
Gender, Mental Health and Socioeconomic Differences in Fibromyalgia: A Retrospective Cohort Study Using Real-World Data from Catalonia
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
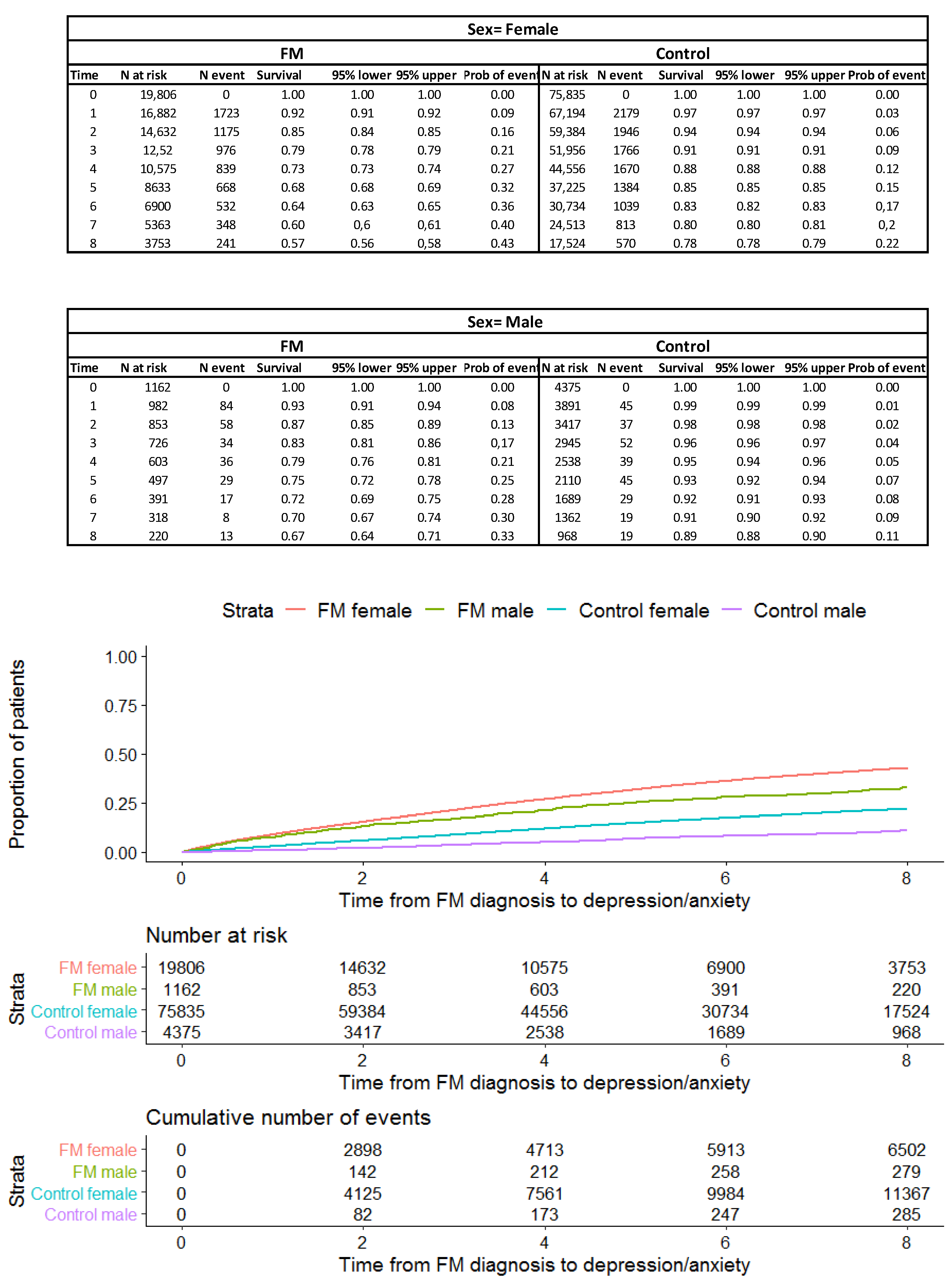
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walittt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef]
- Costa, I.D.S.; Gamundí, A.; Miranda, J.G.V.; França, L.G.S.; De Santana, C.N.; Montoya, P. Altered Functional Performance in Patients with Fibromyalgia. Front. Hum. Neurosci. 2017, 11, 14. [Google Scholar] [CrossRef]
- Kueny, A.; Montesó-Curto, P.; Lunn, S.; Mohabbat, A.B.; Clark, S.; Luedtke, C.; Vincent, A.; Ruschak, I.; Mateu-Gil, M.L.; Panisello-Chavarria, M.L.; et al. Fibromyalgia Pain and Fatigue Symptoms in Spanish and U.S. Men. Pain Manag. Nurs. 2021, 22, 423–428. [Google Scholar] [CrossRef]
- Prados, G.; Miró, E.; Martínez, M.P.; Sánchez, A.I.; López, S.; Sáez, G. Fibromyalgia: Gender differences and sleep-disordered breathing. Clin. Exp. Rheumatol. 2013, 31 (Suppl. S79), S102–S110. [Google Scholar]
- Segura-Jiménez, V.; Estévez-López, F.; Soriano-Maldonado, A.; Álvarez-Gallardo, I.C.; Delgado-Fernández, M.; Ruiz, J.R.; Aparicio, V.A. Gender Differences in Symptoms, Health-Related Quality of Life, Sleep Quality, Mental Health, Cognitive Performance, Pain-Cognition, and Positive Health in Spanish Fibromyalgia Individuals: The Al-Ándalus Project. Pain Res. Manag. 2016, 2016, 5135176. [Google Scholar] [CrossRef]
- Gormsen, L.; Rosenberg, R.; Bach, F.W.; Jensen, T.S. Depression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic pain. Eur. J. Pain 2010, 14, e1–e8. [Google Scholar] [CrossRef]
- Kadimpati, S.; Zale, E.L.; Hooten, M.W.; Ditre, J.W.; Warner, D.O. Associations between Neuroticism and Depression in Relation to Catastrophizing and Pain-Related Anxiety in Chronic Pain Patients. PLoS ONE 2015, 10, e0126351. [Google Scholar]
- Galvez-Sánchez, C.M.; Montoro, C.I.; Duschek, S.; Reyes del Paso, G.A. Depression and trait-anxiety mediate the influence of clinical pain on health-related quality of life in fibromyalgia. J. Affect. Disord. 2020, 265, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.T.; Edwards, R.R.; Robinson, R.C.; Dworkin, R.H. Suicidal ideation, plans, and attempts in chronic pain patients: Factors associated with increased risk. Pain 2004, 111, 201–208. [Google Scholar] [CrossRef]
- Aguglia, A.; Salvi, V.; Maina, G.; Rossetto, I.; Aguglia, E. Fibromyalgia syndrome and depressive symptoms: Comorbidity and clinical correlates. J. Affect. Disord. 2011, 128, 262–266. [Google Scholar] [CrossRef]
- García-Gil, M.D.M.; Hermosilla, E.; Prieto-Alhambra, D.; Fina, F.; Rosell, M.; Ramos, R.; Rodriguez, J.; Williams, T.; van Staa, T.; Bolibar, B. Construction and validation of a scoring system for the selection of high-quality data in a Spanish population primary care database (SIDIAP). Inform. Prim. Care 2011, 19, 135–145. [Google Scholar] [CrossRef]
- Bolíbar, B.; Fina Avilés, F.; Morros, R.; Garcia-Gil, M.M.; Hermosilla, E.; Ramos, R.; Rosell, M.; Rodríguez, J.; Medina, M.; Calero, S.; et al. SIDIAP database: Electronic clinical records in primary care as a source of information for epidemiologic research. Med. Clin. 2012, 138, 617–621. [Google Scholar] [CrossRef]
- Recalde, M.; Rodríguez, C.; Burn, E.; Far, M.; García, D.; Carrere-Molina, J.; Benítez, M.; Moleras, A.; Pistillo, A.; Bolíbar, B.; et al. Data Resource Profile: The Information System for Research in Primary Care (SIDIAP). Int. J. Epidemiol. 2022, 51, e324–e336. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Berjón, M.F.; Borrell, C.; Cano-Serral, G.; Esnaola, S.; Nolasco, A.; Pasarín, M.I.; Ramis, R.; Saurina, C.; Escolar-Pujo, A. Construcción de un índice de privación a partir de datos censales en grandes ciudades españolas:(Proyecto MEDEA). Gac. Sanit. 2008, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Montero, P.J.; Segura-Jimenez, V.; Alvarez-Gallardo, I.C.; Nijs, J.; Mannerkorpi, K.; Delgado-Fernandez, M.; van Wilgen, C.P. Fibromyalgia Impact Score in Women with Fibromyalgia Across Southern, Central, and Northern Areas of Europe. Pain Physician 2019, 22, E511–E516. [Google Scholar]
- Cagnie, B.; Coppieters, I.; Denecker, S.; Six, J.; Danneels, L.; Meeus, M. Central sensitization in fibromyalgia? A systematic review on structural and functional brain MRI. Semin. Arthritis Rheum. 2014, 44, 68–75. [Google Scholar] [CrossRef]
- Thieme, K.; Turk, D.C.; Flor, H. Comorbid Depression and Anxiety in Fibromyalgia Syndrome: Relationship to Somatic and Psychosocial Variables. Psychosom. Med. 2004, 66, 837–844. [Google Scholar] [CrossRef]
- Di Tella, M.; Ghiggia, A.; Tesio, V.; Romeo, A.; Colonna, F.; Fusaro, E.; Torta, R.; Castelli, L. Pain experience in Fibromyalgia Syndrome: The role of alexithymia and psychological distress. J. Affect. Disord. 2017, 208, 87–93. [Google Scholar] [CrossRef]
- Kesebir, S.; Gündoğar, D.; Küçüksubaşı, Y.; Tatlıdil Yaylacı, E. The relation between affective temperament and resilience in depression: A controlled study. J. Affect. Disord. 2013, 148, 352–356. [Google Scholar] [CrossRef]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes Del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol Res Behav Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Neumeister, M.W.; Neumeister, E.L. Fibromyalgia. Clin. Plast Surg. 2020, 47, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Wan, B.; Gebauer, S.; Salas, J.; Jacobs, C.K.; Breeden, M.; Scherrer, J.F. Gender-Stratified Prevalence of Psychiatric and Pain Diagnoses in a Primary Care Patient Sample with Fibromyalgia. Pain Med. 2019, 20, 2129–2133. [Google Scholar] [CrossRef]
- Fietta, P.; Fietta, P.; Manganelli, P. Fibromyalgia and psychiatric disorders. Acta Biomed. 2007, 78, 88–95. [Google Scholar]
- Soriano-Maldonado, A.; Amris, K.; Ortega, F.B.; Segura-Jiménez, V.; Estévez-López, F.; Álvarez-Gallardo, I.C.; A Aparicio, V.; Delgado-Fernández, M.; Henriksen, M.; Ruiz, J.R. Association of different levels of depressive symptoms with symptomatology, overall disease severity, and quality of life in women with fibromyalgia. Qual. Life Res. 2015, 24, 2951–2957. [Google Scholar] [CrossRef] [PubMed]
- Yunus, M.B.; Inanici, F.; Aldag, J.C.; Mangold, R.F. Fibromyalgia in men: Comparison of clinical features with women. J. Rheumatol. 2000, 27, 485–490. [Google Scholar]
- Henao-Pérez, M.; López-Medina, D.C.; Arboleda, A.; Bedoya Monsalve, S.; Zea, J.A. Patients With Fibromyalgia, Depression, and/or Anxiety and Sex Differences. Am. J. Mens Health 2022, 16, 15579883221110351. [Google Scholar] [CrossRef]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef]
- Gota, C.E.; Kaouk, S.; Wilke, W.S. The impact of depressive and bipolar symptoms on socioeconomic status, core symptoms, function and severity of fibromyalgia. Int. J. Rheum. Dis. 2017, 20, 326–339. [Google Scholar] [CrossRef]
- Diaz-Piedra, C.; Di Stasi, L.L.; Baldwin, C.M.; Buela-Casal, G.; Catena, A. Sleep disturbances of adult women suffering from fibromyalgia: A systematic review of observational studies. Sleep Med. Rev. 2015, 21, 86–99. [Google Scholar] [CrossRef]
- Andrade, A.; Vilarino, G.T.; Sieczkowska, S.M.; Coimbra, D.R.; Bevilacqua, G.G.; Steffens R de, A.K. The relationship between sleep quality and fibromyalgia symptoms. J. Health Psychol. 2020, 25, 1176–1186. [Google Scholar] [CrossRef] [PubMed]
- Keskindag, B.; Karaaziz, M. The association between pain and sleep in fibromyalgia. Saudi Med. J. 2017, 38, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Sauch Valmaña, G.; Miró Catalina, Q.; Vidal-Alaball, J. Prevalence and Incidence of Patients With Fibromyalgia in Catalonia Between 2010 and 2017: A Descriptive Observational Study. J. Prim. Care Community Health 2022, 13, 215013192210941. [Google Scholar] [CrossRef]
- Gendelman, O.; Amital, H.; Bar-On, Y.; Ben-Ami Shor, D.; Amital, D.; Tiosano, S.; Shalev, V.; Chodick, G.; Weitzman, D. Time to diagnosis of fibromyalgia and factors associated with delayed diagnosis in primary care. Best Pract. Res. Clin. Rheumatol. 2018, 32, 489–499. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case—Incident | Case—Prevalent | p-Overall b | Case, n (%) | Control, n (%) | p-Overall b | |
|---|---|---|---|---|---|---|
| N = 13,327 | N = 7641 | N = 20,968 | N = 80,210 | |||
| Sex | 0.020 | 0.633 | ||||
| Female | 12,551 (94.2%) | 7255 (94.9%) | 19,806 (94.5%) | 75,835 (94.5%) | ||
| Male | 776 (5.82%) | 386 (5.05%) | 1162 (5.54%) | 4375 (5.45%) | ||
| Age a | 52.6 (12.1) | 53.6 (11.9) | <0.001 | 53.0 (12.1); | 52.6 (11.8); | <0.001 |
| 52 [45; 60] | 54 [46; 62] | 53.0 [45.0;61.0] | 53.0 [45.0;60.0] | |||
| MedeA * | 0.006 | <0.001 | ||||
| Missing | 9 (0.07%) | 11 (0.14%) | 20 (0.10%) | 121 (0.15%) | ||
| R | 2296 (17.2%) | 1304 (17.1%) | 3600 (17.2%) | 14,450 (18.0%) | ||
| U | 946 (7.10%) | 641 (8.39%) | 1587 (7.57%) | 6270 (7.82%) | ||
| U1 | 1734 (13.0%) | 1015 (13.3%) | 2749 (13.1%) | 11,515 (14.4%) | ||
| U2 | 1939 (14.5%) | 1136 (14.9%) | 3075 (14.7%) | 12,039 (15.0%) | ||
| U3 | 2201 (16.5%) | 1214 (15.9%) | 3415 (16.3%) | 12,374 (15.4%) | ||
| U4 | 2164 (16.2%) | 1240 (16.2%) | 3404 (16.2%) | 12,238 (15.3%) | ||
| U5 | 2038 (15.3%) | 1080 (14.1%) | 3118 (14.9%) | 11,203 (14.0%) | ||
| Patients at the end of follow-up | <0.001 | <0.001 | ||||
| Alive | 12,445 (93.4%) | 6767 (88.6%) | 19,212 (91.6%) | 70,691 (88.1%) | ||
| Dead | 178 (1.34%) | 202 (2.64%) | 380 (1.81%) | 1894 (2.36%) | ||
| Transferred | 704 (5.28%) | 672 (8.79%) | 1376 (6.56%) | 7625 (9.51%) | ||
| Alcohol risk: | <0.001 | <0.001 | ||||
| Without risk | 6918 (51.9%) | 1768 (23.1%) | 8686 (41.4%) | 23,686 (29.5%) | ||
| Low risk | 1981 (14.9%) | 367 (4.80%) | 2348 (11.2%) | 8250 (10.3%) | ||
| High risk | 66 (0.50%) | 24 (0.31%) | 90 (0.43%) | 345 (0.43%) | ||
| Unknown | 4362 (32.7%) | 5482 (71.7%) | 9844 (46.9%) | 47,929 (59.8%) | ||
| Tobacco consumption: | <0.001 | 0.000 | ||||
| Non-smoker | 7146 (53.6%) | 3614 (47.3%) | 10,760 (51.3%) | 35,159 (43.8%) | ||
| Smoker | 2729 (20.5%) | 1500 (19.6%) | 4229 (20.2%) | 12,033 (15.0%) | ||
| Ex-smoker | 1479 (11.1%) | 526 (6.88%) | 2005 (9.56%) | 5712 (7.12%) | ||
| Unknown | 1973 (14.8%) | 2001 (26.2%) | 3974 (19.0%) | 27,306 (34.0%) |
| Case—Incident | Case—Prevalent | p-Overall * | |
|---|---|---|---|
| N = 13,327 | N = 7641 | ||
| (n (%)) | (n (%)) | ||
| Anxiety and/or depression | 3750 (28.1%) | 3031 (39.7%) | <0.001 |
| Anxiety post data index | 2409 (18.1%) | 2014 (26.4%) | <0.001 |
| No. of diagnoses of anxiety a | 0.19 (0.43) | 0.29 (0.52) | <0.001 |
| Depression post data index | 2159 (16.2%) | 1826 (23.9%) | <0.001 |
| No. of diagnoses of depression a | 0.18 (0.42) | 0.27 (0.51) | <0.001 |
| Case | Control | p-Overall b | |
| N = 20968 | N = 80210 | ||
| (n (%)) | (n (%)) | ||
| 6781 (32.3%) | 11,652 (14.5%) | 0.000 | |
| 4423 (21.1%) | 8756 (10.9%) | 0.000 | |
| 0.23 (0.47) | 0.12 (0.34) | 0.000 | |
| 3985 (19.0%) | 4661 (5.81%) | 0.000 | |
| 0.21 (0.46) | 0.06 (0.26) | 0.000 | |
| Variables | HR * | CI 95% | p-Value |
|---|---|---|---|
| Group | |||
| Control | 0.42 | (0.40; 0.43) | <0.05 |
| Sex | |||
| Men | 0.55 | (0.50; 0.60) | <0.05 |
| Age | |||
| 25–34 | 0.90 | (0.76; 1.06) | 0.21 |
| 35–44 | 0.94 | (0.80; 1.10) | 0.42 |
| 45–54 | 0.93 | (0.79; 1.09) | 0.38 |
| 55–64 | 0.90 | (0.76; 1.05) | 0.19 |
| 65–74 | 0.90 | (0.76; 1.06) | 0.19 |
| ≥75 | 1.04 | (0.88; 1.24) | 0.63 |
| MedeA | |||
| U | 0.95 | (0.90; 1.02) | 0.16 |
| U1 | 0.89 | (0.84; 0.93) | <0.05 |
| U2 | 0.96 | (0.91; 1.01) | 0.13 |
| U3 | 0.96 | (0.92; 1.01) | 0.14 |
| U4 | 1.01 | (0.96; 1.06) | 0.81 |
| U5 | 1.02 | (0.97; 1.07) | 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauch Valmaña, G.; Miró Catalina, Q.; Carrasco-Querol, N.; Vidal-Alaball, J. Gender, Mental Health and Socioeconomic Differences in Fibromyalgia: A Retrospective Cohort Study Using Real-World Data from Catalonia. Healthcare 2023, 11, 530. https://doi.org/10.3390/healthcare11040530
Sauch Valmaña G, Miró Catalina Q, Carrasco-Querol N, Vidal-Alaball J. Gender, Mental Health and Socioeconomic Differences in Fibromyalgia: A Retrospective Cohort Study Using Real-World Data from Catalonia. Healthcare. 2023; 11(4):530. https://doi.org/10.3390/healthcare11040530
Chicago/Turabian StyleSauch Valmaña, Glòria, Queralt Miró Catalina, Noèlia Carrasco-Querol, and Josep Vidal-Alaball. 2023. "Gender, Mental Health and Socioeconomic Differences in Fibromyalgia: A Retrospective Cohort Study Using Real-World Data from Catalonia" Healthcare 11, no. 4: 530. https://doi.org/10.3390/healthcare11040530