
The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review

Abstract
:1. Background
2. Materials and Methods
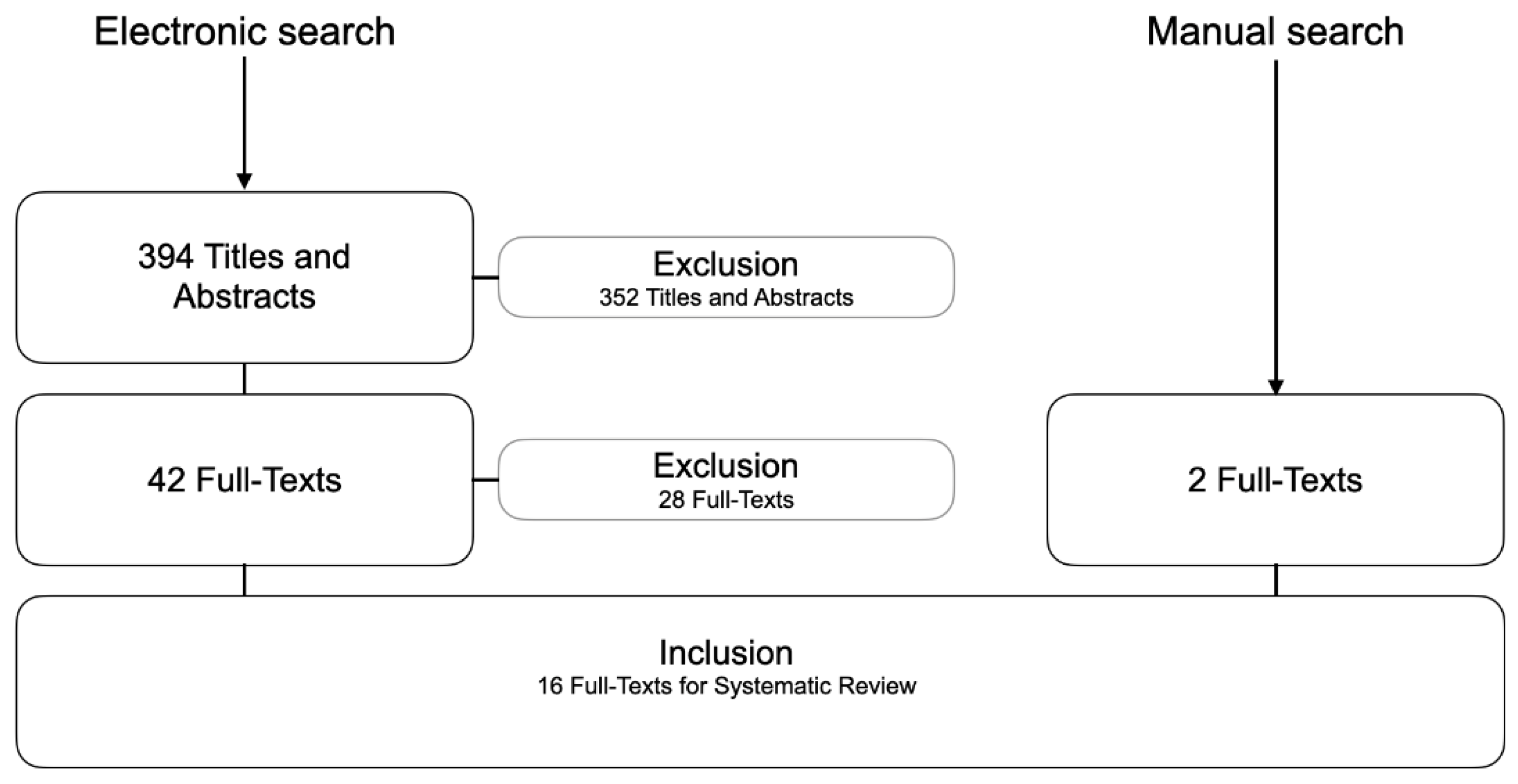
2.1. Search Strategy and Study Selection
2.2. Inclusion Criteria
- Clinical trials, limited to RCTs with at least 10 patients;
- Treatment concepts with FDPs, either tooth-borne or implant-supported for single- or multi-unit restorations;
- Processing of a complete digital workflow (without physical models); and
- Reporting of information on the used clinical work steps and technical production.
2.3. Selection of Studies
2.4. Data Extraction
3. Results
3.1. Included Studies
- No data on complete digital workflows (n = 5)
- Not an RCT (n = 17)
- Workflow did not investigate final prosthetic restorations (n = 6)
3.2. Descriptive Analysis
3.3. Group A1—Tooth-Borne Single-Unit Restorations (Table 3)
3.4. Group B1—Implant-Supported Single-Unit Restorations (Table 4)
3.5. Group B2—Implant-Supported Multi-Unit Restorations (Table 5)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alauddin, M.S.; Baharuddin, A.S.; Mohd Ghazali, M.I. The Modern and Digital Transformation of Oral Health Care: A Mini Review. Healthcare 2021, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Yeung, A.W.K.; Hung, K.; Zitzmann, N.U.; Bornstein, M.M. Disruptive Innovation in Dentistry: What It Is and What Could Be Next. J. Dent. Res. 2021, 100, 448–453. [Google Scholar] [CrossRef] [PubMed]
- van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Morsy, N.; El Kateb, M. Accuracy of intraoral scanners for static virtual articulation: A systematic review and meta-analysis of multiple outcomes. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implants Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef]
- Joda, T.; Zarone, F.; Ferrari, M. The complete digital workflow in fixed prosthodontics: A systematic review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Bernauer, S.A.; Zitzmann, N.U.; Joda, T. The Use and Performance of Artificial Intelligence in Prosthodontics: A Systematic Review. Sensors 2021, 21, 6628. [Google Scholar] [CrossRef]
- Ahmed, N.; Abbasi, M.S.; Zuberi, F.; Qamar, W.; Halim, M.S.B.; Maqsood, A.; Alam, M.K. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry-A Systematic Review. BioMed Res. Int. 2021, 2021, 9751564. [Google Scholar] [CrossRef]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, B.A.; Gallucci, G.O.; Att, W.; Özcan, M.; Krishnamurthy, V.R. Artificial intelligence models for tooth-supported fixed and removable prosthodontics: A systematic review. J. Prosthet. Dent. 2023, 129, 276–292. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.W.; Ye, S.Y.; Chien, C.H.; Chen, C.J.; Papaspyridakos, P.; Ko, C.C. Randomized clinical trial of a conventional and a digital workflow for the fabrication of interim crowns: An evaluation of treatment efficiency, fit, and the effect of clinician experience. J. Prosthet. Dent. 2021, 125, 73–81. [Google Scholar] [CrossRef]
- Haddadi, Y.; Bahrami, G.; Isidor, F. Accuracy of crowns based on digital intraoral scanning compared to conventional impression-a split-mouth randomised clinical study. Clin. Oral Investig. 2019, 23, 4043–4050. [Google Scholar] [CrossRef]
- Mühlemann, S.; Benic, G.I.; Fehmer, V.; Hämmerle, C.H.F.; Sailer, I. Clinical quality and efficiency of monolithic glass ceramic crowns in the posterior area: Digital compared with conventional workflows. Int. J. Comput. Dent. 2018, 21, 215–223. [Google Scholar]
- Park, J.S.; Lim, Y.J.; Kim, B.; Kim, M.J.; Kwon, H.B. Clinical Evaluation of Time Efficiency and Fit Accuracy of Lithium Disilicate Single Crowns between Conventional and Digital Impression. Materials 2020, 13, 5467. [Google Scholar] [CrossRef]
- Sailer, I.; Benic, G.I.; Fehmer, V.; Hämmerle, C.H.F.; Mühlemann, S. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part II: CAD-CAM versus conventional laboratory procedures. J. Prosthet. Dent. 2017, 118, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Sakornwimon, N.; Leevailoj, C. Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. J. Prosthet. Dent. 2017, 118, 386–391. [Google Scholar] [CrossRef]
- Zeltner, M.; Sailer, I.; Mühlemann, S.; Özcan, M.; Hämmerle, C.H.; Benic, G.I. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part III: Marginal and internal fit. J. Prosthet. Dent. 2017, 117, 354–362. [Google Scholar] [CrossRef] [Green Version]
- Capparé, P.; Ferrini, F.; Ruscica, C.; Pantaleo, G.; Tetè, G.; Gherlone, E.F. Digital versus Traditional Workflow for Immediate Loading in Single-Implant Restoration: A Randomized Clinical Trial. Biology 2021, 10, 1281. [Google Scholar] [CrossRef]
- Hanozin, B.; Li Manni, L.; Lecloux, G.; Bacevic, M.; Lambert, F. Digital vs. conventional workflow for one-abutment one-time immediate restoration in the esthetic zone: A randomized controlled trial. Int. J. Implant Dent. 2022, 8, 7. [Google Scholar] [CrossRef]
- Kunavisarut, C.; Jarangkul, W.; Pornprasertsuk-Damrongsri, S.; Joda, T. Patient-reported outcome measures (PROMs) comparing digital and conventional workflows for treatment with posterior single-unit implant restorations: A randomized controlled trial. J. Dent. 2022, 117, 103875. [Google Scholar] [CrossRef]
- Mangano, F.; Veronesi, G. Digital versus Analog Procedures for the Prosthetic Restoration of Single Implants: A Randomized Controlled Trial with 1 Year of Follow-Up. BioMed Res. Int. 2018, 2018, 5325032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlemann, S.; Lamperti, S.T.; Stucki, L.; Hämmerle, C.H.F.; Thoma, D.S. Time efficiency and efficacy of a centralized computer-aided-design/computer-aided-manufacturing workflow for implant crown fabrication: A prospective controlled clinical study. J. Dent. 2022, 127, 104332. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.; Guo, D.; Zhou, Y.; Jung, R.E.; Hämmerle, C.H.F.; Mühlemann, S. Time efficiency and quality of outcomes in a model-free digital workflow using digital impression immediately after implant placement: A double-blind self-controlled clinical trial. Clin. Oral Implants Res. 2019, 30, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Jiang, X.; Lin, Y.; Di, P. Crown Accuracy and Time Efficiency of Cement-Retained Implant-Supported Restorations in a Complete Digital Workflow: A Randomized Control Trial. J. Prosthodont. 2022, 31, 405–411. [Google Scholar] [CrossRef]
- Zhang, Y.; Tian, J.; Wei, D.; Di, P.; Lin, Y. Quantitative clinical adjustment analysis of posterior single implant crown in a chairside digital workflow: A randomized controlled trial. Clin. Oral Implants Res. 2019, 30, 1059–1066. [Google Scholar] [CrossRef]
- Gintaute, A.; Weber, K.; Zitzmann, N.U.; Brägger, U.; Ferrari, M.; Joda, T. A Double-Blind Crossover RCT Analyzing Technical and Clinical Performance of Monolithic ZrO2 Implant Fixed Dental Prostheses (iFDP) in Three Different Digital Workflows. J. Clin. Med. 2021, 10, 2661. [Google Scholar] [CrossRef]
- Gintaute, A.; Zitzmann, N.U.; Brägger, U.; Weber, K.; Joda, T. Patient-reported outcome measures compared to professional dental assessments of monolithic ZrO2 implant fixed dental prostheses in complete digital workflows: A double-blind crossover randomized controlled trial. J. Prosthodont. 2023, 32, 18–25. [Google Scholar] [CrossRef]
- Hashemi, A.M.; Hashemi, H.M.; Siadat, H.; Shamshiri, A.; Afrashtehfar, K.I.; Alikhasi, M. Fully Digital versus Conventional Workflows for Fabricating Posterior Three-Unit Implant-Supported Reconstructions: A Prospective Crossover Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 11456. [Google Scholar] [CrossRef]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N.U. Time-efficiency and cost-analysis comparing three digital workflows for treatment with monolithic zirconia implant fixed dental prostheses: A double-blinded RCT. J. Dent. 2021, 113, 103779. [Google Scholar] [CrossRef]
- Feine, J.; Abou-Ayash, S.; Al Mardini, M.; de Santana, R.B.; Bjelke-Holtermann, T.; Bornstein, M.M.; Braegger, U.; Cao, O.; Cordaro, L.; Eycken, D.; et al. Group 3 ITI Consensus Report: Patient-reported outcome measures associated with implant dentistry. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 270–275. [Google Scholar] [CrossRef]
- Kapos, T.; Evans, C. CAD/CAM technology for implant abutments, crowns, and superstructures. Int. J. Oral Maxillofac. Implants 2014, 29 (Suppl. 2014), 117–136. [Google Scholar] [CrossRef] [Green Version]
- van der Zande, M.M.; Gorter, R.C.; Bruers, J.J.M.; Aartman, I.H.A.; Wismeijer, D. Dentists’ opinions on using digital technologies in dental practice. Community Dent. Oral Epidemiol. 2018, 46, 143–153. [Google Scholar] [CrossRef]
- Joda, T.; Ferrari, M.; Gallucci, G.O.; Wittneben, J.G.; Brägger, U. Digital technology in fixed implant prosthodontics. Periodontol. 2000 2017, 73, 178–192. [Google Scholar] [CrossRef]
- Al-Thobity, A.M. Titanium Base Abutments in Implant Prosthodontics: A Literature Review. Eur. J. Dent. 2022, 16, 49–55. [Google Scholar] [CrossRef]
- Siqueira, R.; Galli, M.; Chen, Z.; Mendonca, G.; Meirelles, L.; Wang, H.L.; Chan, H.L. Intraoral scanning reduces procedure time and improves patient comfort in fixed prosthodontics and implant dentistry: A systematic review. Clin. Oral Investig. 2021, 25, 6517–6531. [Google Scholar] [CrossRef]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef]
- Baghani, M.T.; Shayegh, S.S.; Johnston, W.M.; Shidfar, S.; Hakimaneh, S.M.R. In vitro evaluation of the accuracy and precision of intraoral and extraoral complete-arch scans. J. Prosthet. Dent. 2021, 126, 665–670. [Google Scholar] [CrossRef]
- Gintaute, A.; Keeling, A.J.; Osnes, C.A.; Zitzmann, N.U.; Ferrari, M.; Joda, T. Precision of maxillo-mandibular registration with intraoral scanners in vitro. J. Prosthodont. Res. 2020, 64, 114–119. [Google Scholar] [CrossRef]
- Morton, D.; Gallucci, G.; Lin, W.S.; Pjetursson, B.; Polido, W.; Roehling, S.; Sailer, I.; Aghaloo, T.; Albera, H.; Bohner, L.; et al. Group 2 ITI Consensus Report: Prosthodontics and implant dentistry. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 215–223. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Kohal, R.J.; Spies, B.C.; Pjetursson, B.E.; Lang, N.P.; Gotfredsen, K.L.; Ellingsen, J.E.; Francisco, H.; Özcan, M.; et al. Reconstructive aspects: Summary and consensus statements of group 3. The 5th EAO Consensus Conference 2018. Clin. Oral Implants Res. 2018, 29 (Suppl. 18), 237–242. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Focused question (PICO) | Is a complete digital workflow with intraoral optical scanning (IOS) plus virtual design plus monolithic restoration for patients receiving prosthodontic treatments with (A) tooth-borne or (B) implant-supported fixed restorations comparable to conventional or mixed analog-digital workflows with conventional impression and/or lost-wax-technique and/or framework and veneering in terms of feasibility in general or survival/success-analysis including complication assessment with a minimum follow-up of one year or economics or esthetics or patient-centered factors? | |
| Timeline | From 16 September 2016 until 31 October 2022 | |
| Search Strategy | Problem | {(“Dental Prosthesis” [6]) OR (“Crowns” [6]) OR (“Dental Prosthesis, Implant-Supported” [6] OR (“Crowns, Implant-Supported” [6]) OR (crown) OR (fixed dental prosthesis) OR (fixed reconstruction) OR (fixed restoration) OR (dental bridge) OR (implant crown) OR (implant prosthesis) OR (implant restoration) OR (implant reconstruction)} |
| Intervention | {(“Computer-Aided Design” [6]) OR (digital workflow) OR (digital technology) OR (computerized dentistry) OR (intraoral scan) OR (digital impression) OR (scanbody) OR (virtual design) OR (digital design) OR (cad/cam) OR (rapid prototyping) OR (monolithic) OR (full-contour)} | |
| Control | {(“Dental Technology” [6]) OR (conventional workflow) OR (lost-wax-technique) OR (porcelain-fused-to-metal) OR (PFM) OR (implant impression) OR (hand-layering) OR (veneering) OR (framework)} | |
| Outcome | {(“Study, Feasibility” [6]) OR (“Survival” [MeSH]) OR (“Success” [MeSH]) OR (“Economics” [MeSH]) OR (“Costs, Cost Analysis” [MeSH]) OR (“Esthetics, Dental” [MeSH]) OR (“Patient Satisfaction” [MeSH]) OR (feasibility) OR (efficiency) OR (esthetics) OR (patient-centered outcome)} | |
| No. | Study (Year) | Author | Study Design | Type of Restoration | Number of Subjects | Outcome |
|---|---|---|---|---|---|---|
| 1. | 2016 2016 | Seiler et al. [15] Zeltner et al. [17] | RCT
| A1. Tooth-borne crowns
| 10 patients 50 crowns | |
| 2. | 2018 | Mangano et al. [21] | RCT
| B1. Implant-supported crowns
| 50 patients 50 crowns |
|
| 3. | 2018 | Mühlemann et al. [13] | RCT
| A1. Tooth-borne crowns
| 10 patients 50 crowns |
|
| 4. | 2018 | Sakornwimon et al. [16] | RCT
| A1: Tooth-borne crowns
| 16 patients 32 crowns |
|
| 5. | 2019 | Haddadi et al. [12] | RCT
| A1. Tooth-borne crowns
| 19 patients 38 crowns |
|
| 6. | 2019 | Pan et al. [23] | RCT
| B1. Implant-supported crowns
| 40 patients 80 crowns |
|
| 7. | 2019 | Zhang et al. [25] | RCT
| B1. Implant-supported crowns
| 33 patients 33 crowns |
|
| 8. | 2020 | Park et al. [14] | RCT
| A1. Tooth-borne crowns
| 13 patients 26 crowns |
|
| 9. | 2021 | Cappare et al. [18] | RCT
| B1. Implant-supported crowns
| 50 patients 50 crowns |
|
| 10. | 2021 | Cheng et al. [11] | RCT
| A1. Tooth-borne crowns
| 40 patients 40 (interim) crowns |
|
| 11. | 2021 2021 2022 | Joda et al. [29] Gintaute et al. [26] Gintaute et al. [27] | RCT
| B2. Implant-supported three-unit restorations.
| 20 patients 60 three-unit FDPs | |
| 12. | 2021 | Kunavisarut et al. [20] | RCT
| B1. Implant-supported crowns
| 40 patients 40 crowns |
|
| 13. | 2021 | Ren et al. [24] | RCT
| B1. Implant-supported crowns
| 40 patients 40 crowns |
|
| 14. | 2022 | Hanozin et al. [19] | RCT
| B1. Implant-supported crowns
| 18 patients 18 crowns |
|
| 15. | 2022 | Hashemi et al. [28] | RCT
| B2. Implant-supported three-unit restorations
| 10 patients 20 three-unit FDPs |
|
| 16. | 2022 | Mühlemann et al. [22] | RCT
| B1. Implant-supported crowns
| 31 patients 31 crowns |
|
| No. | Study | Number of Subjects | Number of Prosthetic Units | Number of Abutment Teeth | Workflow and Materials | Results |
|---|---|---|---|---|---|---|
| 1. | 2017, Haddadi et al. [12] | n = 19 | n = 38 [19 + 19] | n = 38 | Digital: Tooth-borne premolar or molar crowns; digital impressions (Trios 3, 3shape); design (Dental System design software, 3Shape, Denmark); milling of LS2 crowns (Röders RXD5, Röders GmbH, Soltau, Germany); evaluation. Conventional: Tooth-borne premolar or molar crowns; conventional impressions (Extrude, Kerr, Orange, USA); fabrication of stone casts; labside scanning (D640, 3Shape, Denmark); design (Dental System design software, 3Shape, Denmark); milling of LS2 crowns (Röders RXD5, Röders GmbH, Soltau, Germany); evaluation. | Precision:
|
| 2. | 2017, Sailer et al. [15] 2018, Zeltner et al. [17] | n = 10 | n = 50 [10 + 10 + 10 + 10 + 10] | n = 10 | Digital: Group CiL: Tooth-borne premolar or molar crowns; digital impressions (Cerec Bluecam, Dentsply Sirona); CAD software (Cerec Connect software and Cerec inLab 3D, Dentsply Sirona); Labside milling of LS2 crowns (Cerec inLab MC XL milling unit, Dentsply Sirona); evaluation. Digital with physical cast: Tooth-borne premolar or molar crowns.
Conventional: Group K: Tooth-borne premolar or molar crowns; conventionally acquired impressions; fabrication of dental stone cast (Quadro-rock Plus; Picodent); waxing; investing; heat pressing the lithium disilicate glass ceramic blank (IPS e.max Press; Ivoclar Vivadent AG); devesting. | Precision:
|
| 3. | 2017, Sakorniwomo et al. [16] | n = 16 | n = 32 (16 + 16) | n = 16 | Digital: Tooth-borne molar crowns; digital impressions; design (3shape); milling of monolithic ZrO2 crowns (Lava Plus High Translucency Zirconia, 3M ESPE; hiCut CNC, Hint-Els); clinical evaluation. Conventional: Tooth-borne molar crowns; conventional impressions (Express xT Putty Soft and Express XT Light Body, 3M ESPE); fabrication of stone casts; labside scanning (D900L Scanner, 3Shape); design (3Shape); milling of monolithic ZrO2 crowns (Lava Plus High Translucency Zirconia, 3M ESPE; hiCut CNC, Hint-Els); clinical evaluation. | Precision:
|
| 4. | 2018, Mühlemann et al. [13] | n = 10 | n = 50 [10 + 10 + 10 + 10 + 10] | n = 10 | Digital: Tooth-borne crowns; complete digital workflow with four different methods:
Conventional: Tooth-borne crowns; conventional impressions (President, Coltene); stone casts; production of ceramic crown using lost-wax technique. | Precision:
|
| 5. | 2020, Park et al. [14] | n = 13 | n = 26 [13 + 13] | n = 13 | Digital: Tooth-borne crowns; complete digital workflow (AEGIS.PO, Digital Dentistry Solution, CEREC Omnicam, Sirona); design (DESIGN + Suite, Digital Dentistry Solution) and milling (SPEED +, Digital Dentistry Solution) of LS2 crowns (IPS e.max CAD; Ivoclar Vivadent). Conventional: Tooth-borne crowns; conventional impressions; fabrication and scan of master casts (Identica Hybrid, Medit); design (DESIGN + Suite, Digital Dentistry Solution) and milling (SPEED +, Digital Dentistry Solution) of LS2 crowns (IPS e.max CAD; Ivoclar Vivadent). | Precision:
|
| 6. | 2021, Cheng et al. [11] | n = 40 | n = 40 [20 + 20] | n = 40 | Digital: Tooth-borne interim crowns; impression taking (CS 3500, Carestream Dental); CAD (Exocad, Exocad GmbH); milling out of PMMA (PMMA Disk, Ymahachi Dental); clinical evaluation. Conventional: Tooth-borne interim crowns; conventional impression (Cavex CA37, Cavex); diagnostic wax-up and fabrication of vacuum formed translucent-matrices; direct interim crowns on the abutment tooth using PMMA (ALIKE, GC) and the vacuum-formed matrix; clinical evaluation. | Precision:
|
| No. | Study | Number of Subjects | Number of Prosthetic Units | Number of Implant Abutments | Workflow and Materials | Results |
|---|---|---|---|---|---|---|
| 1. | 2018, Mangano et al. [21] | n = 50 | n = 50 [25 + 25] | n = 50 | Digital: Impression-taking (CS3600, Carestream Dental, Rochester, NY, USA); design of individualized ZrO2 abutments and temporary PMMA crowns (Exocad Dental CAD); replacement of interim crowns after 2 months with monolithic ZrO2 crowns (Katana, Kuraray Noritake). Conventional: Impression-taking (Elite HDPlus, Zhermack); plaster models; dental technician prepared the Ti-abutment, temporary crowns and wax-up for the metal structures; replacement of interims after 2 months following second impressions with polyvinyl siloxane over metal copings; veneering of the metal structures; application of the final metal-ceramic crowns. | Cost efficiency:
|
| 2. | 2019, Pan et al. [23] | n = 40 | n = 80 [40 + 40] | n = 80 | Digital: Impression-taking immediately after implant placement (Trios, 3Shape); fabrication of screw-retained monolithic ZrO2 (Zenotec select hybrid, Wieland Dental); milling and sintering (Zenotec select hybrid, Wieland Dental). Conventional: Conventional impressions 3 months after implant placement (Impregum Penta, 3M ESPE); fabrication and digitization of stone models with lab-scanner (D3000, 3Shape), milling and sintering of screw-retained monolithic ZrO2 crowns (Zenotec select hybrid, Wieland Dental); adjustments by dental technician. | Precision:
|
| 3. | 2019, Zhang et al. [25] | n = 33 | n = 33 [17 + 16] | n = 33 | Digital: Digital impressions; design of the crown (CEREC Omnicam, Sirona, Dentsply); milling (CEREC MC XL Premium, Sirona, Dentsply) of monolithic LS2-crowns (IPS e.max CAD, Ivoclar Vivadent). Conventional: Silicone impressions (Silagum, DMG); fabrication and scan of stone models; milling and sintering of ZrO2 frameworks and ceramic veneering. | Precision:
|
| 4. | 2021, Cappare et al. [18] | n = 50 | n = 50 [25 + 25] | n = 50 | Digital: Implant and temporary abutment insertion; impression recorded using CAD/CAM system (Cerec Omnicam, Dentsply Sirona); fabrication of temporary prosthesis in PMMA (Sirona Cerec MCXL milling machine, Dentsply Sirona); four months after final digital impressions were recorded (Cerec Omnicam, Dentsply Sirona); insertion of final prosthesis in zirconia ceramic. Conventional: Implant and temporary abutment insertion; pre-fabricated acrylic resin crowns were obtained and adapted with an auto-polymerizing acrylic resin (Duralay, Reliance Dental Manufacturing LLC) along the margins of the temporary abutment; after 4 months, final impressions were taken using polyether (Impregum Penta, 3M ESPE); insertion of final ZrO2 crowns. | Esthetics:
|
| 5. | 2021, Kunavisarut et al. [20] | n = 40 | n = 40 [10 + 10 + 10 + 10] | n = 40 | Digital: Digital impressions (Trios, 3Shape); division into subgroups according to the restorative material: LS2 (N!CE, Straumann) or PICN (Enamic, Vita); chairside design and production (CARES Visual Chairside; C-Series CAD/CAM Milling, Straumann); bonding to Ti-base (Variobase, Straumann); clinical try-in and adjustments. Conventional: Conventional closed tray silicone impressions (Impregum, 3M Espe); digitalization of master casts lab-scanner (D900L, 3Shape); division into subgroups according to the restorative material: LS2 (N!CE, Straumann) or PICN (Enamic, Vita); chairside design and production (CARES Visual Chairside; C-Series CAD/CAM Milling, Straumann); bonding to Ti-bases (Variobase, Straumann); clinical try-in and adjustments. | Patient satisfaction:
|
| 6. | 2021, Ren et al. [24] | n = 40 | n = 40 [20 + 20] | n = 40 | Digital: Digital impression (Trios, 3Shape); Ti-abutment and ZrO2 crowns were designed and milled (Organical Multi 5X, Organical CAD/CAM GmbH); a dental technician polished and refined the milled abutments and crowns; IOS before and after clinical adjustment of the crowns (Trios, 3Shape); STL files were analyzed with Geomagic or crown adjustment evaluation. Conventional: Conventional silicone impressions; digitalization of master casts by lab-scanner [3Shape]; Ti-abutments were designed and milled (Organical Multi 5X, Organical CAD/CAM GmbH); a dental technician adjusted the abutments; new model scan, crowns were designed and milled (Organical Multi 5X, Organical CAD/CAM GmbH); refined by a dental technician; IOS before and after clinical adjustments of the crowns (Trios, 3Shape); STL files were analyzed with Geomatic or crown adjustment evaluation. | Precision:
|
| 7. | 2022, Hanozin et al. [19] | n = 18 | n = 18 [9 + 9] | n = 18 | Digital: Digital impression (Trios, 3Shape); Digital wax-up (CARES software) for implant planification (coDiagnostiX), digitally design of custom-made ZrO2 abutment (CARES X-Stream abutment, Straumann) and CAD/CAM PMMA crown; fully guided implantation; digital impression with scanbody (Trios, 3Shape); clinical check of the final ZrO2 abutment and provisional crown with immediate loading. Conventional: alginate impressions; digital implant planning (coDiagnostiX) based on a conventional wax-up; free-hand surgical implantation, conventional impressions with open tray, design of the final ZrO2 abutment and PMMA crown; insertion 10 days postoperative. | Esthetic:
|
| 8. | 2022, Mühlemann et al. [22] | n = 31 | n = 31 [12 + 19] | n = 31 | Digital: Digital impressions (Trios 3, 3Shape); scan data were uploaded to a centralized server (Virtual Atlantis Design, Dentsply Sirona); remote validation by dental technician and centralized CAM of the abutment (Atlantis, CustomBase solution, Dentsply Sirona) and ZrO2 crowns (Atlantis Crown, Full-contour, Dentsply Sirona); ZrO2 crowns in sintered stage, customized Ti-abutment and digital models were shipped; crowns were prepared for try-in by temporarily cementing on abutments; clinical evaluation; finalization by dental technician. Hybrid: Conventional impressions (Permadyne, 3M, ESEP GmbH); fabrication of stone models, digitalization with lab-scanner (Ceramill Map 400, Amann Girrbach); in house CAD (Ceramill, Amann Girrbach) of monolithic crowns on Ti-base abutments; crowns were prepared for try-in by temporarily cementing on abutments; clinical evaluation; finalization by dental technician. | Precision:
|
| No. | Study | Number of Subjects | Number of Prosthetic Units | Number of Implant Abutments | Workflow and Materials | Results |
|---|---|---|---|---|---|---|
| 1. | 2021, Joda et al. [29] 2021, Gintaute et al. [26] 2022, Gintaute et al. [27] | n = 20 | n = 60 [20 + 20 + 20] | n = 40 | Digital: Digital impressions; model-free fabrication of three-unit monolithic ZrO2 iFDPs using two different IOS systems; Test 1: (Trios 3, 3Shape), and Test 2 (Virtuo Vivo, Dental Wings) including company-related CAD/CAM lab software; milling of the three-unit monolithic ZrO2 iFDPs (Ceramill 2 Motion, Amann Girrbach), clinical assessment of restorations. Conventional: Classical impression-taking (Impregum, 3M ESPE), digitization of the gypsum casts with lab-scan (Ceramill Map 400+, Amann Girrbach), Exocad Lab-Software, milling of three-unit monolithic ZrO2 iFDPs (Ceramill 2 Motion, Amann Girrbach), clinical assessment of restorations. | Time efficiency:
|
| 2. | 2022, Hashemi et al. [28] | n = 10 | n = 20 [10 + 10] | n = 20 | Digital: Digital impressions (Trios 3, 3Shape); design (Dental system, 3Shape) and milling (Amann Girrbach) of screw-retained monolithic ZrO2 iFDPs (Katana translucent, Kuraray); clinical evaluation. Conventional: Conventional impressions (Panasil, Kettenbach GmbH & Co.), fabrication of stone models and lab-scan (Atos Core 5 Mp 80 mm; Rev. 02; GOM GmbH); metal casting abutments for full-contour waxing, cut-back and cast with cobalt-chromium alloy; veneering of the framework; clinical reevaluation. | Accuracy of IOS:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernauer, S.A.; Zitzmann, N.U.; Joda, T. The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review. Healthcare 2023, 11, 679. https://doi.org/10.3390/healthcare11050679
Bernauer SA, Zitzmann NU, Joda T. The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review. Healthcare. 2023; 11(5):679. https://doi.org/10.3390/healthcare11050679
Chicago/Turabian StyleBernauer, Selina A., Nicola U. Zitzmann, and Tim Joda. 2023. "The Complete Digital Workflow in Fixed Prosthodontics Updated: A Systematic Review" Healthcare 11, no. 5: 679. https://doi.org/10.3390/healthcare11050679