
Treatment of Esophago–Airway Fistula after Esophageal Resection

Abstract
:1. Introduction
2. Material and Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Patient-Inclusion Criteria
- Patients after radical esophagectomy R0.
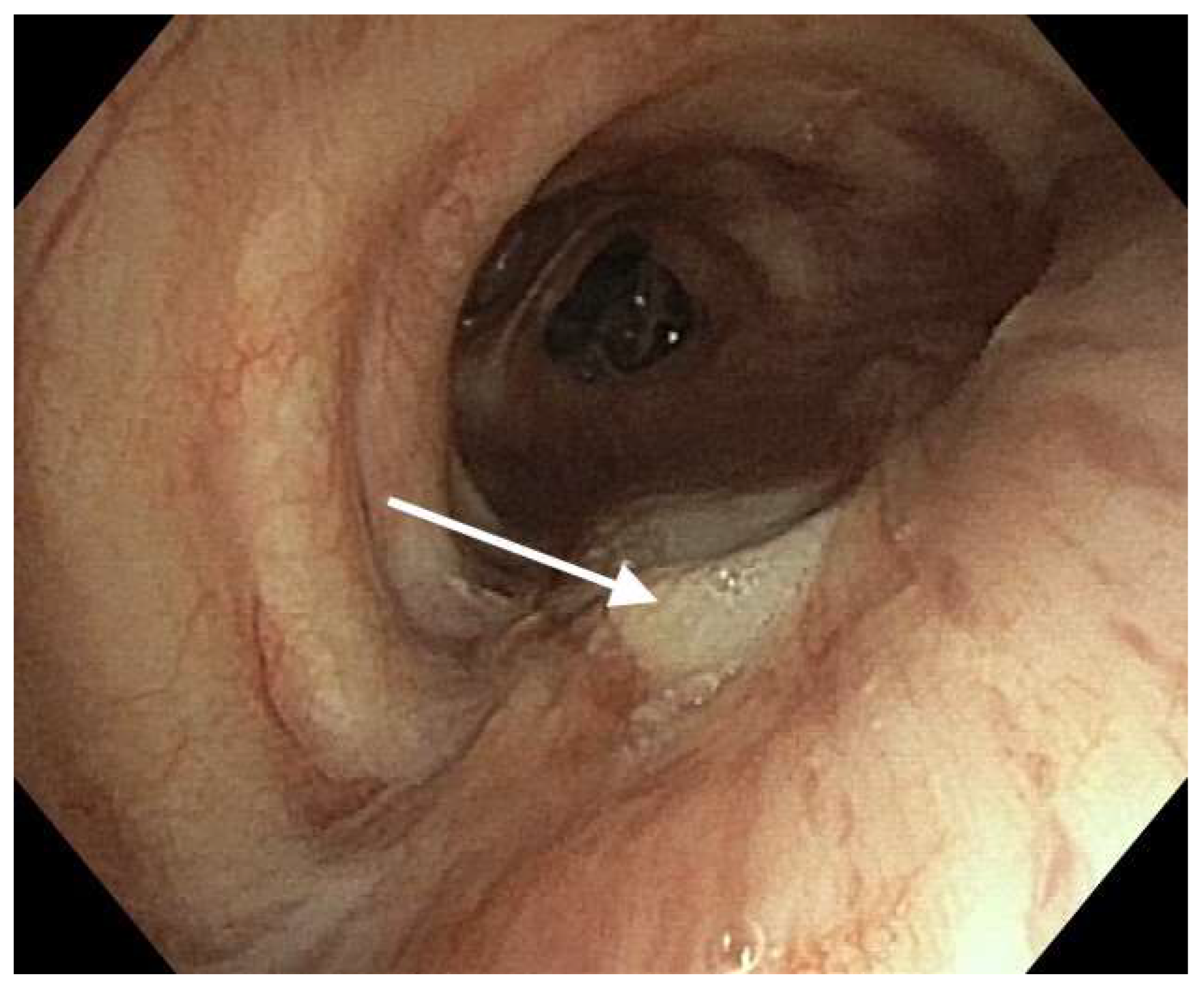
- Patients with an endoscopically confirmed EAF.
- Patients undergoing chemoradiotherapy for a cancer other than esophageal cancer and esophageal surgery resulting in an EAF.
2.1.2. Patient-Exclusion Criteria
- Patients after non-radical esophageal resection with an R1 feature.
- Patients after intraoperative injury to the bronchial tree.
- Patients with confirmed leakage only in the esophagogastric anastomosis.
- Patients with a preoperatively confirmed EAF in the course of esophageal cancer.
- Severe patient condition disqualifying them from surgical treatment.
2.2. Surgical Technique
2.2.1. Open Esophageal Resection (OER)
2.2.2. Esophageal Resection Using a Minimally Invasive Technique (MIT)
2.2.3. Intraoperative Ventilation
2.3. Surgical Treatment
Patients with Postoperative EAF
- Primary repair was performed in patients with an anastomotic leak of no more than 2 cm and no macroscopic evidence of gastric conduit necrosis. A fistula in the tracheo-bronchial tree (TBT) was repaired when it was no larger than 2 cm. The suture line was covered by an intercostal muscle flap (IMF) or latissimus dorsi muscle (LDM), GOF, and a conduit.
- Patients who did not meet the criteria for primary repair were eligible for esophageal diversion and bronchial tree fistuloplasty. A fistuloplasty was performed using either an IMF, pectoralis major muscle (PMM), LDM, GOF, or a biomaterial.
- Conservative treatment was initiated in patients who had a fistula of up to 1 cm in size, no pleural fluid on CT scan, distended pulmonary parenchyma without pneumothorax, air leakage, and a gastric graft covering the fistula. All patients were started on broad-spectrum antibiotic therapy. Control bronchoscopies were performed on postoperative days 1, 3, 5, and 7.
- Use of TBT or esophageal stents were used in patients whose clinical condition prohibited surgical treatment or supportive treatment was ineffective.
2.4. IMF Technique
2.5. Fistula Greater Than 2 cm—Technique
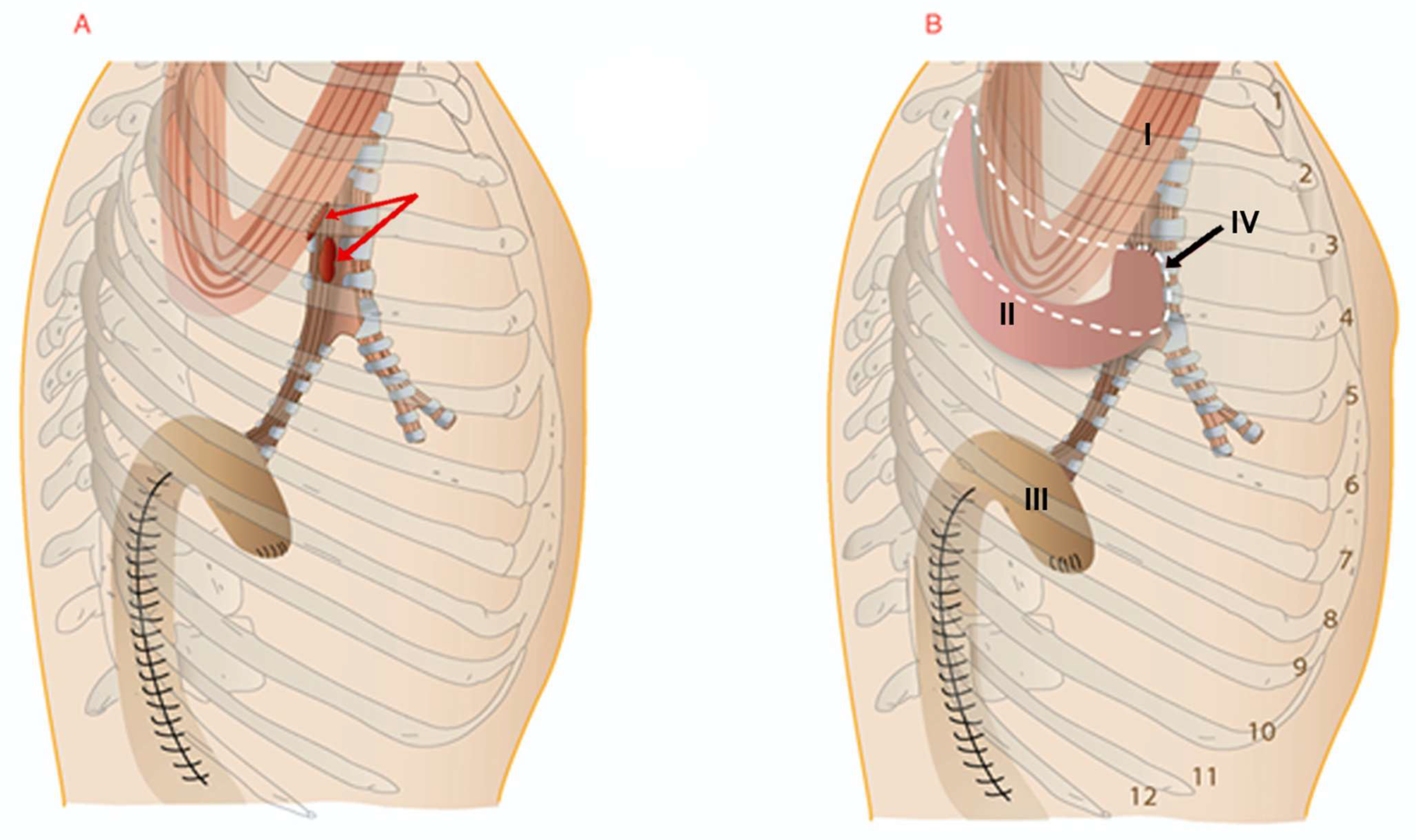
- Fistula after intraoperative repair of a tracheobronchial tree (TBT) injury
- Esophageal anastomotic leak with a fistula in the TBT without conduit necrosis
- Esophageal anastomotic leak with a fistula in the TBT with conduit necrosis
- Fistula in the TBT without evidence of an esophageal anastomotic leak
- Lung parenchyma fistula with or without evidence of an esophageal anastomotic leak
Follow-Up
2.6. Statistical Analysis
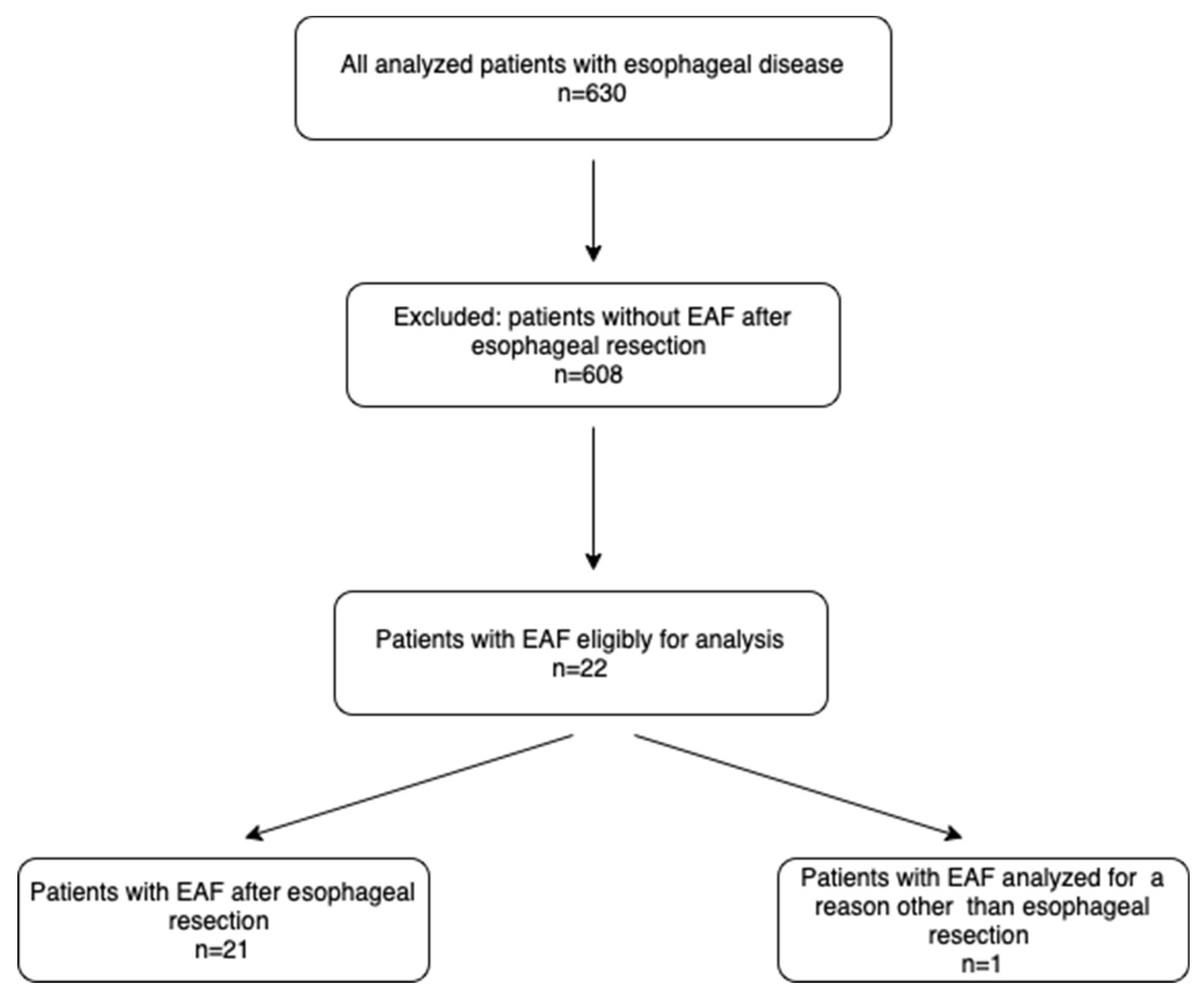
3. Results
3.1. Patient Characteristics
3.2. Characteristic of the Study Group
- thirteen (59.1%) patients had a bronchial fistula in the left main bronchus,
- seven (31.2%) developed a tracheal fistula,
- one (4.5%) patient developed a fistula to the right bronchus,
- one (4.5%) patient developed a fistula to the right lower lobe
3.3. Surgical Treatment and Outcomes (Table 1)
3.3.1. Primary Fistula Treatment without Esophageal Diversion

{kind=link}
{kind=link}
{kind=link}
| No/Sex/Age | Indication for Esophagectomy | Type of Fistula | Location of Damage of the Bronchial Tree | Diagnosis of Damage Time | Type of Surgical Repair | Restoration of Alimentary Tract | Results | Post Operative Survival/Days |
|---|---|---|---|---|---|---|---|---|
| 1/M/52 | SCC | BF type II | LMB | PD (6) | Stenting of LMB | - | Death | |
| 2/M/58 | SCC | BF type II (suspected) | LMB | PD (10) | Conservative | - | Good | 269 |
| 3/M/68 | SCC | BF type II | LMB | PD (7) | Suture of LMB and ICF plastic DE | Colon | Good | 485 |
| 4/M/72 | SCC | BF type II | RMB | PD (7) | Suture of RMB and plastic IMF, DE | No restoration due to dissemination | Bad | 268 |
| 5/M/65 | SCC | BF type II | LMB | PD (7) | Suture of LMB and IMF, DE | Colon | Good | 895 |
| 6/M/63 | SCC | BF type II | RMB | PD (8) | Suture of RMB and IMF, DE | Colon | Good | 528 |
| 7/M/69 | SCC | BF type II | LMB | PD (7) | Plastic with biomaterial, DE | Colon | Good | 579 |
| 8/M/74 | AEG | BF type II | LMB | PD (10) | Plastic with biomaterial, DE | No restoration due to dissemination | Good | 295 |
| 9/M/68 | SCC | BF type II | LMB | PD (8) | Suture of RMB and IMF, DE | Colon | Good | 285 |
| 10/M/55 | SCC | TF type II, F-LRL type IV | T, LRL | PD (7) | Suture of T and PMM plastic. After 2 years, hemorrhage, resection of the gastric graft, DE. Wedge resection of the lung parenchyma with fistula of the LRL. | Colon | Good | 369 |
| 11/M/68 | AEG | BF type I | RMB | PD (8) | Primary suture of RMB and IMF, anastomosis plastic, recurrence of esophageal fistula, stenting | - | Bad | 85 |
| 12/F/63 | SCC | TF type II | T | PD (7) | Suture of LMB and IMF, DE | Colon | Good | 469 |
| 13/M/50 | SCC | TF type I | T | PD (8) | Primary treatment | LDM | Bad—fistula recurrence | 356 |
| 14/F/17 | HL | TF | T | Stenting injury | Primary McKeown operation, suture of trachea and GOP | Gastric conduit | Good | Alive |
| 15/M/69 | SCC | BF type I | LMB | PD (9) | Primary suture of esophago-gastric anastomosis, myoplasty of the fistula IMF | Gastric conduit | Good | 725 |
| 16/M/64 | SCC | TF type II | T | PD (12) | Suture of fistula myoplastic with IMF, DE | Colon | Good | 586 |
| 17/M/62 | SCC | BF type II | LMB | PD (11) | Suture of fistula myoplastic with IMF, DE | Colon | Good | 489 |
| 18/F/52 | AEG | BF type II | LMB | PD (7) | Suture of fistula myoplastic with ICF, decortication of the right lung, DE | Colon | Good | 701 |
| 19/M/58 | SCC | BF type II | LMB | PD (12) | Suture of fistula myoplastic with IMF, DE | Colon | Good | 735 |
| 20 20 M/68 | SCC | BF type II | LMB | PD (10) | Suture of fistula myoplastic with IMF, DE | Colon | Good | 690 |
| 21/M/55 | SCC | BF type II | LMB | PD (8) | Suture of fistula myoplastic with IMF, DE | Colon | Good | Alive |
| 22/M55 | SCC | BF type II | URB | PD (12) | Primary esophago-gastric re-anastomosis, URL | - | Good | Alive |
3.3.2. Secondary Fistula Treatment with Diversion of the Esophagus
3.3.3. Stenting
3.3.4. Conservative Treatment
3.4. Bacterial Characteristics and Septic Threats
3.5. Postoperative Management
3.6. Restoring the Continuity of the Gastrointestinal Tract
Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tapias, L.F.; Mathisen, D.J.; Wright, C.D.; Wain, J.C.; Gaissert, H.A.; Muniappan, A.; Lanuti, M.; Donahue, D.M.; Morse, C.R. Outcomes with Open and Minimally Invasive Ivor Lewis Esophagectomy After Neoadjuvant Therapy. Ann. Thorac. Surg. 2016, 101, 1097–1103. [Google Scholar] [CrossRef]
- Houssein, A.; Harris, Y.K.; Awab, A.; Keddissi, J.L. Bronchoscopic advances in the management of aerodigestive fistulas. J. Thorac. Dis. 2018, 10, 5636–5647. [Google Scholar]
- Lambertz, R.; Holscher, A.H.; Bludau, M.; Leers, J.M.; Gutschow, C.; Schroder, W. Management of tracheo- or bron-choesophageal fistula after Ivor-Lewis esophagectomy. World J. Surg. 2016, 40, 1680–1687. [Google Scholar] [CrossRef]
- International Union Against Cancer (UICC). TNM Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2017. [Google Scholar]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.B.; Hulshof, M.C.C.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; Richel, D.J.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; et al. CROSS Group Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef]
- Hoeppner, J.; Lordick, F.; Brunner, T.; Glatz, T.; Bronsert, P.; Röthling, N.; Schmoor, C.; Lorenz, D.; Ell, C.; Hopt, U.T.; et al. ESOPEC: Prospective randomized controlled multicenter phase III trial comparing perioperative chemotherapy (FLOT protocol) to neoadjuvant chemoradiation (CROSS protocol) in patients with adenocarcinoma of the esophagus (NCT02509286). BMC Cancer 2016, 19, 503. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensiv. Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Tapias, L.; Wright, C.D.; Lanuti, M.X.; Geissert, H.A.; Mathisen, D.J.; Muniappan, A. Surgical Management of Post-Esophagectomy Tracheo-Bronchial-Esophageal Fistula. Ann. Thorac. Surg. 2018, 106, 1640–1646. [Google Scholar] [CrossRef]
- Rosskopfova, P.; Perentes, J.Y.; Schäfer, M.; Krueger, T.; Lovis, A.; Dorta, G.; Baeriswyl, M.; Ris, H.-B.; Gonzalez, M. Repair of challenging non-malignant tracheo- or broncho-oesophageal fistulas by extrathoracic muscle flaps. Eur. J. Cardio Thorac. Surg. 2017, 51, 844–851. [Google Scholar] [CrossRef]
- Schweigert, M.; Dubecz, A.; Beron, M.; Muschweck, H.; Stein, H.J. Managament of anastomotic leakage-induced tracheo-bronchial fistula following oesophagectomy: The role of endoscopic stents insertion. Eur. J. Cardiothorac. Surg. 2012, 41, e74–e80. [Google Scholar] [CrossRef]
- Wang, C.; Li, C.; Yang, X. The classification and treatment strategies of post-esophagectomy airway-gastric fistula. J. Thorac. Dis. 2020, 12, 3602–3610. [Google Scholar] [CrossRef] [PubMed]
- Bertheuil, N.; Duisit, J.; Isola, N.; Lengelé, B.; Bergeat, D.; Meunier, B. Perforator-Based Intercostal Artery Muscle Flap: A Novel Approach for the Treatment of Tracheoesophageal or Bronchoesophageal Fistulas. Plast. Reconstr. Surg. 2021, 147, 795e–800e. [Google Scholar] [CrossRef]
- Fricke, A.; Bannasch, H.; Klein, H.F.; Wiesemann, S.; Samson-Himmelstjerna, P.; Passlick, B.; Beyersdorf, F.; Hoeppner, J.; Penna, V.; Eisenhardt, S.U.; et al. Pedicled and free flaps for intrathoracic fistula management. Eur. J. Cardio Thorac. Surg. 2017, 52, 1211–1217. [Google Scholar] [CrossRef]
- Palmes, D.; Kebschull, L.; Bahde, R.; Senninger, N.; Pascher, A.; Laukötter, M.G.; Eichelmann, A.-K. Management of Nonmalignant Tracheo- and Bronchoesophageal Fistula after Esophagectomy. Thorac. Cardiovasc. Surg. 2021, 69, 216–222. [Google Scholar] [CrossRef]
- Maruyama, K.; Motoyama, S.; Sato, Y.; Hayashi, K.; Usami, S.; Minamiya, Y.; Ogawa, J. Tracheobronchial Lesions Following Esophagectomy: Erosions, Ulcers, and Fistulae, and the Predictive Value of Lymph Node-Related Factors. World J. Surg. 2009, 33, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Sugimura, K.; Yamasaki, M.; Miyata, M.; Motoori, M.; Shizaki, H.; Mori, M.; Doki, Y. Ten cases of gastro-tracheobronchial fistula: A serious complication after esophagectomy and reconstruction using posterior mediastinal gastric tube. Dis. Esophagus 2012, 25, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.E.; Stein, H.J.; Siewert, J.R. Tracheobronchial lesions following oesophagectomy: Prevalence, predisposing factors and outcome. Br. J. Surg. 1998, 85, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Tachimori, Y.; Kanamori, N.; Uemura, N.; Hokamura, N.; Igaki, H.; Kato, H. Salvage esophagectomy after high-dose chemoradiotherapy for esophageal squamous cell carcinoma. J. Thorac. Cardiovasc. Surg. 2009, 137, 49–54. [Google Scholar] [CrossRef]
- Wang, S.; Tachimori, Y.; Hokamura, N.; Igaki, H.; Kishino, T.; Nakazato, H. A Retrospective Study on Nonmalignant Airway Erosion After Right Transthoracic Subtotal Esophagectomy: Incidence, Diagnosis, Therapy, and Risk Factors. Ann. Thorac. Surg. 2014, 97, 467–473. [Google Scholar] [CrossRef]
- Udelsman, B.V.; Eaton, J.; Muniappan, A.; Morse, C.R.; Wright, C.D.; Mathisen, D.J. Repair of large airway defects with bioprosthetic materials. J. Thorac. Cardiovasc. Surg. 2016, 152, 1388–1397. [Google Scholar] [CrossRef]
- Wang, H.; Tao, M.; Zhang, N.; Zou, H.; Li, D.; Ma, H.; Dogmei, L.; Hongming, M.; Zhou, Y. Single application of airway stents in thoracogastric-airway fistula: Results and prognostic factors for its healing. Ther. Adv. Respir. Dis. 2019, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]



| Fistula Type | Decortications | Abscess | Empyema | Mediastinitis | |
|---|---|---|---|---|---|
| L | P | ||||
| Type II | 1 | 0 | 1 | 4 | 1 |
| Type III | 7 | 3 | 7 | 7 | |
| Fistula Type | Respiratory Insufficiency | Sepsis Shock | Circulatory Insufficiency | Renal Insufficiency | Multiorgan Dysfunction | Death |
|---|---|---|---|---|---|---|
| Type II | 1 | 1 | 3 | 0 | ||
| Type III | 3 | 3 | 5 | 2 | 1 | 1 |
| Type of Tested Material | Type of Microorganism | Number of Isolates |
|---|---|---|
| Bronchoalveolar lavage (BAL) | Physiological flora | 7 (31.8%) |
| Candida albicans | 4 (18.2%) | |
| Streptococcus pneumoniae | 8 (36.4%) | |
| Escherichia coli | 5 (22.7%) | |
| Pseudomonas aeruginosa | 5 (22.7) | |
| Proteus vulgaris | 2 (9.1%) | |
| Pleural cavity fluid | Physiological flora | 2 (9.1%) |
| Candida albicans | 7 (31.8%) | |
| Candida glabrata | 5 (22.7%) | |
| Streptococcus pneumoniae | 7 (31.8%) | |
| Escherichia coli | 7 (31.8%) | |
| Pseudomonas aeruginosa | 8 (36.4%) | |
| Proteus vulgaris | 5 (22.7%) | |
| Klebsiella pneumoniae | 6 (27.3%) | |
| Klebsiella pneumoniae (ESBL) | 2 (9.1%) | |
| Staphylococcus aureus | 5 (22.7%) | |
| Moraxella catharalis | 2 (9.1%) | |
| Enterococcus faecium | 2 (9.1%) | |
| Corynebacterium sp. | 4 (18.2%) | |
| Enterococcus faecalis (VRE) | 2 (9.1%) |
| Grade | Number (%) | Definition |
|---|---|---|
| I | 17 (72.3%) | Urinary tract infection—7 (31.8%); wound infection—3 (13.6%); temporary mental disorders (postoperative delirium)—5 (22.7%) Any deviation from the normal postoperative course without the need for pharmacological treatment or surgical, endoscopic, and radiological interventions. Allowed therapeutic regimens are drugs such as antiemetics, antipyretics, analgetics, diuretics, and electrolytes and physiotherapy. This grade also includes wound infections opened at the bedside. |
| II | 6 (27.2%) | Pneumonia—4 (18.1%), Nervus laryngeus paresis—2 (9.0%) Requiring pharmacological treatment with drugs other than those allowed for grade I complications. Blood transfusions and total parenteral nutrition are also included. |
| III | 14 (63.6%) | Patients requiring bronchoscopy—8 (36.4%), tracheostomy—6 (27.2%) Requiring surgical, endoscopic, or radiological intervention. |
| IIIa | Intervention not under general anesthesia. | |
| IIIb | Intervention under general anesthesia. | |
| IV | 8 (36.3%) | Respiratory insufficiency—4 (18.1%), Septic shock—4 (18.1%) Respiratory insufficiency. Life-threatening complication (including CNS complications); * requiring IC/ICU-management |
| IVa | 6 (27.2%) | Single organ dysfunction (including dialysis) Renal insufficiency—2 (9.0%), Circulatory insufficiency—4 (18.1%) |
| IVb | 1 (4.5%) | Sepsis—1 (4.5%) Multiorgan dysfunction. |
| V | 1 (4.5%) | 1 (4.5%) Death of a patient. |
| Reference Author | Year | No. of Patients after Esophagectomy | EAF after Other Esophageal, Mediastinal, or Other Disease | EAF after Airway Tract Resection | Primary Closure | Diversion of the Esophagus | Type of Flap Used for Reconstruction or Stenting | EAF Postoperative Mortality | Restoring the Continuity of Digestive Tract | EAF Recurrence | No. of Patients Who Survived (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Balakrishnan et al. [9] | 2018 | 11 | none | none | 3 (27.3%) and 1 pr | 7 (63.6%) | PMF | 3 (27%) | 2 (18.2%) | 2 (18.2%) | 3 (27.3%) |
| Rosskopfova et al. [10] | 2017 | 22 | 5 | 2 | 5 (22.7%) | 9 (40.9%) | LDF, MSAF, PMF | 4 (18%) | 5 (22.7%) | 2 (4.5%) | 18 (81.8%) |
| Shweigert et al. [11] | 2012 | 7 | none | none | 1 (14.3%) (ct) | 2 (28.6%) | Stent, MSA, | 2/2 (28.6%) | none | 2 (28.6%) | 2 (28.6%) |
| Lambertz et al. [3] | 2016 | 13 | none | none | 3 (27.3%) after stenting, | 2 (63.6%) | Stenting, PPF, SCMM, | 5 (38.5%) | unknown | 2 (18.2%) | 7 (63.6%) |
| Wang et al. [12] | 2020 | 26 | none | none | 4 (15%) (ct) | none | PSFF, IMF, stent, | 11 (42.3%) | none | 1 (3.8%) | 15 (57.7%) |
| Bertheuil et al. [13] | 2021 | 8 | none | none | none | 0 | pIMF | 0 | 8 (10) | 2 (25%) | 8 (100%) |
| Fricke et al. [14] | 2017 | 13 | 2 | 4 | 0 | 1 (7.7%) | IMF, PMF, LDF, RAMF, FTPFF | 0 | 13(100%) | 5 (38.5%), after re-op 1 | 13 (100%) |
| Palmes et al. [15] | 2021 | 15 | none | none | 3 (ct) | 4 (26.7%) | Stent, ps | 7 (47%) | unknown | 1 (6.7%) | 7 (46.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Włodarczyk, J.; Smęder, T.; Obarski, P.; Ziętkiewicz, M. Treatment of Esophago–Airway Fistula after Esophageal Resection. Healthcare 2023, 11, 3165. https://doi.org/10.3390/healthcare11243165
Włodarczyk J, Smęder T, Obarski P, Ziętkiewicz M. Treatment of Esophago–Airway Fistula after Esophageal Resection. Healthcare. 2023; 11(24):3165. https://doi.org/10.3390/healthcare11243165
Chicago/Turabian StyleWłodarczyk, Janusz, Tomasz Smęder, Piotr Obarski, and Mirosław Ziętkiewicz. 2023. "Treatment of Esophago–Airway Fistula after Esophageal Resection" Healthcare 11, no. 24: 3165. https://doi.org/10.3390/healthcare11243165
APA StyleWłodarczyk, J., Smęder, T., Obarski, P., & Ziętkiewicz, M. (2023). Treatment of Esophago–Airway Fistula after Esophageal Resection. Healthcare, 11(24), 3165. https://doi.org/10.3390/healthcare11243165