
Trends of Medical Service Utilization for Tinnitus: Analysis Using 2010–2018 Health Insurance Review and Assessment Service National Patient Sample Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
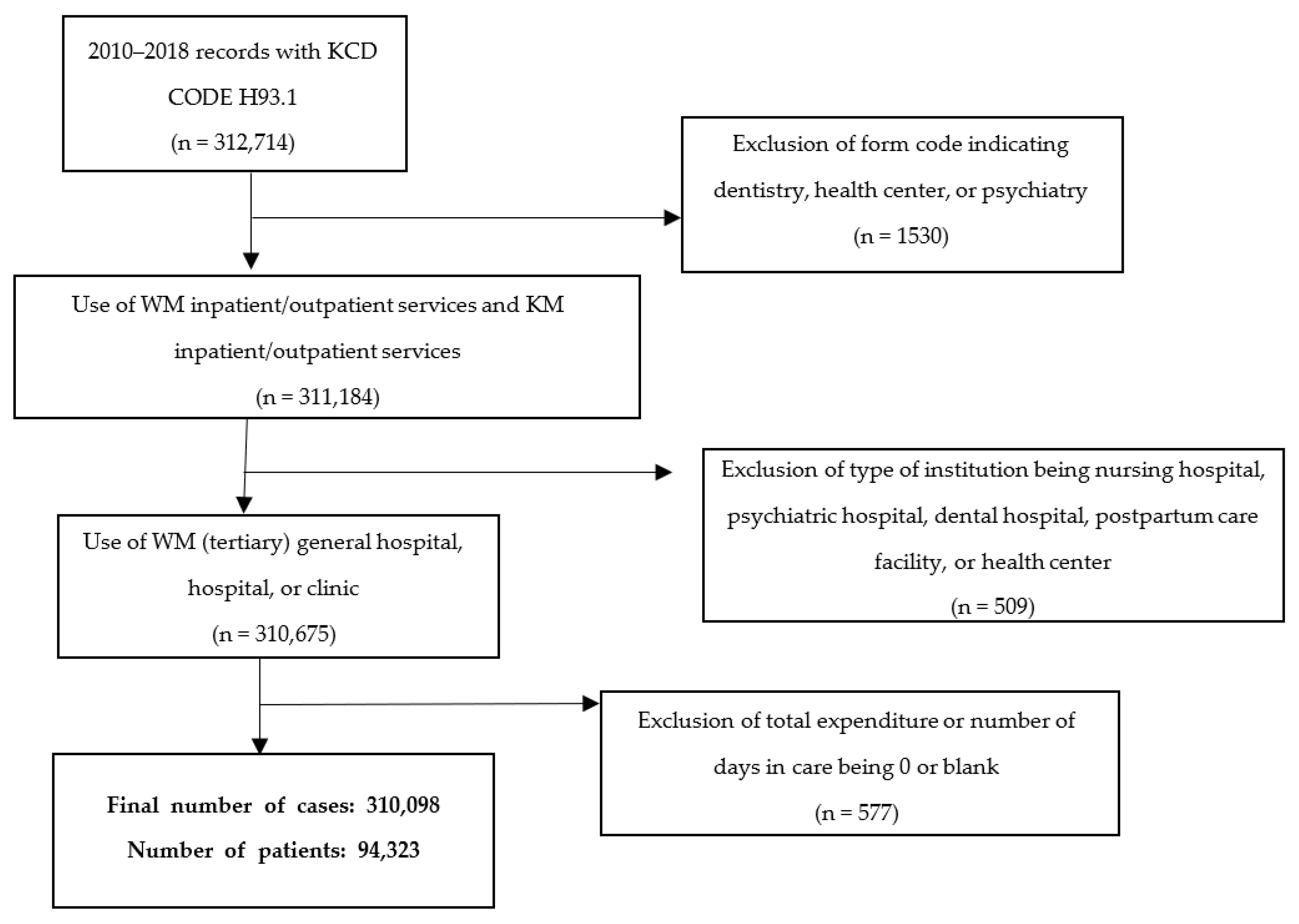
2.2. Study Design and Population
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. General Characteristics of Medical Service Use by Patients with Tinnitus in Korea
3.2. Basic Characteristics of Patients with Tinnitus
3.3. Tinnitus Health Expenditure
3.4. Medication Prescribed for Patients with Tinnitus in Korea
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bauer, C.A. Tinnitus. N. Engl. J. Med. 2018, 378, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Salvi, R.; Elgoyhen, A.B. Emerging pharmacotherapy of tinnitus. Expert Opin. Emerg. Drugs 2009, 14, 687–702. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.M.; Lecluyse, W.; McFerran, D.; Meddis, R. Tinnitus and patterns of hearing loss. J. Assoc. Res. Otolaryngol. 2013, 14, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B. Treatment of tinnitus. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Li, H.; Chen, L. Advances in Understanding, Diagnosis, and Treatment of Tinnitus. Adv. Exp. Med. Biol. 2019, 1130, 109–128. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, H.J.; An, S.Y.; Sim, S.; Park, B.; Kim, S.W.; Lee, J.S.; Hong, S.K.; Choi, H.G. Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS ONE 2015, 10, e0127578. [Google Scholar] [CrossRef]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef]
- Degeest, S.; Corthals, P.; Vinck, B.; Keppler, H. Prevalence and characteristics of tinnitus after leisure noise exposure in young adults. Noise Health 2014, 16, 26–33. [Google Scholar] [CrossRef]
- Nondahl, D.M.; Cruickshanks, K.J.; Huang, G.H.; Klein, B.E.; Klein, R.; Nieto, F.J.; Tweed, T.S. Tinnitus and its risk factors in the Beaver Dam offspring study. Int. J. Audiol. 2011, 50, 313–320. [Google Scholar] [CrossRef]
- Gopinath, B.; McMahon, C.M.; Rochtchina, E.; Karpa, M.J.; Mitchell, P. Risk factors and impacts of incident tinnitus in older adults. Ann. Epidemiol. 2010, 20, 129–135. [Google Scholar] [CrossRef]
- Goldstein, E.; Ho, C.X.; Hanna, R.; Elinger, C.; Yaremchuk, K.L.; Seidman, M.D.; Jesse, M.T. Cost of care for subjective tinnitus in relation to patient satisfaction. Otolaryngol. Head Neck Surg. 2015, 152, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Maes, I.H.; Cima, R.F.; Vlaeyen, J.W.; Anteunis, L.J.; Joore, M.A. Tinnitus: A cost study. Ear Hear. 2013, 34, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Stockdale, D.; McFerran, D.; Brazier, P.; Pritchard, C.; Kay, T.; Dowrick, C.; Hoare, D.J. An economic evaluation of the healthcare cost of tinnitus management in the UK. BMC Health Serv. Res. 2017, 17, 577. [Google Scholar] [CrossRef]
- National_Health_Insurance_Service, Healthcare Bigdata Hub. 2010–2018. Available online: http://opendata.hira.or.kr/op/opc/olap4thDsInfo.do (accessed on 6 April 2021).
- Kramer, F.; Ortigoza, Á. Ginkgo biloba for the treatment of tinnitus. Medwave 2018, 18, e7295. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudian-Sani, M.R.; Hashemzadeh-Chaleshtori, M.; Asadi-Samani, M.; Yang, Q. Ginkgo biloba in the treatment of tinnitus: An updated literature review. Int. Tinnitus J. 2017, 21, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Pichora-Fuller, M.K.; Santaguida, P.; Hammill, A.; Oremus, M.; Westerberg, B.; Ali, U.; Patterson, C.; Raina, P. AHRQ Comparative Effectiveness Reviews. In Evaluation and Treatment of Tinnitus: Comparative Effectiveness; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2013. [Google Scholar]
- Hoekstra, C.E.; Rynja, S.P.; van Zanten, G.A.; Rovers, M.M. Anticonvulsants for tinnitus. Cochrane Database Syst. Rev. 2011, 7, CD007960. [Google Scholar] [CrossRef]
- Hilton, M.P.; Zimmermann, E.F.; Hunt, W.T. Ginkgo biloba for tinnitus. Cochrane Database Syst. Rev. 2013, 3, CD003852. [Google Scholar] [CrossRef]
- Baldo, P.; Doree, C.; Molin, P.; McFerran, D.; Cecco, S. Antidepressants for patients with tinnitus. Cochrane Database Syst. Rev. 2012, 2012, CD003853. [Google Scholar] [CrossRef]
- Korean Medicine Utilization and Awareness by Koreans. Korea Institute for Health and Social Affairs; pp. 1–8. Available online: http://repository.kihasa.re.kr/handle/201002/8383 (accessed on 25 October 2021).
- Schaette, R.; Kempter, R. Development of tinnitus-related neuronal hyperactivity through homeostatic plasticity after hearing loss: A computational model. Eur. J. Neurosci. 2006, 23, 3124–3138. [Google Scholar] [CrossRef]
- Hesser, H.; Weise, C.; Westin, V.Z.; Andersson, G. A systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress. Clin. Psychol. Rev. 2011, 31, 545–553. [Google Scholar] [CrossRef]
- Soleimani, R.; Jalali, M.M.; Hasandokht, T. Therapeutic impact of repetitive transcranial magnetic stimulation (rTMS) on tinnitus: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2016, 273, 1663–1675. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Lee, Y.-R.; Chae, Y.; Park, S.-Y.; Oh, I.-H.; Jang, B.-H. Translation of Korean medicine use to ICD-codes using national health insurance service-national sample cohort. Evid.-Based Complement. Altern. Med. 2016, 2016, 8160838. [Google Scholar] [CrossRef] [PubMed]
- Tunkel, D.E.; Bauer, C.A.; Sun, G.H.; Rosenfeld, R.M.; Chandrasekhar, S.S.; Cunningham, E.R., Jr.; Archer, S.M.; Blakley, B.W.; Carter, J.M.; Granieri, E.C.; et al. Clinical practice guideline: Tinnitus. Otolaryngol. Head Neck Surg. 2014, 151, S1–S40. [Google Scholar] [CrossRef]
- Doi, M.Y.; Tano, S.S.; Schultz, A.R.; Borges, R.; Marchiori, L.L. Effectiveness of acupuncture therapy as treatment for tinnitus: A randomized controlled trial. Braz. J. Otorhinolaryngol. 2016, 82, 458–465. [Google Scholar] [CrossRef]
- Liu, F.; Han, X.; Li, Y.; Yu, S. Acupuncture in the treatment of tinnitus: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2016, 273, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Liang, S.; Chen, L.; Grellet, A. Acupuncture for tinnitus: A systematic review and meta-analysis of randomized controlled trials. Acupunct. Med. 2020, 39, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Health Insurance Review and Assessment Service: Reimbursement Status of Medications Covered by NHIS, 2010–2018. Available online: https://www.hira.or.kr/ (accessed on 10 November 2021).
- Miller, T.R.; Serulle, Y.; Gandhi, D. Arterial Abnormalities Leading to Tinnitus. Neuroimaging Clin. N. Am. 2016, 26, 227–236. [Google Scholar] [CrossRef]
- Johnson, R.M.; Brummett, R.; Schleuning, A. Use of alprazolam for relief of tinnitus. A double-blind study. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 842–845. [Google Scholar] [CrossRef]
- Dobie, R.A. A review of randomized clinical trials in tinnitus. Laryngoscope 1999, 109, 1202–1211. [Google Scholar] [CrossRef]
- Choung, Y.H.; Park, H.J.; Song, J.W.; Ryu, S.J.; Moon, S.K.; Park, K. Treatment effects of glutamate antagonist for tinnitus. Korean J. Otolaryngol.-Head Neck Surg. 2003, 46, 935–939. [Google Scholar]
- Nishad, R.K.; Jain, A.K.; Singh, M.; Verma, R.; Jain, S. Randomised Controlled Clinical Study of Injection Caroverine and Ginkgo Biloba Extract in Cochlear Synaptic Tinnitus. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 1523–1528. [Google Scholar] [CrossRef] [PubMed]
- Radunz, C.L.; Okuyama, C.E.; Branco-Barreiro, F.C.A.; Pereira, R.M.S.; Diniz, S.N. Clinical randomized trial study of hearing aids effectiveness in association with Ginkgo biloba extract (EGb 761) on tinnitus improvement. Braz. J. Otorhinolaryngol. 2020, 86, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.Y.; Kim, T.S.; Moon, I.S.; Park, S.N.; Shin, J.E.; Lee, H.K.; Im, G.J.; Jang, J.H.; Jeon, E.J.; Choi, S.H.; et al. Current Trends in the Treatment of Subjective Tinnitus at University Hospitals in Korea. Korean J. Otorhinolaryngol.-Head Neck Surg. 2013, 56, 266–277. [Google Scholar] [CrossRef]
- Negrila-Mezei, A.; Enache, R.; Sarafoleanu, C. Tinnitus in elderly population: Clinic correlations and impact upon QoL. J. Med. Life 2011, 4, 412–416. [Google Scholar]
- Barozzi, S.; Socci, M.; Ginocchio, D.; Filipponi, E.; Martinazzoli, M.G.; Cesarani, A. Benign paroxysmal positional vertigo and tinnitus. Int. Tinnitus J. 2013, 18, 16–19. [Google Scholar] [CrossRef]
- Kim, S.Y.; Jeon, Y.J.; Lee, J.Y.; Kim, Y.H. Characteristics of tinnitus in adolescents and association with psychoemotional factors. Laryngoscope 2017, 127, 2113–2119. [Google Scholar] [CrossRef]
- Lee, C.C.; Ho, H.C.; Su, Y.C.; Chiu, B.C.; Su, Y.C.; Lee, Y.D.; Chou, P.; Chien, S.H.; Huang, Y.S. Increased risk of vascular events in emergency room patients discharged home with diagnosis of dizziness or vertigo: A 3-year follow-up study. PLoS ONE 2012, 7, e35923. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Year | Type of Visit | Number of Patients | Total Claims | Total Expenditure ($) |
|---|---|---|---|---|
| 2010 | Total | 10,460 | 32,791 | 552,801.32 |
| WM | 8908 | 21,009 | 390,276.54 | |
| KM | 1552 | 11,782 | 162,524.78 | |
| 2011 | Total | 10,720 | 31,816 | 581,596.10 |
| WM | 9293 | 21,964 | 427,641.15 | |
| KM | 1427 | 9852 | 153,954.95 | |
| 2012 | Total | 10,678 | 34,924 | 640,470.20 |
| WM | 9181 | 22,406 | 449,846.96 | |
| KM | 1497 | 12,518 | 190,623.24 | |
| 2013 | Total | 10,255 | 31,723 | 638,507.68 |
| WM | 8813 | 21,290 | 467,390.31 | |
| KM | 1442 | 10,433 | 171,117.37 | |
| 2014 | Total | 10,565 | 34,588 | 750,577.31 |
| WM | 8904 | 21,473 | 516,507.09 | |
| KM | 1661 | 13,115 | 234,070.22 | |
| 2015 | Total | 11,364 | 35,276 | 771,677.49 |
| WM | 9756 | 23,058 | 564,362.78 | |
| KM | 1608 | 12,218 | 207,314.71 | |
| 2016 | Total | 11,218 | 34,728 | 812,234.59 |
| WM | 9695 | 23,428 | 611,270.83 | |
| KM | 1523 | 11,300 | 200,963.76 | |
| 2017 | Total | 11,782 | 36,508 | 937,176.46 |
| WM | 10,093 | 24,020 | 701,422.60 | |
| KM | 1689 | 12,488 | 235,753.86 | |
| 2018 | Total | 11,822 | 37,744 | 1,110,783.95 |
| WM | 10,098 | 23,815 | 819,945.73 | |
| KM | 1724 | 13,929 | 290,838.22 |
| Category | Patient | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (2010–2018) | Only WM (2010–2018) | Only KM (2010–2018) | Both WM and KM (2010–2018) | ||||||
| Total N | Percent | Total N | Percent | Total N | Percent | Total N | Percent | ||
| Total number of patients | 94,323 | 100 | 80,200 | 85.0 | 9582 | 10.2 | 4541 | 4.8 | |
| Age | <15 | 1784 | 1.89 | 1696 | 2.11 | 66 | 0.69 | 22 | 0.48 |
| 15–24 | 5424 | 5.75 | 5061 | 6.31 | 243 | 2.54 | 120 | 2.64 | |
| 25–34 | 6903 | 7.32 | 6128 | 7.64 | 537 | 5.6 | 238 | 5.24 | |
| 35–44 | 10,793 | 11.44 | 9083 | 11.33 | 1163 | 12.14 | 547 | 12.05 | |
| 45–54 | 17,826 | 18.9 | 14,644 | 18.26 | 2117 | 22.09 | 1065 | 23.45 | |
| 55–64 | 21,389 | 22.68 | 17,724 | 22.1 | 2460 | 25.67 | 1205 | 26.54 | |
| 65–74 | 19,426 | 20.6 | 16,477 | 20.54 | 2003 | 20.9 | 946 | 20.83 | |
| 75– | 10,778 | 11.43 | 9387 | 11.7 | 993 | 10.36 | 398 | 8.76 | |
| Gender | Male | 39,495 | 41.87 | 33,659 | 41.97 | 3929 | 41 | 1907 | 42 |
| Female | 54,828 | 58.13 | 46,541 | 58.03 | 5653 | 59 | 2634 | 58 | |
| Payer type * | NHIS | 89,653 | 95.05 | 75,961 | 94.71 | 9289 | 96.94 | 4403 | 96.96 |
| Medicaid | 4326 | 4.59 | 3901 | 4.86 | 293 | 3.06 | 132 | 2.91 | |
| Others | 344 | 0.36 | 338 | 0.42 | - | - | 6 | 0.13 | |
| All | WM | KM | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Expenditure | No. of Claims | Total Expenditure | No. of Claims | Total Expenditure | No. of Claims | |||||||
| Avr. Exp * | Avr. CR * | Avr. No | Avr. CR | Avr. Exp * | Avr. CR * | Avr. Exp * | Avr. CR * | Avr. Exp * | Avr. CR * | Avr. Exp * | Avr. CR * | |
| Injection fee | 124,039 | 7.9 | 40,907 | 4.5 | 3954 | 3.8 | 4115 | 1.3 | 120,084 | 8.0 | 36,792 | 4.9 |
| Consultation fee | 328,971 | 6.1 | 43,619 | 5.9 | 246,793 | 6.0 | 31,055 | 7.2 | 82,178 | 6.2 | 12,563 | 2.9 |
| Testing fee | 249,171 | 12.7 | 23,463 | 7.2 | 249,171 | 12.7 | 23,463 | 7.2 | 1028 | (7.8) | 281 | (5.0) |
| Medication/prescription fee | 8839 | 2.7 | 8720 | 3.2 | 5822 | (5.4) | 6076 | (3.8) | 3016 | 21.3 | 2644 | 24.9 |
| Hospitalization fee | 4439 | 10.5 | 135 | 7.1 | 3703 | 11.2 | 118 | 9.8 | 736 | 13.2 | 17 | (2.7) |
| Treatment fee (surgery, psychotherapy, physical therapy, anesthesia, etc.) | 19,692 | 8.8 | 4449 | 3.6 | 18,664 | 9.8 | 4168 | 4.1 | - | - | - | - |
| Radiology fee | 20,697 | 8.4 | 775 | 2.4 | 20,697 | 8.4 | 775 | 2.4 | - | - | - | - |
| Categories | Total Claims | Average Expenditure per Claim | Average Expenditure per Patient |
|---|---|---|---|
| Blood circulation agents | 127,430 | 3.82 | 11.22 |
| Psychiatric agents | 131,725 | 1.75 | 6.3 |
| Gastrointestinal agents | 88,470 | 2.2 | 5.75 |
| Tinnitus medicine | 22,612 | 3.48 | 7.59 |
| Vertigo medicine | 10,184 | 0.92 | 1.97 |
| Respiratory agents | 15,382 | 0.86 | 1.77 |
| Antipyretic, pain reliever medication | 16,209 | 1.1 | 1.98 |
| Allergy medication | 23,005 | 1.64 | 4.04 |
| Antibacterial agent | 4599 | 4.56 | 7.25 |
| Other drugs | 39,781 | 0.82 | 1.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Min, T.; Yeo, J.; Lee, Y.-S.; Kim, S.-Y.; Lee, D.; Ha, I.-H. Trends of Medical Service Utilization for Tinnitus: Analysis Using 2010–2018 Health Insurance Review and Assessment Service National Patient Sample Data. Healthcare 2022, 10, 1547. https://doi.org/10.3390/healthcare10081547
Min T, Yeo J, Lee Y-S, Kim S-Y, Lee D, Ha I-H. Trends of Medical Service Utilization for Tinnitus: Analysis Using 2010–2018 Health Insurance Review and Assessment Service National Patient Sample Data. Healthcare. 2022; 10(8):1547. https://doi.org/10.3390/healthcare10081547
Chicago/Turabian StyleMin, Taewoon, Jiyoon Yeo, Ye-Seul Lee, Song-Yi Kim, Donghyo Lee, and In-Hyuk Ha. 2022. "Trends of Medical Service Utilization for Tinnitus: Analysis Using 2010–2018 Health Insurance Review and Assessment Service National Patient Sample Data" Healthcare 10, no. 8: 1547. https://doi.org/10.3390/healthcare10081547
APA StyleMin, T., Yeo, J., Lee, Y.-S., Kim, S.-Y., Lee, D., & Ha, I.-H. (2022). Trends of Medical Service Utilization for Tinnitus: Analysis Using 2010–2018 Health Insurance Review and Assessment Service National Patient Sample Data. Healthcare, 10(8), 1547. https://doi.org/10.3390/healthcare10081547