Integrating Acupuncture into a Dialysis Center

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participant Criteria
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Acceptance
3.1.1. Adherence
3.1.2. Patients’ and Healthcare Professionals’ Attitudes toward Acupuncture
3.2. Feasibility
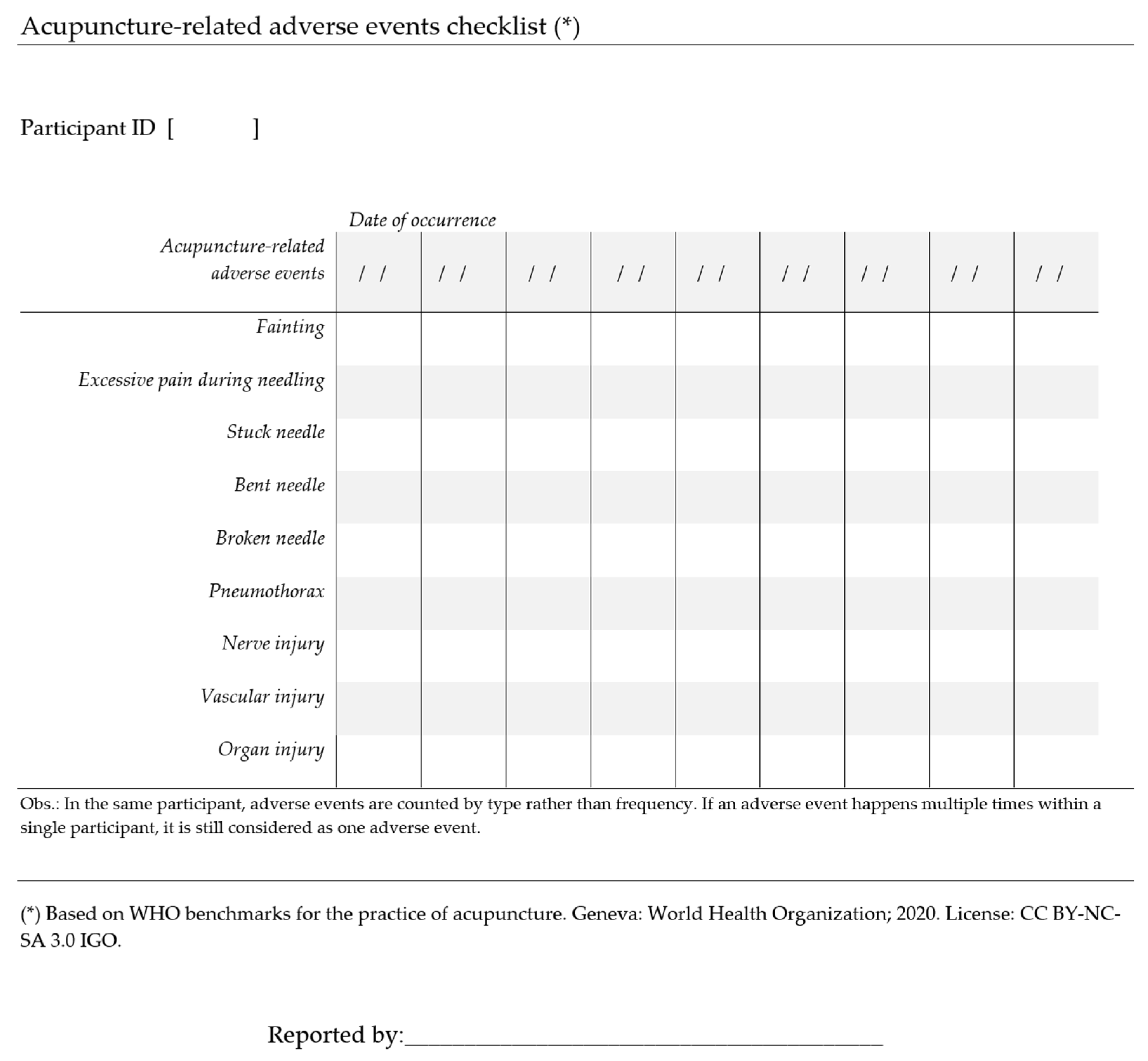
3.2.1. Safety
3.2.2. Effectiveness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. WHO Traditional Medicine Strategy: 2014–2023; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Programme on Traditional Medicine. WHO Traditional Medicine Strategy 2002–2005; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Bai, X.; Ta, N.; Gong, G.-H.; Zhang, B.; Wei, C.-X. Effects of Integrated Chinese Traditional Medicine and Conventional Western Medicine on the Quality of Life of Breast Cancer Patients: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2022, 2022, 3123878. [Google Scholar] [CrossRef] [PubMed]
- Sum, C.H.; Ching, J.; Zhang, H.; Loo, S.; Lo, C.W.; Lai, M.K.; Cheong, P.K.; Yu, C.L.; Lin, Z.-X. Integrated Chinese and western medicine interventions for atopic dermatitis: A systematic review and meta-analysis. Chin. Med. 2021, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Xu, N.; Zhou, Y.; Song, J.; Liu, J.; Zhu, H.; Jiang, J.; Xu, Y.; Li, R. Contribution of traditional Chinese medicine combined with conventional western medicine treatment for the novel coronavirus disease (COVID-19), current evidence with systematic review and meta-analysis. Phytother. Res. 2021, 35, 5992–6009. [Google Scholar] [CrossRef] [PubMed]
- Assembleia da República. Lei nº 45/2003. Diário da República nº193/2003, Série I-A de 22 de Agosto de 2003. 2003, pp. 5391–5392. Available online: https://files.dre.pt/1s/2003/08/193a00/53915392.pdf (accessed on 24 March 2023).
- Assembleia da República. Lei nº 95/2019. Diário da República nº 169/2019 Série I de 2019-08-04. 2019, pp. 6259–6661. Available online: https://files.dre.pt/1s/2019/09/16900/0005500066.pdf (accessed on 24 March 2023).
- Assembleia da República. Lei nº 109/2019. Diário da República nº 172/2019, Série I de 2019-09-09. 2019, pp. 92–93. Available online: https://files.dre.pt/1s/2019/09/17200/0009200093.pdf (accessed on 24 March 2023).
- Administração Central do Sistema de Saúde (ACSS). I. Lista de Cédulas Emitidas. Available online: https://rnp.min-saude.pt/tnc/faces/listaProfissionais.jsf (accessed on 24 March 2023).
- Amaral, P.; Fronteira, I. Regulation of non-conventional therapies in Portugal: Lessons learnt for strengthening human resources in health. Hum. Resour. Health 2021, 19, 114. [Google Scholar] [CrossRef] [PubMed]
- Zahm, A. Integrating Acupuncture into Primary Care. J. Altern. Complement. Med. 2021, 27, 384–389. [Google Scholar] [CrossRef]
- Harrison, J.D.; Reddy, S.; Liu, R.; Adler, S.R.; Chao, M.T. Implementing an Inpatient Acupuncture Service for Pain and Symptom Management: Identifying Opportunities and Challenges. J. Altern. Complement. Med. 2019, 25, 503–508. [Google Scholar] [CrossRef]
- Garcia, M.K.; Cohen, L.; Spano, M.; Spelman, A.; Hashmi, Y.; Chaoul, A.; Wei, Q.; Lopez, G. Inpatient Acupuncture at a Major Cancer Center. Integr. Cancer Ther. 2018, 17, 148–152. [Google Scholar] [CrossRef]
- Hurstak, E.; Chao, M.T.; Leonoudakis-Watts, K.; Pace, J.; Walcer, B.; Wismer, B. Design, Implementation, and Evaluation of an Integrative Pain Management Program in a Primary Care Safety-Net Clinic. J. Altern. Complement. Med. 2019, 25, S78–S85. [Google Scholar] [CrossRef]
- Zhang, N.M.; Vesty, G.; Zheng, Z. Healthcare Professionals’ Attitudes to Integration of Acupuncture in Western Medicine: A Mixed-Method Systematic Review. Pain Manag. Nurs. 2021, 22, 684–693. [Google Scholar] [CrossRef]
- Tempest, H.; Reynard, J.; Bryant, R.J.; Hamdy, F.C.; Larré, S. Acupuncture in urological practice—A survey of urologists in England. Complement. Ther. Med. 2011, 19, 27–31. [Google Scholar] [CrossRef]
- Shao, J.Y.J.; Borthwick, A.M.; Lewith, G.T.; Hopwood, V.; Borthwick, A.M. Attitudes towards Traditional Acupuncture in the UK. Evidence-Based Integr. Med. 2005, 2, 37–45. [Google Scholar] [CrossRef]
- Lipman, L.; Dale, J.; MacPherson, H. Attitudes of GPs towards the provision of acupuncture on the NHS. Complement. Ther. Med. 2003, 11, 110–114. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, M.C.; de Azevedo, J.N.; Azevedo, P.; Pires, C.; Laranjeira, M.; Machado, J.P. Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial. Healthcare 2022, 10, 1947. [Google Scholar] [CrossRef] [PubMed]
- Correia de Carvalho, M.N.d.A.J.; Azevedo, P.; Pires, C.; Machado, J.P.; Laranjeira, M. Effectiveness of Acupuncture on Health-Related Quality of Life in Patients Receiving Maintenance Hemodialysis. Healthcare 2023, 11, 1355. [Google Scholar] [CrossRef]
- de Carvalho, M.C.; Machado, J.P.; Laranjeira, M.; de Azevedo, J.N.; Azevedo, P. Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial. Healthcare 2022, 10, 2050. [Google Scholar] [CrossRef]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D.; on behalf of the STRICTA Revision Group. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT Statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef]
- IBM. SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Bahall, M. Use of complementary and alternative medicine by patients with end-stage renal disease on haemodialysis in Trinidad: A descriptive study. BMC Complement. Altern. Med. 2017, 17, 250. [Google Scholar] [CrossRef]
- Zhang, N.M.; Daly, D.; Terblanche, M.; Joshi, S.; Tacey, M.; Vesty, G.; Zheng, Z. Doctors’ and Nurses’ Attitudes of Acupuncture and Acupressure use in Perioperative Care: An Australian National Survey. Pain Manag. Nurs. 2022, 23, 800–810. [Google Scholar] [CrossRef]
- Liu, L.; Tang, Y.; Baxter, G.D.; Yin, H.; Tumilty, S. Complementary and alternative medicine—Practice, attitudes, and knowledge among healthcare professionals in New Zealand: An integrative review. BMC Complement. Med. Ther. 2021, 21, 63. [Google Scholar] [CrossRef]
- Zhang, J.; Mu, Y.; Zhang, Y. Effects of Acupuncture and Rehabilitation Training on Limb Movement and Living Ability of Patients with Hemiplegia after Stroke. Behav. Neurol. 2022, 2022, 2032093. [Google Scholar] [CrossRef]
- Lin, C.-J.; Yeh, M.-L.; Wu, S.-F.; Chung, Y.-C.; Lee, J.C.-H. Acupuncture-related treatments improve cognitive and physical functions in Alzheimer’s disease: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2022, 36, 609–635. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, W.; Gao, W.; Yang, D. Comparison of Acupuncture and Sham Acupuncture in Migraine Treatment: An Overview of Systematic Reviews. Neurologist 2022, 27, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.-J.; Wu, X.-Y.; Wang, W.; Chang, X.-S.; Zhan, D.-D.; Diao, D.-C.; Xiao, J.; Li, Y.; Ma, D.; Hu, M.; et al. Acupuncture for Quality of Life in Gastric Cancer Patients Undergoing Adjuvant Chemotherapy. J. Pain Symptom Manag. 2022, 63, 210–220. [Google Scholar] [CrossRef]
- Lee, B.; Kwon, C.-Y.; Park, M.Y. Acupuncture for the Treatment of Chronic Rhinosinusitis: A PRISMA-Compliant Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2022, 2022, 6429836. [Google Scholar] [CrossRef]
- Höxtermann, M.D.; Haller, H.; Aboudamaah, S.; Bachemir, A.; Dobos, G.; Cramer, H.; Voiss, P. Safety of acupuncture in oncology: A systematic review and meta-analysis of randomized controlled trials. Cancer 2022, 128, 2159–2173. [Google Scholar] [CrossRef]
- Xu, Z.; Wang, X.; Wu, Y.; Wang, C.; Fang, X. The effectiveness and safety of acupuncture for chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Front. Neurol. 2022, 13, 963358. [Google Scholar] [CrossRef]
- Zhang, L.; Li, Y.; Xiao, X.; Shi, Y.; Xu, D.; Li, N.; Deng, Y. Acupuncture for Uremic Pruritus: A Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2022, 65, e51–e62. [Google Scholar] [CrossRef]

{kind=link}
| VA Group (n = 23) | SA Group (n = 22) | Total (N = 45) | p-Value | ||
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Age | Minimum–Maximum | 60–84 | 57–91 | 57–91 | 0.496 (2) |
| Mean (SD) | 71.2 (5.1) | 72.6 (8.3) | 71.9 (6.8) | ||
| n (%) | n (%) | n (%) | |||
| Gender | Female | 9 (39.1) | 8 (36.4) | 17 (37.8) | 1.000 (1) |
| Male | 14 (60.9) | 14 (63.6) | 28 (62.2) | ||
| Residence | Urban | 9 (39.1) | 8 (36.4) | 17 (37.8) | 1.000 (1) |
| Rural | 14 (60.9) | 14 (63.6) | 28 (62.2) | ||
| Education level | No literacy | 0 (0.0) | 2 (9.1) | 2 (4.4) | 1.000 (1) |
| 1° Cycle (4 years) | 20 (87.0) | 17 (77.3) | 37 (82.2) | ||
| 2° Cycle (6 years) | 2 (8.7) | 1 (4.5) | 3 (6.7) | ||
| High school (12 years) | 1 (4.3) | 2 (9.1) | 3 (6.7) | ||
| Professional status | Employed | 0 (0.0) | 2 (9.1) | 2 (4.4) | 0.782 (1) |
| Self-employed | 2 (8.7) | 0 (0.0) | 2 (4.4) | ||
| Unemployed | 1 (4.3) | 1 (4.5) | 2 (4.4) | ||
| Retired | 20 (87.0) | 19 (86.4) | 39 (86.7) | ||
| Clinical | n (%) | n (%) | n (%) | ||
| CKD causes | Diabetes mellitus | 10 (43.5) | 10 (45.5) | 20 (44.4) | 0.202 (1) |
| Chronic rejection | 1 (4.3) | 4 (18.2) | 5 (11.1) | ||
| Hypertensive nephropathy | 3 (13.0) | 0 (0.0) | 3 (6.7) | ||
| High blood pressure | 0 (0.0) | 1 (4.5) | 1 (2.2) | ||
| Glomerulonephritis | 1 (4.3) | 0 (0.0) | 1 (2.2) | ||
| Interstitial tubular necrosis | 0 (0.0) | 2 (9.1) | 2 (4.4) | ||
| Other | 3 (13.0) | 1 (4.5) | 4 (8.9) | ||
| Unknown | 5 (21.7) | 4 (18.2) | 9 (20.0) | ||
| Hemodialysis time | <12 months | 2 (8.7) | 0 (0.0) | 2 (4.4) | 0.544 (1) |
| 12 to 120 months | 19 (82.6) | 20 (90.9) | 39 (86.7) | ||
| >120 months | 2 (8.7) | 2 (9.1) | 4 (8.9) | ||
| Vascular access | Arteriovenous fistula | 22 (95.7) | 18 (81.8) | 40 (88.9) | 0.187 (1) |
| Central venous catheter | 1 (4.3) | 4 (18.2) | 5 (11.1) |
| n (%) | ||
|---|---|---|
| Gender | Female | 5 (41.7) |
| Male | 7 (58.3) | |
| Age | Minimum–Maximum | 23–73 |
| Mean (SD) | 51.2 (13.7) | |
| Education level | Bachelor’s Degree | 10 (83.3) |
| Master’s Degree | 2 (16.7) | |
| Profession | Doctor | 5 (41.7) |
| Nurse | 7 (58.3) | |
| Medical specialty | General Practice/Family Medicine | 3 (25.0) |
| (Doctors: N = 5) | Nephrology | 2 (16.7) |
| Nursing specialty | Medical-surgical | 1 (14.3) |
| Rehabilitation | 1 (14.3) | |
| Public health | 1 (14.3) | |
| (Nurses: N = 7) | None | 4 (57.1) |
| VA Group (n) | SA Group (n) | Total (n/%) | p-Value (1) | |
|---|---|---|---|---|
| Baseline assessment | 24 | 24 | 48 (100) | |
| Treatment | 24 | 24 | 48 (100) | |
| Post-treatment assessment | 24 | 24 | 48 (100) | |
| 12-week follow-up assessment | 23 | 22 | 45 (93.4) | |
| Lost in follow-up/Dropout | 1 | 2 | 3 (6.6) | |
| Reason | Kidney transplantation | Hospitalization, death | ||
| Analyzed-n (%) | 23 (95.8%) | 22 (91.7%) | 45 (93.4%) | 1.000 |
| VA Group (n = 23) | SA Group (n = 22) | Total (N = 45) | p-Value (1) | ||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Do you know what Acupuncture is? | No | 11 (47.8) | 14 (63.6) | 25 (55.6) | 0.373 |
| Yes | 12 (52.2) | 8 (36.4) | 20 (44.4) | ||
| Have you received any Acupuncture treatment before your participation in this study? | No | 23 (100.0) | 21 (95.5) | 44 (97.8) | 0.489 |
| Yes | 0 (0.0) | 1 (4.5) | 1 (2.2) | ||
| If so, how long ago has it been? | >3 months | - | |||
| And for what purpose? | Osteoarticular pain | - | |||
| Are you willing to receive an Acupuncture treatment? | No | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Yes | 23 (100.0) | 22 (100.0) | 45 (100.0) |
| VA Group (n = 23) | SA Group (n = 22) | Total (N = 45) | p-Value (1) | ||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Degree of discomfort felt when puncturing the acupuncture needle. | Totally uncomfortable | - | - | - | 0.858 |
| Uncomfortable | 8 (34.8) | 6 (27.3) | 14 (31.1) | ||
| Neither comfortable, nor uncomfortable | 11 (47.8) | 11 (50.0) | 22 (48.9) | ||
| Comfortable | 4 (17.4) | 5 (22.7) | 9 (20.0) | ||
| Totally comfortable | - | - | - | ||
| Degree of discomfort during acupuncture treatment. | Totally uncomfortable | - | - | - | 0.488 |
| Uncomfortable | - | - | - | ||
| Neither comfortable, nor uncomfortable | 3 (13.0) | 5 (22.7) | 8 (17.8) | ||
| Comfortable | 10 (43.5) | 6 (27.3) | 16 (35.6) | ||
| Totally comfortable | 10 (43.5) | 11 (50.0) | 21 (46.7) | ||
| Would you recommend acupuncture treatment to others? | No | 2 (8.7) | 2 (9.1) | 4 (8.9) | 1.000 |
| Yes | 21 (91.3) | 20 (90.9) | 41 (91.1) | ||
| In your opinion, did the Acupuncture treatments interfere with your hemodialysis routine? | No | 23 (100.0) | 22 (100.0) | 45 (100.0) | - |
| Yes | - | - | - |
| n (%) | ||
|---|---|---|
| Do you know what Acupuncture is? | No | - |
| Yes | 12 (100.0) | |
| Have you ever received any acupuncture treatment? | No | 8 (66.7) |
| Yes | 4 (33.3) | |
| If so, how long ago has it been? | >3 months | 4 (100.0) |
| And for what purpose? | Osteoarticular pain | 2 (50.0) |
| Muscle pain | 3 (75.0) | |
| Would you recommend acupuncture treatment to others? | No | - |
| Yes | 12 (100.0) | |
| Would you be receptive to receiving acupuncture treatment? | No | 1 (8.3) |
| Yes | 11 (91.7) | |
| What is your general opinion on Acupuncture? | Very negative | - |
| Negative | - | |
| Neither negative nor positive | 2 (16.7) | |
| Positive | 8 (66.7) | |
| Very positive | 2 (16.7) | |
| What is your opinion on the efficacy and clinical applicability of Acupuncture? | Very negative | - |
| Negative | - | |
| Neither negative nor positive | 1 (8.3) | |
| Positive | 9 (75.0) | |
| Very positive | 2 (16.7) | |
| Have you ever suggested acupuncture to a patient? | No | 4 (33.3) |
| Yes | 8 (66.7) | |
| In your opinion, did the acupuncture treatments provided to patients interfere with the hemodialysis routine? | No | 12 (100.0) |
| Yes | - | |
| What is your opinion on the integration of acupuncture into the care of patients on hemodialysis? | Very negative | - |
| Negative | - | |
| Neither negative nor positive | 1 (8.3) | |
| Positive | 4 (33.3) | |
| Very positive | 7 (58.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia de Carvalho, M.; Azevedo, P.; Pires, C.; Machado, J.P.; Laranjeira, M.; Nunes de Azevedo, J. Integrating Acupuncture into a Dialysis Center. Healthcare 2023, 11, 1463. https://doi.org/10.3390/healthcare11101463
Correia de Carvalho M, Azevedo P, Pires C, Machado JP, Laranjeira M, Nunes de Azevedo J. Integrating Acupuncture into a Dialysis Center. Healthcare. 2023; 11(10):1463. https://doi.org/10.3390/healthcare11101463
Chicago/Turabian StyleCorreia de Carvalho, Marta, Pedro Azevedo, Carlos Pires, Jorge Pereira Machado, Manuel Laranjeira, and José Nunes de Azevedo. 2023. "Integrating Acupuncture into a Dialysis Center" Healthcare 11, no. 10: 1463. https://doi.org/10.3390/healthcare11101463