
Trend of Admissions Due to Chronic Lower Respiratory Diseases: An Ecological Study
Department of Respiratory Care, College of Applied Medical Sciences, King Faisal University, Al-Ahsa 31982, Saudi Arabia
Healthcare 2023, 11(1), 65; https://doi.org/10.3390/healthcare11010065
Submission received: 16 November 2022
/
Revised: 19 December 2022
/
Accepted: 22 December 2022
/
Published: 26 December 2022
Abstract
:Objective: This study aimed to examine the trend of hospital admissions related to chronic lower respiratory diseases in England and Wales between 1999 and 2020. Method: This ecological analysis used data that were made accessible to the public and were taken from the Patient Episode Database for Wales (PEDW) and the Hospital Episode Statistics (HES) databases in England for the time span between April 1999 and April 2020. The patients were grouped into four age groups: under 15, 15–59, 60–74, and 75 years and above. Results: In 2020, there were 432,193 chronic lower respiratory disease hospital admissions, which increased from 239,606 in 1999. The hospital admission rate increased by 57.5% (from 459.54 (95% CI 457.71–461.38) in 1999 to 723.70 (95% CI 721.55–725.85) in 2020 per 100,000 people, p < 0.5). The majority of hospital admissions for chronic lower respiratory diseases were found to be directly linked to age (more prevalent in the 75+ age group). Moreover, female hospital admission rates for chronic lower respiratory diseases grew by 85.2% between 1999 and 2020, increasing from 445.45 (95% CI 442.92–447.97) to 824.96 (95% CI 821.73–828.19) per 100,000 people. Conclusion: The rate of hospital admissions due to chronic lower respiratory diseases has sharply increased during the past two decades. COPD was the most common cause for chronic lower respiratory disease admissions. Ageing was also found to be a factor in increased hospital admissions. Future studies are warranted to identify other risk factors of hospital admissions due to chronic lower respiratory diseases and specifically COPD.
1. Introduction
Respiratory diseases are disorders of the lungs and other respiratory system structures [1]. Infections, smoking, second-hand smoke, asbestos, radon, and other types of air pollution can all lead to respiratory diseases [1]. In the United Kingdom (UK), lung diseases affect one in five persons. Additionally, lung diseases contribute to more than 6 million inpatient bed days, 45,833 new diagnoses per month, and more than 700,000 hospital admissions per year in the UK [2]. The respiratory system can be impacted by a wide range of problems, including chronic diseases and infectious diseases.
As described by the International Classification of Diseases 10th Revision (ICD-10), chronic lower respiratory diseases include eight chronic diseases: bronchiectasis, other chronic obstructive pulmonary diseases, simple and mucopurulent chronic bronchitis, emphysema, status asthmatics, bronchitis, not specified as acute or chronic, asthma, and unspecified chronic bronchitis [3]. The social determinants of health and health behaviours, such as obesity, cigarette smoking, exposure to occupational agents, physical inactivity, exposure to allergens, outdoor air pollution, and unhealthy diet, are the most universally recognised, significant modifiable risk factors for chronic lower respiratory diseases [4]. Chronic lower respiratory diseases are a significant cause of morbidity and mortality, ranking as the fourth leading cause of death globally [5,6]. Chronic lower respiratory diseases were the third leading cause of mortality in the UK in 2019 and were responsible for 5.9% of all deaths (31,221) [7]. The primary cause of chronic lower respiratory disease mortality and morbidity is the episodic worsening of respiratory symptoms or the exacerbations of chronic lower respiratory disorders [8].
The severe exacerbations that call for hospitalisation or a referral to the emergency department (ED) account for more than 50% of the costs related to chronic lower respiratory diseases [9]. Chronic lower respiratory diseases, which accounted for 26.4% of all hospital admissions for respiratory diseases in England and Wales, were the second most common reason for these admissions [10]. Understanding hospitalisation patterns for chronic lower respiratory diseases might help physicians treat patients more effectively, which reduces the number of hospital admissions associated with these diseases. Despite the intensive research that has recently been conducted in the UK by Naser and his colleagues, who examined the epidemiology of multiple acute and chronic health conditions [11,12,13,14,15], there is no previous research that examined the epidemiology of admissions related to chronic lower respiratory diseases. A recent study by Naser et al. examined the epidemiology of respiratory disease admissions in general but did not focus on hospital admissions related to chronic lower respiratory diseases [10]. This study aimed to examine the trend of hospital admissions related to chronic lower respiratory diseases in England and Wales between 1999 and 2020.
2. Methods
2.1. Study Sources and the Population
This ecological analysis used data from the Patient Episode Database for Wales (PEDW) and the Hospital Episode Statistics (HES) databases in England for the time span between April 1999 and April 2020. Hospital admission information for patients with chronic lower respiratory diseases from all age groups is available in the HES and PEDW databases. These two medical databases were previously used to examine the admission trends for different health conditions [16,17,18,19,20,21,22,23,24]. The patients in these two medical databases are grouped into four age groups: those under 15 years, those between 15 and 59 years old, those between 60 and 74 years old, and those 75 years of age and older. Using the ICD-10, 5th Edition (the classification system used by the National Health Service (NHS) to define diseases and other health problems), we were able to identify hospital admissions associated with chronic lower respiratory diseases. Chronic lower respiratory diseases (J40–J47) were used in this study.
2.2. Statistical Analysis
SPSS version 25 was used for all analyses (IBM Corp, Armonk, NY, USA). Using the finalised consultant episodes of hospitalisation due to chronic lower respiratory diseases divided by the mid-year population, hospital admission rates with 95% confidence intervals (CIs) were determined. To compare the variations in hospital admission rates between 1999 and 2020, we performed the chi-squared test.
3. Results
In 2020, there were 432,193 chronic lower respiratory disease hospital admissions, which increased from 239,606 in 1999. The hospital admission rate increased by 57.5% (from 459.54 (95% CI 457.71–461.38) in 1999 to 723.70 (95% CI 721.55–725.85) in 2020 per 100,000 people, p < 0.5).
Other chronic obstructive pulmonary diseases (“chronic obstructive pulmonary disease with (acute) lower respiratory infection and chronic obstructive pulmonary disease with (acute) exacerbation”) and asthma accounted for 62.3% and 26.7%, respectively, of all hospital admissions for chronic lower respiratory diseases (Table 1).
A 2.87-fold increase in the rate of hospital admissions for chronic lower respiratory diseases was observed in bronchiectasis over the duration of the study. Additionally, hospital admission rates for chronic lower respiratory diseases in the categories of other chronic obstructive pulmonary diseases, asthma, and bronchitis not classified as acute or chronic increased by 65.5%, 46.1%, and 45.2%, respectively. However, hospital admission rates for unspecified chronic bronchitis, simple and mucopurulent chronic bronchitis, status asthmaticus, and emphysema were reduced by 68.2%, 41.8%, 41.3%, and 7.8%, respectively (Figure 1, Table 2).
The age group of 75 years and above accounted for 33.8% of the total number of hospital admissions for chronic lower respiratory diseases, followed by the age group of 60 to 74 years, with 32.8%, the age group of 15 to 59 years with 24.6%, and the age group of below 15 years with 8.8%.
Hospital admission rates due to chronic lower respiratory diseases dropped by 34.0% for patients under the age of 15 (from 330.24 (95%CI 326.67–333.82) in 1999 to 218.01 (95%CI 215.22–220.80) per 100,000 people) between 1999 and 2020. By contrast, the rate of hospital admissions among patients aged 15 to 59 years increased by 80.1% from 181.77 (95%CI 180.28–183.26) in 1999 to 327.28 (95%CI 325.38–329.19) in 2020. Moreover, in patients aged 60 to 74 years, the rate of hospital admission for chronic lower respiratory diseases increased by 34.5% (from 1136.62 (95%CI 1128.74–1144.51) in 1999 to 1528.94 (95%CI 1521.08–1536.81) in 2020 per 100,000 people). Hospital admission rates for individuals 75 years of age and older who had chronic lower respiratory diseases increased by 60.6% (from 1812.51 (95%CI 1799.29–1825.72) in 1999 to 2911.64 (95%CI 2897.15–2926.13) in 2020 per 100,000 people) (Figure 2).
During the study period, England and Wales reported a total of 6,817,120 hospital admission episodes for chronic lower respiratory diseases. Females accounted for 3,688,092 hospital admission episodes, or 54.1% of all hospital admissions related to chronic lower respiratory diseases, at a mean rate of 175,623 per year. Female hospital admission rates for chronic lower respiratory diseases grew by 85.2% between 1999 and 2020, increasing from 445.45 (95% CI 442.92–447.97) to 824.96 (95% CI 821.73–828.19) per 100,000 people. Male hospital admission rates for chronic lower respiratory diseases increased by 30.7% (from 474.31 (95% CI 471.64–476.98) in 1999 to 620.15 (95% CI 617.32–622.98) in 2020 per 100,000 people) (Figure 3).
3.1. Chronic Lower Respiratory Disease Admission Rate by Gender
The majority of chronic lower respiratory diseases, such as bronchitis that was not classified as acute or chronic, other chronic obstructive lung diseases, asthma, status asthmaticus, and bronchiectasis, had higher hospital admission rates in females than in males (Supplementary Material S1). However, hospital admission rates for emphysema, nonspecific chronic bronchitis, and simple and mucopurulent chronic bronchitis were greater in males than in females (Supplementary Material S1).
3.2. Chronic Lower Respiratory Diseases Admission Rate by Age Group
The majority of hospital admissions for chronic lower respiratory diseases were found to be directly linked to age (more prevalent in the 75 and older age group), and these diseases include bronchitis that is neither acute nor chronic, simple and mucopurulent chronic bronchitis, unspecified chronic bronchitis, emphysema, other chronic obstructive pulmonary diseases, and bronchiectasis. Even so, hospital admissions for asthma were more frequent in the following age groups: 15 years and under, 75 and older, 60 to 74 years, and 15 to 59 years, respectively. Status-asthmaticus-related hospital admissions were more prevalent in the following age groups: 60 to 74 years, 75 years and older, and those under 15 years (Supplementary Material S2).
4. Discussion
This was an ecological study that examined the trend of hospital admissions related to chronic lower respiratory diseases in England and Wales between 1999 and 2020. The key findings are as follows: The hospital admission rate per 100,000 people increased by 57.5% from 1999 to 2020. The majority of hospital admissions for chronic lower respiratory diseases were found to be directly linked to age (more prevalent in the 75+ age group). Female hospital admission rates increased by 85.2%, while male hospital admission rates increased by 30.7%. Other chronic obstructive pulmonary diseases (chronic obstructive pulmonary with (acute) lower respiratory infection and (acute) exacerbation), and asthma accounted for 89% of all hospital admissions for chronic lower respiratory diseases. Hospital admissions for other chronic obstructive pulmonary diseases were more frequent in the age groups of 60 to 74 years, and 75 and older, whereas asthma was more frequent in the age group of 15 years and under.
In 2019, the World Health Organization (WHO) ranked chronic obstructive pulmonary (COPD), and lower respiratory infections as the third and fourth leading causes of death globally, respectively [25]. Similarly, in the UK, chronic lower respiratory diseases ranked as the fourth leading cause of death [26]. Therefore, it is not surprising that the rate of hospital admission increased by 57.5%. However, this increase would increase the burden on the healthcare system. According to the British Lung Foundation, the UK spends GBP 11 billion a year on lung disease [27]. Around 58% of the total cost is associated with COPD (29%), lower respiratory infections (16%), and asthma (13%). This is consistent with the findings of this study, as 89% of all hospital admissions were due to COPD (62.3%) and asthma (26.7%). Despite the positive outcomes of the current practice of self-management, rescue packs, and pulmonary rehabilitation [28], the results of this study indicate that more work is needed on the management plan and that it might be possible to incorporate new health solutions, such as telehealth, which could enable early detection and quick access to medical services or interventions that could prevent hospital admission, thereby lowering the rate of hospital admissions [29,30].
The UK’s population in 2019 is predicted to be equal to 66.8 million, according to the Office for National Statistics release of the results of the 2021 census. The number of people 65 and older increased from 15.8% in 1999 to 18.5% in 2019 and is projected to reach 23.9% by 2039. Along with an increase in persons living alone, they also noted that rural and coastal areas have a higher percentage of senior residents. This could reduce the likelihood of having quick and simple access to healthcare support when needed or for routine care, which could cause deterioration and necessitate hospitalisation [31]. In this study, there was a linkage between the rate of admission and the age group (Supplementary Material S2). The age group of 75 years and above accounted for 33.8% of the total number of hospital admissions for chronic lower respiratory diseases, followed by the age group of 60 to 74 years with 32.8%, and the age group of 15 to 59 years with 24.6%. This could be due to the fact that ageing is associated with changes in the structure of the thoracic cavity and a reduction in the strength of the inspiratory and expiratory muscles [32,33,34]. Additionally, a decrease in the strength of the respiratory muscles could have an effect on how well the airways are cleared because a weaker cough could result in an accumulation of secretions [33]. Peak cough flow (PCF) and peak expiratory flow (PEF) were found to be higher in people who were more active, according to a study by Freitas et al. on 61 elderly healthy individuals [35]. Age-related structural changes and their effects may increase the risk of infections and hospitalisation [36].
In this study, the hospital admissions rate for other chronic obstructive pulmonary diseases (chronic obstructive pulmonary with (acute) lower respiratory infection and (acute) exacerbation) was higher in the age groups of 65–74 years and 75 years and above. This increase could be due to three factors, which are ageing-related FEV1 reduction, exacerbation susceptibility, and disease prognosis and severity [37]. A study conducted by Hurst et al. revealed that the severity and frequency of COPD exacerbations are related to the disease’s severity (prognosis), which may eventually raise the hospitalisation rate [38]. Evidence demonstrates that repeated or frequent exacerbations raise a patient’s level of airway inflammation during the stable state [39]. However, the quality of life is also correlated with the frequency of exacerbations [40]. The decrease in the quality of life and physical activity will impact muscle strength, which again may impact airway clearance, and the rate of hospitalisation, as cough and secretion production are associated with exacerbations [36,41,42]. Socio-economic factors could be important contributing factors that increased the rate of hospitalisation in the UK during the study period. Smoking, air pollution, allergen exposure, poor diet, obesity, and lack of physical activity are among the most important modifiable risk factors associated with chronic lower respiratory diseases [4]. In addition, previous studies in the literature reported that education level, income, occupation, and housing conditions are associated with higher rates of hospitalisation and mortality due to chronic lower respiratory diseases [43,44,45].
In this study, hospitalisation for females increased by 85.2% from 1999 to 2020. This might be due to the impact of smoking behaviours through the years or exposure to indoor biomass [28]. However, Montserrat-Capdevila et al. found that females were more susceptible than males to the harmful effects of smoking in a research study they carried out on 24,135 COPD patients in Spain. Additionally, they noted that bronchiectasis and obstructive sleep apnoea were common concomitant conditions in females [46]. Another study assessed the factors related to the frequency of exacerbation and noted that the history of asthma and the rates of previous exacerbations per year were higher in women [38]. Although comorbidities were not evaluated in this study, the rates of admissions due to bronchiectasis and asthma were also higher in females than males, which confirms the findings of previous studies.
This study highlights the need for additional research and treatment options for lower respiratory diseases. Furthermore, the majority of the budget should be devoted to lower respiratory diseases and the elderly age group. Furthermore, it highlights the need for greater focus on other therapy modalities, such as lung rehabilitation and smoking cessation. These findings may also be used to argue for the expansion of telehealth services in order to monitor patients who have little access to medical treatment, such as those who reside in the suburbs, or to help detect any deterioration earlier. However, as comorbidities, medications, and management plans were not examined in this study, due to the ecological nature of the study design (on the population level), the results should be interpreted with caution.
5. Conclusions
The rates of hospital admissions due to chronic lower respiratory diseases have increased during the past two decades in England and Wales. The majority of those admissions were due to COPD. Ageing was found to be a factor in increased hospital admissions. Pulmonary rehabilitation and smoking cessation together with other validated management strategies should be reinforced. Moreover, more research should be conducted in selected groups on utilising advanced innovative solutions to enable early detection of deterioration in health.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare11010065/s1, Supplementary Material S1: Hospital admission rates for chronic lower respiratory diseases in England and Wales stratified by gender; Supplementary Material S2: Hospital admission rates for chronic lower respiratory diseases in England and Wales stratified by age.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Grant No. GRANT2341].
Institutional Review Board Statement
Hospital admissions and population data are publicly available as de-identified data. Therefore, it was considered an exempt category.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Publicly available datasets were analysed in this study. These data can be found at http://http//content.digital.nhs.uk/hes and https://www.wales.nhs.uk/document/176173#:~:text=The%20Patient%20Episode%20Database%20for%20Wales%20%28PEDW%29%20is,major%20operations%2C%20and%20hospital%20stays%20for%20giving%20birth (accessed on 14 September 2022).
Acknowledgments
Author thank the financial support by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Grant No. GRANT2341].
Conflicts of Interest
The author declares that there are no conflict of interest.
References
- National Cancer Institute. NCI Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/respiratory-disease (accessed on 5 November 2022).
- British Lung Foundation. The Battle for Breath: The Impact of Lung Disease in the UK. Available online: https://www.blf.org.uk/policy/the-battle-for-breath-2016 (accessed on 5 November 2022).
- World Health Organization. ICD-10 Version: 2019. Available online: https://icd.who.int/browse10/2019/en#/J40-J47 (accessed on 5 November 2022).
- World Health Organization. Global Surveillance, Prevention and Control of CHRONIC Respiratory Diseases. Available online: https://www.who.int/publications/i/item/global-surveillance-prevention-and-control-of-chronic-respiratory-diseases (accessed on 5 November 2022).
- Pesce, G. Mortality rates for chronic lower respiratory diseases in Italy from 1979 to 2010: An age-period-cohort analysis. ERJ Open Res. 2016, 2, 00093-02015. [Google Scholar] [CrossRef] [Green Version]
- Townsend, C.M. Sabiston Textbook of Surgery E-Book: The Biological Basis of Modern Surgical Practice; Elsevier Health Sciences: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Office for National Statistics. Deaths Registered in England and Wales. Available online: https://www.ons.gov.uk/file?uri=/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsregisteredinenglandandwalesseriesdrreferencetables/2019/finalreftables2019.xlsx (accessed on 5 November 2022).
- Wedzicha, J.A.; Seemungal, T.A. COPD exacerbations: Defining their cause and prevention. Lancet 2007, 370, 786–796. [Google Scholar] [CrossRef]
- Criner, G.J.; Bourbeau, J.; Diekemper, R.L.; Ouellette, D.R.; Goodridge, D.; Hernandez, P.; Curren, K.; Balter, M.S.; Bhutani, M.; Camp, P.G.; et al. Executive summary: Prevention of acute exacerbation of COPD: American college of chest physicians and canadian thoracic society guideline. Chest 2015, 147, 883–893. [Google Scholar] [CrossRef]
- Naser, A.Y.; Mansour, M.M.; Alanazi, A.F.R.; Sabha, O.; Alwafi, H.; Jalal, Z.; Paudyal, V.; Dairi, M.S.; Salawati, E.M.; Alqahtan, J.S.; et al. Hospital admission trends due to respiratory diseases in England and Wales between 1999 and 2019: An ecologic study. BMC Pulm. Med. 2021, 21, 356. [Google Scholar] [CrossRef]
- Naser, A.Y.; Alrawashdeh, H.M.; Alwafi, H.; AbuAlhommos, A.K.; Jalal, Z.; Paudyal, V.; Alsairafi, Z.K.; Salawati, E.M.; Samannodi, M.; Sweiss, K.; et al. Hospital admission trends due to viral infections characterised by skin and mucous membrane lesions in the past two decades in england and wales: An ecological study. Int. J. Environ. Res. Public Health 2021, 18, 1649. [Google Scholar] [CrossRef]
- Naser, A.Y.; Alwafi, H.; Hemmo, S.I.; Alrawashdeh, H.M.; Alqahtani, J.S.; Alghamdi, S.M.; Mustafa Ali, M.K. Trends in hospital admissions due to neoplasms in england and wales between 1999 and 2019: An ecological study. Int. J. Environ. Res. Public Health 2022, 19, 8054. [Google Scholar] [CrossRef]
- Naser, A.Y.; Dahmash, E.Z.; Al-Daghastani, T.; Alwafi, H.; Abu Hamdah, S.; Alsairafi, Z.K.; Alsaleh, F.M. An ecological analysis of hospitalization patterns for diseases of the nervous system in england and wales over the last 20 years. Healthcare 2022, 10, 1670. [Google Scholar] [CrossRef]
- Naser, A.Y.; Dahmash, E.Z.; Alqahtani, J.S.; Alsairafi, Z.K.; Alsaleh, F.M.; Alwafi, H. Trends in hospital admissions for mental, behavioural and neurodevelopmental disorders in england and wales between 1999 and 2019: An ecological study. Healthcare 2022, 10, 2191. [Google Scholar] [CrossRef]
- Naser, A.Y.; Wang, Q.; Wong, L.Y.L.; Ilomaki, J.; Bell, J.S.; Fang, G.; Wong, I.C.K.; Wei, L. Hospital admissions due to dysglycaemia and prescriptions of antidiabetic medications in england and wales: An ecological study. Diabetes Ther. 2018, 9, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Alanazi, A.F.R.; Naser, A.Y.; Pakan, P.; Alanazi, A.F.; Alanazi, A.A.A.; Alsairafi, Z.K.; Alsaleh, F.M. Trends of hospital admissions due to congenital anomalies in england and wales between 1999 and 2019: An ecological study. Int. J. Environ. Res. Public Health 2021, 18, 11808. [Google Scholar] [CrossRef]
- Al-Daghastani, T.; Naser, A.Y. Hospital admission profile related to poisoning by, adverse effect of and underdosing of psychotropic drugs in England and Wales: An ecological study. Saudi Pharm. J. 2022, 30, 1262–1272. [Google Scholar] [CrossRef] [PubMed]
- Alrawashdeh, H.M.; Naser, A.Y.; Alwafi, H.; AbuAlhommos, A.K.; Jalal, Z.; Paudyal, V.; Abdulmannan, D.M.; Hassanin, F.F.; Hemmo, S.I.; Al Sarireh, F. Trends in hospital admission due to diseases of the eye and adnexa in the past two decades in england and wales: An ecological study. Int. J. Gen. Med. 2022, 15, 1097–1110. [Google Scholar] [CrossRef]
- Al-shehri, H.; Dahmash, D.T.; Rochow, N.; Alturki, B.; Alrajhi, D.; Alayed, F.; Alhazani, F.; Alsuhibany, H.; Naser, A.Y. Hospital admission profile of neonates for conditions originating in the perinatal period in england and wales between 1999–2020: An ecological study. Int. J. Gen. Med. 2022, 15, 1973–1984. [Google Scholar] [CrossRef]
- Hemmo, S.I.; Naser, A.Y.; Alwafi, H.; Mansour, M.M.; Alanazi, A.F.R.; Jalal, Z.; Alsairafi, Z.K.; Paudyal, V.; Alomari, E.; Al-Momani, H.; et al. Hospital admissions due to ischemic heart diseases and prescriptions of cardiovascular diseases medications in england and wales in the past two decades. Int. J. Environ. Res. Public Health 2021, 18, 7041. [Google Scholar] [CrossRef] [PubMed]
- Sweiss, K.; Naser, A.Y.; Alrawashdeh, H.M.; Alharazneh, A. Hospital admissions due to vasomotor and allergic rhinitis in England and Wales between 1999 and 2019: An ecological study. Ir. J. Med. Sci. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sweiss, K.; Naser, A.Y.; Samannodi, M.; Alwafi, H. Hospital admissions due to infectious and parasitic diseases in England and Wales between 1999 and 2019: An ecological study. BMC Infect. Dis. 2022, 22, 398. [Google Scholar] [CrossRef] [PubMed]
- Mustafa Ali, M.; Naser, A.; AbuAlhommos, A.K.; Al-Daghastani, T.; Alrawashdeh, H.M.; Mustafa Ali, S.; Alwafi, H.; Alqurashi, M.; Basha Ahmed, A.; Albarqi, H. Hospital admissions secondary to diseases of the blood, blood-forming organs, and immune system in england and wales. Cureus 2022, 14, 30179. [Google Scholar] [CrossRef]
- Mustafa Ali, S.; Naser, A.Y.; Alghanemi, A.G.; AbuAlhommos, A.K.; Sabha, M.; Mustafa Ali, M.K.; Hemmo, S.I.; Alrajeh, A.M.; Alqahtani, J.S.; Aldhahir, A.M.; et al. Musculoskeletal system and connective tissue related hospital admission in england and wales between 1999 and 2019: An ecologic study. Cureus 2022, 14, 32453. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 14 September 2022).
- Office for National Statistics. Leading Causes of Death, UK: 2001 to 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/articles/leadingcausesofdeathuk/2001to2018 (accessed on 14 September 2022).
- Trueman, D.W.F.; Hancock, E. Estimating the Economic Burden of Respiratory Illness in the UK. 28/10. Available online: https://www.blf.org.uk/policy/economic-burden (accessed on 14 September 2022).
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease; GOLD Report; Global Initiative for Chronic Obstructive Lung Disease: Deer Park, IL, USA, 2022. [Google Scholar]
- Al Rajeh, A.; Hurst, J. Monitoring of physiological parameters to predict exacerbations of chronic obstructive pulmonary disease (copd): A systematic review. J. Clin. Med. 2016, 5, 108. [Google Scholar] [CrossRef]
- Al Rajeh, A.M.; Aldabayan, Y.S.; Aldhahir, A.; Pickett, E.; Quaderi, S.; Alqahtani, J.S.; Mandal, S.; Lipman, M.C.I.; Hurst, J.R. Once daily versus overnight and symptom versus physiological monitoring to detect exacerbations of chronic obstructive pulmonary disease: Pilot randomized controlled trial. JMIR Mhealth Uhealth 2020, 8, e17597. [Google Scholar] [CrossRef]
- Office for National Statistics. Overview of the UK Population. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/articles/overviewoftheukpopulation/january2021 (accessed on 14 September 2022).
- Bartynski, W.S.; Heller, M.T.; Grahovac, S.Z.; Rothfus, W.E.; Kurs-Lasky, M. Severe thoracic kyphosis in the older patient in the absence of vertebral fracture: Association of extreme curve with age. AJNR Am. J. Neuroradiol. 2005, 26, 2077–2085. [Google Scholar] [PubMed]
- Sharma, G.; Goodwin, J. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 2006, 1, 253. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, E.; Lowery, E.; Kuhlmann, E.; Brubaker, A. The aging lung. Clin. Interv. Aging 2013, 8, 1489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, F.S.; Ibiapina, C.C.; Alvim, C.G.; Britto, R.R.; Parreira, V.F. Relationship between cough strength and functional level in elderly. Braz. J. Phys. Ther. 2010, 14, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Burgel, P.-R.; Nesme-Meyer, P.; Chanez, P.; Caillaud, D.; Carré, P.; Perez, T.; Roche, N. Cough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjects. Chest 2009, 135, 975–982. [Google Scholar] [CrossRef]
- Brandstetter, R.D.; Kazemi, H. Aging and the respiratory system. Med. Clin. N. Am. 1983, 67, 419–431. [Google Scholar] [CrossRef]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Müllerova, H.; Tal-Singer, R.; Miller, B.; Lomas, D.A.; Agusti, A.; MacNee, W.; et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef] [Green Version]
- Bhowmik, A.; Seemungal, T.A.; Sapsford, R.J.; Wedzicha, J.A. Relation of sputum inflammatory markers to symptoms and lung function changes in COPD exacerbations. Thorax 2000, 55, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Seemungal, T.A.; Donaldson, G.C.; Paul, E.A.; Bestall, J.C.; Jeffries, D.J.; Wedzicha, J.A. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 1418–1422. [Google Scholar] [CrossRef]
- Miravitlles, M.; Guerrero, T.; Mayordomo, C.; Sánchez-Agudo, L.; Nicolau, F.; Segú, J.L. Factors associated with increased risk of exacerbation and hospital admission in a cohort of ambulatory copd patients: A multiple logistic regression analysis. Respiration 2000, 67, 495–501. [Google Scholar] [CrossRef]
- Foreman, M.G.; DeMeo, D.L.; Hersh, C.P.; Reilly, J.J.; Silverman, E.K. Clinical determinants of exacerbations in severe, early-onset COPD. Eur. Respir. J. 2007, 30, 1124–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huisman, M.; Kunst, A.E.; Bopp, M.; Borgan, J.K.; Borrell, C.; Costa, G.; Deboosere, P.; Gadeyne, S.; Glickman, M.; Marinacci, C.; et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations. Lancet 2005, 365, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Pleasants, R.A.; Riley, I.L.; Mannino, D.M. Defining and targeting health disparities in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2475–2496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prescott, E.; Godtfredsen, N.; Vestbo, J.; Osler, M. Social position and mortality from respiratory diseases in males and females. Eur. Respir. J. 2003, 21, 821–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montserrat-Capdevila, J.; Marsal, J.R.; Ortega, M.; Castañ-Abad, M.T.; Alsedà, M.; Barbé, F.; Godoy, P. Clinico-epidemiological characteristics of men and women with a new diagnosis of chronic obstructive pulmonary disease: A database (SIDIAP) study. BMC Pulm. Med. 2021, 21, 44. [Google Scholar] [CrossRef]
Figure 1.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by type between 1999 and 2020.
Figure 1.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by type between 1999 and 2020.
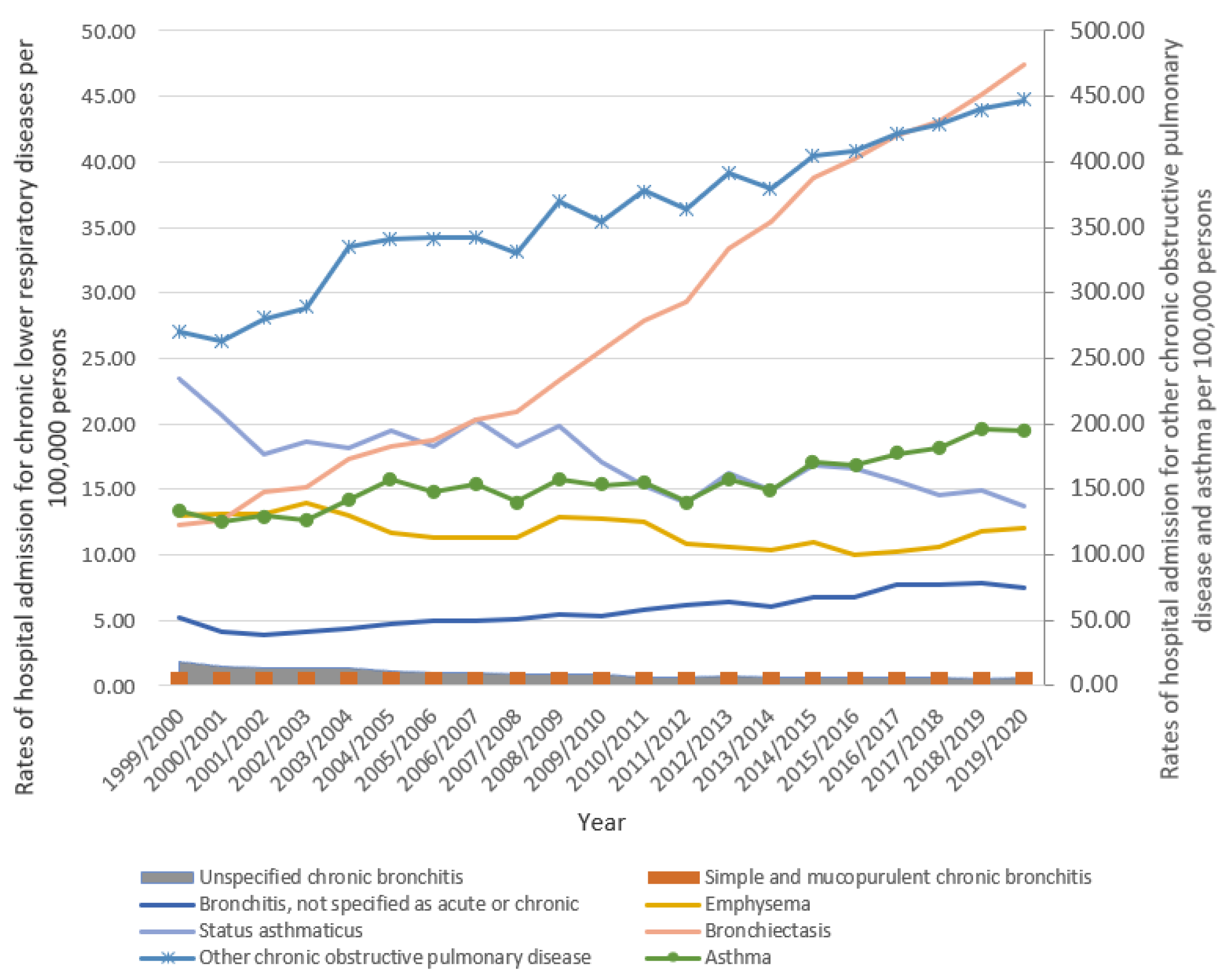
Figure 2.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by age group.
Figure 2.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by age group.

Figure 3.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by gender.
Figure 3.
Rates of hospital admission for chronic lower respiratory diseases in England and Wales stratified by gender.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Percentage of chronic lower respiratory diseases hospital admission from total number of admissions between 1999 and 2020.
Table 1.
Percentage of chronic lower respiratory diseases hospital admission from total number of admissions between 1999 and 2020.
| ICD Code | Description | Percentage from Total Number of Admissions |
|---|---|---|
| J40 | “Bronchitis, not specified as acute or chronic” | 1.0% |
| J41 | “Simple and mucopurulent chronic bronchitis” | <0.1% |
| J42 | “Unspecified chronic bronchitis” | 0.2% |
| J43 | “Emphysema” | 2.0% |
| J44 | “Other chronic obstructive pulmonary diseases (chronic obstructive pulmonary disease with (acute) lower respiratory infection and chronic obstructive pulmonary disease with (acute) exacerbation)” | 62.3% |
| J45 | “Asthma” | 26.7% |
| J46 | “Status asthmaticus” | 3.0% |
| J47 | “Bronchiectasis” | 4.8% |
ICD: International Statistical Classification of Diseases system.
Table 2.
Percentage change in the hospital admission rates for chronic lower respiratory diseases from 1999 to 2020.
Table 2.
Percentage change in the hospital admission rates for chronic lower respiratory diseases from 1999 to 2020.
| Diseases | Rate of Diseases in 1999 Per 100,000 Persons (95% CI) | Rate of Diseases in 2020 Per 100,000 Persons (95% CI) | Percentage Change from 1999 to 2020 | p-Value |
|---|---|---|---|---|
| “Bronchitis, not specified as acute or chronic” | 5.14 (4.94–5.33) | 7.46 (7.24–7.68) | 45.2% | ≤0.01 |
| “Simple and mucopurulent chronic bronchitis” | 0.11 (0.08–0.14) | 0.06 (0.04–0.08) | −41.8% | ≤0.01 |
| “Unspecified chronic bronchitis” | 1.82 (1.71–1.94) | 0.58 (0.52–0.64) | −68.2% | ≤0.01 |
| “Emphysema” | 12.99 (12.68–13.30) | 11.98 (11.71–12.26) | −7.8% | ≥0.05 |
| “Other chronic obstructive pulmonary diseases” | 270.18 (268.77–271.59) | 447.18 (445.49–448.88) | 65.5% | ≤0.01 |
| “Asthma” | 133.59 (132.60–134.58) | 195.24 (194.12–196.36) | 46.1% | ≤0.01 |
| “Status asthmaticus” | 23.45 (23.04–23.87) | 13.77 (13.47–14.06) | −41.3% | ≤0.01 |
| “Bronchiectasis” | 12.26 (11.96–12.56) | 47.43 (46.88–47.98) | 287.0% | ≤0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Al Rajeh, A.M. Trend of Admissions Due to Chronic Lower Respiratory Diseases: An Ecological Study. Healthcare 2023, 11, 65. https://doi.org/10.3390/healthcare11010065
AMA Style
Al Rajeh AM. Trend of Admissions Due to Chronic Lower Respiratory Diseases: An Ecological Study. Healthcare. 2023; 11(1):65. https://doi.org/10.3390/healthcare11010065
Chicago/Turabian StyleAl Rajeh, Ahmed M. 2023. "Trend of Admissions Due to Chronic Lower Respiratory Diseases: An Ecological Study" Healthcare 11, no. 1: 65. https://doi.org/10.3390/healthcare11010065
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.