
Behavioral Strengths and Difficulties and Their Associations with Academic Performance in Math among Rural Youth in China

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Outcome Measures
2.3. Family Functioning, Peer Victimization, and the Social Environment
2.4. Statistical Analysis
3. Results
3.1. Summary Statistics
3.2. OLS Regression of Factors Correlated with Student Mental Health
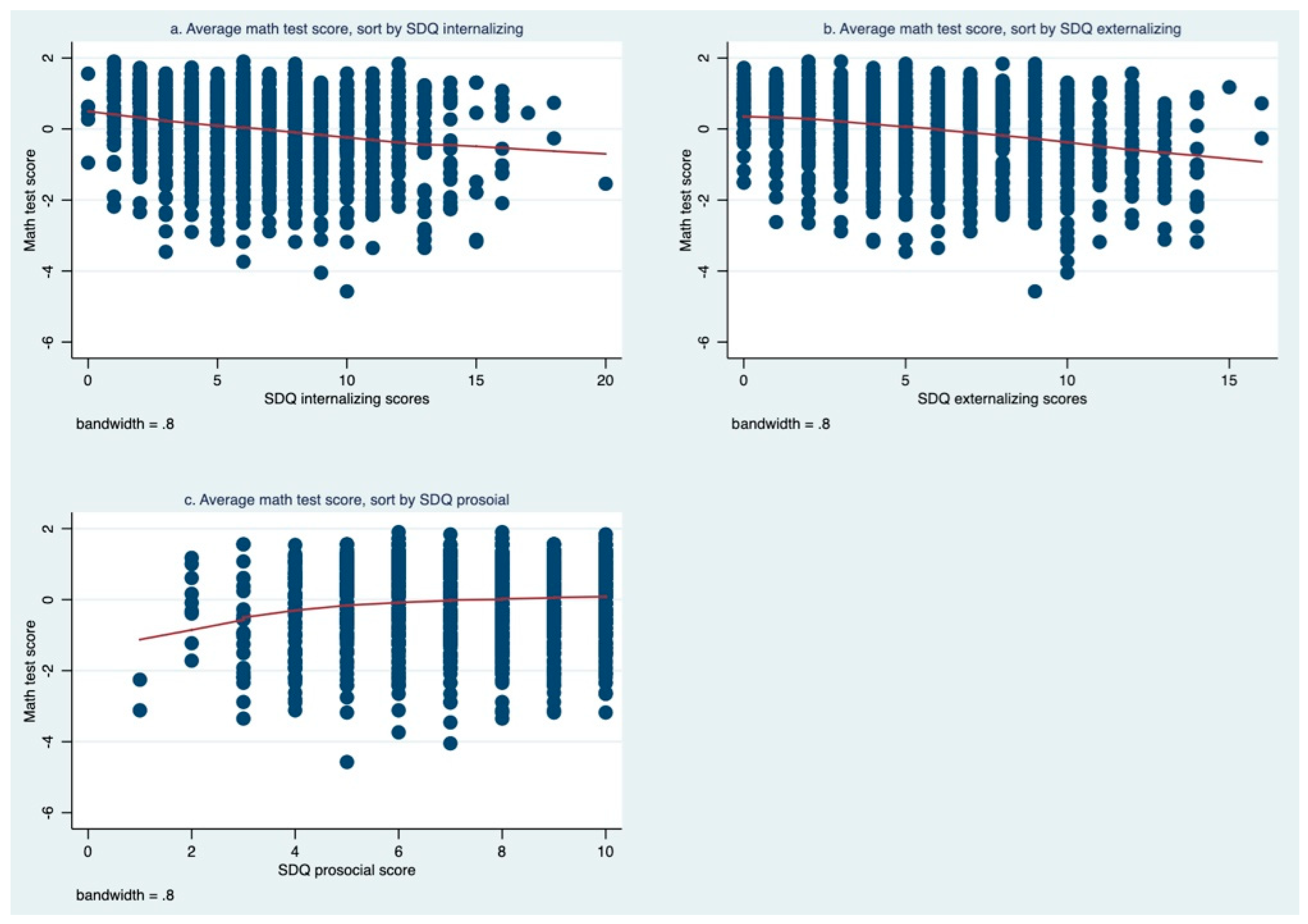
3.3. Association between Student Mental Health and Academic Performance in Math
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Adolescent Mental Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed on 3 December 2021).
- Pedersen, G.A.; Smallegange, E.; Coetzee, A.; Hartog, K.; Turner, J.; Jordans, M.J.D.; Brown, F.L. A Systematic Review of the Evidence for Family and Parenting Interventions in Low- and Middle-Income Countries: Child and Youth Mental Health Outcomes. J. Child Fam. Stud. 2019, 28, 2036–2055. [Google Scholar] [CrossRef]
- Shah, A.; Jenkins, R. Mental health economic studies from developing countries reviewed in the context of those from developed countries. Acta Psychiatr. Scand. 2000, 101, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Klasen, H.; Crombag, A.-C. What works where? A systematic review of child and adolescent mental health interventions for low and middle income countries. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 595–611. [Google Scholar] [CrossRef] [PubMed]
- Omigbodun, O. Developing child mental health services in resource-poor countries. Int. Rev. Psychiatry 2008, 20, 225–235. [Google Scholar] [CrossRef]
- Parchment, T.M.; Small, L.; Osuji, H.; McKay, M.; Bhana, A. Familial and Contextual Influences on Children’s Prosocial Behavior: South African Caregivers as Adult Protective Shields in Enhancing Child Mental Health. Glob. Soc. Welf. 2016, 3, 1–10. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Sankoh, O.; Sevalie, S.; Weston, M. Mental health in Africa. Lancet Glob. Health 2018, 6, e954–e955. [Google Scholar] [CrossRef]
- Desocio, J.; Hootman, J. Children’s Mental Health and School Success. J. Sch. Nurs. 2004, 20, 189–196. [Google Scholar] [CrossRef]
- Duncan, G.J.; Dowsett, C.J.; Claessens, A.; Magnuson, K.; Huston, A.C.; Klebanov, P.; Pagani, L.S.; Feinstein, L.; Engel, M.; Brooks-Gunn, J.; et al. School readiness and later achievement. Dev. Psychol. 2007, 43, 1428. [Google Scholar] [CrossRef]
- Loona, M.I.; Kamal, D.A. Assessment of Disruptive Behaviour Disorder, Academic Performance, and School Social Behaviour of Children. Found. Univ. J. Psychol. 2019, 3, 24–55. [Google Scholar] [CrossRef]
- Zarrella, I.; Lonigro, A.; Perrella, R.; Caviglia, G.; Laghi, F. Social behaviour, socio-cognitive skills and attachment style in school-aged children: What is the relation with academic outcomes? Early Child Dev. Care 2018, 188, 1442–1453. [Google Scholar] [CrossRef]
- Murray, N.G.; Low, B.J.; Hollis, C.; Cross, A.W.; Davis, S.M. Coordinated School Health Programs and Academic Achievement: A Systematic Review of the Literature. J. Sch. Health 2007, 77, 589–600. [Google Scholar] [CrossRef]
- O’Connor, M.; Cloney, D.; Kvalsvig, A.; Goldfeld, S. Positive Mental Health and Academic Achievement in Elementary School: New Evidence From a Matching Analysis. Educ. Res. 2019, 48, 205–216. [Google Scholar] [CrossRef]
- Moilanen, K.L.; Shaw, D.S.; Maxwell, K.L. Developmental cascades: Externalizing, internalizing, and academic competence from middle childhood to early adolescence. Dev. Psychopathol. 2010, 22, 635–653. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Scott, S. Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is Small Beautiful? J. Abnorm. Child Psychol. 1999, 27, 17–24. [Google Scholar] [CrossRef]
- Zelazo, P.D. The Oxford Handbook of Developmental Psychology, Vol. 2: Self and Other; OUP: New York, NY, USA, 2013. [Google Scholar]
- Schonfeld, D.J.; Adams, R.E.; Fredstrom, B.K.; Weissberg, R.P.; Gilman, R.; Voyce, C.; Tomlin, R.; Speese-Linehan, D. Cluster-randomized trial demonstrating impact on academic achievement of elementary social-emotional learning. Sch. Psychol. Q. 2014, 30, 406. [Google Scholar] [CrossRef]
- van Lier, P.A.C.; Vitaro, F.; Barker, E.D.; Brendgen, M.; Tremblay, R.E.; Boivin, M. Peer Victimization, Poor Academic Achievement, and the Link Between Childhood Externalizing and Internalizing Problems. Child Dev. 2012, 83, 1775–1788. [Google Scholar] [CrossRef]
- Cole, D.A.; Martin, J.M.; Powers, B.; Truglio, R. Modeling causal relations between academic and social competence and depression: A multitrait-multimethod longitudinal study of children. J. Abnorm. Psychol. 1996, 105, 258. [Google Scholar] [CrossRef]
- Thornberry, T.P.; Krohn, M.D. Taking Stock of Delinquency: An Overview of Findings from Contemporary Longitudinal Studies; Springer Science & Business Media: New York, NY, USA, 2006. [Google Scholar]
- Kilian, J.M.; Kilian, D.W. A school intervention to increase prosocial behavior and improve academic performance of at-risk students. Improv. Sch. 2011, 14, 65–83. [Google Scholar] [CrossRef]
- Caprara, G.V.; Barbaranelli, C.; Pastorelli, C.; Bandura, A.; Zimbardo, P.G. Prosocial Foundations of Children’s Academic Achievement. Psychol. Sci. 2000, 11, 302–306. [Google Scholar] [CrossRef]
- Kusi-Mensah, K.; Donnir, G.; Wemakor, S.; Owusu-Antwi, R.; Omigbodun, O. Prevalence and patterns of mental disorders among primary school age children in Ghana: Correlates with academic achievement. J. Child Adolesc. Ment. Health 2019, 31, 214–223. [Google Scholar] [CrossRef]
- Yousefi, F.; Redzuan, M.; Mansor, M.B.; Abu Talib, M.; Juhari, R.B. Memory as a Mediator between Depression and Academic Achievement among Iranian Adolescents. Eur. J. Psychol. 2009, 5, 40–51. [Google Scholar] [CrossRef]
- Guzman, M.P.; Jellinek, M.; George, M.; Hartley, M.; Squicciarini, A.M.; Canenguez, K.M.; Kuhlthau, K.A.; Yucel, R.; White, G.W.; Guzman, J.; et al. Mental health matters in elementary school: First-grade screening predicts fourth grade achievement test scores. Eur. Child Adolesc. Psychiatry 2011, 20, 401–411. [Google Scholar] [CrossRef]
- Soomro, N.H.; Clarbour, J. Emotional Behaviour and Academic Achievement in Middle School Children. Pak. J. Soc. Clin. Psychol. 2012, 9, 10–16. [Google Scholar]
- Arnold, D.H.; Doctoroff, G.L. The Early Education of Socioeconomically Disadvantaged Children. Annu. Rev. Psychol. 2003, 54, 517–545. [Google Scholar] [CrossRef]
- Hinshaw, S.P. Externalizing behavior problems and academic underachievement in childhood and adolescence: Causal relationships and underlying mechanisms. Psychol. Bull. 1992, 111, 127–155. [Google Scholar] [CrossRef]
- Barriga, A.Q.; Doran, J.W.; Newell, S.B.; Morrison, E.M.; Barbetti, V.; Robbins, B.D. Relationships Between Problem Behaviors and Academic Achievement in Adolescents: The Unique Role of Attention Problems. J. Emot. Behav. Disord. 2002, 10, 233–240. [Google Scholar] [CrossRef]
- Frick, P.J.; Kamphaus, R.W.; Lahey, B.B.; Loeber, R.; Christ, M.A.G.; Hart, E.L.; Tannenbaum, L.E. Academic underachievement and the disruptive behavior disorders. J. Consult. Clin. Psychol. 1991, 59, 289–294. [Google Scholar] [CrossRef]
- Gustafsson, B.; Li, S. Expenditures on education and health care and poverty in rural China. China Econ. Rev. 2004, 15, 292–301. [Google Scholar] [CrossRef]
- Ma, Z.; Huang, H.; Chen, Q.; Chen, F.; Abdullah, A.S.; Nie, G.; Feng, Q.; Wei, B. Mental Health Services in Rural China: A Qualitative Study of Primary Health Care Providers. BioMed Res. Int. 2015, 2015, 1–6. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. China Statistical Yearbook 2010. 2010. Available online: http://www.stats.gov.cn/tjsj/ndsj/2010/indexeh.htm (accessed on 19 January 2022).
- National Bureau of Statistics of China. China Statistical Yearbook 2018. 2018. Available online: http://www.stats.gov.cn/tjsj/ndsj/2018/indexeh.htm (accessed on 19 January 2022).
- Young, D.J. Rural and urban differences in student achievement in science and mathematics: A multilevel analysis. Sch. Eff. Sch. Improv. 1998, 9, 386–418. [Google Scholar] [CrossRef]
- Zhou, D.; Liu, J.; Liu, J. On the different effects of teacher–student rapport on urban and rural students’ math learning in China: An empirical study. Psychol. Sch. 2021, 58, 268–285. [Google Scholar] [CrossRef]
- Fan, Y.K.; Wu, Z.H. A research report on balanced development of rural and urban education resource in China. Educ. Res. 2014, 11, 32–44. [Google Scholar]
- Cooper, H.; Nye, B.; Charlton, K.; Lindsay, J.; Greathouse, S. The Effects of Summer Vacation on Achievement Test Scores: A Narrative and Meta-Analytic Review. Rev. Educ. Res. 1996, 66, 227–268. [Google Scholar] [CrossRef]
- Gao, Q.; Li, H.; Zou, H.; Cross, W.; Bian, R.; Liu, Y. The mental health of children of migrant workers in Beijing: The protective role of public school attendance. Scand. J. Psychol. 2015, 56, 384–390. [Google Scholar] [CrossRef]
- Wang, J.; Gu, S.; Ye, B.; Gao, J.; Wang, F.; Dai, J.; Fu, H. The effect of migration and the hukou registration system on psychosocial domains and family functioning of children in Shanghai, China. Int. Health 2019, 11 (Suppl. 1), S24–S32. [Google Scholar] [CrossRef]
- Guo, S.; Qu, D. Flourishing of Rural Adolescents in China: A Moderated Mediation Model of Social Capital and Intrinsic Motivation. Int. J. Environ. Res. Public Health 2021, 18, 8158. [Google Scholar] [CrossRef]
- Guo, X.; Lv, B.; Zhou, H.; Liu, C.; Liu, J.; Jiang, K.; Luo, L. Gender Differences in How Family Income and Parental Education Relate to Reading Achievement in China: The Mediating Role of Parental Expectation and Parental Involvement. Front. Psychol. 2018, 9, 783. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Zhao, X.; Ding, X.-X.; Yang, H.-Y.; Qian, Z.-Z.; Feng, F.; Lu, S.-S.; Hu, C.-Y.; Gong, F.-F.; Sun, Y.-H. A prospective study of psychological resilience and depression among left-behind children in China. J. Health Psychol. 2017, 22, 627–636. [Google Scholar] [CrossRef]
- Zhan, M. Assets, parental expectations and involvement, and children’s educational performance. Child. Youth Serv. Rev. 2006, 28, 961–975. [Google Scholar] [CrossRef]
- Wang, H.; Guan, H.; Yi, H.; Seevak, E.; Manheim, R.; Boswell, M.; Rozelle, S.; Kotb, S. Independent reading in rural China’s elementary schools: A mixed-methods analysis. Int. J. Educ. Dev. 2020, 78, 102241. [Google Scholar] [CrossRef]
- Chen, Q.; Chen, Y.; Zhao, Q. Impacts of boarding on primary school students’ mental health outcomes—Instrumental-Variable evidence from rural northwestern China. Econ. Hum. Biol. 2020, 39, 100920. [Google Scholar] [CrossRef]
- Guo, S.; Li, L.; Sun, Y.; Houang, R.; Schmidt, W.H. Does boarding benefit the mathematics achievement of primary and middle school students? Evidence from China. Asia Pac. J. Educ. 2021, 41, 16–38. [Google Scholar] [CrossRef]
- Statistical Report of Economic and Social Development of Pingliang Prefecture. 2019. Available online: http://gansu.gscn.com.cn/system/2020/04/09/012361955.shtml (accessed on 19 January 2022).
- Achenbach, T.M.; Becker, A.; Döpfner, M.; Heiervang, E.; Roessner, V.; Steinhausen, H.-C.; Rothenberger, A. Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: Research findings, applications, and future directions. J. Child Psychol. Psychiatry 2008, 49, 251–275. [Google Scholar] [CrossRef]
- Woerner, W.; Becker, A.; Rothenberger, A. Normative data and scale properties of the German parent SDQ. Eur. Child Adolesc. Psychiatry 2004, 13, ii3–ii10. [Google Scholar] [CrossRef]
- Yang, X.; Jiang, C.; Pan, W.; Xu, W.; Liang, F.; Li, N.; Mu, H.; Na, J.; Lv, M.; An, X.; et al. Prevalence of Psychiatric Disorders among Children and Adolescents in Northeast China. PLoS ONE 2014, 9, e111223. [Google Scholar] [CrossRef]
- Yao, S.; Zhang, C.; Zhu, X.; Jing, X.; McWhinnie, C.M.; Abela, J.R. Measuring adolescent psychopathology: Psychometric properties of the self-report strengths and difficulties questionnaire in a sample of Chinese adolescents. J. Adolesc. Health 2009, 45, 55–62. [Google Scholar] [CrossRef]
- Lai, K.Y.C.; Luk, E.S.L.; Leung, P.W.L.; Wong, A.S.Y.; Law, L.S.-C.; Ho, K. Validation of the Chinese version of the strengths and difficulties questionnaire in Hong Kong. Soc. Psychiat. Epidemiol. 2010, 45, 1179–1186. [Google Scholar] [CrossRef]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. 2001. Available online: https://www.sdqinfo.org/a0.html (accessed on 23 November 2021).
- Goodman, A.; Goodman, R. Strengths and difficulties questionnaire as a dimensional measure of child mental health. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef]
- SDQ, Scoring the Strengths & Difficulties Questionnaire for Age 4–17 or 18+. 2016. Available online: https://www.sdqinfo.org/py/sdqinfo/c0.py (accessed on 24 November 2021).
- Ma, Y.; Fairlie, R.; Loyalka, P.; Rozelle, S. Isolating the ‘Tech’ from EdTech: Experimental Evidence on Computer Assisted Learning in China. National Bureau of Economic Research. 2020. Available online: https://www.nber.org/papers/w26953 (accessed on 24 November 2021).
- Mo, D.; Bai, Y.; Shi, Y.; Abbey, C.; Zhang, L.; Rozelle, S.; Loyalka, P. Institutions, implementation, and program effectiveness: Evidence from a randomized evaluation of computer-assisted learning in rural China. J. Dev. Econ. 2020, 146, 102487. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China, China Statistical Yearbook 2008. 2008. Available online: http://www.stats.gov.cn/tjsj/ndsj/2008/indexeh.htm (accessed on 19 January 2022).
- Cheng, J. A Study on the Relationship between Family Functioning, Personality Traits and Self-Efficacy of Middle School Students, Tianjin Normal University. 2018. Available online: https://cdmd.cnki.com.cn/Article/CDMD-10065-1018266480.htm (accessed on 24 November 2021).
- Tiesel, J.W.; Olson, D.H. Preventing Family Problems: Troubling Trends and Promising Opportunities. Fam. Relat. 1992, 41, 398. [Google Scholar] [CrossRef]
- Kashani, J.H.; Allan, W.D.; Dahlmeier, J.M.; Rezvani, M.; Reid, J.C. An examination of family functioning utilizing the circumplex model in psychiatrically hospitalized children with depression. J. Affect. Disord. 1995, 35, 65–73. [Google Scholar] [CrossRef]
- Phillips, M.R.; West, C.L.; Shen, Q.; Zheng, Y. Comparison of Schizophrenic Patients’ Families and Normal Families in China, Using Chinese Versions of FACES-II and the Family Environment Scales. Fam. Process 1998, 37, 95–106. [Google Scholar] [CrossRef]
- Place, M.; Hulsmeier, J.; Brownrigg, A.; Soulsby, A. The Family Adaptability and Cohesion Evaluation Scale (FACES): An instrument worthy of rehabilitation? Psychiatr. Bull. 2005, 29, 215–218. [Google Scholar] [CrossRef]
- Wang, Y.; Xue, H.; Chen, Q. Effects of family cohesion and adaptability on behavioral problems in preschool children. Zhongguo Dang Dai Er Ke Za Zhi 2016, 18, 421–425. [Google Scholar] [CrossRef]
- Bear, G.; Yang, C.; Harris, A.; Mantz, L.; Hearn, S.; Boyer, D. Technical Manual for the Delaware School Survey: Scales of School Climate; Bullying Victimization; Student Engagement; Positive, Punitive, and Social Emotional Learning Techniques; and Social and Emotional Competencies. 2016. Available online: http://wh1.oet.udel.edu/pbs/wp-content/uploads/2011/12/Delaware-School-Survey-Technical-Manual-Fall-2016.pdf (accessed on 31 May 2019).
- Harris, A.B.; Bear, G.G.; Chen, D.; Lisboa, C.S.D.M.; Holst, B. Perceptions of Bullying Victimization: Differences between Once-Retained and Multiple-Retained Students in Public and Private Schools in Brazil. Child Ind. Res. 2019, 12, 1677–1696. [Google Scholar] [CrossRef]
- Xie, J.; Lv, Y.; Bear, G.; Yang, C.; Marshall, S.; Gong, R. The Validity and Reliability of the Chinese Version of Delaware Bullying Victimization Scale-Student. Chin. J. Clin. Psychol. 2015, 23, 594–596. [Google Scholar] [CrossRef]
- Mullis, I.V.S.; Martin, M.O.; Foy, P.; Drucker, K.T. PIRLS 2011 International Results in Reading. International Association for the Evaluation of Educational Achievement; 2012. Available online: https://eric.ed.gov/?id=ED544362 (accessed on 24 November 2021).
- Ravens-Sieberer, U.; Erhart, M.; Gosch, A.; Wille, N.; European Kidscreen Group. Mental health of children and adolescents in 12 European countries—results from the European KIDSCREEN study. Clin. Psychol. Psychother. 2008, 15, 154–163. [Google Scholar] [CrossRef]
- Hu, H.; Lu, S.; Huang, C.-C. The psychological and behavioral outcomes of migrant and left-behind children in China. Child. Youth Serv. Rev. 2014, 46, 1–10. [Google Scholar] [CrossRef]
- Bourdon, K.H.; Goodman, R.; Rae, D.S.; Simpson, G.; Koretz, D.S. The Strengths and Difficulties Questionnaire: U.S. Normative Data and Psychometric Properties. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Maurice-Stam, H.; Haverman, L.; Splinter, A.; Van Oers, H.A.; Schepers, S.A.; Grootenhuis, M.A. Dutch norms for the Strengths and Difficulties Questionnaire (SDQ)—Parent form for children aged 2–18 years. Health Qual. Life Outcomes 2018, 16, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, A.; Rothenberger, A.; Sohn, A.; The BELLA Study Group. Six years ahead: A longitudinal analysis regarding course and predictive value of the Strengths and Difficulties Questionnaire (SDQ) in children and adolescents. Eur. Child Adolesc. Psychiatry 2015, 24, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.; Parker, P.D.; Del Pozo-Cruz, B.; Noetel, M.; Lonsdale, C. Type of screen time moderates effects on outcomes in 4013 children: Evidence from the Longitudinal Study of Australian Children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 117. [Google Scholar] [CrossRef]
- He, J.-P.; Burstein, M.; Schmitz, A.; Merikangas, K.R. The Strengths and Difficulties Questionnaire (SDQ): The Factor Structure and Scale Validation in U.S. Adolescents. J. Abnorm. Child Psychol. 2013, 41, 583–595. [Google Scholar] [CrossRef]
- Hawes, D.J.; Dadds, M.R. Australian Data and Psychometric Properties of the Strengths and Difficulties Questionnaire. Aust. N. Z. J. Psychiatry 2004, 38, 644–651. [Google Scholar] [CrossRef]
- Wang, F.; Li, Y.; Zhang, S. Study on Relationship Between Learning Achievement and Mental Health Status in Junior School Students. China Public Health 2002, 18, 1121–1122. [Google Scholar]
- Wang, F.; Lin, L.; Xu, M.; Li, L.; Lu, J.; Zhou, X. Mental Health among Left-Behind Children in Rural China in Relation to Parent-Child Communication. Int. J. Environ. Res. Public Health 2019, 16, 1855. [Google Scholar] [CrossRef]
- Wang, F.; Lin, L.; Lu, J.; Cai, J.; Xu, J.; Zhou, X. Mental health and substance use in urban left-behind children in China: A growing problem. Child. Youth Serv. Rev. 2020, 116, 105135. [Google Scholar] [CrossRef]
- Adhikari, R.; Jampaklay, A.; Chamratrithirong, A.; Richter, K.; Pattaravanich, U.; Vapattanawong, P. The Impact of Parental Migration on the Mental Health of Children Left Behind. J. Immigr. Minority Health 2014, 16, 781–789. [Google Scholar] [CrossRef]
- Wang, L.; Mesman, J. Child development in the face of rural-to-urban migration in China: A meta-analytic review. Perspect. Psychol. Sci. 2015, 10, 813–831. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, X.; Ge, X. Left too early: The effects of age at separation from parents on Chinese rural children’s symptoms of anxiety and depression. Am. J. Public Health 2009, 99, 2049–2054. [Google Scholar] [CrossRef]
- Wen, M.; Lin, D. Child development in rural China: Children left behind by their migrant parents and children of nonmigrant families. Child Dev. 2012, 83, 120–136. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Li, L.; Chan, E.Y.Y.; Lau, J.; Griffiths, S.M. Parental migration, self-efficacy and cigarette smoking among rural adolescents in south China. PLoS ONE 2013, 8, e57569. [Google Scholar] [CrossRef]
- Tang, W.; Wang, G.; Hu, T.; Dai, Q.; Xu, J.; Yang, Y.; Xu, J. Mental health and psychosocial problems among Chinese left-behind children: A cross-sectional comparative study. J. Affect. Disord. 2018, 241, 133–141. [Google Scholar] [CrossRef]
- Chen, X.; Li, D.; Liu, J.; Fu, R.; Liu, S. Father Migration and Mother Migration: Different Implications for Social, School, and Psychological Adjustment of Left-Behind Children in Rural China. J. Contemp. China 2019, 28, 849–863. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, D.; Simpkins, S.; Warschauer, M. Does It Matter Which Parent is Absent? Labor Migration, Parenting, and Adolescent Development in China. J. Child Fam. Stud. 2019, 28, 1635–1649. [Google Scholar] [CrossRef]
- Chang, F.; Jiang, Y.; Loyalka, P.; Chu, J.; Shi, Y.; Osborn, A.; Rozelle, S. Parental migration, educational achievement, and mental health of junior high school students in rural China. China Econ. Rev. 2019, 54, 337–349. [Google Scholar] [CrossRef]
- McGill, B.S. Navigating New Norms of Involved Fatherhood: Employment, Fathering Attitudes, and Father Involvement. J. Fam. Issues 2014, 35, 1089–1106. [Google Scholar] [CrossRef]
- Luo, R.; Shi, Y.; Zhang, L.; Liu, C.; Rozelle, S.; Sharbono, B.; Yue, A.; Zhao, Q.; Martorell, R. Nutrition and Educational Performance in Rural China’s Elementary Schools: Results of a Randomized Control Trial in Shaanxi Province. Econ. Dev. Cult. Chang. 2012, 60, 735–772. [Google Scholar] [CrossRef]
- Babic, M.J.; Smith, J.J.; Morgan, P.J.; Eather, N.; Plotnikoff, R.C.; Lubans, D.R. Longitudinal associations between changes in screen-time and mental health outcomes in adolescents. Ment. Health Phys. Act. 2017, 12, 124–131. [Google Scholar] [CrossRef]
- Loewen, O.K.; Maximova, K.; Ekwaru, J.P.; Faught, E.L.; Asbridge, M.; Ohinmaa, A.; Veugelers, P.J. Lifestyle behavior and mental health in early adolescence. Pediatrics 2019, 143, e20183307. [Google Scholar] [CrossRef]
- Männikkö, N.; Ruotsalainen, H.; Miettunen, J.; Marttila-Tornio, K.; Kääriäinen, M. Parental socioeconomic status, adolescents’ screen time and sports participation through externalizing and internalizing characteristics. Heliyon 2020, 6, e03415. [Google Scholar] [CrossRef] [Green Version]
- Zink, J.; Belcher, B.R.; Imm, K.; Leventhal, A.M. The relationship between screen-based sedentary behaviors and symptoms of depression and anxiety in youth: A systematic review of moderating variables. BMC Public Health 2020, 20, 472. [Google Scholar] [CrossRef]
- Eccles, J.S.; Barber, B.L.; Stone, M.; Hunt, J. Extracurricular activities and adolescent development. J. Soc. Issues 2003, 59, 865–889. [Google Scholar] [CrossRef]
- Oberle, E.; Ji, X.R.; Kerai, S.; Guhn, M.; Schonert-Reichl, K.A.; Gadermann, A.M. Screen time and extracurricular activities as risk and protective factors for mental health in adolescence: A population-level study. Prev. Med. 2020, 141, 106291. [Google Scholar] [CrossRef]
- Dashiff, C.; DiMicco, W.; Myers, B.; Sheppard, K. Poverty and adolescent mental health. J. Child Adolesc. Psychiatr. Nurs. 2009, 22, 23–32. [Google Scholar] [CrossRef]
- Aber, J.L.; Jones, S.; Cohen, J. The Impact of Poverty on the Mental health and Development of Very Young Children. In Handbook of Infant Mental Health, 2nd ed.; The Guilford Press: New York, NY, USA, 2000; pp. 113–128. [Google Scholar]
- Duncan, G.J.; Magnuson, K. Socioeconomic status and cognitive functioning: Moving from correlation to causation. Wiley Interdiscip. Rev. Cogn. Sci. 2012, 3, 377–386. [Google Scholar] [CrossRef]
- Reijntjes, A.; Kamphuis, J.H.; Prinzie, P.; Telch, M.J. Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abus. Negl. 2010, 34, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Seeley, K.; Tombari, M.L.; Bennett, L.J.; Dunkle, J.B. Bullying in Schools: An Overview. Juvenile Justice Bulletin. Office of Juvenile Justice and Delinquency Prevention; 2011. Available online: https://eric.ed.gov/?id=ED528252 (accessed on 19 January 2022).
- Chang, F.-C.; Lee, C.-M.; Chiu, C.-H.; Hsi, W.-Y.; Huang, T.-F.; Pan, Y.-C. Relationships among Cyberbullying, School Bullying, and Mental Health in Taiwanese Adolescents. J. Sch. Health 2013, 83, 454–462. [Google Scholar] [CrossRef]
- Benedict, F.T.; Vivier, P.M.; Gjelsvik, A. Mental Health and Bullying in the United States among Children Aged 6 to 17 Years. J. Interpers Violence 2015, 30, 782–795. [Google Scholar] [CrossRef]
- Dwyer, S.B.; Nicholson, J.M.; Battistutta, D. Parent and Teacher Identification of Children at Risk of Developing Internalizing or Externalizing Mental Health Problems: A Comparison of Screening Methods. Prev. Sci. 2006, 7, 343–357. [Google Scholar] [CrossRef] [PubMed]
- Hancock, K.J.; Mitrou, F.; Shipley, M.; Lawrence, D.; Zubrick, S.R. A three generation study of the mental health relationships between grandparents, parents and children. BMC Psychiatry 2013, 13, 299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sisask, M.; Värnik, P.; Värnik, A.; Apter, A.; Balazs, J.; Balint, M.; Bobes, J.; Brunner, R.; Corcoran, P.; Cosman, D.; et al. Teacher satisfaction with school and psychological well-being affects their readiness to help children with mental health problems. Health Educ. J. 2014, 73, 382–393. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Obs. | Mean | Std. Dev. | Min | Max | |
|---|---|---|---|---|---|
| Gender (1 = female) | 1500 | 47.8% | 0.5 | 0 | 1 |
| Age, years | 1500 | 11.468 | 1.646 | 7.917 | 15.5 |
| Over 11 years old (1 = Yes) | 1500 | 51.3% | 0.5 | 0 | 1 |
| Boards at school (1 = Yes) | 1500 | 14.3% | 0.35 | 0 | 1 |
| Parents are divorced (1 = Yes) | 1500 | 7.7% | 0.267 | 0 | 1 |
| Father has passed away (1 = Yes) | 1500 | 1.7% | 0.131 | 0 | 1 |
| Mother has passed away (1 = Yes) | 1500 | 1.1% | 0.103 | 0 | 1 |
| Father’s age, years | 1500 | 40.967 | 6.161 | 26 | 69 |
| Mother’s age, years | 1500 | 37.932 | 5.636 | 21 | 64 |
| Father’s education level (>9-year, 1 = Yes) | 1500 | 23.3% | 0.423 | 0 | 1 |
| Mother’s education level (>9-year, 1 = Yes) | 1500 | 14.3% | 0.35 | 0 | 1 |
| Left-behind child (both out, 1 = Yes) | 1500 | 20.7% | 0.405 | 0 | 1 |
| Migrant father (1 = yes) | 1500 | 54.7% | 0.498 | 0 | 1 |
| Migrant mother (1 = yes) | 1500 | 27.4% | 0.446 | 0 | 1 |
| Standardized values of math raw score | 1500 | −0.01 | 1.039 | −4.573 | 1.902 |
| Balanced family (1 = Yes) | 1500 | 18.4% | |||
| Mid-range family (1 = Yes) | 1500 | 51.8% | |||
| Extreme family (1 = Yes) | 1500 | 29.8% | |||
| Being bullied at school | 1500 | 85.2% | 0.355 | 0 | 1 |
| Being verbally bullied (1 = Yes) | 1500 | 76.6% | 0.424 | 0 | 1 |
| Being physically bullied (1 = Yes) | 1500 | 69% | 0.463 | 0 | 1 |
| Being social-relationally bullied (1 = Yes) | 1500 | 65.3% | 0.476 | 0 | 1 |
| Being cyberbullied (1 = Yes) | 1500 | 28.7% | 0.452 | 0 | 1 |
| Phone time after school (mins) | 1500 | 10.274 | 21.117 | 0 | 300 |
| Daily phone time over 30 min (1 = Yes) | 1500 | 13.5% | 0.342 | 0 | 1 |
| Often attend group activities (1 = Yes) | 1500 | 68.4% | 0.465 | 0 | 1 |
| Obs. | Mean | Std. Dev. | Min | Max | |
|---|---|---|---|---|---|
| SDQ total difficulties score | 1500 | 12.389 | 5.354 | 1 | 34 |
| SDQ internalizing scores | 1500 | 6.619 | 3.232 | 0 | 20 |
| SDQ emotional problems score | 1500 | 3.533 | 2.362 | 0 | 10 |
| SDQ peer problems score | 1500 | 3.085 | 1.64 | 0 | 10 |
| SDQ externalizing scores | 1500 | 5.771 | 3.09 | 0 | 16 |
| SDQ conduct problems score | 1500 | 2.451 | 1.731 | 0 | 9 |
| SDQ hyperactivity score | 1500 | 3.319 | 2.003 | 0 | 10 |
| SDQ prosocial score | 1500 | 7.661 | 1.959 | 1 | 10 |
| Abnormal mental health status, according to SDQ cut-off points | |||||
| Abnormal SDQ total difficulties (1 = Yes) | 1500 | 10.3% | 0.304 | 0 | 1 |
| Abnormal SDQ emotional problems (1 = Yes) | 1500 | 11.5% | 0.319 | 0 | 1 |
| Abnormal SDQ peer problems score (1 = Yes) | 1500 | 9.2% | 0.289 | 0 | 1 |
| Abnormal SDQ conduct problems (1 = Yes) | 1500 | 12.2% | 0.327 | 0 | 1 |
| Abnormal SDQ hyperactivity score (1 = Yes) | 1500 | 6.1% | 0.24 | 0 | 1 |
| Abnormal SDQ prosocial score (1 = Yes) | 1500 | 7.4% | 0.262 | 0 | 1 |
| Variables | SDQ Externalizing Score | SDQ Internalizing Score | SDQ Prosocial Score |
|---|---|---|---|
| (1) | (2) | (3) | |
| Gender, 1 = female, 0 = male | −0.01 | 0.58 *** | 0.41 *** |
| (0.15) | (0.16) | (0.10) | |
| Over 11 years old (1 = Yes) | −0.20 | −0.13 | −0.13 |
| (0.26) | (0.28) | (0.17) | |
| Board at school (1 = Yes) | 0.36 | 0.44 | −0.05 |
| (0.29) | (0.30) | (0.19) | |
| Father has passed away (1 = Yes) | 0.17 | 0.54 | −0.12 |
| (0.59) | (0.62) | (0.39) | |
| Mother has passed away (1 = Yes) | 0.16 | 0.06 | 0.56 |
| (0.74) | (0.78) | (0.49) | |
| Parents are divorced (1 = yes) | 0.33 | 0.77 ** | −0.10 |
| (0.30) | (0.32) | (0.20) | |
| Father’s age, years | 0.04 * | 0.02 | −0.00 |
| (0.02) | (0.02) | (0.01) | |
| Mother’s age, years | 0.01 | −0.00 | −0.00 |
| (0.02) | (0.02) | (0.02) | |
| Father’s education level (>9 years) (1 = Yes) | −0.12 | −0.18 | 0.07 |
| (0.20) | (0.21) | (0.13) | |
| Mother’s education level (>9 years) (1 = Yes) | −0.10 | −0.31 | −0.15 |
| (0.24) | (0.25) | (0.16) | |
| Migrant father (1 = yes) | 0.36 ** | 0.16 | −0.30 *** |
| (0.16) | (0.17) | (0.11) | |
| Migrant mother (1 = yes) | −0.03 | 0.15 | −0.12 |
| (0.19) | (0.20) | (0.13) | |
| Midrange family (1 = Yes) | −0.22 | −0.25 | 0.08 |
| (0.21) | (0.22) | (0.14) | |
| Extreme family (1 = Yes) | −0.26 | −0.20 | 0.24 |
| (0.23) | (0.24) | (0.15) | |
| Being verbally bullied (1 = Yes) | 0.91 *** | 0.61 *** | −0.20 |
| (0.22) | (0.23) | (0.15) | |
| Being physically bullied (1 = Yes) | 0.69 *** | 0.75 *** | 0.02 |
| (0.21) | (0.22) | (0.14) | |
| Being social-relationally bullied (1 = Yes) | 0.24 | 0.67 *** | −0.39 *** |
| (0.21) | (0.22) | (0.14) | |
| Being cyberbullied (1 = Yes) | 1.25 *** | 1.14 *** | −0.26 ** |
| (0.19) | (0.20) | (0.13) | |
| Daily phone time over 30 min (1 = Yes) | 0.89 *** | 0.60 ** | −0.08 |
| (0.23) | (0.24) | (0.15) | |
| Often attend group activities at school (1 = Yes) | −0.53 *** | −0.19 | 0.58 *** |
| (0.17) | (0.18) | (0.11) | |
| Family asset index (1 = bottom 25%) | −0.16 | 0.40 ** | 0.00 |
| (0.18) | (0.19) | (0.12) | |
| Constant | 2.25 *** | 3.92 *** | 8.04 *** |
| (0.82) | (0.86) | (0.55) | |
| Observations | 1500 | 1500 | 1500 |
| R-squared | 0.230 | 0.227 | 0.155 |
| Independent Variables | Standardized Values of Math Test Scores | |||||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| Step 1: Control variables | ||||||
| Gender, 1 = female, 0 = male | −0.13 ** | −0.15 *** | −0.15 *** | −0.12 ** | −0.17 *** | −0.15 *** |
| (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | (0.05) | |
| Over 11 years old (1 = Yes) | −0.22 ** | −0.20 ** | −0.22 ** | −0.21 ** | −0.20 ** | −0.22 ** |
| (0.09) | (0.09) | (0.09) | (0.09) | (0.09) | (0.09) | |
| Left-behind child (1 = Yes) (both parents out) | 0.01 | 0.02 | 0.04 | 0.03 | 0.03 | 0.05 |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | |
| Boarding at school (1 = Yes) | −0.18 * | −0.15 | −0.12 | −0.13 | −0.14 | −0.11 |
| (0.10) | (0.10) | (0.10) | (0.10) | (0.10) | (0.09) | |
| Daily phone time over 30 min (1 = Yes) | −0.18 ** | −0.16 ** | −0.11 | −0.14 * | −0.16 ** | −0.10 |
| (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | |
| Often attends group activities at school (1 = Yes) | 0.24 *** | 0.21 *** | 0.18 *** | 0.20 *** | 0.19 *** | 0.16 *** |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | |
| Father has passed away (1 = Yes) | 0.37 * | 0.35 * | 0.37 * | 0.38 * | 0.36 * | 0.38 ** |
| (0.20) | (0.20) | (0.19) | (0.20) | (0.20) | (0.19) | |
| Mother has passed away (1 = Yes) | 0.02 | 0.10 | 0.11 | 0.11 | 0.08 | 0.09 |
| (0.25) | (0.25) | (0.24) | (0.25) | (0.25) | (0.24) | |
| Parents are divorced (1 = Yes) | −0.05 | −0.04 | −0.03 | −0.01 | −0.04 | −0.01 |
| (0.10) | (0.10) | (0.10) | (0.10) | (0.10) | (0.10) | |
| Father’s age, years | −0.01 | −0.01 | −0.01 | −0.01 | −0.01 | −0.01 |
| (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | |
| Mother’s age, years | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | (0.01) | |
| Father’s education level (>9 years) (1 = Yes) | 0.12 * | 0.10 | 0.09 | 0.09 | 0.09 | 0.08 |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | |
| Mother’s education level (>9 years) (1 = Yes) | 0.17 ** | 0.16 * | 0.15 * | 0.14 * | 0.16 ** | 0.14 * |
| (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | (0.08) | |
| Family asset index, 1 = bottom 25% | −0.05 | −0.05 | −0.06 | −0.03 | −0.05 | −0.05 |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | |
| Step 2: Bullying status | ||||||
| Being verbally bullied (1 = Yes) | 0.09 | 0.15 ** | 0.12 | 0.10 | 0.16 ** | |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | ||
| Being physically bullied (1 = Yes) | −0.10 | −0.05 | −0.06 | −0.10 | −0.04 | |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | ||
| Being social-relationally bullied (1 = Yes) | −0.02 | −0.01 | 0.01 | −0.01 | 0.02 | |
| (0.07) | (0.07) | (0.07) | (0.07) | (0.07) | ||
| Being cyberbullied (1 = Yes) | −0.40 *** | −0.32 *** | −0.35 *** | −0.39 *** | −0.30 *** | |
| (0.06) | (0.06) | (0.06) | (0.06) | (0.06) | ||
| Step 3: SDQ subscales | ||||||
| SDQ externalizing scores | −0.07 *** | −0.05 *** | ||||
| (0.01) | (0.01) | |||||
| SDQ internalizing scores | −0.05 *** | −0.03 *** | ||||
| (0.01) | (0.01) | |||||
| SDQ prosocial score | 0.04 *** | 0.02 * | ||||
| (0.01) | (0.01) | |||||
| Constant | 0.02 | 0.24 | 0.40 | 0.42 | −0.10 | 0.29 |
| (0.27) | (0.27) | (0.27) | (0.27) | (0.29) | (0.29) | |
| Class fixed effect | Yes | Yes | Yes | Yes | Yes | Yes |
| Observations | 1500 | 1500 | 1500 | 1500 | 1500 | 1500 |
| R-squared | 0.201 | 0.231 | 0.260 | 0.247 | 0.237 | 0.266 |
| R-squared change | 0.030 | 0.029 | 0.016 | 0.006 | 0.035 | |
| F-test | 13.513 *** | 53.945 *** | 28.635 *** | 10.562 *** | 22.223 *** | |
| Independent Variables | Standardized Values of Math Test Scores | |||||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| SDQ externalizing scores | −0.06 *** | −0.05 *** | ||||
| (0.01) | (0.01) | |||||
| SDQ internalizing scores | −0.04 *** | −0.03 *** | ||||
| (0.01) | (0.01) | |||||
| Abnormal SDQ externalizing score (Both) (1 = Yes) | −0.67 *** | −0.46 ** | ||||
| (0.18) | (0.18) | |||||
| Abnormal SDQ internalizing score (Both) (1 = Yes) | −0.52 ** | −0.43 ** | ||||
| (0.17) | (0.16) | |||||
| Abnormal SDQ externalizing score (Any) (1 = Yes) | −0.45 *** | −0.35 *** | ||||
| (0.07) | (0.07) | |||||
| Abnormal SDQ internalizing score (Any) (1 = Yes) | −0.31 *** | −0.23 *** | ||||
| (0.07) | (0.07) | |||||
| SDQ prosocial score | 0.03 ** | 0.02 * | ||||
| (0.01) | (0.01) | |||||
| Abnormal SDQ prosocial score (1 = Yes) | −0.44 *** | −0.36 *** | −0.39 *** | −0.33 *** | ||
| (0.10) | (0.10) | (0.10) | (0.10) | |||
| Bulling status controlled | Yes | Yes | Yes | Yes | Yes | Yes |
| Fixed effect in class level | Yes | Yes | Yes | Yes | Yes | Yes |
| Control variables | No | Yes | No | Yes | No | Yes |
| Constant | 0.42 ** | 0.29 | 0.17 | 0.31 | 0.23 | 0.25 |
| (0.21) | (0.29) | (0.17) | (0.27) | (0.16) | (0.27) | |
| Observations | 1500 | 1500 | 1500 | 1500 | 1500 | 1500 |
| R-squared | 0.227 | 0.266 | 0.190 | 0.247 | 0.218 | 0.262 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, W.; Abbey, C.; Qian, Y.; Wang, H.; Rozelle, S.; Singh, M.K. Behavioral Strengths and Difficulties and Their Associations with Academic Performance in Math among Rural Youth in China. Healthcare 2022, 10, 1642. https://doi.org/10.3390/healthcare10091642
Yu W, Abbey C, Qian Y, Wang H, Rozelle S, Singh MK. Behavioral Strengths and Difficulties and Their Associations with Academic Performance in Math among Rural Youth in China. Healthcare. 2022; 10(9):1642. https://doi.org/10.3390/healthcare10091642
Chicago/Turabian StyleYu, Wenjing, Cody Abbey, Yiwei Qian, Huan Wang, Scott Rozelle, and Manpreet K. Singh. 2022. "Behavioral Strengths and Difficulties and Their Associations with Academic Performance in Math among Rural Youth in China" Healthcare 10, no. 9: 1642. https://doi.org/10.3390/healthcare10091642
APA StyleYu, W., Abbey, C., Qian, Y., Wang, H., Rozelle, S., & Singh, M. K. (2022). Behavioral Strengths and Difficulties and Their Associations with Academic Performance in Math among Rural Youth in China. Healthcare, 10(9), 1642. https://doi.org/10.3390/healthcare10091642