


The Facial Characteristics of Individuals with Posterior Crossbite: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Methodology
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- Patients with posterior crossbites have increased face height compared to those without crossbites.
- Crossbite may interfere with associational patterns of the facial structures.
- Crossbite, if left untreated, may alter the parameters of the face.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Altorkat, Y.; Khambay, B.S.; McDonald, J.P.; Cross, D.L.; Brocklebank, L.M.; Ju, X. Immediate effects of rapid maxillary expansion on the naso-maxillary facial soft tissue using 3D stereophotogrammetry. Surgeon 2016, 14, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Claes, P.; Roosenboom, J.; White, J.D.; Swigut, T.; Sero, D.; Li, J.; Lee, M.K.; Zaidi, A.; Mattern, B.C.; Liebowitz, C.; et al. Genome-wide mapping of global-to-local genetic effects on human facial shape. Nat. Genet. 2018, 50, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Hoskens, H.; Liu, D.; Naqvi, S.; Lee, M.K.; Eller, R.J.; Indencleef, K.; White, J.D.; Li, J.; Larmuseau, M.H.D.; Hens, G.; et al. 3D facial phenotyping by biometric sibling matching used in contemporary genomic methodologies. PLoS Genet. 2021, 17, e1009528. [Google Scholar] [CrossRef]
- Richmond, S.; Howe, L.J.; Lewis, S.; Stergiakouli, E.; Zhurov, A. Facial Genetics: A Brief Overview. Front. Genet. 2018, 9, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, J.B.; Manyama, M.; Larson, J.R.; Liberton, D.K.; Ferrara, T.M.; Riccardi, S.L.; Li, M.; Mio, W.; Klein, O.D.; Santorico, S.A.; et al. Human Facial Shape and Size Heritability and Genetic Correlations. Genetics. 2017, 205, 967–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djordjevic, J.; Zhurov, A.I.; Richmond, S.; Visigen Consortium. Genetic and Environmental Contributions to Facial Morphological Variation: A 3D Population-Based Twin Study. PLoS ONE 2016, 11, e0162250. [Google Scholar] [CrossRef] [Green Version]
- Daskalogiannakis, J. Glossary of Orthodontic Terms; Quintessence Publishing: Chicago, IL, USA, 2000; pp. 85–88. [Google Scholar]
- Iodice, G.; Danzi, G.; Cimino, R.; Paduano, S.; Michelotti, A. Association between posterior crossbite, skeletal, and muscle asymmetry: A systematic review. Eur. J. Orthod. 2016, 38, 638–651. [Google Scholar] [CrossRef] [Green Version]
- Ugolini, A.; Agostino, P.; Silvestrini-Biavati, A.; Harrison, J.E.; Batista, K.B. Orthodontic treatment for posterior crossbites. Cochrane Database Syst. Rev. 2021, 12, CD000979. [Google Scholar]
- Grippaudo, C.; Paolantonio, E.G.; Antonini, G.; Saulle, R.; La Torre, G.; Deli, R. Association between oral habits, mouth breathing and malocclusion. Acta Otorhinolaryngol. Ital. 2016, 36, 386–394. [Google Scholar] [CrossRef]
- Al Ali, A.; Richmond, S.; Popat, H.; Toma, A.M.; Playle, R.; Zhurov, A.I.; Marshall, D.; Rosin, P.L.; Henderson, J. The influence of asthma on face shape: A three-dimensional study. Eur. J. Orthod. 2014, 36, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Al Ali, A.; Richmond, S.; Popat, H.; Playle, R.; Pickles, T.; Zhurov, A.I.; Marshall, D.; Rosin, P.L.; Henderson, J.; Bonuck, K. The influence of snoring, mouth breathing and apnoea on facial morphology in late childhood: A three-dimensional study. BMJ Open 2015, 5, e009027. [Google Scholar] [CrossRef]
- Baysal, A.; Ozturk, M.A.; Sahan, A.O.; Uysal, T. Facial soft-tissue changes after rapid maxillary expansion analyzed with 3-dimensional stereophotogrammetry: A randomized, controlled clinical trial. Angle Orthod. 2016, 86, 934–942. [Google Scholar] [CrossRef] [Green Version]
- Venezia, P.; Nucci, L.; Moschitto, S.; Malgioglio, A.; Isola, G.; Ronsivalle, V.; Venticinque, V.; Leonardi, R.; Lagraverè, M.O.; Lo Giudice, A. Short-Term and Long-Term Changes of Nasal Soft Tissue after Rapid Maxillary Expansion (RME) with Tooth-Borne and Bone-Borne Devices. A CBCT Retrospective Study. Diagnostics 2022, 12, 875. [Google Scholar] [CrossRef] [PubMed]
- Akan, B.; Gökçe, G.; Şahan, A.O.; Veli, İ. Tooth-borne versus tooth-bone-borne rapid maxillary expanders according to a stereophotogrammetric evaluation of facial soft tissues: A randomized clinical trial. Orthod. Craniofac. Res. 2021, 24, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Alkhayer, A.; Becsei, R.; Hegedűs, L.; Párkányi, L.; Piffkó, J.; Braunitzer, G.; Segatto, E. Evaluation of the Soft Tissue Changes after Rapid Maxillary Expansion Using a Handheld Three-Dimensional Scanner: A Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3379. [Google Scholar] [CrossRef]
- Altındiş, S.; Toy, E.; Başçiftçi, F.A. Effects of different rapid maxillary expansion appliances on facial soft tissues using three-dimensional imaging. Angle Orthod. 2016, 86, 590–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richmond, S.; Zhurov, A.I.; Ali, A.B.M.; Pirttiniemi, P.; Heikkinen, T.; Harila, V.; Silinevica, S.; Jakobsone, G.; Urtane, I. Exploring the midline soft tissue surface changes from 12 to 15 years of age in three distinct country population cohorts. Eur. J. Orthod. 2020, 42, 517–524. [Google Scholar] [CrossRef]
- Kesterke, M.J.; Raffensperger, Z.D.; Heike, C.L.; Cunningham, M.L.; Hecht, J.T.; Kau, C.H.; Nidey, N.L.; Moreno, L.M.; Wehby, G.L.; Marazita, M.L.; et al. Using the 3D Facial Norms Database to investigate craniofacial sexual dimorphism in healthy children, adolescents, and adults. Biol. Sex. Differ. 2016, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Assy, Z.; Jager, D.H.J.; Brand, H.S.; Bikker, F.J. Correlations of palatal surface area with anthropometric dimensions of the head and face. Surg. Radiol. Anat. 2022, 44, 1261–1267. [Google Scholar] [CrossRef]
- Matthews, H.S.; Penington, A.J.; Hardiman, R.; Fan, Y.; Clement, J.G.; Kilpatrick, N.M.; Claes, P.D. Modelling 3D craniofacial growth trajectories for population comparison and classification illustrated using sex-differences. Sci. Rep. 2018, 8, 4771. [Google Scholar] [CrossRef] [Green Version]
- Farkas, L.G. Anthropometry of the Head and Face, 2nd ed.; Raven Press: New York, NY, USA, 1994; pp. 20–46. [Google Scholar]
- Toma, A.M.; Zhurov, A.; Playle, R.; Ong, E.; Richmond, S. Reproducibility of facial soft tissue landmarks on 3D laser-scanned facial images. Orthod. Craniofac. Res. 2009, 12, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.; Mohamed, A.S.; Habumugisha, J.; Guo, Y.; Zou, R.; Wang, F. A Study of the Facial Soft Tissue Morphology in Nasal- and Mouth-Breathing Patients. Int. Dent. J. 2023, 73, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Allen, D.; Rebellato, J.; Sheats, R.; Ceron, A.M. Skeletal and dental contributions to posterior crossbites. Angle Orthod. 2003, 73, 515–524. [Google Scholar]
- Saadeh, M.E.; Haddad, R.V.; Ghafari, J.G. Morphometric analysis of palatal rugae in different malocclusions. J. Orofac. Orthop. 2021, 82, 111–120. [Google Scholar] [CrossRef]
- Yap, B.; Kontos, A.; Pamula, Y.; Martin, J.; Kennedy, D.; Sampson, W.; Dreyer, C. Differences in dentofacial morphology in children with sleep disordered breathing are detected with routine orthodontic records. Sleep Med. 2019, 55, 109–114. [Google Scholar] [CrossRef]
- Tsagkrasoulis, D.; Hysi, P.; Spector, T.; Montana, G. Heritability maps of human face morphology through large-scale automated three-dimensional phenotyping. Sci. Rep. 2017, 19, 45885. [Google Scholar] [CrossRef] [Green Version]
- Kairalla, S.A.; Velasco, L.; Bachi, A.L.L.; Yamamoto, L.H.; Cappellette, M., Jr. Evaluation of palatal dimensions in different facial patterns by using digital dental casts. Dental Press J. Orthod. 2022, 27, e222115. [Google Scholar] [CrossRef]
- Burke, P.H.; Hughes-Lawson, C.A. The growth and development of the soft tissues of the human face. J. Anat. 1988, 158, 115–120. [Google Scholar] [PubMed]
- Festa, P.; Mansi, N.; Varricchio, A.M.; Savoia, F.; Calì, C.; Marraudino, C.; De Vincentiis, G.C.; Galeotti, A. Association between upper airway obstruction and malocclusion in mouth-breathing children. Acta Otorhinolaryngol. Ital. 2021, 41, 436–442. [Google Scholar] [CrossRef]
- Lee, K.M.; Hwang, H.S.; Cho, J.H. Comparison of transverse analysis between posteroanterior cephalogram and cone-beam computed tomography. Angle Orthod. 2014, 84, 715–719. [Google Scholar] [CrossRef]
- Djordjevic, J.; Pirttiniemi, P.; Harila, V.; Heikkinen, T.; Toma, A.M.; Zhurov, A.I.; Richmond, S. Three-dimensional longitudinal assessment of facial symmetry in adolescents. Eur. J. Orthod. 2013, 35, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Academy of Pediatric Dentistry. Management of the developing dentition and occlusion in pediatric dentistry. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2021; pp. 408–425. [Google Scholar]

{kind=link}
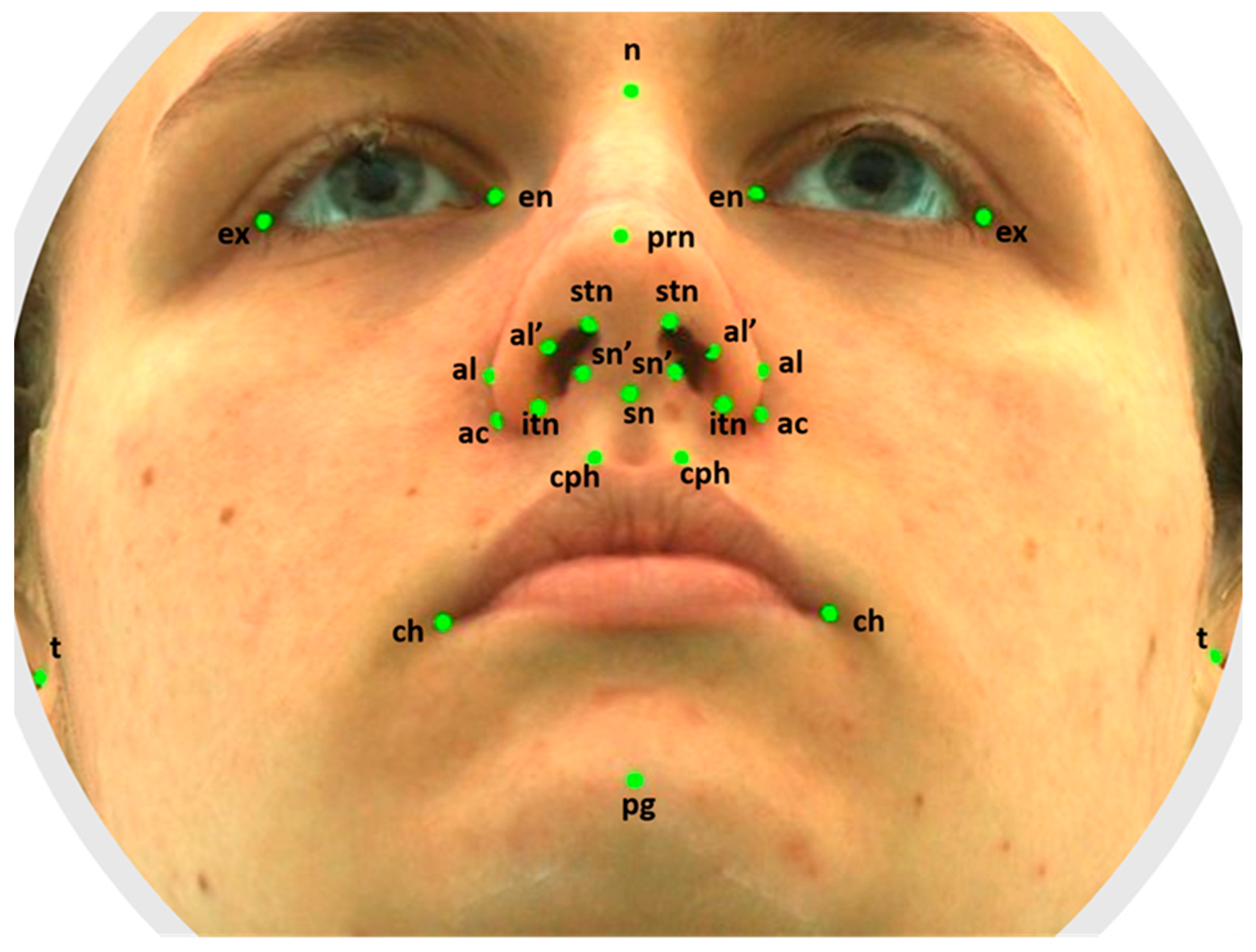
| Landmark | Definition |
|---|---|
| t (tragion) | Notch on the upper margin of the tragus (left and right). |
| n (nasion) | Point in the midline of both the nasal root and the nasofrontal suture. |
| en (endocanthion) | Inner commissure of the eye fissure (left and right). |
| ex (exocanthion) | Outer commissure of the eye fissure (left and right). |
| al (alare) | The most lateral point on alar contour (left and right). |
| ac (alar curvature) | The most lateral point in the curved baseline of ala (left and right). |
| sn (subnasale) | The midpoint of the angle at the columella base where the lower border of the nasal septum and surface of the upper lip meet. |
| prn (pronasale) | The most protruded point of the apex nasi identified in the lateral view of the rest position of the head. |
| al’ (alare’) | Marking level at the midportion of the alae (left and right). |
| sn’ (subnasale’) | The midpoint of the columella crest (left and right). |
| stn | The highest terminal point of the nostril axis (left and right). |
| itn | The lowest terminal point of the nostril axis (left and right). |
| cph (crista philtri) | The point on the elevated margin of the philtrum just above the vermilion line (left and right). |
| ch (cheilion) | The point at labial commissure (left and right). |
| pg (pogonion) | The most anterior midpoint of the chin. |
| Landmarks | Measurements |
|---|---|
| t-t | Facial width. |
| en-en | Intercanthal width. |
| ex-ex | Biocular width. |
| en-ex | Eye fissure length. |
| al-al | Morphological width of the nose. |
| ac-ac | Anatomical width of the nose. |
| n-sn | Height of the nose. |
| sn-prn | Nasal protrusion. |
| al’-sn’ | Nostril width. |
| stn-itn | Nostril height. |
| cph-cph | Width of the philtrum. |
| ch-ch | Width of the mouth. |
| n-pg | Height of the face. |
| Females | Males | Females/Males | ||||||
| Crossbite (n = 22) | Control (n = 22) | p-Value | Crossbite (n = 12) | Control (n = 12) | p-Value | Crossbite | Control | |
| Median (Q1–Q3), mm | Median (Q1–Q3), mm | p-value | ||||||
| t-t | 138.81 (135.95–143.51) | 135.69 (129.9–138.67) | 0.157 | 149.19 (142.75–153.69) | 142.78 (140.1–146.32) | 0.127 | 0.014 | 0.006 |
| en-en | 32.95 (31.19–34.68) | 31.37 (29.20–32.87) | 0.040 | 33.46 (31.33–35.63) | 33.84 (32.66–36.94) | 0.590 | 0.511 | 0.015 |
| ex-ex | 88.25 (86.48–91.03) | 87.71 (85.04–90.50) | 0.453 | 90.45 (88.26–92.63) | 90.70 (88.62–92.26) | 0.932 | 0.031 | 0.011 |
| enR-exR | 28.54 (27.30–29.92) | 29.26 (28.26–30.10) | 0.185 | 29.62 (28.10–30.35) | 29.37 (27.48–30.59) | 0.630 | 0.087 | 1.000 |
| enL-exL | 28.14 (27.12–29.44) | 29.115 (27.87–30.52) | 0.173 | 29.54 (28.02–31.37) | 29.03 (27.39–30.35) | 0.319 | 0.063 | 0.736 |
| alR-alL | 32.54 (30.88–35.02) | 32.445 (30.96–33.33) | 0.213 | 35.40 (33.20–35.98) | 34.71 (33.26–36.08) | 1.000 | 0.094 | <0.001 |
| acR-acL | 32.75 (31.37–33.91) | 30.725 (29.21–32.10) | 0.004 | 34.63 (31.44–35.82) | 33.60 (31.61–35.18) | 0.755 | 0.261 | <0.001 |
| n-sn | 48.09 (47.11–50.06) | 48.16 (44.36–49.87) | 0.425 | 50.40 (48.03–52.32) | 48.77 (46.70–50.45) | 0.219 | 0.136 | 0.363 |
| sn-prn | 19.13 (17.80–20.06) | 19.53 (17.64–20.88) | 0.474 | 20.12 (19.47–21.21) | 19.43 (18.65–19.76) | 0.068 | 0.058 | 0.845 |
| al’R-sn’R | 6.88 (5.90–7.40) | 6.67 (6.18–7.43) | 0.916 | 7.23 (5.98–7.53) | 7.86 (7.29–8.17) | 0.020 | 0.582 | <0.001 |
| al’L-sn’L | 6.73 (6.17–7.54) | 6.83 (6.56–7.14) | 0.833 | 6.56 (6.20–7.74) | 7.75 (7.54–8.28) | 0.028 | 0.817 | <0.001 |
| stnR-itnR | 12.80 (11.49–13.85) | 13.02 (11.95–14.20) | 0.565 | 13.82 (13.51–14.15) | 14.06 (12.93–15.51) | 0.755 | 0.048 | 0.08 |
| stnL-itnL | 13.12 (12.04–14.20) | 13.01 (12.22–14.51) | 0.707 | 13.64 (13.34–15.45) | 14.21 (12.73–15.87) | 0.887 | 0.110 | 0.110 |
| cph-cph | 11.79 (10.54–13.46) | 12.04 (11.01–13.56) | 0.656 | 12.01 (11.09–13.33) | 12.66 (12.00–13.83) | 0.319 | 0.845 | 0.245 |
| ch-ch | 44.28 (42.36–48.03) | 46.63 (42.12–49.00) | 0.241 | 44.20 (41.72–45.75) | 48.06 (43.81–51.08) | 0.078 | 0.657 | 0.363 |
| n-pg | 102.38 (99.32–105.43) | 97.10 (94.63–100.62) | 0.003 | 105.80 (103.03–110.20) | 101.65 (96.06–104.12) | 0.005 | 0.018 | 0.094 |
| t-t ∆ | en-en | ex-ex | al-al | ch-ch | n-pg | cph-cph | n-sn | |
|---|---|---|---|---|---|---|---|---|
| ex-ex | 0.533 *** | 0.347 * | ||||||
| en-en | 0.533 *** | |||||||
| enR-exR | 0.734 *** | |||||||
| enL-exL | 0.819 *** | |||||||
| sn-prn | 0.657 ** | 0.576 *** | 0.462 ** | |||||
| al-al | 0.505 * | 0.347 * | 0.549 *** | 0.510 ** | ||||
| ac-ac | 0.871 *** | 0.511 ** | 0.461 ** | |||||
| al’R-sn’R | 0.457 ** | |||||||
| stnR-itnR | ||||||||
| al’L-sn’L | ||||||||
| stnL-itnL | 0.389 * | 0.462 ** | ||||||
| ch-ch | 0.549 *** | 0.474 ** | −0.408 * | |||||
| cph-cph | 0.510 ** | 0.474 ** | ||||||
| n-sn | −0.408 * | 0.687 *** |
| t-t ∆ | en-en | ex-ex | al-al | ch-ch | n-pg | cph-cph | n-sn | |
|---|---|---|---|---|---|---|---|---|
| ex-ex | 0.718 *** | 0.615 *** | 0.456 ** | 0.394 * | ||||
| en-en | 0.718 *** | 0.448 ** | 0.402 * | 0.349 * | ||||
| enR-exR | 0.385 * | 0.433 * | 0.408 * | |||||
| enL-exL | 0.408 * | 0.424 * | 0.450 ** | |||||
| sn-prn | ||||||||
| al-al | 0.448 ** | 0.615 *** | 0.436 ** | |||||
| ac-ac | 0.547 *** | 0.622 *** | 0.803 *** | 0.454 ** | ||||
| al’R-sn’R | 0.387 * | |||||||
| stnR-itnR | 0.534 *** | |||||||
| al’L-sn’L | 0.413 * | 0.422 * | ||||||
| stnL-itnL | 0.591 *** | 0.445 ** | ||||||
| ch-ch | 0.402 * | 0.456 ** | 0.588 *** | |||||
| cph-cph | 0.349 * | 0.394 * | 0.436 ** | 0.588 *** | ||||
| n-sn | 0.687 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kienkas, K.; Jakobsone, G.; Salms, G. The Facial Characteristics of Individuals with Posterior Crossbite: A Cross-Sectional Study. Healthcare 2023, 11, 1881. https://doi.org/10.3390/healthcare11131881
Kienkas K, Jakobsone G, Salms G. The Facial Characteristics of Individuals with Posterior Crossbite: A Cross-Sectional Study. Healthcare. 2023; 11(13):1881. https://doi.org/10.3390/healthcare11131881
Chicago/Turabian StyleKienkas, Karlina, Gundega Jakobsone, and Girts Salms. 2023. "The Facial Characteristics of Individuals with Posterior Crossbite: A Cross-Sectional Study" Healthcare 11, no. 13: 1881. https://doi.org/10.3390/healthcare11131881
APA StyleKienkas, K., Jakobsone, G., & Salms, G. (2023). The Facial Characteristics of Individuals with Posterior Crossbite: A Cross-Sectional Study. Healthcare, 11(13), 1881. https://doi.org/10.3390/healthcare11131881