
A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania




Abstract
1. Introduction
- -
- To describe the annual volumes of orthopedic surgical interventions in the period 2001–2022 and to estimate the trends of evolution, taking into account the statistical data recorded in the NER;
- -
- To analyze the temporal trends of primary endoprosthesis surgeries, gender differences and regional differences;
- -
- To analyze the current trends in the hip and knee revision burdens and to identify the regional performances;
- -
- To estimate the volumes of surgical interventions that are expected to be performed in the following years by the National Health Service in order to establish the need for specialized human resources and material endowments.
2. Materials and Methods
- Study design and selection of study participants;
- Selection of the variables explored in the study and calculus methodology;
- Data collection and statistical analysis.
2.1. Study Design and Participants
- Hip replacement surgery, detailed by subsequent surgeries: total hip arthroplasty—code O12104 (in turn, detailed into prostheses: cemented total hip arthroplasty, uncemented total hip arthroplasty, hybrid and reverse hybrid total hip arthroplasty), bipolar hemiarthroplasty, unipolar hemiarthroplasty—Moore type—code O12103. We also extracted the gender of the patients who underwent these interventions;
- Knee replacement surgery, detailed by subsequent surgeries: bicondylar knee arthroplasty—code O14902, unicondylar knee arthroplasty—code O14901. We also extracted the gender of the patients who underwent these interventions;
- Revision hip arthroplasty—code O12401;
- Revision knee arthroplasty—code O15501;
- Operated fractures, including some of the following: closed reduction of femur fracture with internal fixation (code O11808), open reduction of the ankle fracture with internal fixation of the diastasis, fibula or malleolus (code O16801), closed reduction of tibial diaphysis fracture with internal fixation (code O14002), open reduction of the radius and ulnar diaphysis fracture with internal fixation (code O06504), closed reduction of the humeral shaft fracture with internal fixation (code O04904), etc.;
- Operated bone tumors, including some of the following: benign bone tumor resection with anatomically specific allograft (code: O19009 ), marginal excision of the malignant bone tumor with cementation of the defect (COD: O19605), en bloc resection of the malignant long bone tumor of the lower limb with arthrodesis of the adjacent joint (COD: O19703), en bloc resection of the malignant long bone tumor of the upper limb with replacement of the adjacent joint (COD: O19702), etc.;
- Hospitalized patients;
- Operated patients.
2.2. Evaluation Variables and Methodologies
2.2.1. The Volumes of Surgical Procedures and Growth Rates
2.2.2. Gender Differences
2.2.3. Regional Prevalence
2.2.4. Revision Burden
2.3. Data Collection and Statistical Analysis
3. Results
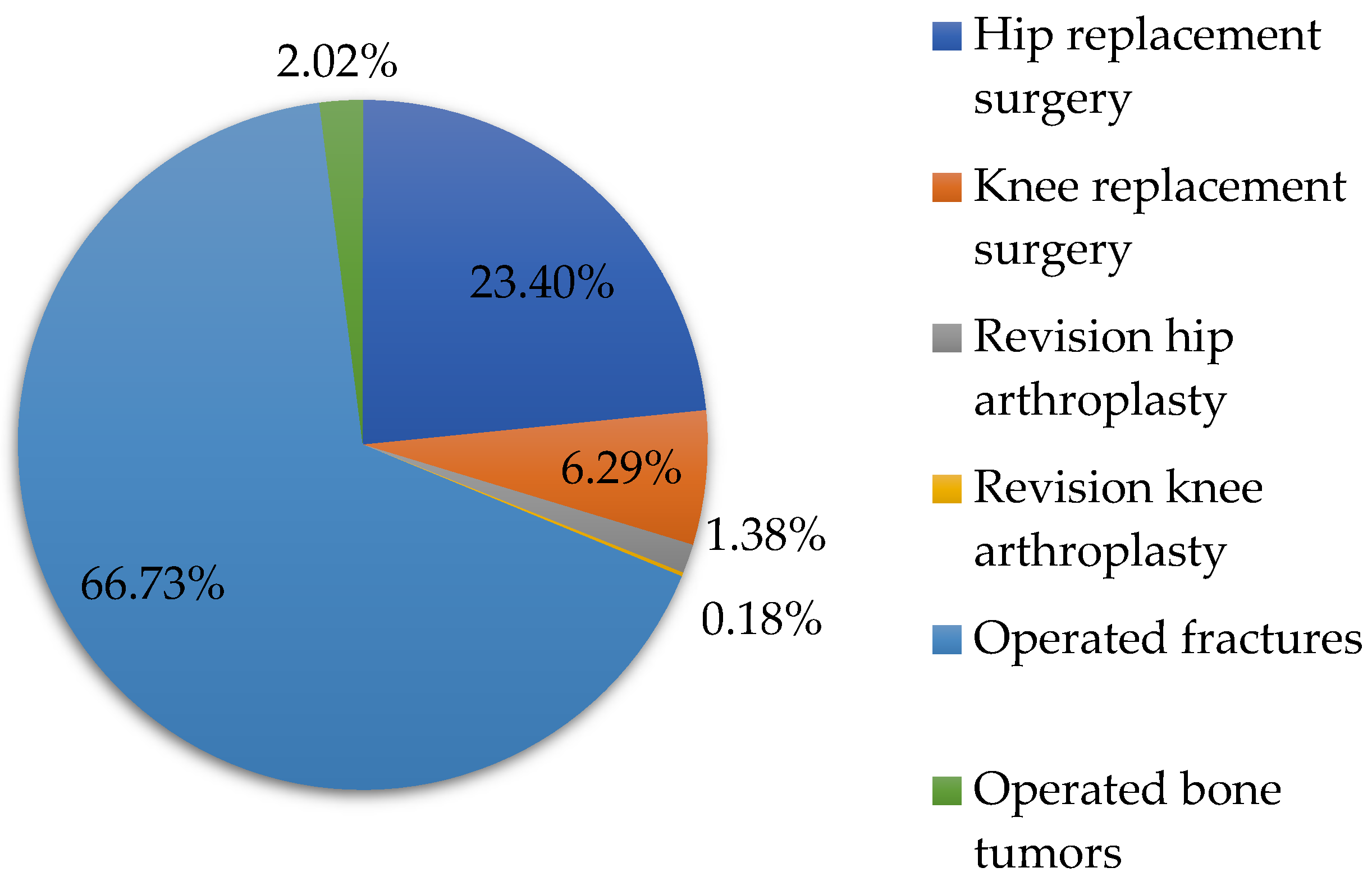
3.1. All Types of Orthopedic Surgeries
3.2. Hip Replacement Surgery
3.3. Knee Replacement Surgery
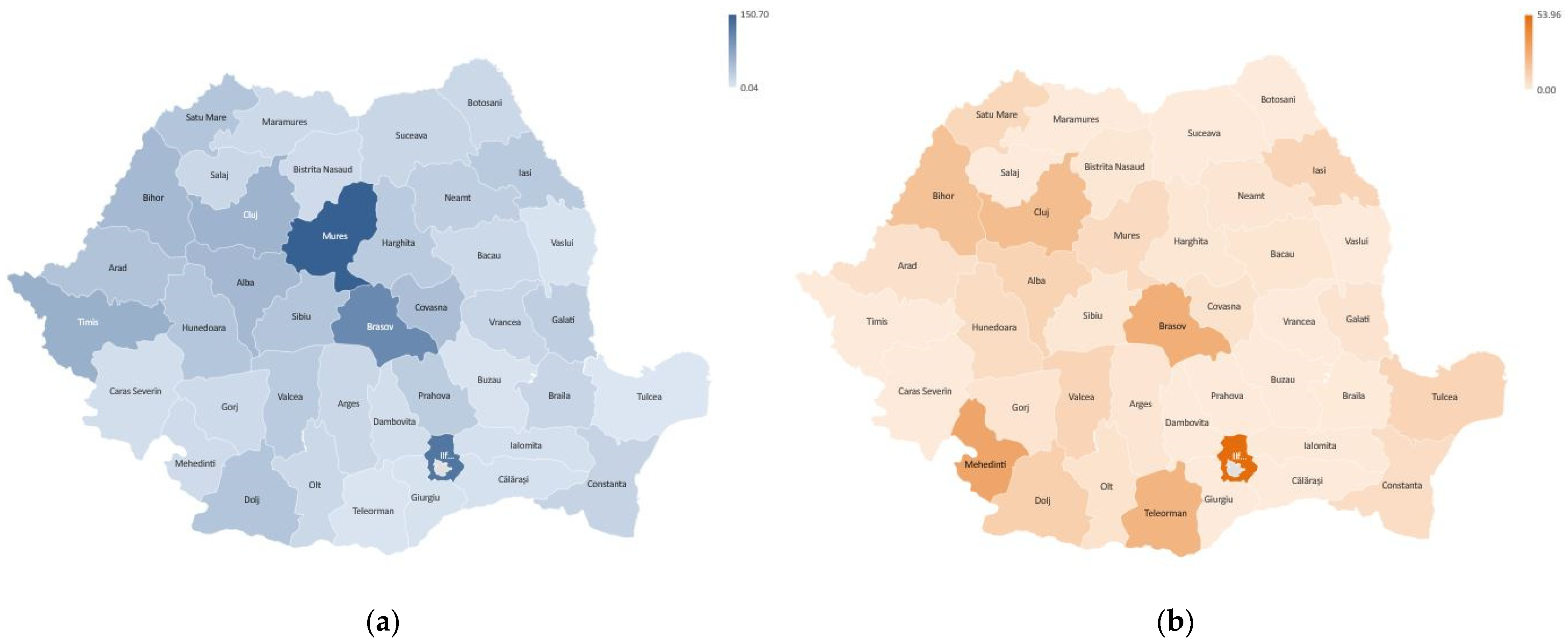
3.4. Regional Prevalence
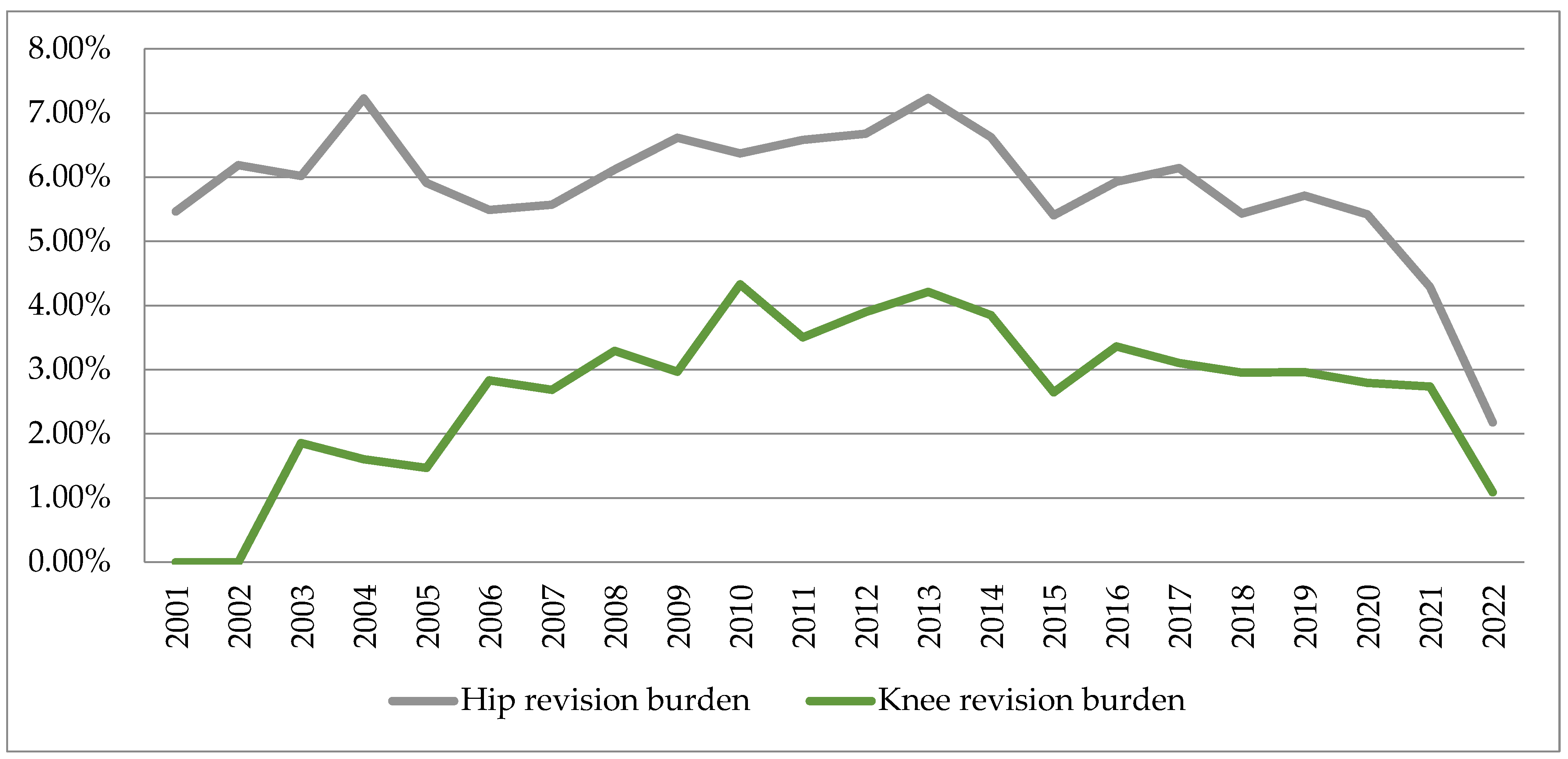
3.5. Revision Burden
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 |
| Hip replacement surgery (nHrs) | |||||||||||||||||||||
| 3312 | 5236 | 5947 | 5922 | 6345 | 7141 | 7286 | 8974 | 8891 | 8869 | 8859 | 8973 | 9814 | 10,401 | 10,546 | 11,554 | 11,705 | 11,893 | 12,134 | 7933 | 9471 | 8675 |
| Total Hip Arthroplasty (nTHA) | |||||||||||||||||||||
| 2252 | 3288 | 3594 | 3719 | 4091 | 4738 | 5004 | 6128 | 6022 | 5710 | 5631 | 5887 | 6544 | 7093 | 7064 | 7838 | 8020 | 8125 | 8546 | 5163 | 6793 | 6693 |
| Cemented Total Hip Arthroplasty (nCTHA) | |||||||||||||||||||||
| 1690 | 2295 | 2495 | 2576 | 2778 | 2915 | 2784 | 3190 | 3089 | 2755 | 2663 | 2812 | 2797 | 2891 | 2620 | 2786 | 2707 | 2610 | 2424 | 1230 | 1665 | 1356 |
| Uncemented Total Hip Arthroplasty (nUTHA) | |||||||||||||||||||||
| 521 | 940 | 1006 | 1048 | 1216 | 1712 | 2106 | 2827 | 2792 | 2655 | 2426 | 2571 | 3086 | 3569 | 3696 | 4263 | 4559 | 4791 | 5294 | 3480 | 4506 | 4722 |
| Hybrid and Reverse Hybrid Total Hip Arthroplasty (nHTHA) | |||||||||||||||||||||
| 41 | 53 | 93 | 95 | 97 | 111 | 114 | 111 | 141 | 300 | 542 | 504 | 661 | 633 | 748 | 789 | 754 | 724 | 828 | 453 | 622 | 615 |
| Bipolar Hemiarthroplasty (nBH) | |||||||||||||||||||||
| 268 | 456 | 481 | 415 | 378 | 519 | 426 | 519 | 516 | 561 | 589 | 563 | 581 | 653 | 718 | 953 | 1312 | 1399 | 1525 | 1365 | 1312 | 1048 |
| Unipolar Hemiarthroplasty—Moore type (nUH) | |||||||||||||||||||||
| 792 | 1492 | 1872 | 1788 | 1876 | 1884 | 1856 | 2327 | 2353 | 2598 | 2639 | 2523 | 2689 | 2655 | 2764 | 2763 | 2373 | 2369 | 2063 | 1405 | 1366 | 934 |
| Hip replacement surgery—male (nHrsM) | |||||||||||||||||||||
| 1286 | 2065 | 2294 | 2299 | 2607 | 2823 | 2904 | 3662 | 3563 | 3552 | 3718 | 3681 | 3990 | 4235 | 4274 | 4756 | 4916 | 5037 | 5267 | 3303 | 4024 | 3934 |
| Hip replacement surgery—female (nHrsF) | |||||||||||||||||||||
| 2026 | 3171 | 3653 | 3623 | 3738 | 4318 | 4382 | 5312 | 5328 | 5317 | 5141 | 5292 | 5824 | 6166 | 6272 | 6798 | 6789 | 6856 | 6867 | 4630 | 5447 | 4741 |
| Knee replacement surgery (nKrs) | |||||||||||||||||||||
| 0 | 27 | 377 | 499 | 613 | 883 | 1154 | 1761 | 1854 | 1685 | 1598 | 1822 | 2255 | 2625 | 3061 | 3958 | 4222 | 4844 | 5704 | 3221 | 3908 | 4964 |
| Bicondylar Knee Arthroplasty (nBKA) | |||||||||||||||||||||
| 0 | 6 | 332 | 469 | 590 | 848 | 1111 | 1684 | 1796 | 1629 | 1538 | 1775 | 2213 | 2580 | 3013 | 3913 | 4202 | 4781 | 5591 | 3141 | 3800 | 4880 |
| Unicondylar Knee Arthroplasty (nUKA) | |||||||||||||||||||||
| 0 | 21 | 45 | 30 | 23 | 35 | 43 | 77 | 58 | 56 | 60 | 47 | 42 | 45 | 48 | 45 | 20 | 63 | 113 | 80 | 108 | 84 |
| Knee replacement surgery—male (nKrsM) | |||||||||||||||||||||
| 0 | 4 | 87 | 118 | 139 | 209 | 275 | 448 | 438 | 390 | 349 | 405 | 525 | 628 | 703 | 916 | 954 | 1128 | 1322 | 778 | 972 | 1248 |
| Knee replacement surgery—female (nKrsF) | |||||||||||||||||||||
| 0 | 23 | 290 | 381 | 474 | 674 | 879 | 1313 | 1416 | 1295 | 1249 | 1417 | 1730 | 1997 | 2358 | 3042 | 3268 | 3716 | 4382 | 2443 | 2936 | 3716 |
| Revision Hip Arthroplasty (nRHA) | |||||||||||||||||||||
| 181 | 324 | 358 | 428 | 375 | 392 | 406 | 549 | 588 | 565 | 583 | 599 | 710 | 689 | 570 | 685 | 719 | 646 | 693 | 430 | 406 | 189 |
| Revision Knee Arthroplasty (nRKA) | |||||||||||||||||||||
| 0 | 0 | 7 | 8 | 9 | 25 | 31 | 58 | 55 | 73 | 56 | 71 | 95 | 101 | 81 | 133 | 131 | 143 | 169 | 90 | 107 | 54 |
| Operated fractures—upper limb, lower limb, pelvis (nOf) | |||||||||||||||||||||
| 15,661 | 24,209 | 26,342 | 31,021 | 28,438 | 30,220 | 30,125 | 28,926 | 26,337 | 29,783 | 32,897 | 29,892 | 28,818 | 26,156 | 28,491 | 25,521 | 22,533 | 23,149 | 18,639 | 14,717 | 11,637 | 7928 |
| Operated bone tumors—upper limb, lower limb, pelvis (nObt) | |||||||||||||||||||||
| 884 | 1109 | 1096 | 1145 | 1129 | 1213 | 1102 | 860 | 691 | 844 | 883 | 875 | 753 | 750 | 816 | 610 | 592 | 474 | 296 | 117 | 115 | 64 |
| Hospitalized patients (nHp) | |||||||||||||||||||||
| 63,399 | 85,682 | 96,460 | 98,394 | 83,617 | 85,197 | 78,146 | 87,170 | 79,374 | 92,661 | 83,782 | 77,765 | 80,728 | 77,763 | 71,783 | 66,748 | 61,481 | 60,091 | 50,321 | 29,564 | 29,122 | 17,999 |
| Operated patients (nOp) | |||||||||||||||||||||
| 33,418 | 48,932 | 55,636 | 61,938 | 55,385 | 55,124 | 53,397 | 59,698 | 54,083 | 62,560 | 60,216 | 58,322 | 60,909 | 57,568 | 57,606 | 53,626 | 51,487 | 46,109 | 40,502 | 25,959 | 24,296 | 16,331 |
References
- Jameson, S.S.; Mason, J.M.; Baker, P.N.; Jettoo, P.; Deehan, D.J.; Reed, M.R. Factors influencing revision risk following 15,740 single-brand hybrid hip arthroplasties: A cohort study from a National Joint Registry. J. Arthroplast. 2013, 28, 1152–1159.e1. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M.; Liu, Y.L.; Graves, S.; de Steiger, R. What Is the Rerevision Rate after Revising a Hip Resurfacing Arthroplasty? Analysis from the AOANJRR. Clin. Orthop. Relat. Res. 2015, 473, 3458–3464. [Google Scholar] [CrossRef] [PubMed]
- Abdelaal, M.S.; Restrepo, C.; Sharkey, P.F. Global Perspectives on Arthroplasty of Hip and Knee Joints. Orthop. Clin. N. Am. 2020, 51, 169–176. [Google Scholar] [CrossRef]
- Malchau, H.; Garellick, G.; Berry, D.; Harris, W.H.; Robertson, O.; Kärrlholm, J.; Lewallen, D.; Bragdon, C.R.; Lidgren, L.; Herberts, P. Arthroplasty implant registries over the past five decades: Development, current, and future impact. J. Orthop. Res. 2018, 36, 2319–2330. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, C.; Bridgens, A.; Berghold, A.; Wurzer, P.; Boehler, N.; Labek, G. Quality of outcome data in total hip arthroplasty: Comparison of registry data and worldwide non-registry studies from 5 decades. Hip Int. 2015, 25, 394–401. [Google Scholar] [CrossRef]
- The National Endoprosthesis Registry. Available online: https://www.rne.ro/rne/informatii/ (accessed on 26 March 2023).
- Ministry of Health. Order No. 1110 of 30 December 2010. Published in M.Of. nr. 53/21 January 2011. Available online: https://www.cdep.ro/pls/legis/legis_pck.htp_act?ida=101357 (accessed on 26 March 2023).
- Bhandari, M.; Smith, J.; Miller, L.E.; Block, J.E. Clinical and economic burden of revision knee arthroplasty. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2012, 5, 89–94. [Google Scholar] [CrossRef]
- Li, C.S.; Bhandari, M. Cost-effectiveness of unicompartmental knee arthroplasty, high tibial osteotomy, and KineSpring® Knee Implant System for unicompartmental osteoarthritis of the knee. J. Long. Term. Eff. Med. Implant. 2013, 23, 189–198. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J. Impact of the economic downturn on total joint replacement demand in the United States: Updated projections to 2021. J. Bone Joint Surg. Am. 2014, 96, 624–630. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Joint Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Mont, M.A.; Issa, K. Updated projections of total joint arthroplasty demands in America. Commentary on an article by Steven M. Kurtz, PhD; et al.: “Impact of the Economic Downturn on Total Joint Replacement Demand in the United States. Updated Projections to 2021”. J. Bone Joint Surg. Am. 2014, 96, e68. [Google Scholar] [CrossRef]
- Sanders, T.L.; MaraditKremers, H.; Schleck, C.D.; Larson, D.R.; Berry, D.J. Subsequent Total Joint Arthroplasty after Primary Total Knee or Hip Arthroplasty: A 40-Year Population-Based Study. J. Bone Joint Surg. Am. 2017, 99, 396–401. [Google Scholar] [CrossRef]
- Matsuoka, H.; Nanmo, H.; Nojiri, S.; Nagao, M.; Nishizaki, Y. Projected numbers of knee and hip arthroplasties up to the year 2030 in Japan. J. Orthop. Sci. 2023, 28, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Ripollés-Melchor, J.; Abad-Motos, A.; Díez-Remesal, Y.; Aseguinolaza-Pagola, M.; Padin-Barreiro, L.; Sánchez-Martín, R.; Logroño-Egea, M.; Catalá-Bauset, J.C.; García-Orallo, S.; Bisbe, E.; et al. Association between Use of Enhanced Recovery after Surgery Protocol and Postoperative Complications in Total Hip and Knee Arthroplasty in the Postoperative Outcomes within Enhanced Recovery after Surgery Protocol in Elective Total Hip and Knee Arthroplasty Study (POWER2). JAMA Surg. 2020, 155, e196024. [Google Scholar] [PubMed]
- Memtsoudis, S.G.; Fiasconaro, M.; Soffin, E.M.; Liu, J.; Wilson, L.A.; Poeran, J.; Bekeris, J.; Kehlet, H. Enhanced recovery after surgery components and perioperative outcomes: A nationwide observational study. Br. J. Anaesth. 2020, 124, 638–647. [Google Scholar] [CrossRef]
- Soffin, E.M.; YaDeau, J.T. Enhanced recovery after surgery for primary hip and knee arthroplasty: A review of the evidence. Br. J. Anaesth. 2016, 117, iii62–iii72. [Google Scholar] [CrossRef]
- Soffin, E.M.; Wainwright, T.W. Hip and Knee Arthroplasty. Anesthesiol. Clin. 2022, 40, 73–90. [Google Scholar] [CrossRef]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L., Jr. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35, S79–S85. [Google Scholar] [CrossRef]
- Roth, A.; Ghanem, M.; Fakler, J. Patellafrakturen in der Knieendoprothetik. Orthopade 2016, 45, 416–424. [Google Scholar] [CrossRef]
- Steinmetz, S.; Brügger, A.; Chauveau, J.; Chevalley, F.; Borens, O.; Thein, E. Practical guidelines for the treatment of patellar fractures in adults. Swiss Med. Wkly. 2020, 150, w20165. [Google Scholar] [CrossRef]
- Sevimli, R.; Korkmaz, M.F. Analysis of orthopedic surgery of patients with metastatic bone tumors and pathological fractures. J. Int. Med. Res. 2018, 46, 3262–3267. [Google Scholar] [CrossRef]
- Bartelstein, M.K.; Boland, P.J. Fifty years of bone tumors. J. Surg. Oncol. 2022, 126, 906–912. [Google Scholar] [CrossRef]
- Ong, K.L.; Mowat, F.S.; Chan, N.; Lau, E.; Halpern, M.T.; Kurtz, S.M. Economic burden of revision hip and knee arthroplasty in Medicare enrollees. Clin. Orthop. Relat. Res. 2006, 446, 22–28. [Google Scholar] [CrossRef]
- Piscitelli, P.; Iolascon, G.; Di Tanna, G.; Bizzi, E.; Chitano, G.; Argentiero, A.; Neglia, C.; Giolli, L.; Distante, A.; Gimigliano, R.; et al. Socioeconomic burden of total joint arthroplasty for symptomatic hip and knee osteoarthritis in the Italian population: A 5-year analysis based on hospitalization records. Arthritis Care Res. 2012, 64, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Iorio, R.; Davis, C.M., 3rd; Healy, W.L.; Fehring, T.K.; O’Connor, M.I.; York, S. Impact of the economic downturn on adult reconstruction surgery: A survey of the American Association of Hip and Knee Surgeons. J. Arthroplast. 2010, 25, 1005–1014. [Google Scholar] [CrossRef]
- Kurtz, S.; Mowat, F.; Ong, K.; Chan, N.; Lau, E.; Halpern, M. Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002. J. Bone Joint Surg. Am. 2005, 87, 1487–1497. [Google Scholar] [PubMed]
- Katano, H.; Ozeki, N.; Kohno, Y.; Nakagawa, Y.; Koga, H.; Watanabe, T.; Jinno, T.; Sekiya, I. Trends in arthroplasty in Japan by a complete survey, 2014–2017. J. Orthop. Sci. 2021, 26, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Melvin, J.S.; Karthikeyan, T.; Cope, R.; Fehring, T.K. Early failures in total hip arthroplasty—A changing paradigm. J. Arthroplast. 2014, 29, 1285–1288. [Google Scholar] [CrossRef] [PubMed]
- Bryan, R.S.; Rand, J.A. Revision total knee arthroplasty. Clin. Orthop. Relat. Res. 1982, 170, 116–122. [Google Scholar] [CrossRef]
- Siqueira, M.B.; Klika, A.K.; Higuera, C.A.; Barsoum, W.K. Modes of failure of total knee arthroplasty: Registries and realities. J. Knee Surg. 2015, 28, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Malchau, H.; Herberts, P.; Eisler, T.; Garellick, G.; Söderman, P. The Swedish Total Hip Replacement Register. J. Bone Joint Surg. Am. 2002, 84, 2–20, Erratum in: J. Bone Joint Surg. Am. 2004, 86, 363. [Google Scholar] [CrossRef]
- Liebs, T.R.; Splietker, F.; Hassenpflug, J. Is a Revision a Revision? An Analysis of National Arthroplasty Registries’ Definitions of Revision. Clin. Orthop. Relat. Res. 2015, 473, 3421–3430. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, C.; Lumenta, D.B.; Cupak, D.; Berghold, A.; Boehler, N.; Labek, G. Quality of outcome data in knee arthroplasty. Acta Orthop. 2015, 86, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.L.; Jiranek, W.A.; Hayes, C.W. Use of a validated algorithm to judge the appropriateness of total knee arthroplasty in the United States: A multicenter longitudinal cohort study. Arthritis Rheumatol. 2014, 66, 2134–2143. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Statistics. Population by Gender, by Residence–Counties and Areas. Available online: https://insse.ro/cms/files/RPL2002INS/vol1/titluriv1.htm (accessed on 26 March 2023).
- Smith, L.K.; Dures, E.; Beswick, A.D. Systematic review of the clinical effectiveness for long-term follow-up of total hip arthroplasty. Orthop. Res. Rev. 2019, 11, 69–78. [Google Scholar] [CrossRef]
- Pabinger, C.; Geissler, A. Utilization rates of hip arthroplasty in OECD countries. Osteoarthr. Cartil. 2014, 22, 734–741. [Google Scholar] [CrossRef]
- Price, A.J.; Alvand, A.; Troelsen, A.; Katz, J.N.; Hooper, G.; Gray, A.; Carr, A.; Beard, D. Knee replacement. Lancet 2018, 392, 1672–1682. [Google Scholar] [CrossRef] [PubMed]
- Sattler, L.; Hing, W.; Vertullo, C. Changes to rehabilitation after total knee replacement. Aust. J. Gen. Pract. 2020, 49, 587–591. [Google Scholar] [CrossRef]
- Pabinger, C.; Lothaller, H.; Geissler, A. Utilization rates of knee-arthroplasty in OECD countries. Osteoarthr. Cartil. 2015, 23, 1664–1673. [Google Scholar] [CrossRef]
- Falbrede, I.; Widmer, M.; Kurtz, S.; Schneidmüller, D.; Dudda, M.; Röder, C. Verwendungsraten von Prothesen der unterenExtremität in Deutschland und der Schweiz: Ein Vergleich der Jahre 2005–2008. Orthopade 2011, 40, 793–801. [Google Scholar] [CrossRef]
- de Steiger, R.N.; Hang, J.R.; Miller, L.N.; Graves, S.E.; Davidson, D.C. Five-year results of the ASR XL Acetabular System and the ASR Hip Resurfacing System: An analysis from the Australian Orthopaedic Association National Joint Replacement Registry. J. Bone Joint Surg. Am. 2011, 93, 2287–2293. [Google Scholar] [CrossRef]
- McGrory, B.J.; MacKenzie, J.; Babikian, G. A High Prevalence of Corrosion at the Head-Neck Taper with Contemporary Zimmer Non-Cemented Femoral Hip Components. J. Arthroplast. 2015, 30, 1265–1268. [Google Scholar] [CrossRef]
- Shao, R.; Wang, Y.; Li, L.; Dong, Y.; Zhao, J.; Liang, W. Bone tumors effective therapy through functionalized hydrogels: Current developments and future expectations. Drug. Deliv. 2022, 29, 1631–1647. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.R.; Kumar, T.S.S.; Jayakrishnan, A. Nanocarrier-based drug delivery systems for bone cancer therapy: A review. Biomed. Mater. 2021, 16, 044107. [Google Scholar] [CrossRef]
- Liao, J.; Han, R.; Wu, Y.; Qian, Z. Review of a new bone tumor therapy strategy based on bifunctional biomaterials. Bone Res. 2021, 9, 18. [Google Scholar] [CrossRef]
- Novicoff, W.M.; Saleh, K.J. Examining sex and gender disparities in total joint arthroplasty. Clin. Orthop. Relat. Res. 2011, 469, 1824–1828. [Google Scholar] [CrossRef]
- Kawata, M.; Sasabuchi, Y.; Inui, H.; Taketomi, S.; Matsui, H.; Fushimi, K.; Chikuda, H.; Yasunaga, H.; Tanaka, S. Annual trends in knee arthroplasty and tibial osteotomy: Analysis of a national database in Japan. Knee 2017, 24, 1198–1205. [Google Scholar] [CrossRef]
- Koh, I.J.; Kim, M.W.; Kim, J.H.; Han, S.Y.; In, Y. Trends in High Tibial Osteotomy and Knee Arthroplasty Utilizations and Demographics in Korea from 2009 to 2013. J. Arthroplast. 2015, 30, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Best, J.T. Revision total hip and total knee arthroplasty. Orthop. Nurs. 2005, 24, 174–179. [Google Scholar] [CrossRef]
- McGrory, B.J.; Etkin, C.D.; Lewallen, D.G. Comparing contemporary revision burden among hip and knee joint replacement registries. Arthroplast. Today 2016, 2, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Sabah, S.A.; Henckel, J.; Koutsouris, S.; Rajani, R.; Hothi, H.; Skinner, J.A.; Hart, A.J. Are all metal-on-metal hip revision operations contributing to the National Joint Registry implant survival curves? A study comparing the London Implant Retrieval Centre and National Joint Registry datasets. Bone Joint J. 2016, 98, 33–39. [Google Scholar] [CrossRef]
- Moldovan, F.; Gligor, A.; Moldovan, L.; Bataga, T. The Impact of the COVID-19 Pandemic on the Orthopedic Residents: A Pan-Romanian Survey. Int. J. Environ. Res. Public Health 2022, 19, 9176. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F.; Gligor, A.; Moldovan, L.; Bataga, T. An Investigation for Future Practice of Elective Hip and Knee Arthroplasties during COVID-19 in Romania. Medicina 2023, 59, 314. [Google Scholar] [CrossRef] [PubMed]









| Hip Replacement Surgery | Knee Replacement Surgery | Revision Hip Arthroplasty | Revision Knee Arthroplasty | Operated Fractures | Operated Bone Tumors | Hospitalized Patients | Operated Patients |
|---|---|---|---|---|---|---|---|
| 189,881 | 51,035 | 11,085 | 1497 | 541,440 | 16,418 | 1,557,247 | 1,093,102 |
| Orthopedic Interventions | Variation Trends | |
|---|---|---|
| Including Pandemic [%] | Without Pandemic [%] | |
| Hip replacement surgery (Hrs) | 5.89 | 8.19 |
| Total hip arthroplasty (THA) | 6.59 | 8.21 |
| Cemented total hip arthroplasty (CTHA) | 0.6 | 2.51 |
| Uncemented total hip arthroplasty (UTHA) | 13.05 | 15.22 |
| Hybrid and reverse hybrid total hip arthroplasty (HTHA) | 0.18 | 0.22 |
| Bipolar hemiarthroplasty (BH) | 0.09 | 0.12 |
| Unipolar hemiarthroplasty—Moore type (UH) | 0.03 | 0.07 |
| Hip replacement surgery—male (HrsM) | 0.07 | 0.09 |
| Hip replacement surgery—female (HrsF) | 0.05 | 0.08 |
| Knee replacement surgery (Krs) | 16.72 | 19.55 |
| Bicondylar knee arthroplasty (BKA) | 17.48 | 20.41 |
| Unicondylar knee arthroplasty (UKA) | 14.43 | 18.16 |
| Knee replacement surgery—male (KrsM) | 17.57 | 20.87 |
| Knee replacement surgery—female (KrsF) | 16.48 | 19.57 |
| Revision hip arthroplasty (RHA) | 3.46 | 9.43 |
| Revision knee arthroplasty (RKA) | 19.98 | 28.57 |
| Operated fractures (Of) | −1.73 | 2.08 |
| Operated bone tumors (Obt) | −8.95 | −4.52 |
| Hospitalized patients (Hp) | −4.33 | −0.56 |
| Operated patients (Op) | −1.96 | −1.89 |
| 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hip | |||||||||||
| Primary | 3312 | 5236 | 5947 | 5922 | 6345 | 7141 | 7286 | 8974 | 8891 | 8869 | 8859 |
| Revision | 181 | 324 | 358 | 428 | 375 | 392 | 406 | 549 | 588 | 565 | 583 |
| Revision burden | 5.46 | 6.18 | 6.01 | 7.22 | 5.91 | 5.48 | 5.57 | 6.11 | 6.61 | 6.37 | 6.58 |
| Knee | |||||||||||
| Primary | 0 | 27 | 377 | 499 | 613 | 883 | 1154 | 1761 | 1854 | 1685 | 1598 |
| Revision | 0 | 0 | 7 | 8 | 9 | 25 | 31 | 58 | 55 | 73 | 56 |
| Revision burden | 0 | 0 | 1.85 | 1.60 | 1.46 | 2.83 | 2.68 | 3.29 | 2.96 | 4.33 | 3.50 |
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
| Hip | |||||||||||
| Primary | 8973 | 9814 | 10,401 | 10,546 | 11,554 | 11,705 | 11,893 | 12,134 | 7933 | 9471 | 8675 |
| Revision | 599 | 710 | 689 | 570 | 685 | 719 | 646 | 693 | 430 | 406 | 189 |
| Revision burden | 6.67 | 7.23 | 6.62 | 5.40 | 5.92 | 6.14 | 5.43 | 5.71 | 5.42 | 4.28 | 2.17 |
| Knee | |||||||||||
| Primary | 1822 | 2255 | 2625 | 3061 | 3958 | 4222 | 4844 | 5704 | 3221 | 3908 | 4964 |
| Revision | 71 | 95 | 101 | 81 | 133 | 131 | 143 | 169 | 90 | 107 | 54 |
| Revision burden | 3.89 | 4.21 | 3.84 | 2.64 | 3.36 | 3.10 | 2.95 | 2.96 | 2.79 | 2.73 | 1.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moldovan, F.; Moldovan, L.; Bataga, T. A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania. Healthcare 2023, 11, 1866. https://doi.org/10.3390/healthcare11131866
Moldovan F, Moldovan L, Bataga T. A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania. Healthcare. 2023; 11(13):1866. https://doi.org/10.3390/healthcare11131866
Chicago/Turabian StyleMoldovan, Flaviu, Liviu Moldovan, and Tiberiu Bataga. 2023. "A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania" Healthcare 11, no. 13: 1866. https://doi.org/10.3390/healthcare11131866
APA StyleMoldovan, F., Moldovan, L., & Bataga, T. (2023). A Comprehensive Research on the Prevalence and Evolution Trend of Orthopedic Surgeries in Romania. Healthcare, 11(13), 1866. https://doi.org/10.3390/healthcare11131866