
Family Counseling after the Diagnosis of Congenital Heart Disease in the Fetus: Scoping Review

 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of the Research Question
2.2. Identification of Relevant Studies
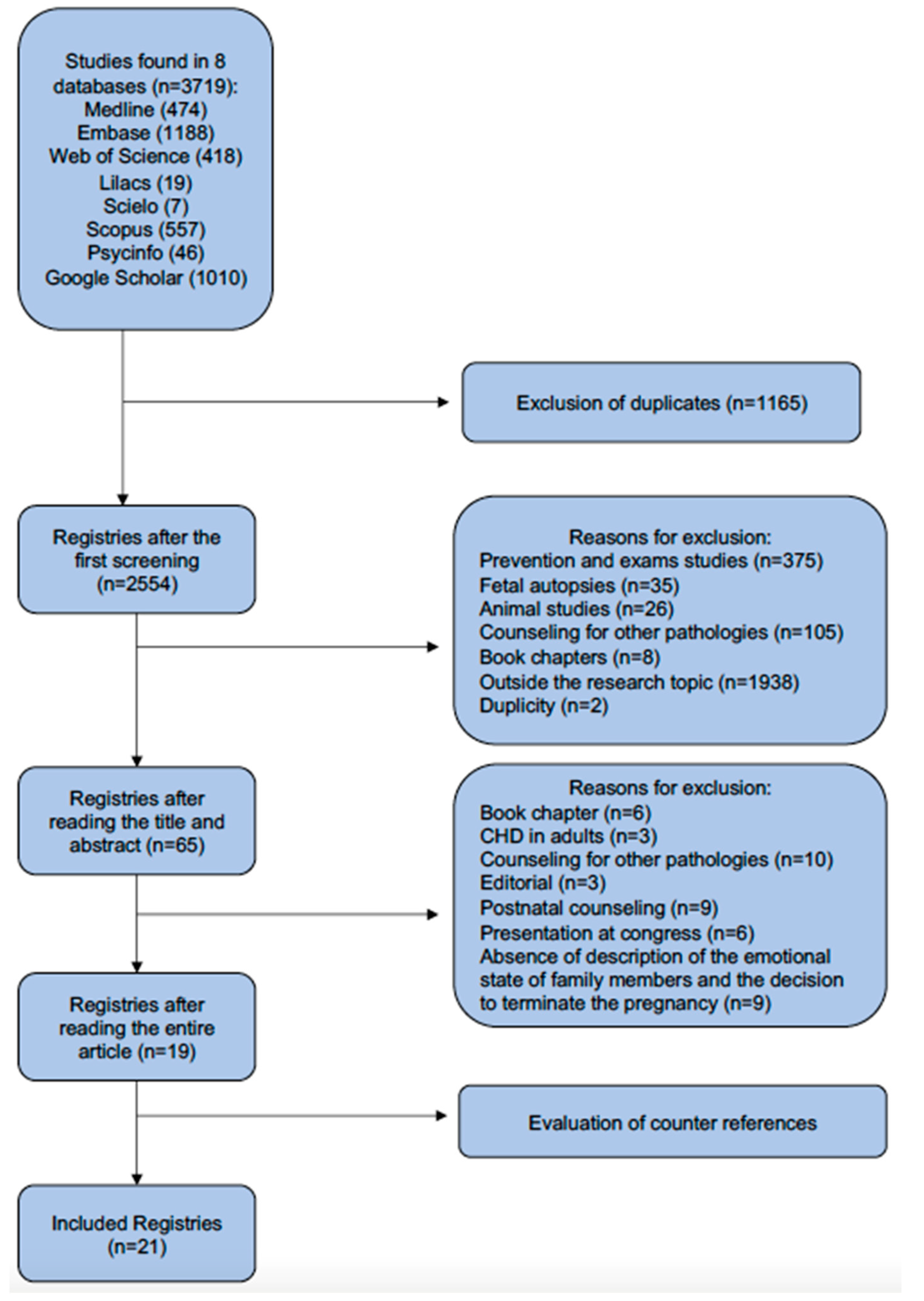
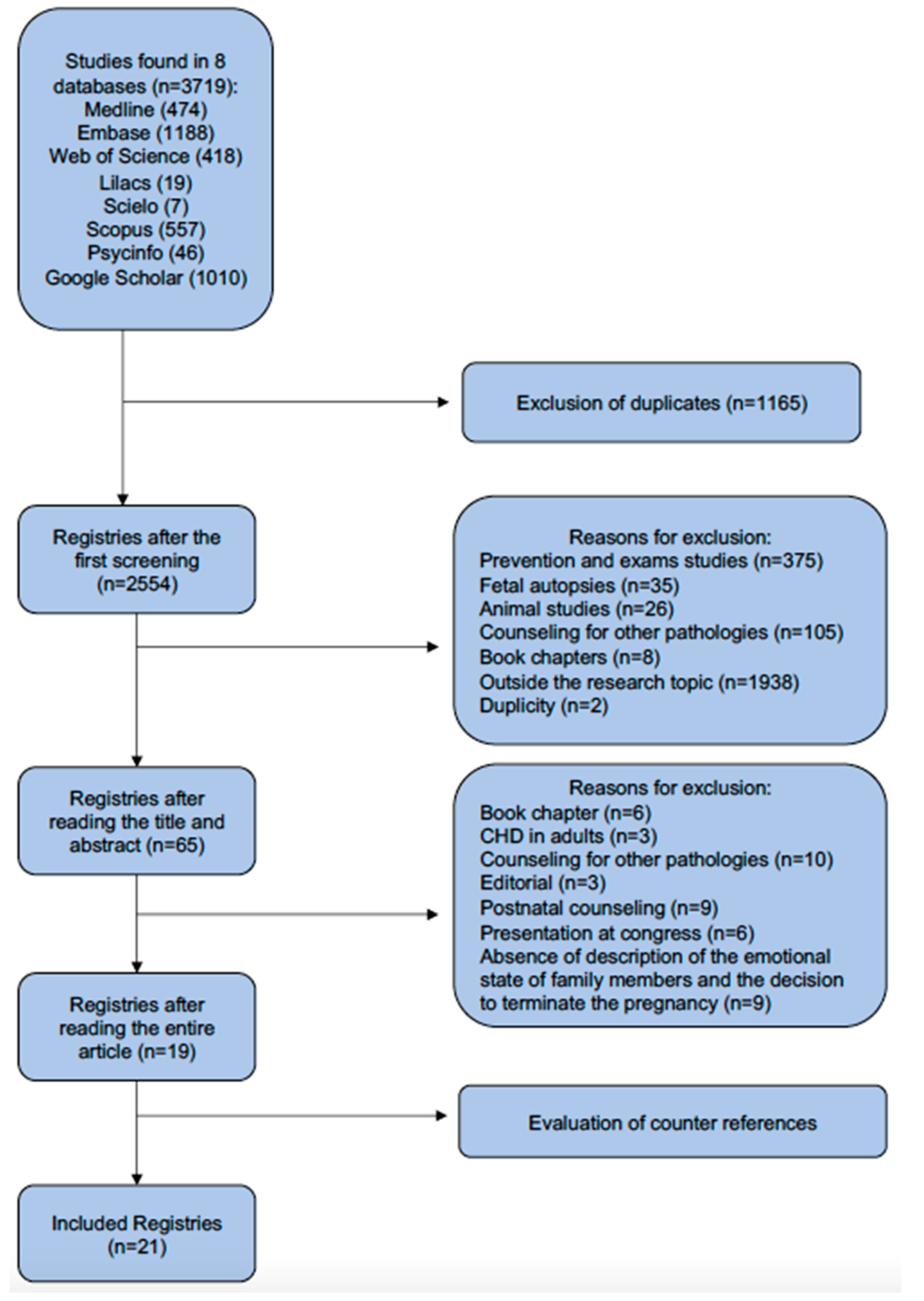
2.3. Selection of Studies
2.4. Data Mapping
2.5. Results Demonstration
3. Results
4. Discussion
4.1. Obstacles to Effective Family Counseling in Cases of Diagnosis Heart Disease in the Fetus
4.2. Strengths for Effective Family Counseling
4.3. Opportunities for Services and the Healthcare Team in Relation to Appropriate Family Counseling
4.4. Challenges for Services and the Health Team in Relation to Adequate Family Counseling in These Cases
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donofrio, M.T.; Moon-Grady, A.J.; Hornberger, L.K.; Copel, J.A.; Sklansky, M.S.; Abuhamad, A.; Cuneo, B.F.; Huhta, J.C.; Jonas, R.A.; Krishnan, A.; et al. Diagnosis and Treatment of Fetal Cardiac Disease: A Scientific Statement from the American Heart Association. Circulation 2014, 129, 2183–2242. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, A.; Simmelbauer, A.; Starystach, S.; Elsässer, M.; Sohn, C.; Müller, A.; Bär, S.; Gorenflo, M. Assessment of Needs for Counseling after Prenatal Diagnosis of Congenital Heart Disease—A Multidisciplinary Approach. Klin. Padiatr. 2018, 230, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, A.; Elsässer, M.; Fluhr, H.; Müller, A.; Starystach, S.; Bär, S.; Gorenflo, M. Counseling for Fetal Heart Disease—Current Standards and Best Practice. Transl. Pediatr. 2021, 10, 2225–2234. [Google Scholar] [CrossRef]
- Rosano, A.; Botto, L.D.; Botting, B.; Mastroiacovo, P. Infant Mortality and Congenital Anomalies from 1950 to 1994: An International Perspective. J. Epidemiol. Community Health 2000, 54, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, A.; Simmelbauer, A.; Starystach, S.; Elsässer, M.; Müller, A.; Bär, S.; Gorenflo, M. Counseling for Prenatal Congenital Heart Disease-Recommendations Based on Empirical Assessment of Counseling Success. Front. Pediatr. 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, T.; Marttala, U.M.; Wadensten, B.; Bergman, G.; Mattsson, E. Involvement of Persons with Lived Experience of a Prenatal Diagnosis of Congenital Heart Defect: An Explorative Study to Gain Insights into Perspectives on Future Research. Res. Involv. Engagem. 2016, 2, 35. [Google Scholar] [CrossRef]
- Kovacevic, A.; Wacker-Gussmann, A.; Bär, S.; Elsässer, M.; Motlagh, A.M.; Ostermayer, E.; Oberhoffer-Fritz, R.; Ewert, P.; Gorenflo, M.; Starystach, S. Parents’ Perspectives on Counseling for Fetal Heart Disease: What Matters Most? J. Clin. Med. 2022, 11, 278. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Social. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Menahem, S.; Grimwade, J. Effective Counselling of Pre-Natal Diagnosis of Serious Heart Disease—An Aid to Maternal Bonding? Diagn. Ther. 2004, 19, 470–474. [Google Scholar] [CrossRef]
- Rempel, G.R.; Cender, L.M.; Lynam, M.J.; Sandor, G.G.; Farquharson, D. Parents’ Perspectives on Decision Making after Antenatal Diagnosis of Congenital Heart Disease. JOGNN J. Obstet. Gynecol. Neonatal Nurs. 2004, 33, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Hilton-Kamm, D.; Sklansky, M.; Chang, R.K. How Not to Tell Parents about Their Child’s New Diagnosis of Congenital Heart Disease: An Internet Survey of 841 Parents. Pediatr. Cardiol. 2014, 35, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, T.; Bergman, G.; Marttala, U.M.; Wadensten, B.; Mattsson, E. Information Following a Diagnosis of Congenital Heart Defect: Experiences among Parents to Prenatally Diagnosed Children. PLoS ONE 2015, 10, e0117995. [Google Scholar] [CrossRef] [PubMed]
- Bratt, E.L.; Järvholm, S.; Ekman-Joelsson, B.M.; Mattson, L.Å.; Mellander, M. Parent’s Experiences of Counselling and Their Need for Support Following a Prenatal Diagnosis of Congenital Heart Disease—A Qualitative Study in a Swedish Context. BMC Pregnancy Childbirth 2015, 15, 171. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, T.; Marttala, U.M.; Mattsson, E.; Ringnér, A. Experiences and Preferences of Care among Swedish Immigrants Following a Prenatal Diagnosis of Congenital Heart Defect in the Fetus: A Qualitative Interview Study. BMC Pregnancy Childbirth 2016, 16, 130. [Google Scholar] [CrossRef]
- Walsh, M.J.; Verghese, G.R.; Ferguson, M.E.; Fino, N.F.; Goldberg, D.J.; Owens, S.T.; Pinto, N.; Zyblewski, S.C.; Quartermain, M.D. Counseling Practices for Fetal Hypoplastic Left Heart Syndrome. Pediatr. Cardiol. 2017, 38, 946–958. [Google Scholar] [CrossRef]
- Lee, C.K. Prenatal Counseling of Fetal Congenital Heart Disease. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 5. [Google Scholar] [CrossRef]
- Carlsson, T.; Mattsson, E. Emotional and Cognitive Experiences during the Time of Diagnosis and Decision-Making Following a Prenatal Diagnosis: A Qualitative Study of Males Presented with Congenital Heart Defect in the Fetus Carried by Their Pregnant Partner. BMC Pregnancy Childbirth 2018, 18, 26. [Google Scholar] [CrossRef]
- YM, I.; TJ, Y.; IY, Y.; Kim, S.; Jin, J.; Kim, S. The Pregnancy Experience of Korean Mothers with a Prenatal Fetal Diagnosis of Congenital Heart Disease. BMC Pregnancy Childbirth 2018, 18, 467. [Google Scholar]
- Bertaud, S.; Lloyd, D.F.A.; Sharland, G.; Razavi, R.; Bluebond-Langner, M. The Impact of Prenatal Counselling on Mothers of Surviving Children with Hypoplastic Left Heart Syndrome: A Qualitative Interview Study. Health Expect. 2020, 23, 1224–1230. [Google Scholar] [CrossRef]
- Kovacevic, A.; Bär, S.; Starystach, S.; Simmelbauer, A.; Elsässer, M.; Müller, A.; Motlagh, A.M.; Oberhoffer-Fritz, R.; Ostermayer, E.; Ewert, P.; et al. Objective Assessment of Counselling for Fetal Heart Defects: An Interdisciplinary Multicenter Study. J. Clin. Med. 2020, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Holmes, K.W.; Huang, J.H.; Gutshall, K.; Kim, A.; Ronai, C.; Madriago, E.J. Fetal Counseling for Congenital Heart Disease: Is Communication Effective? J. Matern. Fetal Neonatal Med. 2021, 35, 5049–5053. [Google Scholar] [CrossRef] [PubMed]
- Kovacevic, A.; Bär, S.; Starystach, S.; Elsässer, M.; van der Locht, T.; Motlagh, A.M.; Ostermayer, E.; Oberhoffer-Fritz, R.; Ewert, P.; Gorenflo, M.; et al. Fetal Cardiac Services during the COVID-19 Pandemic: How Does It Affect Parental Counseling? J. Clin. Med. 2021, 10, 3423. [Google Scholar] [CrossRef] [PubMed]
- Delaney, R.K.; Pinto, N.M.; Ozanne, E.M.; Stark, L.A.; Pershing, M.L.; Thorpe, A.; Witteman, H.O.; Thokala, P.; Lambert, L.M.; Hansen, L.M.; et al. Study Protocol for a Randomised Clinical Trial of a Decision Aid and Values Clarification Method for Parents of a Fetus or Neonate Diagnosed with a Life-Threatening Congenital Heart Defect. BMJ Open 2021, 11, e055455. [Google Scholar] [CrossRef] [PubMed]
- Gendler, Y.; Birk, E. Developing a Standardized Approach to Prenatal Counseling Following the Diagnosis of a Complex Congenital Heart Abnormality. Early Hum. Dev. 2021, 163, 105507. [Google Scholar] [CrossRef]
- Harris, K.W.; Hammack-Aviran, C.M.; Brelsford, K.M.; Kavanaugh-McHugh, A.; Clayton, E.W. Mapping Parents’ Journey Following Prenatal Diagnosis of CHD: A Qualitative Study. Cardiol. Young 2022, 33, 1387–1395. [Google Scholar] [CrossRef]
- Rodriguez, J.G.; Holmes, R.; Martin, R.; Wilde, P.; Soothill, P. Prognosis Following Prenatal Diagnosis of Heart Malformations. Early Hum. Dev. 1998, 52, 13–20. [Google Scholar] [CrossRef]

{kind=link}
| Database | Search | Filter | Items Found | Search Date |
|---|---|---|---|---|
| Medline | ((Counseling) AND (“Heart Defects, Congenital” [Mesh] OR “Defect, Congenital Heart” OR “Abnormality, Heart” OR “Heart Abnormality” OR “Congenital Heart Defect” OR “Heart, Malformation Of” OR “Malformation Of Heart” OR “Defects, Congenital Heart” OR “Heart Abnormalities” OR “Heart Defect, Congenital” OR “Congenital Heart Disease” OR “Congenital Heart Diseases” OR “Disease, Congenital Heart” OR “Heart Disease, Congenital” OR “Congenital Heart Defects”) AND (fetal heart)) | Humans | 474 | 28 September 2022 |
| Embase | (‘counseling’/exp OR counseling OR ‘parent counseling’/exp OR (counseling, AND parent) OR (guidance, AND parent) OR (parent AND guidance)) AND (‘congenital heart malformation’/exp OR (congenital AND heart AND anomaly) OR (congenital AND heart AND defect) OR (congenital AND heart AND defects) OR (heart AND anomaly) OR (heart AND congenital AND anomaly) OR (heart AND congenital AND defect) OR (heart AND congenital AND malformation) OR (heart AND defects, AND congenital) OR (heart AND malformation)) AND (‘fetus heart’/exp OR (fetal AND heart) OR (foetal AND heart) OR (heart, AND fetus)) AND [Embase]/lim AND [humans]/lim | Humans | 1188 | 28 September 2022 |
| LILACS | (mh:”Aconselhamento” OR (consejo) OR (counseling) OR (conselho) OR mh: f02.784.176* OR mh:f04.408.413* OR mh:n02.421.143.303* OR mh:n02.421.461.363*) AND (mh: “Cardiopatias Congênitas” OR (cardiopatías congénitas) OR (heart defects, congenital) OR (malformação cardiovascular) OR (defeitos cardiovasculares congênitos) OR (anormalidades cardíacas) OR mh:c14.240.400* OR mh:c14.280.400* OR mh:c16.131.240.400*) AND (mh: “Coração Fetal” OR (corazón fetal) OR (fetal heart) OR mh:a07.541.278* OR mh:a16.378.303*) AND (db:(“LILACS”)) | Title, abstract and subject | 19 | 28 September 2022 |
| Scielo | ((Coração Fetal) OR (Corazón Fetal) OR (Fetal Heart)) AND ((Cardiopatias Congênitas) OR (Cardiopatías Congénitas) OR (Heart Defects, Congenital)) AND ((Aconselhamento) OR (Consejo) OR (Counseling)) | No filter | 7 | 1 October 2022 |
| Scopus | (ALL (“Hearts, Fetal” OR “Heart, Fetal” OR “Fetal Hearts”) AND ALL (“Defect, Congenital Heart “ OR “Abnormality, Heart” OR “Abnormality Congenital Heart” OR “Defect Heart, Malformation Of” OR “Malformation Of Heart” OR “Malformation Of Hearts” OR “Defects, Congenital Heart” OR “Heart Abnormalities” OR “Heart Defect, Congenital” OR “Congenital Heart Disease” OR “Congenital Heart Diseases” OR “Disease, Congenital Heart” OR “Heart Disease, Congenital” OR “Congenital Heart Defects”) AND ALL (“counseling” OR “counseling, parent” OR “parent counseling” OR “guidance, parent” OR “parent guidance”)) | Medicine; Biochemistry, Genetics and Molecular Biology; Health Professions; Nursing; Multidisciplinary; Psychology | 577 | 1 October 2022 |
| Web of science | fetal heart and congenital heart disease and counseling | No filter | 418 | 1 October 2022 |
| PsycINFO | congenital heart disease AND counseling | No filter | 46 | 1 October 2022 |
| Google Scholar | “fetal heart” and “congenital heart disease” and “counseling” | No filter | first 1010 articles | 1 October 2022 |
| Study | Reference | Objective | Methodology | Team | Results |
|---|---|---|---|---|---|
| 1 | Menahem S and Grinwade J. Australia 2004 [10] | Assessment of family members of the counseling provided at the service. | Qualitative study * | PC, FC, and FP ** | Counseling improved understanding of CHD and postnatal treatment. Drawings provide a better understanding of CHD. |
| 2 | Rempel, GR; et al. Canada. 2004 [11] | Discover and describe how parents make decisions after a diagnosis of CHD during pregnancy and guide professionals in counseling. | Qualitative study | PC, FC ** | Healthcare professionals must understand each parent, know their professional influence, and support each family decision. |
| 3 | Hilton-Kamm, D; et al. California, USA 2014 [12] | Study the perceptions of parents and experiences upon receiving a diagnosis of CHD. | Cross-sectional study * | PC | The way information is presented to family members can shape parents’ decision making. |
| 4 | Carlsson, T; et al. Sweden 2015 [13] | Describe the experiences of parents after a prenatal diagnosis of CHD. | Cross-sectional study * | PC | Valuing early and honest information. The illustrations as a complement to the oral information help in understanding the CHD. Reliable sources on the internet for more information about CHD. |
| 5 | Bratt, EL; et al. Sweden 2015 [14] | Describe counseling in cases of fetal CHD and the need for continuous pregnancy monitoring. | Qualitative study * | PC, FC, nurse, obstetric team, psychologist, and social worker ** | The short period between suspicion and accurate diagnosis of CHD in the fetus. Continuous counseling during pregnancy. Written and quality information about CHD. Similar explanations for the partner. |
| 6 | Carlsson, T et al. Sweden 2016 [15] | Describe the experiences of Swedish immigrant family members diagnosed with CHD in the fetus. | Qualitative study * | Obstetric nurse | The need for an interpreter, visual information, and psychosocial support, and respecting religion regarding the termination of pregnancy. |
| 7 | Carlsson, T; et al. Sweden 2016 [6] | Describe the experiences of parents following a prenatal diagnosis of CHD through group discussion. | Qualitative study | PC | Emotional support for the couple is important. Additional information about CHD. Follow-up of the pregnant woman to repeat information about CHD. |
| 8 | Walsh, MJ et al. USA 2017 [16] | Assessment counseling for family members with a fetal diagnosis of hypoplastic left heart syndrome. | Cross-sectional study * | PC, FC | Great variability between forms of counseling. Difficulty in addressing the prognosis. |
| 9 | Lee, CK. Missouri, USA 2017 [17] | Review the benefits and objectives of counseling in the prenatal stage, the problems encountered, the topics to be covered, and considerations for family support during prenatal care. | Cross-sectional study | PC, FC | Family members believe that cardiologists should increase the amount of information related to CHD from prenatal care and continue for the rest of life. |
| 10 | Carlsson, T.; et al. Sweden 2018 [18] | Describe the experiences of parents following a prenatal diagnosis of CHD through group discussion. | Qualitative study | PC | Additional information about CHD. Monitoring the pregnant woman to repeat information about CHD. |
| 11 | Kovacevic, A; et al. Germany 2018 [2] | Develop an appropriate questionnaire to assess parental counseling needs. | Cross-sectional study * | PC, FP, and sociologists | The questionnaire applied can be a tool to evaluate the success of family counseling and recommends multidisciplinary counseling. |
| 12 | Im, YM; et al. South Korea 2018 [19] | Describe the experience of Korean mothers with prenatal diagnosis of CHD. | Qualitative study | Specialist healthcare professional | Importance of family counseling. The movement of the fetus helps in understanding that the fetus is an independent being and can be influenced by external factors. Importance of the religious and spiritual aspects (Taekyo technique). |
| 13 | Bertaud S; et al. England 2020 [20] | Evaluate counseling for family members with a fetal diagnosis of hypoplastic left heart syndrome. | Qualitative study * | PC, FC | Counseling for these family members offers a better view of your child’s prospects. |
| 14 | Kovacevic, A; et al. Germany 2020 [21] | Evaluation of family counseling after the diagnosis of CHD in the fetus. | Cross-sectional study * | PC, FP, and sociologists. | Continuous family counseling, with a private room, adequate dialogue time, native language, and use of written or web information to understand CHD. It suggests greater success if performed by a cardiologist. |
| 15 | Kovacevic, A; et al. Germany 2021 [3] | Assess the effects of parental counseling for fetal CHD. | Cross-sectional study | PC, FP, and sociologists | Implementing alternative and innovative approaches (e.g., online conferences or virtual reality tools) may aid in facilitating high-quality services in critical times such as in the COVID pandemic. |
| 16 | Holmes, KW; et al. Portland, USA 2021 [22] | Assess the understanding of family members of fetal heart defects after counseling. | Cross-sectional study * | PC, FC, and nurse | Fetal counseling was effective in conveying the anatomy and need for surgery. There was less understanding for women with less education. The following were evaluated: description of the cardiac condition, how confident they were in the diagnosis, and whether the fetus would require heart surgery. |
| 17 | Kovacevic, A; et al. Germany 2021 [23] | Evaluating family counseling for fetal CHD during COVID-19 pandemic. | Multicenter cross-sectional study * | PC, FC, and PF | There was no significant difference between the groups in relation to the success of counseling these family members even with the COVID-19 pandemic. |
| 18 | Delaney, RK; et al. Utah, USA 2021 [24] | To evaluate the effect of two family counseling protocols in cases of CHD in the fetus. | Randomized clinical trial | PC, FC, surgeon, social worker, and palliative care | Publication of the study protocol. |
| 19 | Gendler, Y; et al. Israel 2021 [25] | Assessment of family members of the standardized counseling provided at the service. | Cross-sectional study * | PC | Standardized counseling using a checklist helps provide information. Parental satisfaction in the counseling process. Good perception of cardiologists regarding the family understanding of CHD. |
| 20 | Kovacevic, A; et al. Germany 2022 [7] | Identify which factors play an important role in the success of family counseling in cases of fetal CHD. | Multicenter cross-sectional study * | PC, FC, and FP | Short time between suspicion and accurate diagnosis of CHD and explanation by the specialist. Information about CHD in a clear and illustrated way. |
| 21 | Harris, KW; et al. Pittsburgh, USA 2022 [26] | Describe the experience of parents who receive a diagnosis of fetal CHD (pre and postnatal). | Qualitative study * | PC | Uncertainty about the diagnosis and lack of adequate information increases the stress on families. Family members prefer fetal cardiologists to clarify and deal with the situation. |
| Thematic Approach | Included Studies |
|---|---|
| Theme 1: Obstacles to effective family counseling | |
| Ineffective doctor–patient relationship | 1,2,3,4,6,7,8,10,12,13,14,15,21 |
| The information was provided in an inappropriate manner | 5,6,8,9,10,12,13,17 |
| Difficulty in standardizing the language | 1,3,7,10,11,16,17,18,19,20 |
| Theme 2: Strengths for effective family counseling | |
| Understanding heart disease | 1,3,4,5,9,10,11,12,14,17,19,20,21 |
| The manner in which the diagnosis is communicated | 1,2,6,7,12 |
| Good infrastructure | 5,8,9,15,17 |
| Theme 3: Opportunities for the healthcare services and the health team | |
| Focus on humanization | 1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21 |
| Multidisciplinary support network | 6,8,9,10,12,13,17 |
| Comprehension of the disease | 5,7,8,10,12,15 |
| Family’s trust in the team | 1,2,3,4,7,10,12 |
| Confidence in decision making | 1,2,3,4,7,10,12 |
| Theme 4: Challenges for the healthcare services and the health team | |
| Continuous family counseling | 4,6,8,10,12,13,14,15,21 |
| Presence of fetal and pediatric cardiologist | 1,3,4,5,9,10,11,12,14,17,19,20,21 |
| Multidisciplinary team | 5,6,8,9,10,12,13,17 |
| Audiovisual resources | 1,3,7,10,11,16,17,18,19,20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, S.L.d.M.; Tuda, L.T.S.; Dias, M.B.; Carvalho, L.I.A.d.; Estevam, T.L.L.; Novelleto, A.L.M.T.; Araujo Júnior, E.; Rocha Amorim, L.A.d. Family Counseling after the Diagnosis of Congenital Heart Disease in the Fetus: Scoping Review. Healthcare 2023, 11, 2826. https://doi.org/10.3390/healthcare11212826
Almeida SLdM, Tuda LTS, Dias MB, Carvalho LIAd, Estevam TLL, Novelleto ALMT, Araujo Júnior E, Rocha Amorim LAd. Family Counseling after the Diagnosis of Congenital Heart Disease in the Fetus: Scoping Review. Healthcare. 2023; 11(21):2826. https://doi.org/10.3390/healthcare11212826
Chicago/Turabian StyleAlmeida, Sophia Livas de Morais, Luisa Tiemi Souza Tuda, Marcela Bezerra Dias, Luana Izabela Azevedo de Carvalho, Thayla Lais Lima Estevam, Ana Luiza Menezes Teles Novelleto, Edward Araujo Júnior, and Luciane Alves da Rocha Amorim. 2023. "Family Counseling after the Diagnosis of Congenital Heart Disease in the Fetus: Scoping Review" Healthcare 11, no. 21: 2826. https://doi.org/10.3390/healthcare11212826