitude, intention and practice and influencing factors. J. Clin. Nurs. 2017, 26, 4479–4488. [Google Scholar] [CrossRef] [PubMed]
- Krugman, M.; Smith, K.; Goode, C.J. A clinical advancement program: Evaluating 10 years of progressive change. J. Nurs. Adm. 2000, 30, 215–225. [Google Scholar] [CrossRef]
- Pierson, M.A.; Liggett, C.; Moore, K.S. Twenty years of experience with a clinical ladder: A tool for professional growth, evidence-based practice, recruitment, and retention. J. Contin. Educ. Nurs. 2010, 41, 33–40. [Google Scholar] [CrossRef]
- Burket, T.L.; Fermlee, M.; Greider, P.J.; Hippensteel, D.M.; Rohrer, E.A.; Shay, M.L. Clinical ladder program evolution: Journey from novice to expert to enhancing outcomes. J. Contin. Educ. Nurs. 2010, 41, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Meucci, J.; McGrath, J. Attributes of a successful clinical ladder program for nurses: An integrative review. Worldviews Evid.-Based Nurs. 2019, 16, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Weng, Y.H.; Chen, C.; Kuo, K.N.; Yang, C.-Y.; Lo, H.-L.; Chen, K.-H.; Chiu, Y.-W. Implementation of evidence-based practice in relation to a clinical nursing ladder system: A national survey in Taiwan. Worldviews Evid.-Based Nurs. 2015, 12, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Chen, F.C.; Kuo, C.H.; Lin, P.C.; Cheng, H.R.; Chiu, Y.-W. The exploration of nurses’ knowledge, attitude, behavior and their influencing factors on N3 case report of the clinical ladder program. Tzu Chi. Med. J. 2004, 3, 60–69. [Google Scholar]
- Messmer, P.R.; Jones, S.G.; Taylor, B.A. Enhancing knowledge and self-confidence of novice nurses: The“ Shadow-A-Nurse” ICU program. Nurs. Educ. Perspect. 2004, 25, 131–136. [Google Scholar] [PubMed]
- Serafin, L.; Pawlak, N.; Strząska-Kliś, Z.; Bobrowska, A.; Czarkowska-Pączek, B. Novice nurses’ readiness to practice in an ICU: A qualitative study. Nurs. Crit. Care 2021, 27, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Santana-Padilla, Y.G.; Santana-Cabrera, L.; Bernat-Adell, M.D.; Linares-Pérez, T.; Alemán-González, J.; Acosta-Rodríguez, R.F. Training needs detected by nurses in an intensive care unit: A phenomenological study. Enferm. Intensiva Engl. Ed. 2019, 30, 181–191. [Google Scholar] [CrossRef]
- Barr, J.; Frazer, G.L.; Puntillo, K.; Ely, E.W.; Gelinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; Kress, J.P.; Joffe, A.M.; et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gelinas, C.; Needham, D.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Khoundabi, B.; Ansari, A.F.; Hashemian, S.M. Impact of PAD guideline on masih daneshvari hospital ICU. Biom. Biostat. Int. J. 2019, 8, 145–149. [Google Scholar] [CrossRef]
- Hermes, C.; Acevedo-Nuevo, M.; Berry, A.; Kjellgren, T.; Negro, A.; Massarotto, P. Gaps in pain, agitation and delirium management in intensive care: Outputs from a nurse workshop. Intensive Crit. Care Nurs. 2018, 48, 52–60. [Google Scholar] [CrossRef]
- Tsang, J.L.; Ross, K.; Miller, F.; Maximous, R.; Yung, P.; Marshall, C.; Camargo, M.; Fleming, D.; Law, M. Qualitative descriptive study to explore nurses’ perceptions and experience on pain, agitation and delirium management in a community intensive care unit. BMJ Open 2019, 9, e024328. [Google Scholar] [CrossRef]
- Benner, P. From novice to expert. Am. J. Nurs. 1982, 82, 402–407. [Google Scholar] [PubMed]
- Guidelines for the Nursing Ladder System Planning of the Clinical Professional Competence for Primary Nursing Staff. Available online: https://www.twna.org.tw/WebPad/WebPad.aspx?1x8jyHnXeNSHfBGHev4mkg%3D%3D (accessed on 12 June 2022).
- Min, A.-R.; Kim, I.S. Relationship of perception of clinical ladder system with professional self-concept and empowerment based on nurses’ clinical career stage. J. Korean Acad. Nurs. Adm. 2013, 19, 254–264. [Google Scholar] [CrossRef]
- Ajri-Khameslou, M.; Najafi, M.; Karimollahi, M. Vigilance in Nurses Working in Intensive Care Units. Open J. Nurs. 2021, 11, 715–727. [Google Scholar] [CrossRef]
- Li, Y.-H.; Chou, M.-C.; Lin, L.-D.; Tsai, C.-C.; Lin, M.-H. Relationships between willingness to participate in the nursing clinical ladder program and its related factors among clinical nurses. Healthcare 2022, 10, 369. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xiao, Q.; Zhang, C.; Jia, Y.; Shi, C. Intensive care unit nurses’ knowledge, attitudes, and perceived barriers regarding early mobilization of patients. Nurs. Crit. Care 2020, 25, 339–345. [Google Scholar] [CrossRef]
- Tan, C.M.; Camargo, M.; Miller, F.; Ross, K.; Maximous, R.; Yung, P.; Marshall, C.; Fleming, D.; Law, M.; Tsang, J.L. Impact of a nurse engagement intervention on pain, agitation and delirium assessment in a community intensive care unit. BMJ Open Qual. 2019, 8, e000421. [Google Scholar] [CrossRef] [PubMed]
- Eskandari, F.; Abdullah, K.L.; Zainal, N.Z.; Wong, L.P. The effect of educational intervention on nurses’ knowledge, attitude, intention, practice and incidence rate of physical restraint use. Nurse Educ. Pract. 2018, 32, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Ramoo, V.; Adu, H.; Rai, V.; Singh, S.K.S.; Baharudin, A.A. Educational intervention on delirium assessment using confusion assessment method-ICU (CAM-ICU) in a general intensive care unit. J. Clin. Nurs. 2018, 27, 4028–4039. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.H.; Hsiao, C.Y.; Ho, T.H.; Chiang, M.C.; Lin, L.W.; Hsu, C.Y.; Lin, S.Y. The effects of continuing education in restraint reduction on novice nurses in intensive care units. J. Nurs. Res. 2004, 12, 246–256. [Google Scholar] [CrossRef]
- Chyan, M.; Chen, Y.-C.; Guo, R.-M.; Lee, Y.-W. The effects of education intervention on nurses’ knowledge, attitude, and behavior of restrains in the intensive care units. Chang. Gung Nurs. 2004, 15, 248–257. (In Chinese) [Google Scholar] [CrossRef]
- Burry, L.; Hutton, B.; Williamson, D.R.; Mehta, S.; Adhikari, N.K.; Cheng, W.; Ely, E.W.; Egerod, I.; Fergusson, D.A.; Rose, L. Pharmacological interventions in the treatment of delirium in critical adults. Cochrane Database Syst. Rev. 2019, 9, CD011749. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Mędrzycka-Dąbrowska, W.; Friganovic, A.; Oomen, B.; Krupa, S. Non-pharmacological nursing interventions preventing delirium in ICU patients—Umbrella review with implications for evidence-based practice. J. Pers. Med. 2022, 12, 760. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Mędrzycka-Dąbrowska, W.; Friganovic, A.; Oomen, B.; Krupa, S. Delirium in patients with critical disease and potential role of thiamine therapy in prevention and treatment: Results of scoping review with implications for evidence-based practice. Int. J. Environ. Res. Public Health 2021, 18, 8809. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Lee, H.-B. Prevention and management of delirium in critically ill adult patients in the intensive care unit: A review based on the 2018 PADIS guidelines. Acute Crit. Care 2019, 34, 117. [Google Scholar] [CrossRef]
- Xu, C.; Chen, Z.; Zhang, L.; Guo, H. Systematic review and meta-analysis on the incidence of delirium in intensive care unit inpatients after cognitive exercise intervention. Ann. Palliat. Med. 2022, 11, 663. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n | % |
|---|---|---|
| Age (M ± SD) | 29.9 ± 8.4 | |
| Gender | ||
| Male | 7 | 6.3 |
| Female | 105 | 93.8 |
| Age | ||
| 20–29 | 74 | 66.1 |
| 30–39 | 20 | 17.9 |
| 40–49 | 13 | 11.6 |
| 50–59 | 5 | 4.5 |
| Marital status | ||
| Single | 95 | 84.8 |
| Married | 17 | 5.2 |
| Education Background | ||
| College | 11 | 9.8 |
| University | 95 | 84.8 |
| Master | 6 | 5.4 |
| ICU working experience | ||
| 0–1year | 19 | 17 |
| 1–2 years | 17 | 15.2 |
| 2–3 years | 11 | 9.8 |
| 3 above | 65 | 58 |
| Clinical Ladder | ||
| N | 15 | 13.4 |
| N1 | 51 | 45.5 |
| N2 | 29 | 25.9 |
| N3 | 16 | 14.3 |
| N4 | 1 | 0.9 |
| Nursing working experience | ||
| 0–1 year | 18 | 16.1 |
| 1–2 years | 15 | 13.4 |
| 2–3 years | 9 | 8.0 |
| 3–5 years | 18 | 16.1 |
| 5 years above | 52 | 46.6 |
| ICU license | ||
| Yes | 82 | 73.2 |
| No | 30 | 26.8 |
| Novice Nurses (n = 95) | Advanced Nurses (n = 17) | t/X2 | p | |
|---|---|---|---|---|
| Variables | n (%) | n (%) | ||
| Age (M ± SD) | 27.66 ± 2.56 | 42.47 ± 3.41 | ||
| Age | 45.35 | 0.00 | ||
| 20–29 | 74 (78) | 0 (0) | ||
| 30–39 | 13 (14) | 7 (41) | ||
| 40–49 | 7 (7) | 6 (35) | ||
| 50–59 | 1 (1) | 4 (24) | ||
| Gender | −1.15 | 0.007 | ||
| Male | 7 (7) | 0 (0) | ||
| Female | 88 (93) | 17 (100) | ||
| Marital status | −9.06 | 0.00 | ||
| Single | 90 (95) | 6 (35) | ||
| Married | 5 (5) | 11 (65) | ||
| Education Background | 6.12 | 0.04 | ||
| College | 10 (11) | 1 (6) | ||
| University | 82 (86) | 13 (76) | ||
| Master | 3 (3) | 3 (18) | ||
| Nursing working experience | 14.48 | 0.00 | ||
| <2 years | 33 (35) | 0 (0) | ||
| 3–5 years | 27 (28) | 0 (0) | ||
| >5 years | 35 (37) | 17 (100) | ||
| ICU working experience | 23.12 | 0.00 | ||
| <3 years | 47 (49) | 0 (0) | ||
| >3 years | 48 (51) | 17 (100) | ||
| ICU license | 2.77 | 0.00 | ||
| Yes | 65 (68) | 17 (100) | ||
| No | 30 (32) | 0 (0) |
| Total (n = 112) | Advanced Nurses (n = 17) | Novice Nurses (n = 95) | p | ||
|---|---|---|---|---|---|
| Times | Variables | (M ± SD) | (M ± SD) | (M ± SD) | |
| T1 | PADIS score | 40.70 ± 16.66 | 52.76 ± 10.33 | 40.33 ± 16.44 | 0.006 |
| Knowledge | 17.3 ± 8.04 | 23.11 ± 5.27 | 17.23 ± 7.95 | 0.013 | |
| Attitudes | 9.48 ± 3.78 | 11.41 ± 2.73 | 9.48 ± 3.75 | 0.11 | |
| Skills | 13.88 ± 6.06 | 18.23 ± 3.57 | 13.62 ± 5.98 | 0.002 | |
| T2 | PADIS Score | 63.54 ± 11.66 | 66.88 ± 8.72 | 62.77 ± 11.28 | 0.64 |
| Knowledge | 29.57 ± 5.30 | 31.47 ± 4.63 | 29.15 ± 5.05 | 0.93 | |
| Attitudes | 12.94 ± 2.38 | 13.47 ± 1.73 | 12.86 ± 2.35 | 0.53 | |
| Skills | 20.97 ± 5.67 | 21.94 ± 3.05 | 20.80 ± 5.62 | 0.55 | |
| T3 | PADIS Score | 65.91 ± 6.34 | 66.82 ± 6.88 | 65.75 ± 6.27 | 0.83 |
| Knowledge | 30.64 ± 3.30 | 31.00 ± 3.74 | 30.57 ± 3.24 | 0.28 | |
| Attitudes | 13.44 ± 1.27 | 13.76 ± 1.39 | 13.38 ± 1.25 | 0.92 | |
| Skills | 21.83 ± 2.53 | 22.05 ± 2.53 | 21.78 ± 2.55 | 0.50 |
| (Novice Nurses–Advanced Nurses) a | SE | t | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| PADIS total score | ||||||
| Pre-test | −12.428 | 4.136 | −3.005 | −20.624 | −4.232 | 0.003 |
| 1st post-test | −4.103 | 2.883 | −1.423 | −9.816 | 1.610 | 0.157 |
| 2nd post-test | −1.066 | 1.676 | −0.636 | −4.388 | 2.257 | 0.526 |
| Knowledge score | ||||||
| Pre-test | −5.886 | 2.008 | −2.931 | −9.865 | −1.907 | 0.004 |
| 1st post-test | −2.313 | 1.316 | −1.757 | −4.922 | 0.296 | 0.082 |
| 2nd post-test | −0.421 | 0.874 | −0.482 | −2.153 | 1.311 | 0.631 |
| Attitude score | ||||||
| Pre-test | −1.928 | 0.954 | −2.020 | −3.818 | −0.037 | 0.046 |
| 1st post-test | −0.607 | 0.600 | −1.012 | −1.797 | 0.582 | 0.314 |
| 2nd post-test | −0.375 | 0.337 | −1.115 | −1.042 | 0.292 | 0.267 |
| Skills score | ||||||
| Pre-test | −4.576 | 1.505 | −3.040 | −7.559 | −1.593 | 0.003 |
| 1st post-test | −1.133 | 1.405 | −0.806 | −3.916 | 1.651 | 0.422 |
| 2nd post-test | −0.261 | 0.675 | −0.387 | −1.598 | 1.076 | 0.700 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-Y.; Liu, C.-Y.; Wu, T.-Y. The Effects of Pain, Agitation, Delirium, Immobility, and Sleep Disruption Education on Novice Nurses in Adult Intensive Care Units. Healthcare 2022, 10, 1538. https://doi.org/10.3390/healthcare10081538
Lee S-Y, Liu C-Y, Wu T-Y. The Effects of Pain, Agitation, Delirium, Immobility, and Sleep Disruption Education on Novice Nurses in Adult Intensive Care Units. Healthcare. 2022; 10(8):1538. https://doi.org/10.3390/healthcare10081538
Chicago/Turabian StyleLee, Szu-Ying, Chieh-Yu Liu, and Te-Yu Wu. 2022. "The Effects of Pain, Agitation, Delirium, Immobility, and Sleep Disruption Education on Novice Nurses in Adult Intensive Care Units" Healthcare 10, no. 8: 1538. https://doi.org/10.3390/healthcare10081538
APA StyleLee, S.-Y., Liu, C.-Y., & Wu, T.-Y. (2022). The Effects of Pain, Agitation, Delirium, Immobility, and Sleep Disruption Education on Novice Nurses in Adult Intensive Care Units. Healthcare, 10(8), 1538. https://doi.org/10.3390/healthcare10081538