1. Introduction
Recently, human life expectancy rapidly increased [
1] An unprecedented number of people are growing older, with a decline in fertility [
2], and the resulting aging has become a global phenomenon [
3]. In 2019, the World Health Organization reported that the number of people aged ≥60 was 1 billion, which will increase to 1.4 billion by 2030 [
4].
Older adults often experience a decline in physical health, such as increased multimorbidity [
5,
6] and decreased instrumental activities of daily living [
7,
8]. These experiences increase their risk and vulnerability to depression; however, depression is not a normal part of aging [
9,
10]. According to the definition of the National Institute of Mental Health [
11], depression (also called major depressive disorder or clinical depression) is a common but serious mood disorder. As the most frequent cause of emotional distress in later life [
12], it affects people’s feelings, thinking, and handling of daily activities [
11]. Furthermore, it has caused more ‘years lost’ to disability than any other disease [
13] and greatly reduces the quality of life of older adults [
12]. With the dramatic increase in the number of older adults, preventing depression in older adults is a great challenge.
The evidence indicated that the risk of depression decreases in both men and women after menopausal age [
14]. Moreover, sex differences peak in adolescence, diminish, and remain stable in later adulthood [
15]. Additionally, exercise stimulates a complex system and leads to higher resilience to stress-related mental disorders, preventing depression [
16]. Economic status [
17] and chronic diseases [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27] are also associated with depression. To prevent depression in older adults, an important method is to lessen loneliness because loneliness is significantly correlated with depression symptoms [
28]. Domènech-Abella et al. (2019) [
29] reported a bidirectional longitudinal association between loneliness and a higher likelihood of major depressive disorder after 2 years in people aged over 50 years. Erzen and Çikrikci conducted a meta-analysis and concluded that loneliness is an important variable affecting depression [
30]. Lee et al. (2021) demonstrated that higher loneliness scores at baseline were significantly associated with depression symptom scores over 12 years after controlling for other social experiences in people aged >50 years [
31].
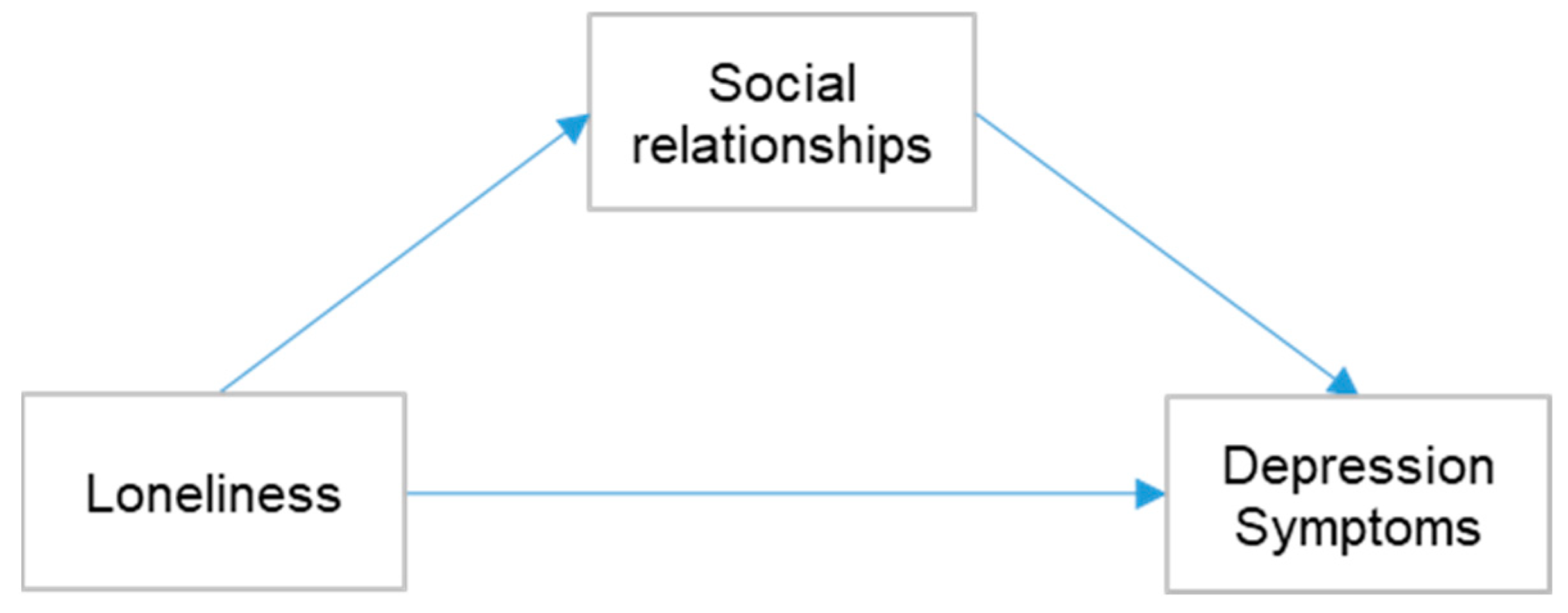
However, after clarifying that lessening loneliness helps to prevent depression in older adults, another question arises: are there other factors contributing to the effects of loneliness on depression? Social relationships have recently been suggested to explain this.
Social relationships are measured by the presence or absence of human relationships in the local community, and the frequency of relationships within one’s environment [
32] was linked to loneliness and depression. Cacioppo and Hawkley(2009) indicated that loneliness can be spread among people and can further reduce their social relationships [
33]. Prince et al. (1997) reported that social support deficits are strongly associated with depression [
34], and Lee et al. (2020) showed that support from friends and romantic partners might lessen depression [
35]. Furthermore, Arslantaş et al. (2015) reported that a lack of hobbies increases loneliness and is associated with depression symptoms [
36]. Seabrook et al. (2016) and Yang et al. (2021) found that positive interactions, social support, and social connections on social networking sites lessen depression and anxiety [
37,
38]. To better understand the role that social relationships play in the association between loneliness and depression, social relationships are studied as a mediator and moderator. Park et al. (2019) used family and friend networks and perceived community support to assess the mediating effects of social engagement on loneliness and depression. [
39] Burholt and Scharf (2014) focused on how social resources (marital status, sociability, religious and other community groups) and social participation (number of activities attended in a month) mediate loneliness and depression [
40]. In addition, Liu et al. (2016) measured the mediating effect of social support on loneliness and depression in 320 older adults using the support of family, friends, and others. [
41]. Zhao et al. (2018) used the same strategy as Liu et al. (2016) to explore the moderating effect of social support on loneliness and depression [
42]. However, social relationships were measured using multifaceted factors, and each aspect has a different focus. For example, social curiosity (social engagement through the internet, newspapers, and books) and interaction (face-to-face socialization with people) are both part of social relationships, but they have completely different emphases. The previous studies only focused on the part of social relationships or treated all aspects as a whole factor, and only general and vague results were provided regarding which part of the social relationship mediates or moderates the effects of loneliness on depression. Furthermore, it remains unknown whether different aspects of social relationships interact with each other regarding the relationship between loneliness and depression.
In the current study, we set two research questions to address this research gap: (1) Are there any relationships between loneliness, social relationships, and depression symptoms? (2) What role do multifaceted social relationships play in the relationship between loneliness and depression symptoms?
3. Results
We described and compared the distribution of demographic characteristics according to depression symptoms (
Table 1).
Depressive symptoms were more frequent in those aged 65–74 years than in those aged ≥75 years (32.9% vs. 31.1%), more frequent in men than in women (32.7% vs. 31.7%), more frequent for those undertaking no exercise than in exercise (36.5% vs. 29.2%), more frequent in no daily alcohol consumption and no daily smoking than in daily alcohol consumption and daily smoking (33.8% vs. 26.7% and 33.2% vs. 25.4%), and more frequent in those who did not have a good economic status than in those with normal and good economic status (44.2% vs. 28.5% vs. 18.5%). In addition, there were statistically significant differences in depressive symptoms depending on economic status, heart disease, respiratory disease, kidney disease, cancer, eye disease, and ear diseases.
The intercorrelations among loneliness, depression symptoms, and social relationships are presented in
Table 2.
The results showed statistically significant differences between any set of two variables, except loneliness and feeling safe. When we focused on depression symptoms as an outcome variable, the results showed a significant correlation between loneliness and depression symptoms, social curiosity and depression symptoms, independence and depression symptoms, interaction and depression symptoms, participation and depression symptoms, and feeling safe and depressive symptoms.
The mediation effect of the multifaceted social relationship between loneliness and depression symptoms is shown in
Table 3.
The direct path of loneliness and depression symptoms was significant in all mediation models (p < 0.01). It is noteworthy that social curiosity and participation acted as mediators between loneliness and depression symptoms, with significant indirect paths for loneliness and social curiosity (B = 0.280, SE = 0.101, and p < 0.01), social curiosity and depression symptoms (B = 0.317, SE = 0.093, and p < 0.01), loneliness and participation (B = 0.195, SE = 0.0070, p < 0.01), and participation and depression symptoms (B = 0.367, SE = 0.134, p < 0.01).
Social curiosity and participation can be mediators between loneliness and depression symptoms. We then tested whether other aspects of social relationships (independence, interaction, feeling safe) could play the role of moderators (
Table 4 and
Table 5).
According to
Table 4, independence (B = −0.375, SE = 0.167, 95% confidence interval [CI] = −0.703, −0.047) and participation (B = −0.241, SE = 0.110, and 95% CI = −0.458, −0.025) played a moderating role in the pre-indirect path, loneliness—social curiosity. In
Table 5, independence (B= −0.256, SE = 0.125, and 95% CI= −0.501, −0.011) played a moderating role in the pre-indirect path of loneliness –participation, and feeling safe (B = 0.515, SE = 0.248, and 95% CI = 0.028, 1.001) played a moderating role in the post-indirect path of participation–depression symptoms. In addition, the results show that interaction can be an individual moderator in the link between loneliness and depression symptoms without any mediator.
Although independence, participation, feeling safe, and interaction may act as moderators, they may have conditional effects. We tested conditional indirect effects and conditional effects of loneliness on depression symptoms at values of multifaceted social relationships (
Table 6).
There was a significant effect when the moderator equaled −1 SD independence (B = 0.112, SE = 0.067, 95% CI = 0.015, 0.274) and when the moderator had equal mean independence (B = 0.060, SE = 0.036, 95% CI = 0.003, 0.145). In addition, a significant effect existed when the moderator equaled −1 SD participation (B = 0.114, SE = 0.064, 95% CI = 0.015–0.260). Furthermore, there was a significant effect when the moderator value was −1 SD independence (B = 0.104, SE = 0.068, 95% CI = 0.006, 0.266) with mean independence (B = 0.055, SE = 0.036, 95% CI = 0.003, 0.140). Similarly, a significant effect was observed when feeling safe was the mean value (B = 0.079, SE = 0.045, 95% CI = 0.012, 0.185) with 1 SD (B = 0.090, SE = 0.049, 95% CI = 0.017, 0.204). In addition, the conditional effects of loneliness on depression symptoms moderated by the interaction were significant when the interaction was −1 SD (B = 1.738, SE = 0.314, 95% CI = 1.112, 2.354) with mean (B = 1.283, SE = 0.218, 95% CI = 0.856, 1.710), and 1 SD (B = 1.122, SE = 0.229, 95% CI = 0.673, 1.571).
4. Discussion
The ISI measures five aspects of social relationships (independence, social curiosity, interaction, participation, and feeling safe). The current study aimed to determine the role that multifaceted social relationships play in the association between loneliness and depression symptoms. According to the statistical evidence, loneliness affected depressive symptoms through social curiosity and participation. In addition, in the model of loneliness–social curiosity–depression symptoms, independence and participation moderated the effect of loneliness–social curiosity. Moreover, in the model of loneliness–participation–depression symptoms, independence and feeling safe moderated the effect of loneliness–participation and participation–depressive symptoms, respectively.
Although no temporal changes can be derived, we confirmed the results of previous studies, where age and sex did not significantly affect depressive symptoms at older ages [
14,
15]. Moreover, as in previous studies [
17], economic status was significantly associated with depression symptoms. Additionally, we found that the risk of depression symptoms in older adults gradually decreases as their economic status improves. This suggests that economic and material affluence is beneficial in lessening the mental stress of older adults. Therefore, improving the economic status is an effective way of improving quality of life and preventing depression symptoms. Furthermore, in a comparison with previous studies [
18,
19,
20,
21,
22,
23,
24,
25,
26,
27], the current study also found that participants with heart, respiratory, kidney, cancer, eye, and ear disorders showed significant differences in depression symptoms compared with those who did not have these diseases. We did not find any statistical evidence for other diseases and exercise affecting depression symptoms. However, this does not mean that there is no association between them. More evidence is required in the future. Future studies are required to explain why the long duration of the disease increases a patient’s stress, whereas these diseases exhibit the same pathological mechanisms as depression symptoms. Therefore, chronic diseases should be investigated further.
As in previous studies [
28,
29,
30,
31], loneliness was significantly correlated with depression symptoms. Compared with previous studies [
34,
35,
36,
37,
38], we found a correlation between various aspects of social relationships (social curiosity, independence, interaction, participation, and feeling safe) and depression symptoms. This may be explained by the fact that satisfying social relationships are essential for good mental and physical health [
53,
54]. The lack of enriching social relationships causes depression in lonely people.
In the mediation analysis, statistical evidence suggested that social relationships can mediate the relationships between loneliness and depression symptoms. Previous studies showed social resources and participation [
40,
41] mediates relationships between loneliness and depression symptoms. Besides this evidence, we also found that social curiosity and participation may play a mediating role in this process. A potential mechanism may be that people may be motivated to seek information (from newspapers, books, magazines, and the internet) when they feel lonely [
55,
56], which, in turn, promotes exploratory acts and affects depression symptoms [
57]. Social curiosity and participation as significant mediators between loneliness and depression symptoms should be emphasized in geriatric medicine. Meanwhile, the results of the present study showed that independence, interaction, and feeling safe did not play a mediating role; however, the statistical results suggested a significant direct association with depression symptoms. Thus, a comprehensive improvement in the social relationships of older adults is an effective way to prevent depressive symptoms.
The moderated mediation model found a more complex interaction effect among multifaceted social relationships, loneliness, and depression symptoms, while previous studies only found that social support could moderate the relationships between loneliness and depression symptoms [
42]. While social curiosity mediates the effect of loneliness on depression symptoms, independence and participation moderated the effect of loneliness on social curiosity, which changed the whole model’s effect. The same situation occurred in the model with participation as a mediator, independence moderated the effect of loneliness on participation, and feeling safe moderated the effect of participation on depression symptoms. In addition, the interaction could directly moderate the effect of loneliness on depression symptoms. However, social relationships cannot be moderators without limitations in this process. In the model of loneliness–social–curiosity–depression symptoms, independence and participation had a moderating effect only when the value was −1 standard deviation of the mean and when b was −1 standard deviation. Similarly, in the loneliness–participation–depression symptoms model, the moderating effect disappeared when the independence over its mean and feeling safe was lower than its mean. Interaction could act as a moderator in all ranges of values. When preventing depression symptoms in older adults, improving social curiosity and participation while conditionally supporting other social relationships will have a more significant effect.
We performed moderated mediation analysis to test the role of multifaceted social relationships in the association between loneliness and depression symptoms. These results prove the existence of complex interaction effects and provide new insights for the prevention of depression in older adults.
However, our study has some limitations. First, it was a cross-sectional study. We could only identify correlations between social relationships, loneliness, and depression symptoms, but not causal associations. Second, we considered many covariables, which caused a high rate of missing data. Future longitudinal studies with a higher data quality are needed to overcome these limitations.


 ,
, 


{kind=link}
{kind=link}