
The Impact of Early Acupuncture on Bell’s Palsy Recurrence: Real-World Evidence from Korea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Ethics Statement
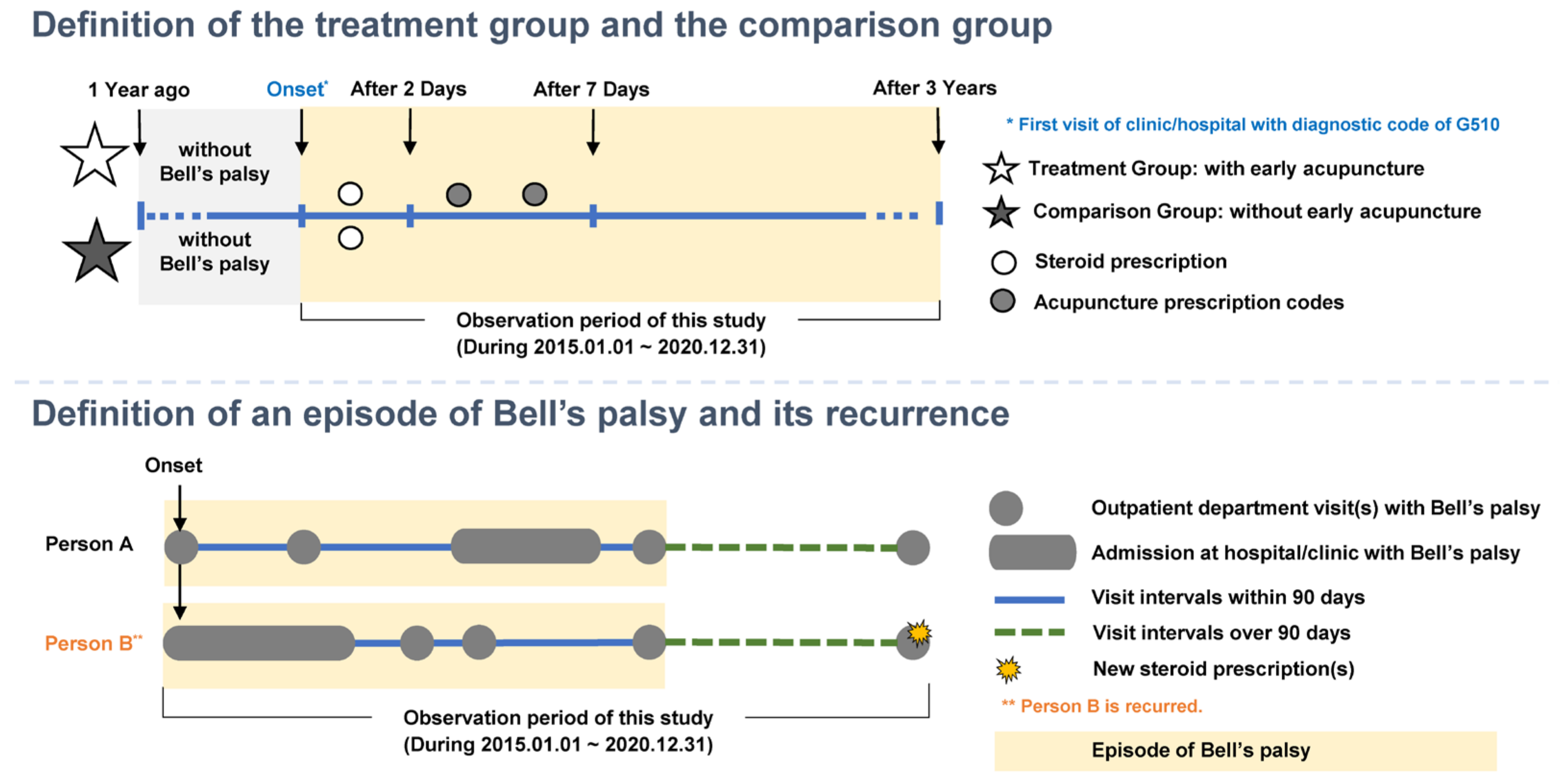
2.2. Study Design
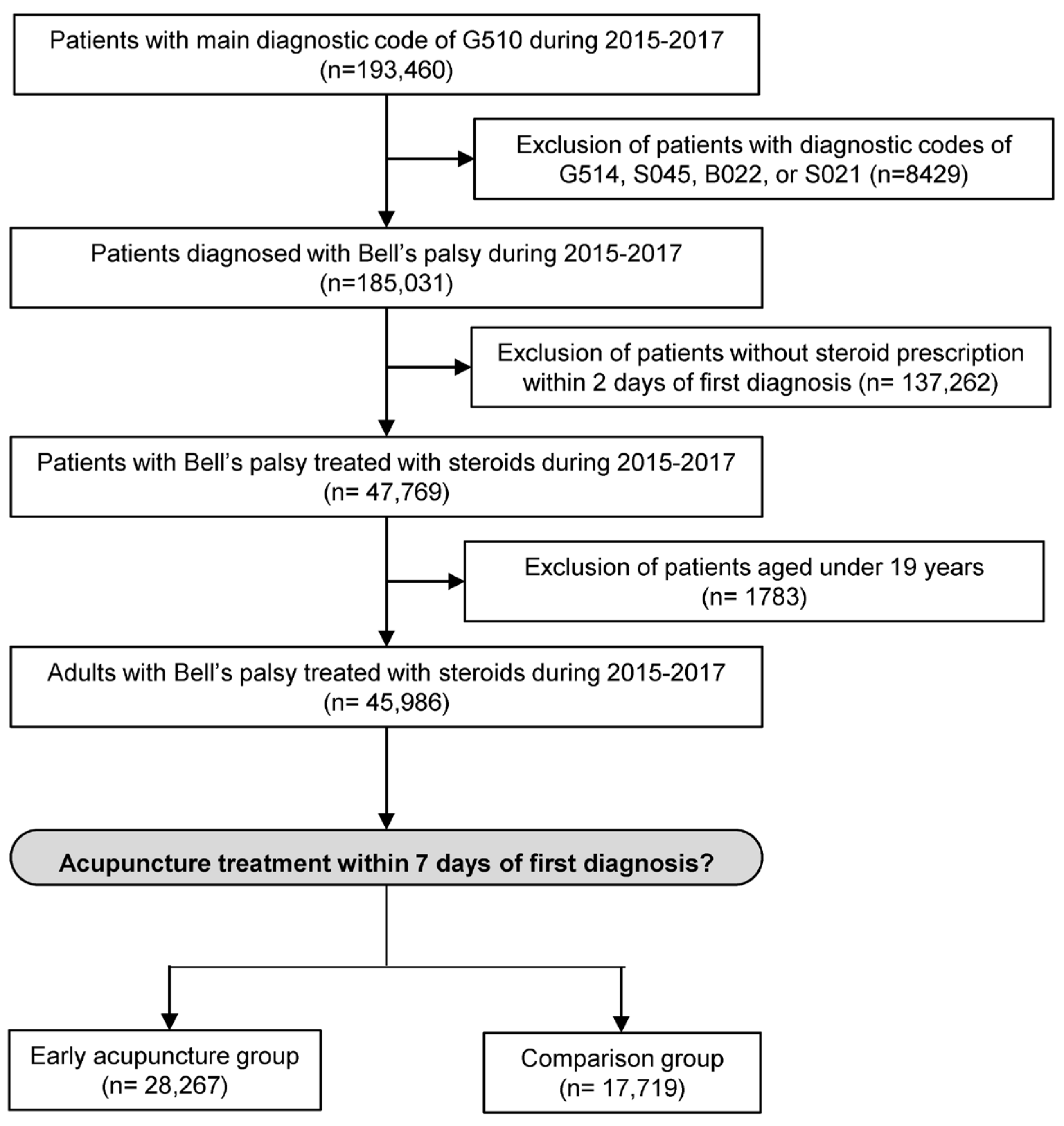
2.3. Definition of Study Population
2.4. Definition of Intervention
2.5. Definition of Outcome
2.6. Extraction of Demographic and Clinical Characteristics
2.7. Statistical Analyses
3. Results
3.1. Schematic Flow
3.2. Demographic and Clinical Characteristics
3.3. Factors Associated with Recurrence of Bell’s Palsy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baugh, R.F.; Basura, G.J.; Ishii, L.E.; Schwartz, S.R.; Drumheller, C.M.; Burkholder, R.; Deckard, N.A.; Dawson, C.; Driscoll, C.; Gillespie, M.B.; et al. Clinical Practice Guideline: Bell’s Palsy. Otolaryngol. Head Neck Surg. 2013, 149 (Suppl. S3), S1–S27. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, Y.H. Epidemiological trends of Bell’s palsy treated with steroids in Korea between 2008 and 2018. Muscle Nerve 2021, 63, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, S.; Hooper, R.; Hughes, R.; Burney, P. The epidemiology and treatment of Bell’s palsy in the UK. Eur. J. Neurol. 2002, 9, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Monini, S.; Lazzarino, A.I.; Iacolucci, C.; Buffoni, A.; Barbara, M. Epidemiology of Bell’s palsy in an Italian Health District: Incidence and case-control study. Acta Otorhinolaryngol. Ital. 2010, 30, 198. [Google Scholar] [PubMed]
- House, J.W.; Brackmann, D.E. Facial nerve grading system. Otolaryngol. Head Neck Surg. 1985, 93, 146–147. [Google Scholar] [CrossRef]
- Gilden, D.H. Clinical practice. Bell’s Palsy. N. Engl. J. Med. 2004, 351, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Adour, K.K.; Wingerd, J. Idiopathic facial paralysis (Bell’s palsy): Factors affecting severity and outcome in 446 patients. Neurology 1974, 24, 1112. [Google Scholar] [CrossRef]
- Engström, M.; Berg, T.; Stjernquist-Desatnik, A.; Axelsson, S.; Pitkäranta, A.; Hultcrantz, M.; Kanerva, M.; Hanner, P.; Jonsson, L. Prednisolone and valaciclovir in Bell’s palsy: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2008, 7, 993–1000. [Google Scholar] [CrossRef]
- Dong, S.H.; Jung, A.R.; Jung, J.; Jung, S.Y.; Byun, J.Y.; Park, M.S.; Kim, S.H.; Yeo, S.G. Recurrent Bell’s palsy. Clin. Otolaryngol. 2019, 44, 305–312. [Google Scholar] [CrossRef]
- Luijmes, R.E.; Pouwels, S.; Beurskens, C.H.G.; Kleiss, I.J.; Siemann, I.; Ingels, K.J.A.O. Quality of life before and after different treatment modalities in peripheral facial palsy: A systematic review. Laryngoscope 2017, 127, 1044–1051. [Google Scholar] [CrossRef]
- Saadi, R.; Shokri, T.; Schaefer, E.; Hollenbeak, C.; Lighthall, J.G. Depression Rates after Facial Paralysis. Ann. Plast. Surg. 2019, 83, 190–194. [Google Scholar] [CrossRef]
- Sullivan, F.M.; Swan, I.R.C.; Donnan, P.T.; Morrison, J.M.; Smith, B.H.; McKinstry, B.; Davenport, R.J.; Vale, L.D.; Clarkson, J.E.; Hammersley, V.; et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N. Engl. J. Med. 2007, 357, 1598–1607. [Google Scholar] [CrossRef]
- Madhok, V.B.; Gagyor, I.; Daly, F.; Somasundara, D.; Sullivan, M.; Gammie, F.; Sullivan, F. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst. Rev. 2016, 7, CD001942. [Google Scholar] [CrossRef]
- Napadow, V.; Kaptchuk, T.J. Patient characteristics for outpatient acupuncture in Beijing, China. J. Altern. Complement. Med. 2004, 10, 565–572. [Google Scholar] [CrossRef]
- Kim, D.; Jung, B.; Cho, M.-U.; Song, S.-B.; Chung, S.H.; Park, T.-Y.; Ha, I.-H. Analysis of medical services provided to patients with peripheral facial palsy in Korea: A descriptive, cross-sectional study of the health insurance review and assessment service national patient sample database. BMC Health Serv. Res. 2021, 21, 1178. [Google Scholar] [CrossRef]
- Lee, S.M.K.; Lee, S.; Park, J.H.; Park, J.J.; Lee, S. A close look at an integrative treatment package for Bell’s palsy in Korea. Complement. Ther. Clin. Pract. 2017, 26, 76–83. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; He, L.; Zhou, D.; Li, N. Acupuncture for Bell’s palsy. Cochrane Database Syst. Rev. 2010, 8, CD002914. [Google Scholar] [CrossRef]
- Li, P.; Qiu, T.; Qin, C. Efficacy of Acupuncture for Bell’s Palsy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2015, 10, e0121880. [Google Scholar] [CrossRef]
- Yang, L.-S.; Zhou, D.-F.; Zheng, S.-Z.; Zhao, B.-M.; Li, H.-G.; Chen, Q.-Q.; Zhong, Y.; Yang, H.-Z.; Zhang, K.; Tang, C.-Z. Early intervention with acupuncture improves the outcome of patients with Bell’s palsy: A propensity score-matching analysis. Front. Neurol. 2022, 13, 943453. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Zheng, Q.; Shi, Y.; Zhang, L.; Zhao, L.; Zhou, S.; Zhang, W.; Cao, W.; Liu, Y.; Li, Y. Association of Patients’ Characteristics with Acupuncture Treatment Outcomes in Treating Bell’s Palsy: Results from a Randomised Controlled Trial. Evid.-Based Complement. Altern. Med. 2019, 2019, 6073484. [Google Scholar] [CrossRef] [PubMed]
- Zou, Z. Comparison of Efficacy and Safety of Acupuncture and Moxibustion in Acute Phase and Non-acute Phase of Bell’s Palsy: A meta-analysis. Neuroendocrinol. Lett. 2021, 42, 438–445. [Google Scholar] [PubMed]
- Tong, F.M.; Chow, S.K.; Chan, P.Y.B.; Wong, A.K.W.; Wan, S.S.Y.; Ng, R.K.W.; Chan, G.; Chan, W.S.; Ng, A.; Law, C.K. A prospective randomised controlled study on efficacies of acupuncture and steroid in treatment of idiopathic peripheral facial paralysis. Acupunct. Med. 2009, 27, 169–173. [Google Scholar] [CrossRef]
- Jeong, J.; Yoon, S.R.; Lim, H.; Oh, J.; Choi, H.S. Risk factors for Bell’s palsy based on the Korean National Health Insurance Service National Sample Cohort data. Sci. Rep. 2021, 11, 23387. [Google Scholar] [CrossRef]
- Wu, X.; Li, Y.; Zhu, Y.-H.; Zheng, H.; Chen, Q.; Li, X.-Z.; Luo, L.; Zeng, F.; Huang, W.-J.; Zhao, L.; et al. Clinical practice guideline of acupuncture for bell’s palsy. World J. Tradit. Chin. Med. 2015, 1, 53. [Google Scholar] [CrossRef]
- Korean Acupuncture and Moxibustion Medicine Society. Clinical Practice Guideline of Korean Medicine for Facial Palsy. National Institute for Korean Medicine Development. 2021. Available online: https://nikom.or.kr/nckm/module/practiceGuide/view.do?guide_idx=150&menu_idx=14 (accessed on 10 December 2023).
- Chang, Y.-S.; Choi, J.E.; Kim, S.W.; Baek, S.-Y.; Cho, Y.-S. Prevalence and associated factors of facial palsy and lifestyle characteristics: Data from the Korean National Health and Nutrition Examination Survey 2010–2012. BMJ Open 2016, 6, e012628. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef]
- Yoo, M.C.; Soh, Y.; Chon, J.; Lee, J.H.; Jung, J.; Kim, S.S.; You, M.-W.; Byun, J.Y.; Kim, S.H.; Yeo, S.G. Evaluation of Factors Associated with Favorable Outcomes in Adults with Bell Palsy. JAMA Otolaryngol.–Head Neck Surg. 2020, 146, 256–263. [Google Scholar] [CrossRef]
- Peitersen, E. Bell’s palsy: The spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Oto-Laryngol. 2002, 122, 4–30. [Google Scholar] [CrossRef]
- Pitts, D.B.; Adour, K.K.; Hilsinger, R.L. Recurrent Bell’s palsy: Analysis of 140 patients. Laryngoscope 1988, 98, 535–540. [Google Scholar] [CrossRef]
- Chung, D.H.; Park, D.C.; Byun, J.Y.; Park, M.S.; Lee, S.Y.; Yeo, S.G. Prognosis of patients with recurrent facial palsy. Eur. Arch. Otorhinolaryngol. 2012, 269, 61–66. [Google Scholar] [CrossRef]
- Mancini, P.; Bottaro, V.; Capitani, F.; De Soccio, G.; Prosperini, L.; Restaino, P.; De Vincentiis, M.; Greco, A.; Bertoli, G.A.; De Seta, D. Recurrent Bell’s palsy: Outcomes and correlation with clinical comorbidities. Acta Otorhinolaryngol. Ital. 2019, 39, 316–321. [Google Scholar] [CrossRef]
- Kikuoka, Y.; Haginomori, S.-I.; Ayani, Y.; Jin-nin, T.; Ichihara, T.; Inaka, Y.; Ozaki, A.; Inui, T.; Kawata, R. Recurrent facial palsy: Characteristics of ipsilateral and alternative palsies of 104 cases. Auris Nasus Larynx 2022, 50, 507–512. [Google Scholar] [CrossRef]
- Kim, S.Y.; Wee, J.H.; Min, C.; Yoo, D.-M.; Choi, H.G. Relationship between Bell’s Palsy and Previous Statin Use: A Case/Non-Case Study. Int. J. Environ. Res. Public Health 2020, 17, 8408. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, Y. A Clinical Study of Collaboration between Western and Korean Medicine for the Treatment of Peripheral Facial Palsy in a Korean Medicine Hospital. J. Acupunct. Res. 2020, 37, 161–166. [Google Scholar] [CrossRef]
- Yoon, S.Y.; Lee, J.H.; Kim, K.; Kim, J.H. Qualitative Study on the Experience of Patients with Facial Palsy Symptoms Treated with Korean Medicine after Western Treatment. J. Korean Med. Ophthalmol. Otolaryngol. Dermatol. 2022, 35, 1–30. [Google Scholar]
- Lee, S.M.; Yang, S.P.; Kim, E.S.; Lee, M.J.; Park, J.M.; Nam, D.W.; Kang, J.W.; Lee, S.H. Admission care for Bell’s palsy patients: A qualitative report on patient experiences. J. Acupunct. Res. 2013, 30, 11–23. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 45,986) | Early Acupuncture (n = 28,267) | Comparison (n = 17,719) | p Value | ||
|---|---|---|---|---|---|
| Demographics | |||||
| Age (years) | 53.8 (15.7) | 54.7 (15.2) | 52.3 (16.2) | <0.0001 | |
| Sex | Women | 22,949 (49.9%) | 14,370 (50.8%) | 8579 (48.4%) | <0.0001 |
| Men | 23,037 (50.1%) | 13,897 (49.2%) | 9140 (51.6%) | ||
| Clinical characteristics | |||||
| Onset season | Warm (7–10) | 15,312 (33.3%) | 9385 (33.2%) | 5927 (33.5%) | 0.6935 |
| Transitional (4–6) | 10,948 (23.8%) | 6766 (23.9%) | 4182 (23.6%) | ||
| Cold (11–3) | 19,726 (42.9%) | 12,116 (42.9%) | 7610 (42.9%) | ||
| Treatment duration | Under 90 days | 34,596 (75.2%) | 19,708 (69.7%) | 14,888 (84.0%) | <0.0001 |
| Over 90 days | 11,390 (24.8%) | 8559 (30.3%) | 2831 (16.0%) | ||
| Comorbidities | |||||
| Diabetes | No | 32,778 (71.3%) | 20,249 (71.6%) | 12,529 (70.7%) | 0.0330 |
| Yes | 13,208 (28.7%) | 8018 (28.4%) | 5190 (29.3%) | ||
| Hypertension | No | 29,555 (64.3%) | 17,991 (63.7%) | 11,564 (65.3%) | 0.0004 |
| Yes | 16,431 (35.7%) | 10,276 (36.3%) | 6155 (34.7%) | ||
| Dyslipidemia | No | 25,558 (55.6%) | 15,647 (55.4%) | 9911 (55.9%) | 0.2244 |
| Yes | 20,428 (44.4%) | 12,620 (44.6%) | 7808 (44.1%) | ||
| Cardiovascular diseases | No | 41,401 (90.0%) | 25,480 (90.1%) | 15,921 (89.9%) | 0.3215 |
| Yes | 4585 (10.0%) | 2787 (9.9%) | 1798 (10.1%) | ||
| Cerebrovascular diseases | No | 39,232 (85.3%) | 24,389 (86.3%) | 14,843 (83.8%) | <0.0001 |
| Yes | 6754 (14.7%) | 3878 (13.7%) | 2876 (16.2%) | ||
| Recurrence | |||||
| Recurrence | No | 45,168 (98.2%) | 27,806 (98.4%) | 17,362 (98.0%) | 0.0026 |
| Yes | 818 (1.8%) | 461 (1.6%) | 357 (2.0%) | ||
| Time to recurrence (days) | 774.6 (474.2) | 834.5 (467.8) | 697.2 (470.9) | <0.0001 | |
| Concurrent treatment | |||||
| Moxibustion | Yes | 23,114 (50.3%) | 17,089 (60.5%) | 6025 (34.0%) | <0.0001 |
| Cupping | Yes | 29,771 (64.7%) | 21,186 (74.9%) | 8585 (48.4%) | <0.0001 |
| Physical therapy | Yes | 34,211 (74.4%) | 24,554 (86.9%) | 9657 (54.5%) | <0.0001 |
| Not Recurred (n = 45,168) | Recurred (n = 818) | p Value | ||
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 53.8 (15.7) | 51.0 (15.0) | <0.0001 | |
| Sex | Women | 22,522 (49.9%) | 427 (52.2%) | 0.1918 |
| Men | 22,646 (50.1%) | 391 (47.8%) | ||
| Clinical characteristics | ||||
| Onset season | Warm (7–10) | 15,044 (33.3%) | 268 (32.8%) | 0.9203 |
| Transitional (4–6) | 10,749 (23.8%) | 199 (24.3%) | ||
| Cold (11–3) | 19,375 (42.9%) | 351 (42.9%) | ||
| Treatment duration | Under 90 days | 34,007 (75.3%) | 569 (69.6%) | 0.0022 |
| Over 90 days | 11,141 (24.7%) | 249 (30.4%) | ||
| Early acupuncture | No | 17,342 (38.4%) | 357 (43.6%) | 0.0026 |
| Yes | 27,806 (61.6%) | 461 (56.4%) | ||
| Comorbidities | ||||
| Diabetes | No | 32,202 (71.3%) | 576 (70.4%) | 0.5853 |
| Yes | 12,966 (28.7%) | 242 (29.6%) | ||
| Hypertension | No | 29,017 (64.2%) | 538 (65.8%) | 0.3771 |
| Yes | 16,151 (35.8%) | 280 (34.2%) | ||
| Dyslipidemia | No | 25,129 (55.6%) | 429 (52.4%) | 0.0702 |
| Yes | 20,039 (44.4%) | 389 (47.6%) | ||
| Cardiovascular diseases | No | 40,657 (89.9%) | 744 (91.0%) | 0.4096 |
| Yes | 4511 (10.0%) | 74 (9.0%) | ||
| Cerebrovascular diseases | No | 38,522 (85.3%) | 710 (86.6%) | 0.2515 |
| Yes | 6646 (14.7%) | 108 (13.2%) |
| Estimate (SE) | Odds Ratio | 95% CI | p Value | ||
|---|---|---|---|---|---|
| Intercept | −3.67 (0.33) | – | – | <0.0001 | |
| Age (years) | −0.02 (0.00) | 0.98 | 0.98–0.99 | <0.0001 | |
| Sex | Women | – | – | – | – |
| Men | −0.14 (0.07) | 0.89 | 0.77–1.02 | 0.0471 | |
| Onset season | Warm (7–10) | – | – | – | – |
| Transitional (4–6) | 0.02 (0.08) | 1.04 | 0.87–1.26 | 0.8400 | |
| Cold (11–3) | 0.01 (0.09) | 1.03 | 0.88–1.21 | 0.9044 | |
| Treatment duration | Under 90 days | – | – | – | – |
| Over 90 days | 0.00 (0.00) | 1.47 | 1.25–1.71 | 0.0064 | |
| Early acupuncture | No | – | – | – | – |
| Yes | −0.25 (0.07) | 0.79 | 0.68–0.91 | 0.0004 | |
| Diabetes | No | – | – | – | – |
| Yes | 0.08 (0.09) | 1.09 | 0.91–1.30 | 0.3969 | |
| Hypertension | No | – | – | – | – |
| Yes | 0.04 (0.09) | 1.04 | 0.86–1.24 | 0.6889 | |
| Dyslipidemia | No | – | – | – | – |
| Yes | 0.24 (0.08) | 1.29 | 1.09–1.52 | 0.0046 | |
| Cardiovascular diseases | No | – | – | – | – |
| Yes | −0.05 (0.13) | 0.95 | 0.73–1.22 | 0.6870 | |
| Cerebrovascular diseases | No | – | – | – | |
| Yes | −0.07 (0.11) | 0.93 | 0.75–1.15 | 0.5541 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Lee, S.; Yang, C.; Ahn, E. The Impact of Early Acupuncture on Bell’s Palsy Recurrence: Real-World Evidence from Korea. Healthcare 2023, 11, 3143. https://doi.org/10.3390/healthcare11243143
Choi Y, Lee S, Yang C, Ahn E. The Impact of Early Acupuncture on Bell’s Palsy Recurrence: Real-World Evidence from Korea. Healthcare. 2023; 11(24):3143. https://doi.org/10.3390/healthcare11243143
Chicago/Turabian StyleChoi, Yujin, Suji Lee, Changsop Yang, and Eunkyoung Ahn. 2023. "The Impact of Early Acupuncture on Bell’s Palsy Recurrence: Real-World Evidence from Korea" Healthcare 11, no. 24: 3143. https://doi.org/10.3390/healthcare11243143
APA StyleChoi, Y., Lee, S., Yang, C., & Ahn, E. (2023). The Impact of Early Acupuncture on Bell’s Palsy Recurrence: Real-World Evidence from Korea. Healthcare, 11(24), 3143. https://doi.org/10.3390/healthcare11243143