
Defining Epiglottic Collapses Patterns in Obstructive Sleep Apnea Patients: Francia-Lugo Classification
 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. DISE Procedure
3. Results
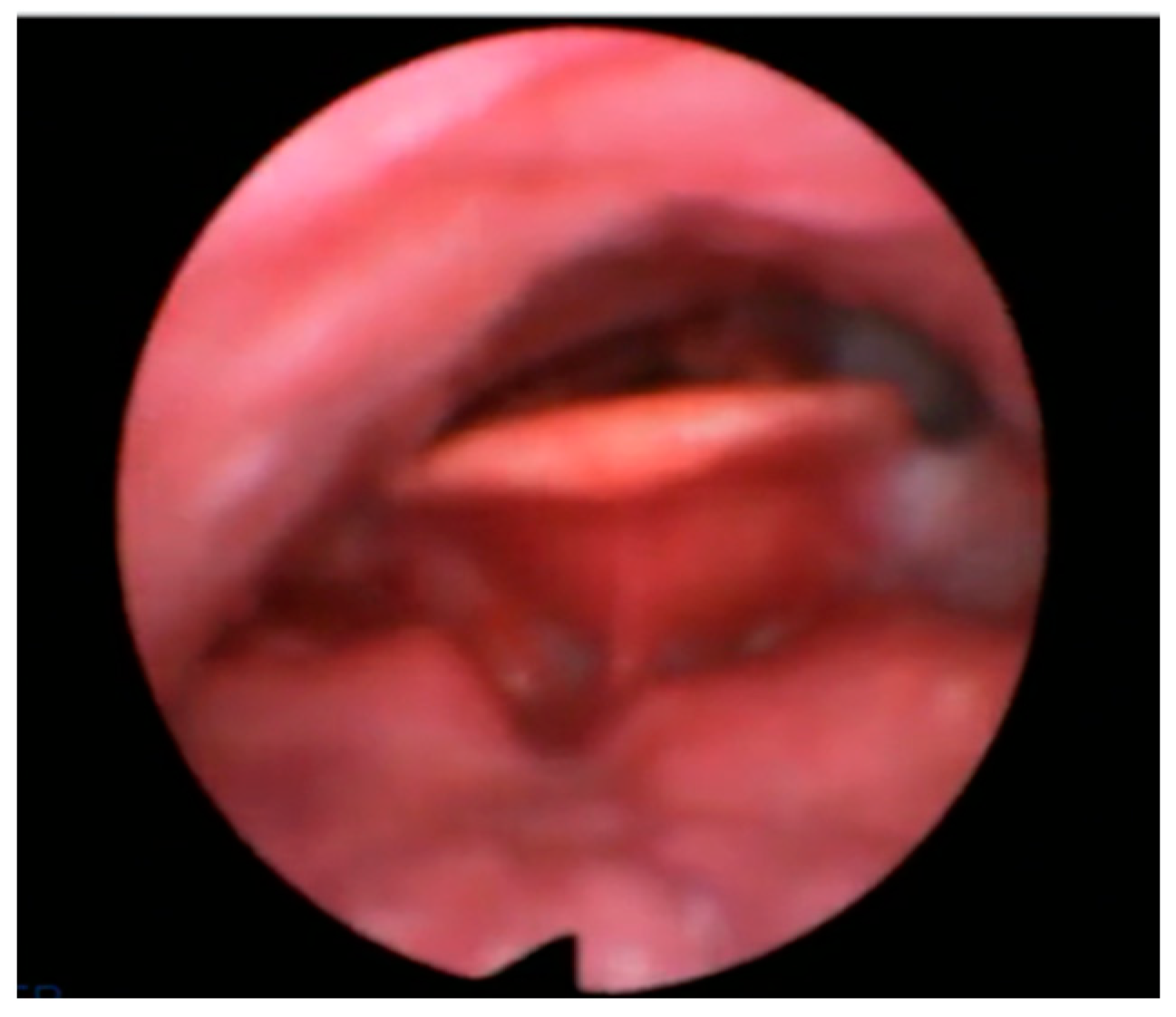
- Anterior–Posterior (AP) primary collapse with rigid component “trapdoor type” in 50 patients (48%);
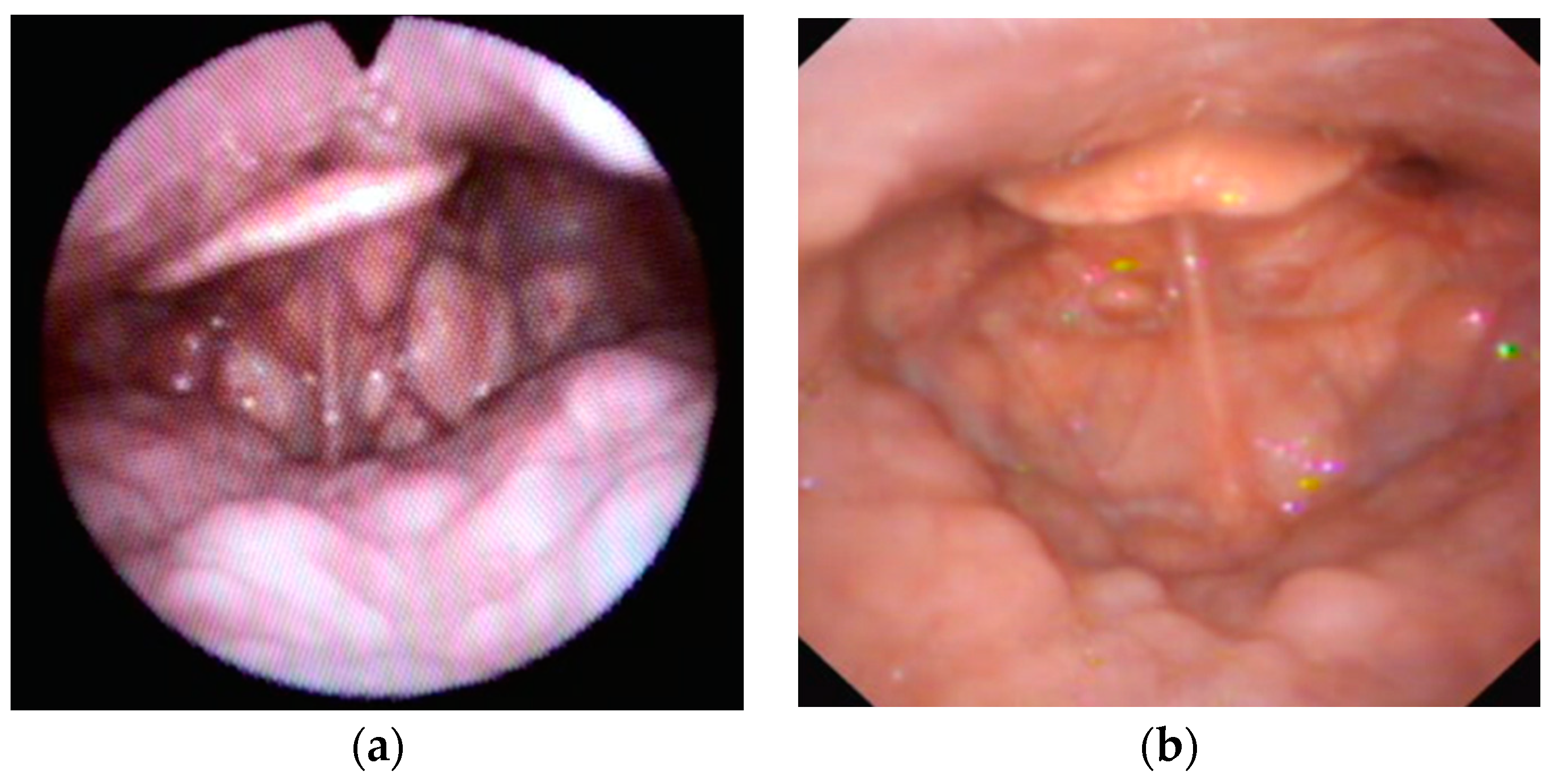
- AP primary collapse with lax component “floppy type” in 14 patients (13.5%);
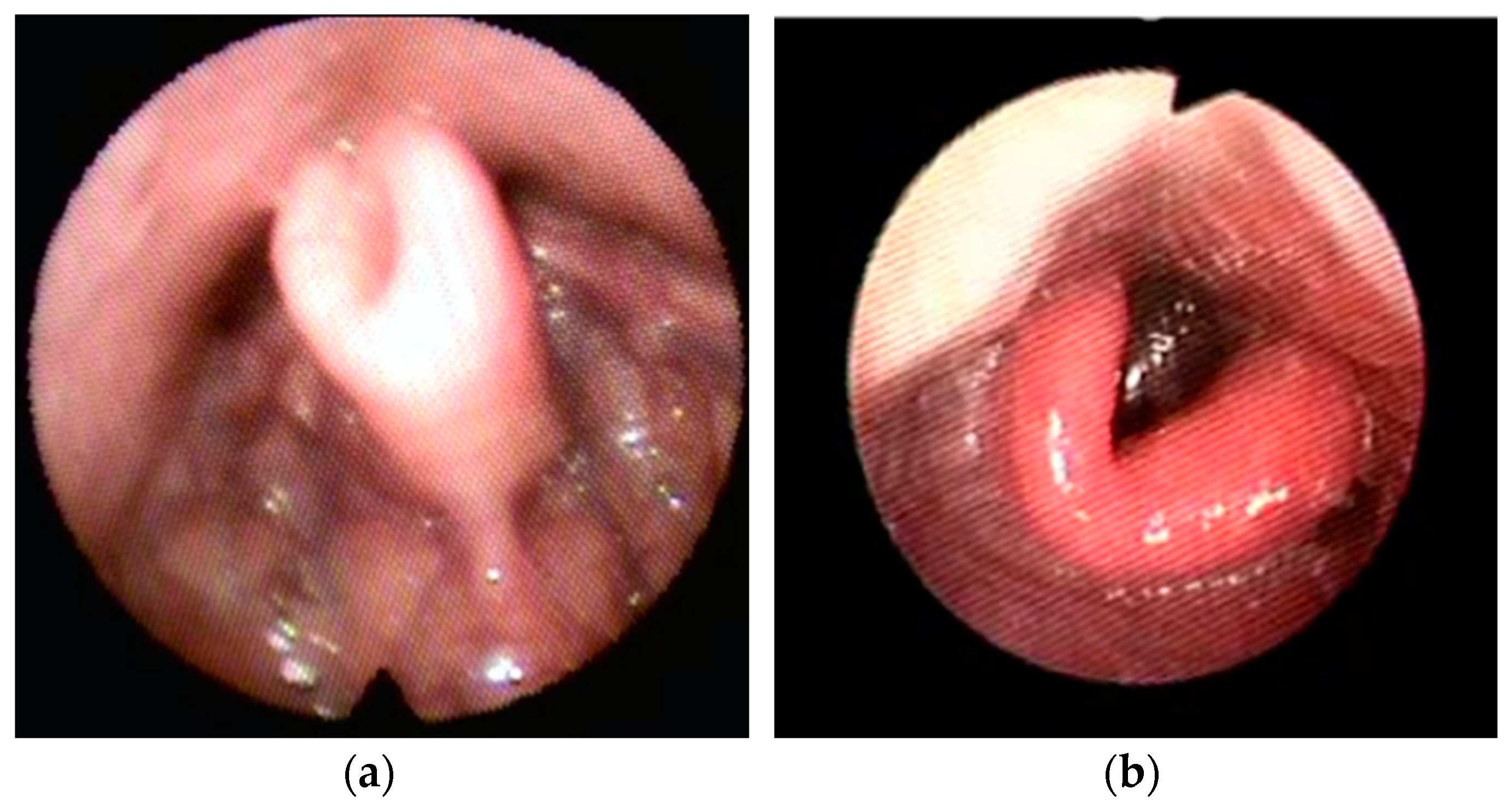
- Lateral–Lateral (LL) primary collapse with omega shape component “book type” in 15 patients (14.5%).
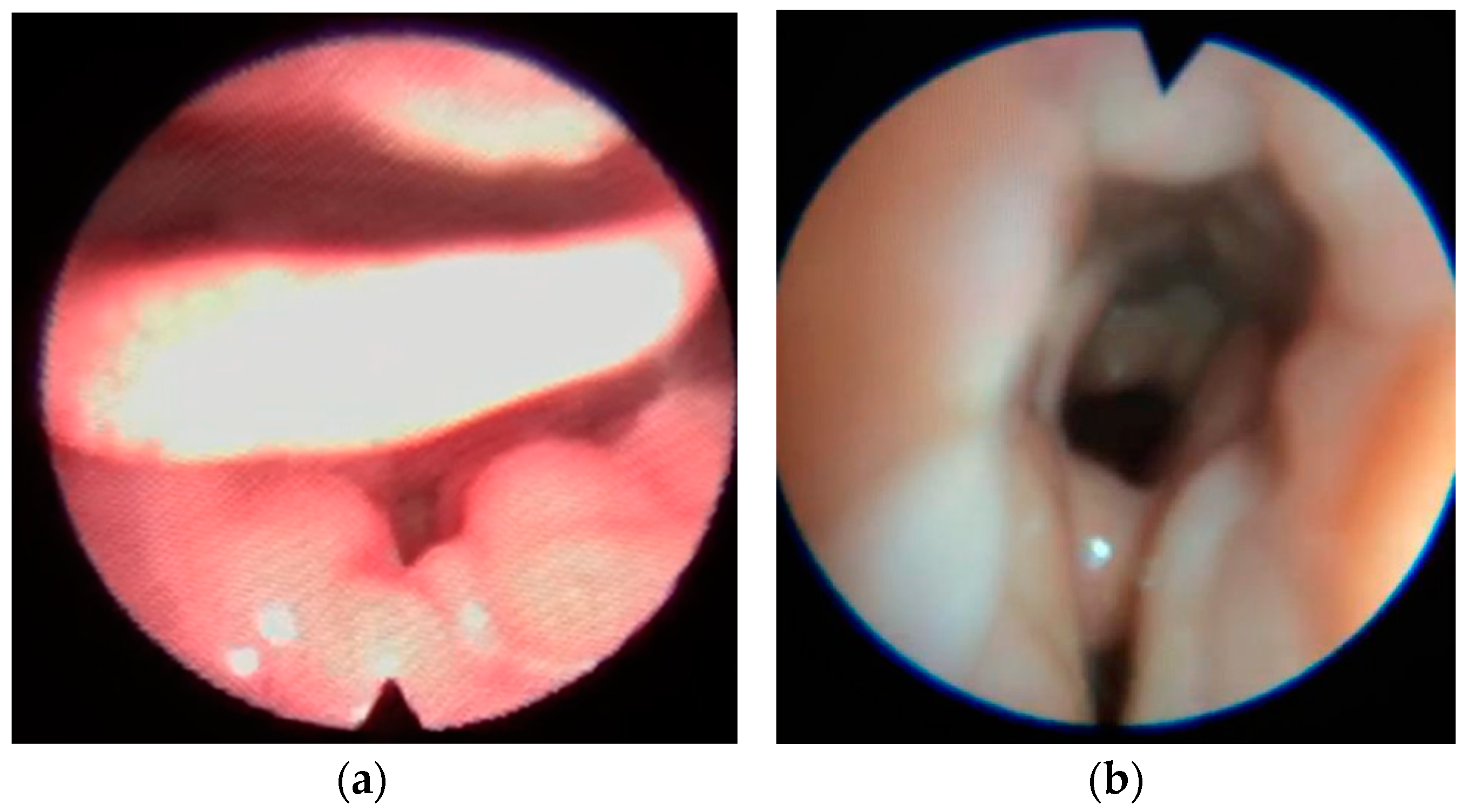
- Secondary collapse due to base tongue or lateral pharyngeal walls collapse in 25 patients (24%).
4. Discussion
- AP collapse with a rigid component (trapdoor).
- AP collapse with a hyperlax epiglottis (floppy).
- LL collapse with an omega-shaped epiglottis (book type).
- Epiglottic with lateral or book cracking, partial resection superior to 75%.
- Epiglottis with AP collapse “floppy” collapse, partial resection of 50% with epiglottopexy.
- Epiglottis with AP crack rigid collapse “trapdoor”, partial resection less than 50% with or without epiglottopexy.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.M.; Carter, S.G.; Carberry, J.C.; Eckert, D.J. Obstructive sleep apnea: Current perspectives. Nat. Sci. Sleep 2018, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Strollo, P.J.; Rogers, R. Obstructive sleep apnea. N. Engl. J. Med. 1996, 334, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef]
- Lurie, A. Obstructive Sleep Apnea in Adults. Adv. Cardiol. 2011, 46, 1–42. [Google Scholar] [CrossRef]
- Grunstein, R.R.; Stenlof, K.; Hedner, J.A.; Sjostrom, L. Impact of Self-Reported Sleep-Breathing Disturbances on Psychosocial Performance in the Swedish Obese Subjects (SOS) Study. Sleep 1995, 18, 635–643. [Google Scholar] [CrossRef]
- Rosario, I. Obstructive sleep apnea: A review and update. Minn. Med. 2011, 94, 44–48. [Google Scholar]
- Marin, J.M.; Agusti, A.; Villar, I.; Forner, M.; Nieto, D.; Carrizo, S.J.; Barbé, F.; Vicente, E.; Wei, Y.; Javier Nieto, F.; et al. Association between treated and untreated obstructive sleep apnea and risk of hypertension. JAMA 2012, 307, 2169–2176. [Google Scholar] [CrossRef]
- Findley, L.J.; Unverzagt, M.E.; Suratt, P.M. Automobile Accidents Involving Patients with Obstructive Sleep Apnea. Am. Rev. Respir. Dis. 2012, 138, 337–340. [Google Scholar] [CrossRef]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Martínez-García, M.Á.; Capote, F.; Campos-Rodríguez, F.; Lloberes, P.; Díaz De Atauri, M.J.; Somoza, M.; Masa, J.F.; González, M.; Sacristán, L.; Barbé, F.; et al. Effect of CPAP on blood pressure in patients with obstructive sleep apnea and resistant hypertension: The HIPARCO randomized clinical trial. JAMA 2013, 310, 2407–2415. [Google Scholar] [CrossRef] [PubMed]
- Vlachantoni, I.T.; Dikaiakou, E.; Antonopoulos, C.N.; Stefanadis, C.; Daskalopoulou, S.S.; Petridou, E.T. Effects of continuous positive airway pressure (CPAP) treatment for obstructive sleep apnea in arterial stiffness: A meta-analysis. Sleep Med. Rev. 2013, 17, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Camacho, M.; Riaz, M.; Capasso, R.; Ruoff, C.M.; Guilleminault, C.; Kushida, C.A.; Certal, V. The effect of nasal surgery on continuous positive airway pressure device use and therapeutic treatment pressures: A systematic review and meta-analysis. Sleep 2015, 38, 279–286A. [Google Scholar] [CrossRef] [PubMed]
- Certal, V.; Nishino, N.; Camacho, M.; Capasso, R. Reviewing the Systematic Reviews in OSA Surgery. Otolaryngol. Head Neck Surg. 2013, 149, 817–829. [Google Scholar] [CrossRef]
- Kezirian, E.J.; Hohenhorst, W.; de Vries, N. Drug-induced sleep endoscopy: The VOTE classification. Eur. Arch. Otorhinolaryngol. 2011, 268, 1233–1236. [Google Scholar] [CrossRef]
- Amos, J.M.; Durr, M.L.; Nardone, H.C.; Baldassari, C.M.; Duggins, A.; Ishman, S.L. Systematic Review of Drug-Induced Sleep Endoscopy Scoring Systems. Otolaryngol. Head Neck Surg. 2018, 158, 240–248. [Google Scholar] [CrossRef]
- Catalfumo, F.J.; Golz, A.; Westerman, S.T.; Gilbert, L.M.; Joachims, H.Z.; Goldenberg, D. The epiglottis and obstructive sleep apnoea syndrome. J. Laryngol. Otol. 1998, 112, 940–943. [Google Scholar] [CrossRef]
- Lan, M.C.; Liu, S.Y.C.; Lan, M.Y.; Modi, R.; Capasso, R. Lateral pharyngeal wall collapse associated with hypoxemia in obstructive sleep apnea. Laryngoscope 2015, 125, 2408–2412. [Google Scholar] [CrossRef]
- Tucker Woodson, B. A method to describe the pharyngeal airway. Laryngoscope 2015, 125, 1233–1238. [Google Scholar] [CrossRef]
- Torre, C.; Camacho, M.; Liu, S.Y.C.; Huon, L.K.; Capasso, R. Epiglottis collapse in adult obstructive sleep apnea: A systematic review. Laryngoscope 2016, 126, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Vallianou, K.; Chaidas, K. Surgical Treatment Options for Epiglottic Collapse in Adult Obstructive Sleep Apnoea: A Systematic Review. Life 2022, 12, 1845. [Google Scholar] [CrossRef] [PubMed]
- Ravesloot, M.J.L.; De Vries, N. One hundred consecutive patients undergoing drug-induced sleep endoscopy: Results and evaluation. Laryngoscope 2011, 121, 2710–2716. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, E.; Veugen, C.C.A.F.M.; Hardeman, J.A.; Copper, M.P. Drug-induced sleep endoscopy while administering CPAP therapy in patients with CPAP failure. Sleep Breath. 2021, 25, 391–398. [Google Scholar] [CrossRef]
- Kim, D.K.; Lee, J.W.; Lee, J.H.; Lee, J.S.; Na, Y.S.; Kim, M.J.; Lee, M.J.; Park, C.H. Drug induced sleep endoscopy for poor-responder to uvulopalatopharyngoplasty in patient with obstructive sleep apnea patients. Korean J. Otorhinolaryngol. Head Neck Surg. 2014, 57, 96–102. [Google Scholar] [CrossRef]
- Berry, R.B.; Brooks, R.; Gamaldo, C.E.; Harding, S.M.; Marcus, C.; Vaughn, B.V. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Version 2.0; American Academy of Sleep Medicine: Darien, IL, USA, 2012; Available online: www.aasmnet.org (accessed on 22 September 2023).
- Centers for Medicare & Medicaid Services. Continuous and Bi-Level Positive Airway Pressure (CPAP/BPAP) Devices: Complying with Documentation and Coverage Requirements. Available online: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-NetworkMLN/MLNProducts/downloads/PAP_DocCvg_Factsheet_ICN905064.pdf (accessed on 20 March 2015).
- Han, L.; Drover, D.R.; Chen, M.C.; Saxena, A.R.; Eagleman, S.L.; Nekhendzy, V.; Pritchard, A.; Capasso, R. EEG response of dexmedetomidine during drug induced sleep endoscopy. Front. Neurosci. 2023, 17, 1144141. [Google Scholar] [CrossRef]
- Kwon, O.E.; Jung, S.Y.; Al-Dilaijan, K.; Min, J.Y.; Lee, K.H.; Kim, S.W. Is epiglottis surgery necessary for obstructive sleep apnea patients with epiglottis obstruction? Laryngoscope 2019, 129, 2658–2662. [Google Scholar] [CrossRef]
- Fernandez-Julian, E.; Garcia-Perez, M.A.; Garcia-Callejo, J.; Ferrer, F.; Marti, F.; Marco, J. Surgical planning after sleep versus awake techniques in patients with obstructive sleep apnea. Laryngoscope 1999, 124, 1970–1974. [Google Scholar] [CrossRef]
- Spinowitz, S.; Kim, M.; Park, S.Y. Patterns of Upper Airway Obstruction on Drug-Induced Sleep Endoscopy in Patients with Sleep-Disordered Breathing with AHI <5. OTO Open 2017, 1, 2473974X17721483. [Google Scholar] [CrossRef]
- Koutsourelakis, I.; Safiruddin, F.; Ravesloot, M.; Zakynthinos, S.; de Vries, N. Surgery for obstructive sleep apnea: Sleep endoscopy determinants of outcome. Laryngoscope 2012, 122, 2587–2591. [Google Scholar] [CrossRef]
- Den Herder, C.; Van Tinteren, H.; De Vries, N. Hyoidthyroidpexia: A Surgical Treatment for Sleep Apnea Syndrome. Laryngoscope 2005, 115, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Vicini, C.; De Vito, A.; Benazzo, M.; Frassineti, S.; Campanini, A.; Frasconi, P.; Mira, E. The nose oropharynx hypopharynx and larynx (NOHL) classification: A new system of diagnostic standardized examination for OSAHS patients. Eur. Arch. Otorhinolaryngol. 2012, 269, 1297–1300. [Google Scholar] [CrossRef] [PubMed]
- Salama, S.; Kamel, E.; Omar, A.; Makhlouf, H.A.; Farghaly, S. Role of sleep endoscopy in obstructive sleep apnea syndrome. Egypt. J. Chest Dis. Tuberc. 2013, 62, 467–473. [Google Scholar] [CrossRef]
- Vonk, P.E.; Ravesloot, M.J.L.; Kasius, K.M.; van Maanen, J.P.; de Vries, N. Floppy epiglottis during drug-induced sleep endoscopy: An almost complete resolution by adopting the lateral posture. Sleep Breath. 2020, 24, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Verse, T.; Pirsig, W. Age-related changes in the epiglottis causing failure of nasal continuous positive airway pressure therapy. J. Laryngol. Otol. 1999, 113, 1022–1025. [Google Scholar] [CrossRef]
- Masárová, M.; Formánek, M.; Jor, O.; Novák, V.; Vrtková, A.; Matoušek, P.; Komínek, P.; Zeleník, K. Epiglottopexy Is a Treatment of Choice for Obstructive Sleep Apnea Caused by a Collapsing Epiglottis. Life 2022, 12, 1378. [Google Scholar] [CrossRef]
- Kim, H.Y.; Sung, C.M.; Jang, H.B.; Kim, H.C.; Lim, S.C.; Yang, H.C. Patients with epiglottic collapse showed less severe obstructive sleep apnea and good response to treatment other than continuous positive airway pressure: A case-control study of 224 patients. J. Clin. Sleep Med. 2021, 17, 413–419. [Google Scholar] [CrossRef]
- Roustan, V.; Barbieri, M.; Incandela, F.; Missale, F.; Camera, H.; Braido, F.; Mora, R.; Peretti, G. Transoral glossoepiglottopexy in the treatment of adult obstructive sleep apnoea: A surgical approach. ACTA Otorhinolaryngol. Ital. 2018, 38, 38–44. [Google Scholar] [CrossRef]
- Lugo, R.; Saldívar, K. Manual de Procedimientos Quirúrgicos en Ronquido y Apnea Obstructiva del Sueño. Nariz, Paladar Blando, Pared Lateral, Lengua, Epiglotis; Amolca: Medellín, Colombia, 2022. [Google Scholar]
- Salamanca, F.; Leone, F.; Bianchi, A.; Bellotto, R.G.S.; Costantini, F.; Salvatori, P. Surgical treatment of epiglottis collapse in obstructive sleep apnoea syndrome: Epiglottis stiffening operation. Acta Otorhinolaryngol. Ital. 2019, 39, 404–408. [Google Scholar] [CrossRef]
- Bourolias, C.; Hajiioannou, J.; Sobol, E.; Velegrakis, G.; Helidonis, E. Epiglottis reshaping using CO2 laser: A minimally invasive technique and its potent applications. Head Face Med. 2008, 4, 5–8. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Francia, C.; Lugo, R.; Moffa, A.; Casale, M.; Giorgi, L.; Iafrati, F.; Di Giovanni, S.; Baptista, P. Defining Epiglottic Collapses Patterns in Obstructive Sleep Apnea Patients: Francia-Lugo Classification. Healthcare 2023, 11, 2874. https://doi.org/10.3390/healthcare11212874
Francia C, Lugo R, Moffa A, Casale M, Giorgi L, Iafrati F, Di Giovanni S, Baptista P. Defining Epiglottic Collapses Patterns in Obstructive Sleep Apnea Patients: Francia-Lugo Classification. Healthcare. 2023; 11(21):2874. https://doi.org/10.3390/healthcare11212874
Chicago/Turabian StyleFrancia, Carlos, Rodolfo Lugo, Antonio Moffa, Manuele Casale, Lucrezia Giorgi, Francesco Iafrati, Simone Di Giovanni, and Peter Baptista. 2023. "Defining Epiglottic Collapses Patterns in Obstructive Sleep Apnea Patients: Francia-Lugo Classification" Healthcare 11, no. 21: 2874. https://doi.org/10.3390/healthcare11212874