
Development of a Set of Indicators for Measuring and Improving Quality of Rehabilitation Care after Ischemic Stroke

 ,
,  , ,
, ,
Abstract
:1. Introduction
1.1. Measuring Stroke Care Performances
1.2. Evaluation and Improvement of Quality in Post-Stroke Rehabilitation
1.3. The EASY-NET Research Program
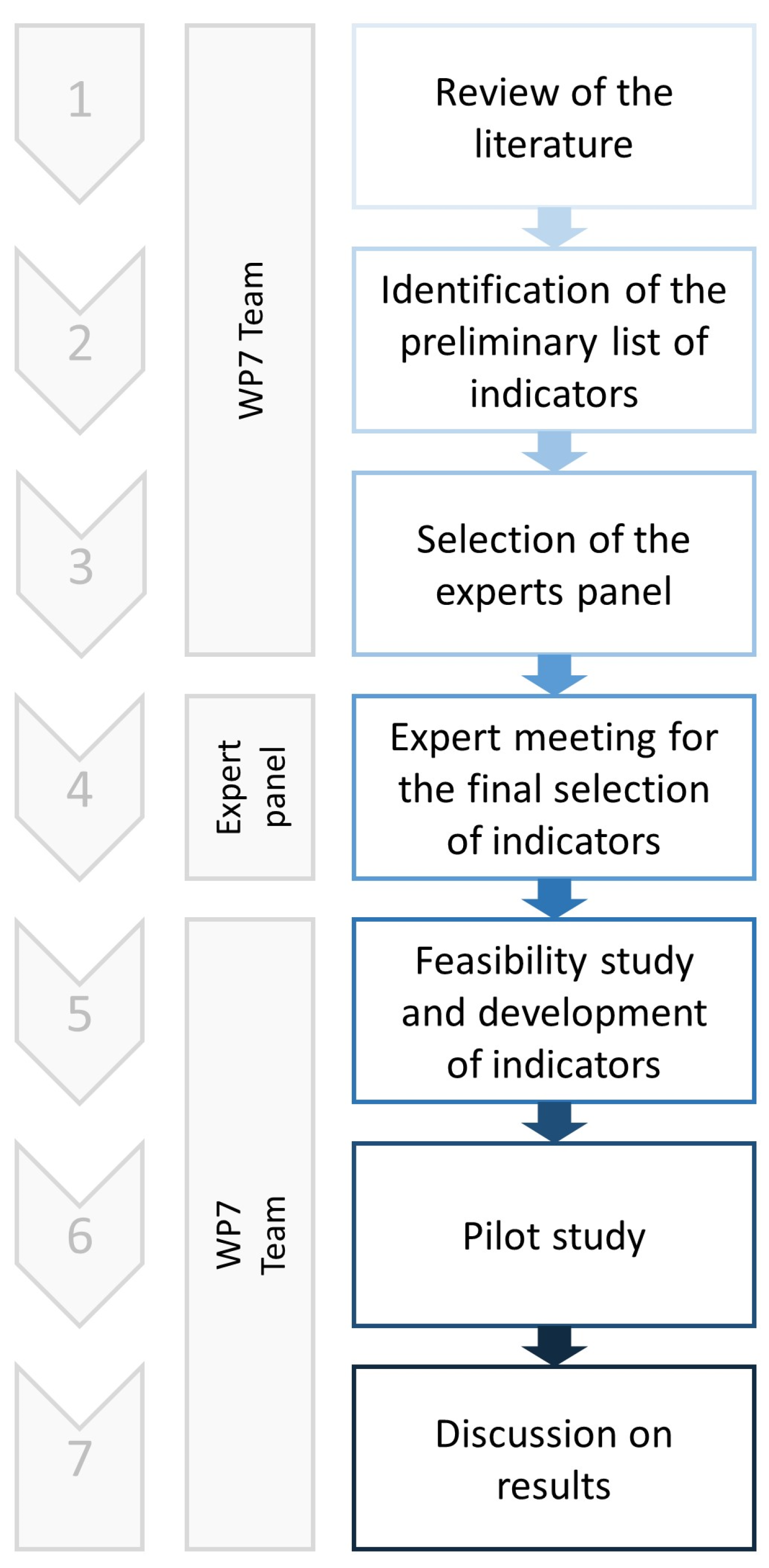
2. Materials and Methods
Data Source and Study Population
3. Results
3.1. Review of the Literature and Qis Extraction
3.2. Expert Panel Approval and Final List of QIs
3.3. Feasibility and Pilot Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization [Internet]. Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 3 May 2023).
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef] [PubMed]
- Eurostat [Internet]. Deaths from Cardiovascular Diseases. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Cardiovascular_diseases_statistics#Deaths_from_cardiovascular_diseases (accessed on 3 May 2023).
- Béjot, Y.; Bailly, H.; Durier, J.; Giroud, M. Epidemiology of stroke in Europe and trends for the 21st century. Presse Med. 2016, 45, e391–e398. [Google Scholar] [CrossRef] [PubMed]
- Rudd, A.G.; Bowen, A.; Young, G.R.; James, M.A. The latest national clinical guideline for stroke. Clin. Med. 2017, 17, 154–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Profes-sionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, E344–E418. [Google Scholar]
- Stroke Foundation [Internet]. Living Clinical Guidelines for Stroke Management. Available online: https://informme.org.au/guidelines/living-clinical-guidelines-for-stroke-management (accessed on 3 May 2023).
- Duncan, P.W.; Horner, R.D.; Reker, D.M.; Samsa, G.P.; Hoenig, H.; Hamilton, B.; LaClair, B.J.; Dudley, T.K. Adherence to postacute rehabilitation guidelines is associated with functional re-covery in stroke. Stroke 2002, 33, 167–177. [Google Scholar] [CrossRef]
- Italian Stroke Association—Associazione Italiana Ictus [Internet]. Linee Guida Italiane di Prevenzione e Trattamento dell’Ictus Cerebrale. Available online: https://isa-aii.com/linee-guida/ (accessed on 3 May 2023).
- Saglietto, A.; Manfredi, R.; Elia, E.; D’Ascenzo, F.; DE Ferrari, G.M.; Zoccai, G.B.; Munzel, T. Cardiovascular disease burden: Italian and global perspectives. Minerva Cardioangiol. 2021, 69, 231–240. [Google Scholar] [CrossRef]
- Italian Ministry of Health—Agenzia Nazionale per I Servizi Sanitari Regionali [Internet]. PNE—Programma Nazionale Esiti. Available online: https://pne.agenas.it/ (accessed on 3 May 2023).
- Béjot, Y.; Bailly, H.; Graber, M.; Garnier, L.; Laville, A.; Dubourget, L.; Mielle, N.; Chevalier, C.; Durier, J.; Giroud, M. Impact of the Ageing Population on the Burden of Stroke: The Dijon Stroke Registry. Neuroepidemiology 2019, 52, 78–85. [Google Scholar] [CrossRef]
- Campanella, P.; Vukovic, V.; Parente, P.; Sulejmani, A.; Ricciardi, W.; Specchia, M.L. The impact of Public Reporting on clinical outcomes: A systematic review and meta-analysis. BMC Health Serv. Res. 2016, 16, 296. [Google Scholar] [CrossRef] [Green Version]
- Lansky, D.; Grossman, M.; Chaloupka, F.J.; Shim, K. Improving Quality Through Public Disclosure of Performance Information. Health Aff. 2002, 21, 52–62. [Google Scholar] [CrossRef] [Green Version]
- Fung, C.H.; Lim, Y.W.; Mattke, S.; Damberg, C.; Shekelle, P.G. Systematic review: The evidence that publishing patient care per-formance data improves quality of care. Ann. Intern. Med. 2008, 148, 111–123. [Google Scholar] [CrossRef]
- Norrving, B.; Bray, B.D.; Asplund, K.; Heuschmann, P.U.; Langhorne, P.; Rudd, A.G.; Wagner, M.; Wiedmann, S.; Wolfe, C.D.; Reeves, M.J.; et al. Cross-National Key Performance Measures of the Quality of Acute Stroke Care in Western Europe. Stroke 2015, 46, 2891–2895. [Google Scholar] [CrossRef] [Green Version]
- Asplund, K.; Åsberg, K.H.; Appelros, P.; Bjarne, D.; Eriksson, M.; Johansson, Å.; Jonsson, F.; Norrving, B.; Stegmayr, B.; Terént, A.; et al. The Riks-Stroke Story: Building a Sustainable National Register for Quality Assessment of Stroke Care. Int. J. Stroke 2010, 6, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Heuschmann, P.U.; Biegler, M.K.; Busse, O.; Elsner, S.; Grau, A.; Hasenbein, U.; Hermanek, P.; Janzen, R.W.C.; Kolominsky-Rabas, P.L.; Kraywinkel, K.; et al. Development and implementation of evidence-based indicators for measuring quality of acute stroke care—The Quality Indicator Board of the German Stroke Registers Study Group (ADSR). Stroke 2006, 37, 2573–2578. [Google Scholar] [CrossRef]
- Colais, P.; Pinnarelli, L.; Mataloni, F.; Giordani, B.; Duranti, G.; D’errigo, P.; Rosato, S.; Seccareccia, F.; Baglio, G.; Davoli, M. The National Outcomes Evaluation Programme in Italy: The Impact of Publication of Health Indicators. Int. J. Environ. Res. Public Health 2022, 19, 11685. [Google Scholar] [CrossRef] [PubMed]
- PNE—Programma Nazionale Esiti [Internet]. Edizione 2022. Available online: https://pne.agenas.it/main/doc/Report_PNE_2022.pdf (accessed on 3 May 2023).
- Italian Ministry of Health [Internet]. La Scheda di Dimissione. Ospedaliera (SDO). Available online: https://www.salute.gov.it/portale/temi/p2_6.jsp?area=ricoveriOspedalieri&id=1232&menu=vuot (accessed on 3 May 2023).
- Italian Ministry of Health [Internet]. Assistenza Emergenza—Urgenza. Available online: https://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=2990&area=sistemaInformativo&menu=emergenza (accessed on 3 May 2023).
- Legg, L.; Langhorne, P.; Outpatient Service Trialists. Rehabilitation therapy services for stroke patients living at home: Systematic review of randomised trials. Lancet 2004, 363, 352–356. [Google Scholar] [CrossRef]
- Teasell, R.; Foley, N.; Salter, K.; Bhogal, S.; Jutai, J.; Speechley, M. Evidence-Based Review of Stroke Rehabilitation: Executive Summary, 12th Edition. Top. Stroke Rehabil. 2009, 16, 463–488. [Google Scholar] [CrossRef] [PubMed]
- Walker, M. Stroke Rehabilitation: Evidence-based or evidence-tinged? J. Rehabil. Med. 2007, 39, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Grube, M.M.; Dohle, C.; Djouchadar, D.; Rech, P.; Bienek, K.; Dietz-Fricke, U.; Jöbges, M.; Kohler, M.; Missala, I.; Schönherr, B.; et al. Evidence-Based Quality Indicators for Stroke Rehabilitation. Stroke 2012, 43, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Zorowitz, R.D. Stroke Rehabilitation Quality Indicators: Raising the Bar in the Inpatient Rehabilitation Facility. Top. Stroke Rehabil. 2010, 17, 294–304. [Google Scholar] [CrossRef]
- Kristensen, H.; Hounsgaard, L. Evaluating the Impact of Audits and Feedback as Methods for Implementation of Evidence in Stroke Rehabilitation. Br. J. Occup. Ther. 2014, 77, 251–259. [Google Scholar] [CrossRef]
- Vratsistas-Curto, A.; McCluskey, A.; Schurr, K. Use of audit, feedback and education increased guideline implementation in a multidisciplinary stroke unit. BMJ Open Qual. 2017, 6, e000212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafei, I.; Karnon, J.; Crotty, M. Quality Improvement in Stroke Rehabilitation: A Scoping Review. J. Multidiscip. Health 2022, ume 15, 2913–2931. [Google Scholar] [CrossRef]
- Cahill, L.S.; Carey, L.M.; Lannin, N.A.; Turville, M.; Neilson, C.L.; Lynch, E.A.; McKinstry, C.E.; Han, J.X.; O’Connor, D. Implementation interventions to promote the uptake of evidence-based practices in stroke rehabilitation. Cochrane Database Syst. Rev. 2020, 2020, CD012575. [Google Scholar] [CrossRef]
- EASY-NET [Internet]. Effectiveness of Audit & Feedback Strategies to Improve Healthcare Practice and Equity in Various Clinical and Organizational Settings. Available online: https://easy-net.info/ (accessed on 3 May 2023).
- Ciurleo, R.; De Cola, M.C.; Agabiti, N.; Di Martino, M.; Bramanti, P.; Corallo, F. Audit and feedback in cardio– and cerebrovascular setting: Toward a path of high reliability in Italian healthcare. Front. Public Health 2022, 10, 907201. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.M.; Braspenning, J.; Hutchinson, A.; Marshall, M. Research methods used in developing and applying quality indi-cators in primary care. Qual. Saf. Health Care 2002, 11, 358–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mant, J. Process versus outcome indicators in the assessment of quality of health care. Int. J. Qual. Health Care 2001, 13, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, J.; Hunter, D. Consensus Methods for Medical and Health-Services Research. Brit. Med. J. 1995, 311, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Fink, A.; Kosecoff, J.; Chassin, M.; Brook, R.H. Consensus methods: Characteristics and guidelines for use. Am. J. Public Health 1984, 74, 979–983. [Google Scholar] [CrossRef] [Green Version]
- Italian Ministry of Health [Internet]. Il Manual ICD9CM. Available online: https://www.salute.gov.it/portale/temi/p2_6.jsp?id=1278&area=ricoveriOspedalieri&menu=cl (accessed on 3 May 2023).
- Miura, S.; Miyata, R.; Matsumoto, S.; Higashi, T.; Wakisaka, Y.; Ago, T.; Kitazono, T.; Iihara, K.; Shimodozono, M. Quality Management Program of Stroke Rehabilitation Using Adherence to Guidelines: A Nationwide Initiative in Japan. J. Stroke Cerebrovasc. Dis. 2019, 28, 2434–2441. [Google Scholar] [CrossRef]
- Dowla, N.; Chan, L. Improving Quality in Stroke Rehabilitation. Top. Stroke Rehabil. 2010, 17, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Purvis, T.; Cadilhac, D.; Donnan, G.; Bernhardt, J. Systematic review of process indicators: Including early rehabilitation inter-ventions used to measure quality of acute stroke care. Int. J. Stroke 2009, 4, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.Q.; PrvuBettger, J.; Guerrier, T.; Hirsch, M.A.; Thomas, J.G.; Pugh, T.M.; Rhoads, C.F. Factors Associated With Discharge to Home Versus Discharge to Institutional Care After Inpatient Stroke Rehabilitation. Arch. Phys. Med. Rehabil. 2015, 96, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Ifejika, N.L.; Bhadane, M.; Cai, C.C.; Watkins, J.N.; Grotta, J.C. Characteristics of Acute Stroke Patients Readmitted to Inpatient Rehabilitation Facilities: A Cohort Study. PMR 2020, 13, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Ingeman, A.; Andersen, G.; Hundborg, H.H.; Svendsen, M.L.; Johnsen, S.P. In-Hospital Medical Complications, Length of Stay, and Mortality Among Stroke Unit Patients. Stroke 2011, 42, 3214–3218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Yu, A.Y.; Bravata, D.M.; Norrving, B.; Reeves, M.J.; Liu, L.; Kilkenny, M.F. Measuring Stroke Quality: Methodological Considerations in Selecting, Defining, and Analyzing Quality Measures. Stroke 2022, 53, 3214–3221. [Google Scholar] [CrossRef]
- Salter, K.; Jutai, J.; Hartley, M.; Foley, N.; Bhogal, S.; Bayona, N.; Teasell, R. Impact of early vs delayed admission to rehabilitation on functional outcomes in persons with stroke. J. Rehabil. Med. 2006, 38, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Noé, E.; Gómez, A.; Bernabeu, M.; Quemada, I.; Rodríguez, R.; Pérez, T.; López, C.; Laxe, S.; Colomer, C.; Ríos, M.; et al. Guidelines: Basic principles of neurorehabilitation for patients with acquired brain injury. Recommendations of the Spanish Society of Neurorehabilitation. Neurologia (Engl. Ed.) 2023. ahead of print. [Google Scholar] [CrossRef]
- Navarro Soler, I.M.; Ignacio García, E.; Masjuan Vallejo, J.; Gállego Culleré, J.; Mira Solves, J.J. A set of care quality indicators for stroke management. Conjunto de indicadores de calidad asistencial en el abordaje del ictus. Neurologia 2019, 34, 497–502. [Google Scholar] [CrossRef]
- De Cola, M.C.; Ielo, A.; Buono, V.L.; Quartarone, A.; Calabrò, R.S. Toward social-health integration in Sicily: Description of the first hub and spoke model to improve the diagnostic therapeutic care paths for neurorehabilitation. Front. Public Health 2023, 11, 1141581. [Google Scholar] [CrossRef]
- Kinoshita, S.; Kakuda, W.; Momosaki, R.; Yamada, N.; Sugawara, H.; Watanabe, S.; Abo, M. Clinical management provided by board-certificated physiatrists in early reha-bilitation is a significant determinant of functional improvement in acute stroke patients: A retrospective analysis of Japan rehabilitation database. J. Stroke Cereb. Dis. 2015, 24, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, E.H.; So, G.; Zappitelli, M.; Chanchlani, R. A Review on the Application and Limitations of Administrative Health Care Data for the Study of Acute Kidney Injury Epidemiology and Outcomes in Children. Front. Pediatr. 2021, 9, 742888. [Google Scholar] [CrossRef] [PubMed]
- Grimley, R.S.; Rosbergen, I.C.; Gustafsson, L.; Horton, E.; Green, T.; Cadigan, G.; Kuys, S.; Andrew, N.E.; Cadilhac, D.A. Dose and setting of rehabilitation received after stroke in Queensland, Australia: A prospective cohort study. Clin. Rehabil. 2020, 34, 812–823. [Google Scholar] [CrossRef] [PubMed]
- Grimley, R.S.; Rosbergen, I.C.; Gustaffson, L.; Horton, E.; Green, T.; Cadigan, G.; Cadilhac, D.A.; Kuys, S. Assessment and selection for rehabilitation following acute stroke: A prospective cohort study in Queensland, Australia. Clin. Rehabil. 2019, 33, 1252–1263. [Google Scholar] [CrossRef]
- Purvis, T.; Hubbard, I.J.; Cadilhac, D.A.; Hill, K.; Watkins, J.; Lannin, N.A.; Faux, S.G.; Kilkenny, M.F. Age-Related Disparities in the Quality of Stroke Care and Outcomes in Rehabilitation Hospitals: The Australian National Audit. J. Stroke Cerebrovasc. Dis. 2021, 30, 105707. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Indicator | Description | Type |
|---|---|---|
| NoRA (Number of Rehabilitation Admissions) | Number of rehabilitation admissions for ischemic stroke | Outcome |
| AWTR (Average Waiting Time for Rehabilitation) | Average waiting time for rehabilitation admission following the discharge from acute hospitalization for ischemic stroke | Process |
| HD (Home Discharges) | Proportion of discharges to the patient’s home following the admission to rehabilitation for ischemic stroke | Outcome |
| PD (Protected Discharges) | Proportion of protected discharges following the admission to rehabilitation for ischemic stroke | Outcome |
| AD (Acute Discharges) | Proportion of transfers to acute care following the admission to rehabilitation for ischemic stroke | Outcome |
| ALoSR (Average Length of Stay in Rehabilitation) | The average number of days that patients spend in rehabilitation | Process |
| MCR (Medical Complications in Rehabilitation) | Proportion of rehabilitation admissions with medical complications | Outcome |
| ACLoD (Average Change in Level of Disability) | Average change in the level of disability from admission to discharge | Outcome |
| RGA (Rehabilitation Goals Achievement) | Proportion of admissions in which rehabilitation goals were achieved | Outcome |
| 2019 | 2020 | 2021 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hospital Unit | NoRa | AWTR | HD | PD | AD | NoRa | AWTR | HD | PD | AD | NoRa | AWTR | HD | PD | AD |
| Bonino Pulejo | 59 | 14.10 | 67.50 | 15.00 | 10.00 | 27 | 0.14 | 71.43 | 9.52 | 14.29 | 16 | 3.00 | 100.00 | 0.00 | 0.00 |
| Pisani | 2 | 0.00 | 100.00 | 0.00 | 0.00 | 0 | 0.00 | 0.00 | 0.00 | 0.00 | 2 | 10.00 | 100.00 | 0.00 | 0.00 |
| Piemonte | 19 | 0.00 | 53.85 | 23.08 | 15.38 | 9 | 0.00 | 40.00 | 0.00 | 0.00 | 6 | 0.00 | 66.67 | 0.00 | 0.00 |
| Cannizzaro | 1 | 0.00 | 0.00 | 0.00 | 100.00 | 4 | 9.00 | 66.67 | 0.00 | 33.33 | 2 | 0.00 | 50.00 | 50.00 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Cola, M.C.; Ielo, A.; Corallo, F.; Pollina Addario, S.; Scondotto, S.; Allotta, A.; Fantaci, G.; Bramanti, P.; Ciurleo, R. Development of a Set of Indicators for Measuring and Improving Quality of Rehabilitation Care after Ischemic Stroke. Healthcare 2023, 11, 2065. https://doi.org/10.3390/healthcare11142065
De Cola MC, Ielo A, Corallo F, Pollina Addario S, Scondotto S, Allotta A, Fantaci G, Bramanti P, Ciurleo R. Development of a Set of Indicators for Measuring and Improving Quality of Rehabilitation Care after Ischemic Stroke. Healthcare. 2023; 11(14):2065. https://doi.org/10.3390/healthcare11142065
Chicago/Turabian StyleDe Cola, Maria Cristina, Augusto Ielo, Francesco Corallo, Sebastiano Pollina Addario, Salvatore Scondotto, Alessandra Allotta, Giovanna Fantaci, Placido Bramanti, and Rosella Ciurleo. 2023. "Development of a Set of Indicators for Measuring and Improving Quality of Rehabilitation Care after Ischemic Stroke" Healthcare 11, no. 14: 2065. https://doi.org/10.3390/healthcare11142065
APA StyleDe Cola, M. C., Ielo, A., Corallo, F., Pollina Addario, S., Scondotto, S., Allotta, A., Fantaci, G., Bramanti, P., & Ciurleo, R. (2023). Development of a Set of Indicators for Measuring and Improving Quality of Rehabilitation Care after Ischemic Stroke. Healthcare, 11(14), 2065. https://doi.org/10.3390/healthcare11142065