


Effectiveness of Drama-Based Intervention in Improving Mental Health and Well-Being: A Systematic Review and Meta-Analysis during the COVID-19 Pandemic and Post-Pandemic Period


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Study Selection
2.5. Data extraction
2.6. Data Analysis
3. Results
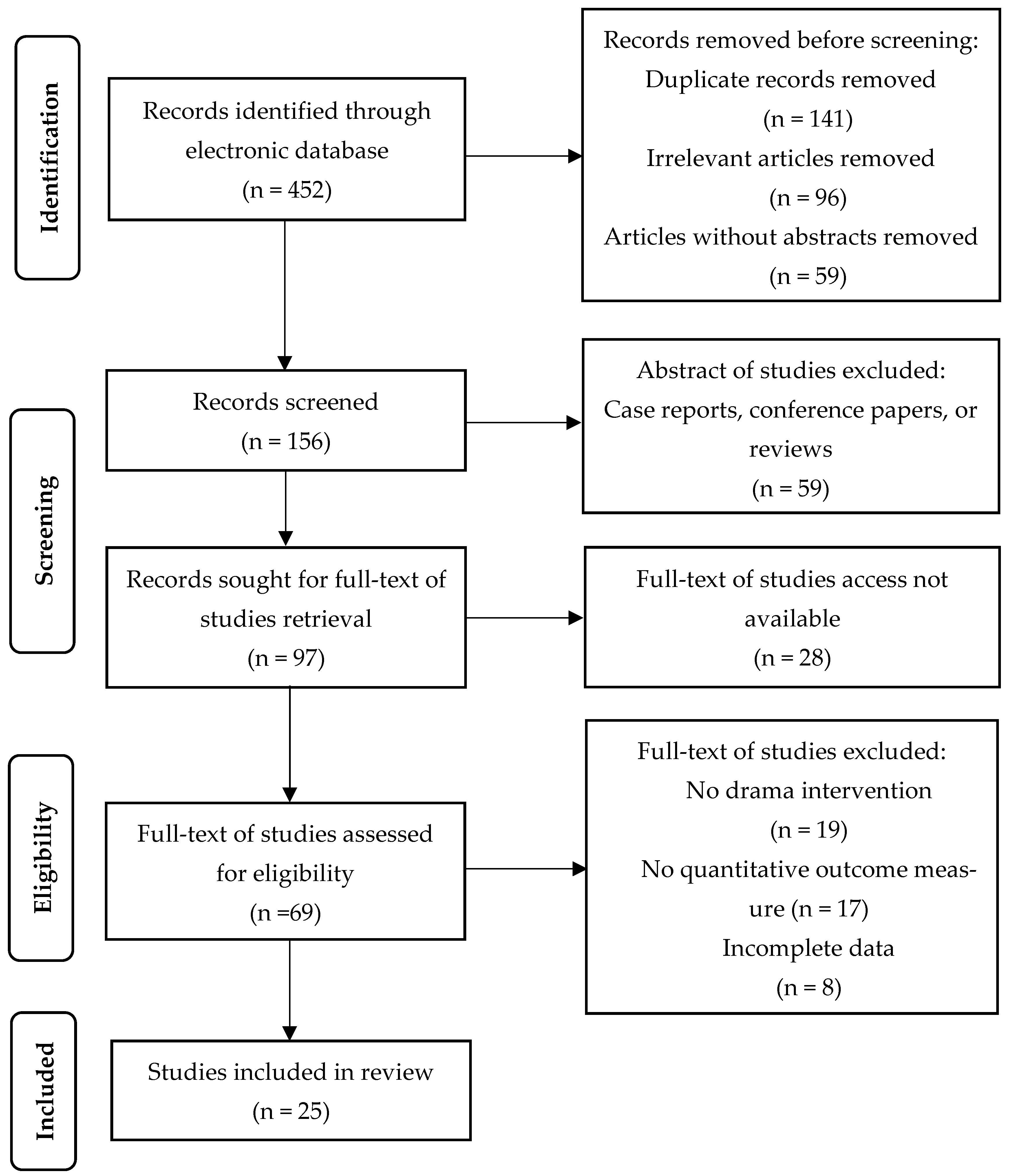
3.1. Study Identification and Selection
3.2. Characteristics of the Included Studies
3.2.1. Sample Characteristics
3.2.2. Intervention Characteristics
3.2.3. Outcome Measures
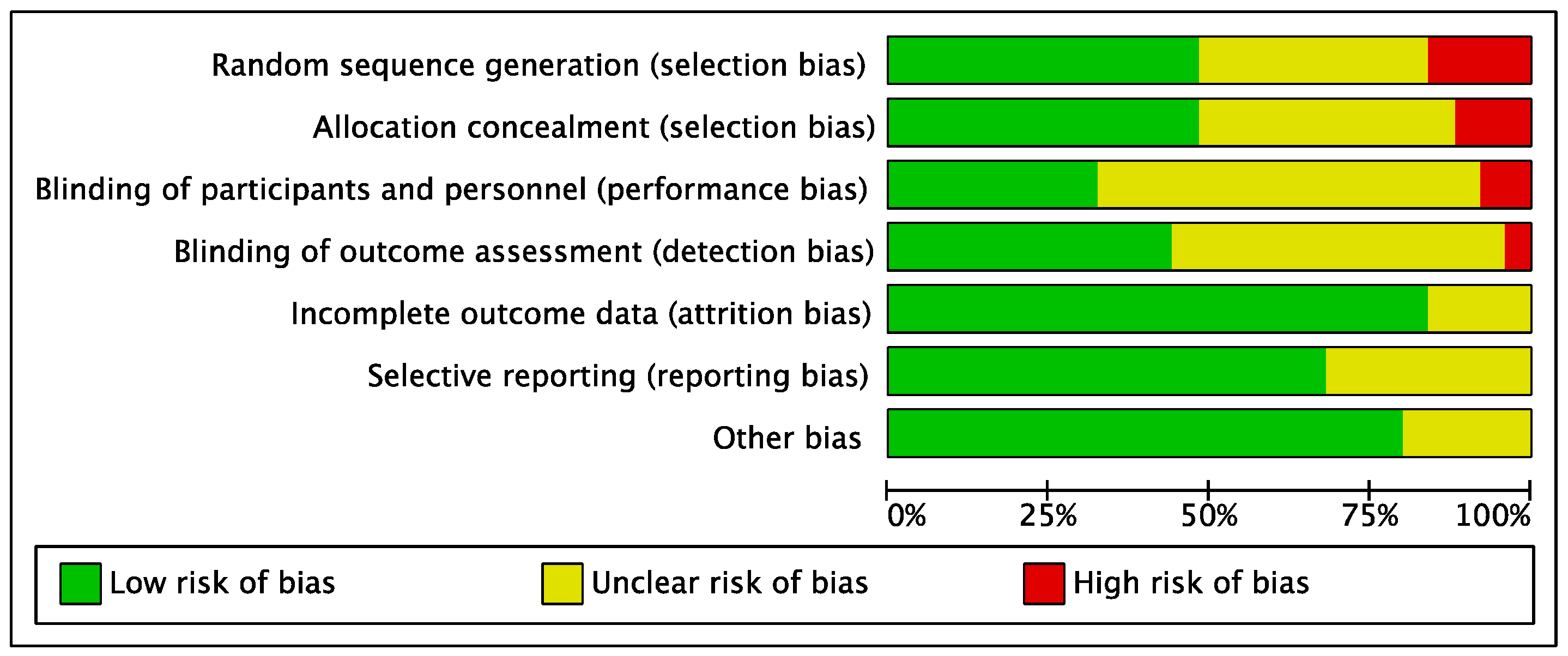
3.3. Risk of Bias Analysis
3.4. Meta-Analysis
3.4.1. Effect on Quality of Life
3.4.2. Effect on Psychological Well-Being
3.4.3. Effect on Depression
3.4.4. Effect on Anxiety
3.4.5. Effect on Trauma-Related Disorders
3.4.6. Effect on Communication Skills
3.4.7. Effect on Cognitive Functioning
3.4.8. Effect on Self-Regard
3.4.9. Overall Effect with Controlled Groups
3.4.10. Overall Effect with Pre/Posttest Groups
3.5. Evaluation of Publication Bias
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burjaq, R.; Hammoudeh, S. Perspective Chapter: The Psychosocial Effects of Isolation and Social Distancing during the Coronavirus Disease 2019 Pandemic: An Overview and Mitigation Strategies. In Psychosocial, Educational, and Economic Impacts of COVID-19; InTech: London, UK, 2022. [Google Scholar]
- Chaturvedi, S.K. COVID-19, Coronavirus and Mental Health Rehabilitation at Times of Crisis; Springer: Berlin/Heidelberg, Germany, 2020; Volume 7, pp. 1–2. [Google Scholar]
- Hossain, M.M.; Sultana, A.; Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: A systematic umbrella review of the global evidence. Epidemiol. Health 2020, 42, e2020038. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental health and the COVID-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Echegaray, F. What POST-COVID-19 lifestyles may look like? Identifying scenarios and their implications for sustainability. Sustain. Prod. Consum. 2021, 27, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and mental health complications post-COVID-19: Scoping review. J. Psychosom. Res. 2021, 147, 110525. [Google Scholar] [CrossRef]
- Vadivel, R.; Shoib, S.; El Halabi, S.; El Hayek, S.; Essam, L.; Bytyci, D.G.; Karaliuniene, R.; Teixeira, A.L.S.; Nagendrappa, S.; Ramalho, R.; et al. Mental health in the post-COVID-19 era: Challenges and the way forward. Gen. Psychiatry 2021, 34, e100424. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Wang, Y.Y.; Lin, H.J.; Chen, X.X.; Wang, H.; Liang, H.B.; Guo, X.Q.; Fu, C.W. Mental Health Problems Among School-Aged Children After School Reopening: A Cross-Sectional Study During the COVID-19 Post-pandemic in East China. Front. Psychol. 2021, 12, 773134. [Google Scholar] [CrossRef]
- Yuan, K.; Gong, Y.M.; Liu, L.; Sun, Y.K.; Tian, S.S.; Wang, Y.J.; Zhong, Y.; Zhang, A.Y.; Su, S.Z.; Liu, X.X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.J.; Zhang, S.F.; Li, W.; Zhang, L.; Cheung, T.; Tang, Y.L.; Ng, C.H.; Yang, B.X.; Xiang, Y.T. Mental health status and quality of life in close contacts of COVID-19 patients in the post-COVID-19 era: A comparative study. Transl. Psychiatry 2021, 11, 505. [Google Scholar] [CrossRef]
- Freeman, M. The World Mental Health Report: Transforming mental health for all. World Psychiatry 2022, 21, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. Eclinicalmedicine 2020, 24, 100424. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L. Mental health as a complete state: How the salutogenic perspective completes the picture. In Bridging Occupational, Organizational and Public Health; Springer: Berlin/Heidelberg, Germany, 2014; pp. 179–192. [Google Scholar]
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a new definition of mental health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, T.N.; Wallstrom, I.G.; Stenager, E.; Bojesen, A.B.; Gluud, C.; Nordentoft, M.; Eplov, L.F. Effects of Individual Placement and Support Supplemented With Cognitive Remediation and Work-Focused Social Skills Training for People With Severe Mental Illness A Randomized Clinical Trial. JAMA Psychiatry 2019, 76, 1232–1240. [Google Scholar] [CrossRef]
- Jensen, A.; Bonde, L.O. The use of arts interventions for mental health and wellbeing in health settings. Perspect. Public Health 2018, 138, 209–214. [Google Scholar] [CrossRef]
- Lykins, E.L.B.; Baer, R.A. Psychological Functioning in a Sample of Long-Term Practitioners of Mindfulness Meditation. J. Cogn. Psychother. 2009, 23, 226–241. [Google Scholar] [CrossRef]
- Matiz, A.; Fabbro, F.; Paschetto, A.; Cantone, D.; Paolone, A.R.; Crescentini, C. Positive Impact of Mindfulness Meditation on Mental Health of Female Teachers during the COVID-19 Outbreak in Italy. Int. J. Environ. Res. Public Health 2020, 17, 6450. [Google Scholar] [CrossRef]
- Emunah, R. Acting for Real: Drama Therapy Process, Technique, and Performance; Routledge: Abingdon-on-Thames, UK, 2013. [Google Scholar]
- Jennings, S. Dramatherapy: Theory and Practice 1; Routledge: Abingdon-on-Thames, UK, 2014. [Google Scholar]
- Jones, P. Drama as Therapy Volume 2: Clinical Work and Research into Practice; Routledge: Abingdon-on-Thames, UK, 2010. [Google Scholar]
- Landy, R.; Montgomery, D.T. Theatre for Change: Education, Social Action and Therapy; Bloomsbury Publishing: London, UK, 2012. [Google Scholar]
- Langley, D.M.; Langley, G.E. Dramatherapy and Psychiatry; Routledge: Abingdon-on-Thames, UK, 2018; Volume 14. [Google Scholar]
- Hougham, R.; Jones, B. Dramatherapy: The Nature of Interruption; Routledge: Abingdon-on-Thames, UK, 2021. [Google Scholar]
- McAdam, E.; Johnson, D.R. Reducing depressive symptoms in adolescents with posttraumatic stress disorder using drama therapy. In Arts Therapies in the Treatment of Depression; Routledge: Abingdon-on-Thames, UK, 2018; pp. 48–67. [Google Scholar]
- Rubin, S. Almost magic: Working with the shame that underlies depression using drama therapy in the imaginal realm. In The Use of the Creative Therapies in Treating Depression; Charles C Thomas Publisher Limited: Springfield, IL, USA, 2015; pp. 231–244. [Google Scholar]
- Sajnani, N.; Cho, A.; Landis, H.; Raucher, G.; Trytan, N. Collaborative discourse analysis on the use of drama therapy to treat depression in adults. In Arts Therapies in the Treatment of Depression; Routledge: Abingdon-on-Thames, UK, 2018; pp. 87–101. [Google Scholar]
- Bleuer, J.; Harnden, B. Translating drama therapy: Reflections on clinical practice with complex trauma. Drama Ther. Rev. 2018, 4, 167–182. [Google Scholar] [CrossRef]
- Haen, C. Vanquishing Monsters: Group Drama Therapy for Treating Trauma; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Ashori, M.; Yazdanipour, M. Investigation of the effictiveness of group play therapy training with cognitive-behavioral approach on the social skills of students with intellectual disability. Arch. Rehabil. 2018, 19, 262–275. [Google Scholar] [CrossRef] [Green Version]
- Geiger, A.; Shpigelman, C.-N.; Feniger-Schaal, R. The socio-emotional world of adolescents with intellectual disability: A drama therapy-based participatory action research. Arts Psychother. 2020, 70, 101679. [Google Scholar] [CrossRef]
- Mora, L.; van Sebille, K.; Neill, L. An evaluation of play therapy for children and young people with intellectual disabilities. Res. Pract. Intellect. Dev. Disabil. 2018, 5, 178–191. [Google Scholar] [CrossRef]
- Snow, S.; D’Amico, M.; Mongerson, E.; Anthony, E.; Rozenberg, M.; Opolko, C.; Anandampillai, S. Ethnodramatherapy applied in a project focusing on relationships in the lives of adults with developmental disabilities, especially romance, intimacy and sexuality. Drama Ther. Rev. 2017, 3, 241–260. [Google Scholar] [CrossRef] [PubMed]
- Abraham, N. The Pedagogy of Reciprocity in Digital Applied Theatre Practice: The antithesis to unjust responses to the COVID-19 pandemic that have devalued and ignored the rights and lives of older adults living with dementia. Welf. Ergon. 2022, 2, 49–63. [Google Scholar] [CrossRef]
- Alizadeh, F.; Jiang, L. Application Of Theatre In Digital Space For Mental Health Care During COVID-19 Pandemic. MIER J. Educ. Stud. Trends Pract. 2022, 223–241. [Google Scholar] [CrossRef]
- Pufahl, J.; Simerly, S.; Bayne, H.; Reina Munoz, C. Virtually Commedia: An interactive online theatre programme for LGBTQ+ youth. J. Appl. Arts Health 2022, 13, 107–117. [Google Scholar] [CrossRef]
- Reyes, O. Drama Therapy Interventions that Support Students with ASD During COVID-19. Expressive Therapies Capstone Theses. Master’s Thesis, Lesley University, Cambridge, MA, USA, 2022. [Google Scholar]
- Ehrlich, H.; McKenney, M.; Elkbuli, A. Protecting our healthcare workers during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 1527. [Google Scholar] [CrossRef]
- Cheek-O’Donnell, S. Theatre; Emerald Group Publishing: Bingley, UK, 2021. [Google Scholar]
- Rosenthal, R.; DiMatteo, M.R. Meta-analysis: Recent developments in quantitative methods for literature reviews. Annu. Rev. Psychol. 2001, 52, 59–82. [Google Scholar] [CrossRef] [Green Version]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, 14651858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon-on-Thames, UK, 2013. [Google Scholar]
- Abeditehrani, H.; Dijk, C.; Toghchi, M.S.; Arntz, A. Integrating cognitive behavioral group therapy and psychodrama for social anxiety disorder: An intervention description and an uncontrolled pilot trial. Clin. Psychol. Eur. 2020, 2, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Albal, E.; Sahin-Bayindir, G.; Alanli, O.; Buzlu, S. The effects of psychodrama on the emotional awareness and communication skills of psychiatric nurses: A randomized controlled trial. Arts Psychother. 2021, 75, 101826. [Google Scholar] [CrossRef]
- Cheung, A.; Agwu, V.; Stojcevski, M.; Wood, L.; Fan, X. A Pilot Remote Drama Therapy Program Using the Co-active Therapeutic Theater Model with People with Serious Mental Illness. Community Ment. Health J. 2022, 58, 1613–1620. [Google Scholar] [CrossRef]
- Fallahi, N.; Tashk, A.; Towhidi, A. The Effectiveness of Cognitive-Behavioral Psychodrama Group Therapy (CBPGT) on Inadequate Guardian Male Adolescents’ Creativity and Critical Thinking. Think. Skills Creat. 2022, 47, 101171. [Google Scholar] [CrossRef]
- Feniger-Schaal, R.; Koren-Karie, N. Using Drama Therapy to Enhance Maternal Insightfulness and Reduce Children’s Behavior Problems. Front. Psychol. 2021, 11, 586630. [Google Scholar] [CrossRef]
- Giacomucci, S.; Marquit, J. The effectiveness of trauma-focused psychodrama in the treatment of PTSD in inpatient substance abuse treatment. Front. Psychol. 2020, 11, 896. [Google Scholar] [CrossRef]
- Giacomucci, S.; Marquit, J.; Walsh, K.M.; Saccarelli, R. A mixed-methods study on psychodrama treatment for PTSD and depression in inpatient substance use treatment: A comparison of outcomes pre-pandemic and during COVID-19. Arts Psychother. 2022, 81, 101971. [Google Scholar] [CrossRef]
- Jang, S.J.; Han, J.-S.; Bang, M.H.; Ahn, J.-W. Effects of a Sociodrama-based Communication Enhancement Program on Mothers of Children with Neurodevelopmental Disorders: A Pilot Study. Asian Nurs. Res. 2022, 16, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Keisari, S.; Palgi, Y.; Yaniv, D.; Gesser-Edelsburg, A. Participation in life-review playback theater enhances mental health of community-dwelling older adults: A randomized controlled trial. Psychol. Aesthet. Creat. Arts 2022, 16, 302. [Google Scholar] [CrossRef]
- Kejani, M.; Raeisi, Z. The effect of drama therapy on working memory and its components in primary school children with ADHD. Curr. Psychol. 2020, 41, 417–426. [Google Scholar] [CrossRef]
- Lin, L.; Lu, Y.; Chang, T.; Yeh, S. Effects of Drama Therapy on Depressive Symptoms, Attention, and Quality of Life in Patients With Dementia. J. Nurs. Res. 2022, 30, e188. [Google Scholar] [CrossRef] [PubMed]
- Manna, N. Velvi’s Theatre Intervention for Children with Autism Spectrum Disorder (ASD): An Assessment of Effect of Drama Therapy. Indian J. Health Wellbeing 2021, 12, 361–366. [Google Scholar]
- Mojahed, A.; Zaheri, Y.; Moqaddam, M.F. Effectiveness of group psychodrama on aggression and social anxiety of children with attention-deficit/hyperactivity disorder: A randomized clinical trial. Arts Psychother. 2021, 73, 101756. [Google Scholar] [CrossRef]
- Mondolfi Miguel, M.L.; Pino-Juste, M. Therapeutic achievements of a program based on drama therapy, the theater of the oppressed, and psychodrama with women victims of intimate partner violence. Violence Against Women 2021, 27, 1273–1296. [Google Scholar] [CrossRef]
- Nemati, A.; Demehri, F.; Saeidmanesh, M. Effect of Psychodrama on Communication Skills of Adolescents with Hearing Loss. Audit. Vestib. Res. 2022, 31, 92–97. [Google Scholar] [CrossRef]
- Purrezaian, H.; Besharat, M.A.; Koochakzadeh, L.; Farahani, H. Psycho-art-drama: Development and testing a new integrated complementary method of psychiatric treatments for hospitalised children with cancer (a case study). Int. J. Psychiatry Clin. Pract. 2020, 24, 183–192. [Google Scholar] [CrossRef]
- Ray, P.; Pendzik, S. Autobiographical therapeutic performance as a means of improving executive functioning in traumatized adults. Front. Psychol. 2021, 12, 599914. [Google Scholar] [CrossRef]
- Sevi, O.M.; Ger, M.; Kaya, F.; Maşalı, B. The effect of psychodrama sessions on psychotic symptoms, depression, quality of life, and sociometric measures in patients with chronic schizophrenia. Arts Psychother. 2020, 71, 101719. [Google Scholar] [CrossRef]
- Simsek, C.; Mengi, A.; Yalcinkaya, E.Y. The effect of psychodrama on quality of life and sleep in mothers of children with cerebral palsy. Arts Psychother. 2021, 72, 101726. [Google Scholar] [CrossRef]
- Swami, V.; Punshon, S.; Paul, T.-D. Promoting positive body image in children through theatre: An evaluation of Cinderella: The AWESOME Truth. Body Image 2022, 42, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Testoni, I.; Bonelli, B.; Biancalani, G.; Zuliani, L.; Nava, F.A. Psychodrama in attenuated custody prison-based treatment of substance dependence: The promotion of changes in wellbeing, spontaneity, perceived self-efficacy, and alexithymia. Arts Psychother. 2020, 68, 101650. [Google Scholar] [CrossRef]
- Testoni, I.; Ronconi, L.; Biancalani, G.; Zottino, A.; Wieser, M.A. My future: Psychodrama and meditation to improve well-being through the elaboration of traumatic loss among Italian high school students. Front. Psychol. 2021, 11, 544661. [Google Scholar] [CrossRef]
- Tümlü, G.Ü.; Şimşek, B.K. The effects of psychodrama groups on feelings of inferiority, flourishing, and self-compassion in research assistants. Arts Psychother. 2021, 73, 101763. [Google Scholar] [CrossRef]
- Vlotinou, P.; Aikaterini, T.; Anna, T.; Alexandrina, N.; Theofanis, V.; Konstantinos, V.; Ioannis, H. Changes in the quality of life of persons with epilepsy, after the implementation of an occupational therapy intervention with drama activities. Epilepsy Behav. 2022, 130, 108694. [Google Scholar] [CrossRef]
- Yu, R.-Q.; Tan, H.; Wang, E.-D.; Huang, J.; Wang, P.-J.; Li, X.-M.; Zheng, H.-H.; Lv, F.-J.; Hu, H. Antidepressants combined with psychodrama improve the coping style and cognitive control network in patients with childhood trauma-associated major depressive disorder. World J. Psychiatry 2022, 12, 1016. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Corey, G. Theory and Practice of Counseling and Psychotherapy; Cengage Learning: Boston, MA, USA, 2012. [Google Scholar]
- Enelow, S. Method Acting and Its Discontents: On American Psycho-Drama; Northwestern University Press: Evanston, IL, USA, 2015. [Google Scholar]
- Wu, J.; Chen, K.; Ma, Y.; Vomočilová, J. Early intervention for children with intellectual and developmental disability using drama therapy techniques. Child. Youth Serv. Rev. 2020, 109, 104689. [Google Scholar] [CrossRef]
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1217–1220. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| #1 | “mental health”[MeSH] OR “psychological wellbeing”[MeSH] |
| #2 | (((((((Mental Health [Title/Abstract]) OR Health, Mental [Title/Abstract]) OR Mental Hygiene [Title/Abstract]) OR Hygiene, Mental [Title/Abstract]) OR psychological wellbeing [Title/Abstract]) OR psychological wellness [Title/Abstract]) OR psychological ill being [Title/Abstract]) OR ill being psychological [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | “drama”[MeSH] OR “psychodrama”[MeSH] OR “role playing”[MeSH] |
| #5 | (((((((drama [Title/Abstract]) OR dramas [Title/Abstract]) OR drama therapy [Title/Abstract]) OR therapy, drama [Title/Abstract]) OR dramatherapy [Title/Abstract]) OR playing, role [Title/Abstract]) OR playings, role [Title/Abstract]) OR role playings [Title/Abstract] |
| #6 | #4 OR #5 |
| #7 | “from 2019–2022” |
| #8 | #3 AND #6 AND #7 |
| First Author (Year) | Country | Population | Design | Age (Mean + SD) | Total/Male/Female | Intervention | Outcome Measure |
|---|---|---|---|---|---|---|---|
| Abeditehrani (2020) [50] | The Netherlands | Adult female patients with SAD | Pre/post treatment | T: 36.6 (17.8) C: NA | T: 5/0/5 C: NA | Psychodrama Period: 12 weeks Freq: once a week Duration: 2.5 h | Quality of life: QLS; Depression: BDI; Anxiety: LSAS |
| Albal (2021) [51] | Turkey | Psychiatric nurses | Randomised controlled trial | T: 35.54 (9.03) C: 39.62 (5.12) | T: 13/1/12 C: 13/0/13 | Psychodrama Period: 8 weeks Freq: once a week Duration: 2 h | Communication skills: CSI |
| Cheung (2022) [52] | USA | People with SMI | Pre/post treatment | T: 51.5 (9.4) C: NA | T: 8/4/4 C: NA | Drama therapy Period: 12 weeks Freq: once a week for 10 weeks Duration: 1.5 h | Psychological well-being: BPRS; Quality of Life: QLESS; Depression: PSS |
| Fallahi (2022) [53] | Iran | Inadequate guardian male adolescents | Controlled trial with pre/posttest | T: NA C: NA | T: 15/15/0 C: 15/15/0 | Psychodrama Period: 6 weeks Freq: NA Duration: 2 h | Cognitive functioning: EMI |
| Feniger-Schaal (2021) [54] | Israel | Mothers of children-at-risk | Pre/post treatment | T: 37 (5.9) C: NA | T: 40/0/40 C: NA | Drama therapy Period: 10 weeks Freq: NA Duration: 1.5 h | Cognitive functioning: CBCL |
| Giacomucci (2020) [55] | USA | People with PTSD | Pre/post treatment | T: 41.34 (12.53) C: NA | T: 86/40/44/ 2 transgenders C: NA | Psychodrama Period: 64 weeks Freq: twice a week Duration: 2.25 h | Trauma-related disorders: PCL |
| Giacomucci (2022) [56] | USA | People with depression and PTSD | Pre/post treatment | T:40.60 (11.79) C: NA | T: 20/6/14 C: NA | Psychodrama Period: 72 weeks Freq: twice a week Duration: 2.25 h | Trauma-related disorders: PCL |
| Jang (2022) [57] | South Korea | Mothers of children with ND | Non-randomised controlled experiment | T: 42.62 (6.29) C: 42.67 (7.34) | T: 16/0/16 C: 18/0/16 | Sociodrama Period: 6 weeks Freq: once a week Duration: 2.5 h | Commination skills: PACS |
| Keisari (2022) [58] | Israel | Community-dwelling older adults | Randomised controlled trial | T: 78.65 (6.91) C: 80.60 (6.81) | T: 40/9/31 C: 38/6/32 | Playback theatre Period: 12-week Freq: once a week Duration: 1.5 h | Quality of life: SLS; Depression: GDS; Self-regard: SEC |
| Kejani (2020) [59] | Iran | ADHD primary school children | Quasi-experiment with pre/posttest | T: NA C: NA | T: 21/10/11 C: 24/12/12 | Drama therapy Period: 6 weeks Freq: twice a week Duration: 1.5 h | Cognitive functioning: WISC |
| Lin (2022) [60] | Taiwan | Patients with dementia | Randomized controlled trial with pre/posttest | T: 82.62 (7.92) C: 82.58 (7.74) | T: 23/4/19 C: 19/5/14 | Drama therapy Period: 8 weeks Freq: once a week Duration: 1.5 h | Quality of life: ADLS; Psychological well-being: MMSE; Depression: CSDD |
| Manna (2021) [61] | India | Children with ASD | Pre/post treatment | T: NA C: NA | T: 16/11/5 C: NA | Drama therapy Period: NA Freq: NA Duration: NA | Cognitive functioning: CSCR |
| Mojahed (2021) [62] | Iran | Children with ADHD | Randomised controlled trial with pre/posttest | T: 9.92 (1.381) C: 9.79 (1.285) | T: 24/24/0 C: 24/24/0 | Psychodrama Period: 10 weeks Freq: once a week Duration: 2 h | Cognitive functioning: CBCL; Anxiety: SCAS |
| Miguel (2021) [63] | Spain | Women victims of intimate partner violence | Pre/post treatment | T: 49 (NA) C: NA | T: 17/0/17 C: NA | Drama therapy, theatre of the oppressed, and psychodrama Period: 20 sessions Freq: NA Duration: 2 h | Trauma-related disorders: SPSS; Quality of life: QLS; Depression: BDI; Self-regard: SES |
| Nemati (2022) [64] | Iran | Adolescents with hearing loss | Quasi-experiment with pre/posttest | T: 13.9(1.46) C: 14.3 (0.86) | T:12/ NA/ NA C: 12/ NA/ NA | Psychodrama Period: 5 weeks Freq: twice a week Duration: 1.5 h | Communication skills: QCST |
| Purrezaian (2020) [65] | Iran | Hospitalised children with cancer | Pre/post treatment | T: 11(1.58) C: NA | T: 5/2/3 C: NA | Psycho-art-drama Period: 8 sessions Freq: NA Duration: 40–60 min | Communication skills: BPSEIH |
| Ray (2021) [66] | Israel | Traumatised adults | Pre/post treatment | T: NA C: NA | T: 10/1/9 C: NA | Autobiographical therapeutic performance Period: 10 month Freq: NA Duration: NA | Cognitive functioning: BRIEF-A |
| Sevi (2020) [67] | Turkey | Patients with chronic schizophrenia | Pre/post treatment | T: 55.52 (7.45) C: NA | T: 31/19/12 C: NA | Psychodrama Period: 19 session Freq: once a week Duration: 1.5−2 h | Depression: CDS; Quality of life: QLS |
| Simsek (2021) [68] | Turkey | Mothers of children with cerebral palsy | Controlled trial | T: 30.8 (7.0) C: 33.1 (7.4) | T: 8/0/8 C: 14/0/14 | Psychodrama Period: 8 weeks Freq: once a week Duration: 2 h | Quality of life: QLS |
| Swami (2022) [69] | UK | Children between 5 and 9 years | Pre/post treatment | T: 7.08 (1.53) C: NA | T: 99/45/54 C: NA | Theatrical performance Period: 8 weeks Freq: NA Duration: NA | Self-regard: BAS |
| Testoni (2020) [70] | Italy | Prisoner with substance dependence | Pre/post treatment | T: 34 (8.71) C: NA | T: 7/7/0 C: NA | Psychodrama Period: 24 weeks Freq: once a week Duration: 1.5 to 2 h | Cognitive functioning: SAI-R; Self-regard: GSE; |
| Testoni (2021) [71] | Italy | Traumatic high school students | Controlled trial with pre/posttest | T: 15.98 (1.12) C: 16.14 (1.00) | T: 45/18/27 C: 37/4/33 | Psychodrama Period: 5 weeks Freq: NA Duration: 2 h | Psychological well-being: PWS; |
| Tümlü (2021) [72] | Turkey | Research assistants | Quasi-experiment with pre/posttest | T: 30.9 (3.3) C: 31.6 (2.9) | T: 7/NA/NA C: 7/NA/NA | Psychodrama Period: 10 weeks Freq: once a week Duration: 3 h | Self-regard: SCS |
| Vlotinou (2022) [73] | Greece | Patients with epilepsy | Pre/post treatment | T: 32.27 (13.55) C: NA | T:15/6/9 C: NA | Occupational therapy program with drama activities Period: 12 weeks Freq: once a week Duration: 2 h | Quality of life: QLS |
| Yu (2022) [74] | China | Patients with childhood trauma-associated MDD | Randomised controlled trial | T: 25.97 (7.189) C: 28.12 (6.214) | T: 29/7/22 C: 17/2/15 | Psychodrama Period: 24 weeks Freq: once eight weeks Duration: 4 days | Depression: BDI; Anxiety: BAI |
| Effects | Heterogeneity | |||||
|---|---|---|---|---|---|---|
| Outcome | Study Design | SAMPLE SIZE | SMD (IV, Random, 95%CI) | p | I2 (%) | p |
| Quality of life | Controlled group (n = 4) | 139 | 2.08 [−0.33, 4.49] | 0.09 | 96 | <0.00001 |
| Pre/posttest group (n = 5) | 74 | 0.86 [0.06, 1.67] | 0.04 | 79 | 0.0002 | |
| Total (n = 9) | 213 | 1.26 [0.33, 2.20] | 0.008 | 91 | <0.00001 | |
| Psychological well-being | Controlled group (n = 4) | 202 | 1.69 [−0.45, 3.83] | 0.12 | 97 | <0.00001 |
| Pre/posttest group (n = 1) | 6 | 0.46 [−0.69, 1.62] | 0.43 | - | - | |
| Total (n = 5) | 208 | 1.40 [−0.32, 3.12] | 0.11 | 96 | <0.00001 | |
| Depression | Controlled group (n = 3) | 166 | 1.17 [−0.35, 2.70] | 0.13 | 95 | <0.00001 |
| Pre/posttest group (n = 4) | 59 | 0.42 [0.05, 0.78] | 0.03 | 0 | 0.82 | |
| Total (n = 7) | 225 | 0.70 [−0.03, 1.42] | 0.03 | 85 | <0.00001 | |
| Anxiety | Controlled group (n = 2) | 94 | 0.88 [−0.82, 2.58] | 0.31 | 93 | 0.0002 |
| Pre/posttest group (n = 1) | 5 | 1.74 [0.16, 3.32] | 0.03 | - | - | |
| Total (n = 3) | 99 | 1.10 [−0.24, 2.45] | 0.11 | 87 | 0.0004 | |
| Trauma-related disorders | Controlled group (n = 1) | 46 | 0.14 [−0.46, 0.74] | 0.65 | - | - |
| Pre/posttest group (n = 3) | 123 | 0.90 [0.52, 1.28] | <0.00001 | 36 | 0.21 | |
| Total (n = 4) | 169 | 0.70 [0.23, 1.17] | 0.003 | 66 | 0.03 | |
| Communication skills | Controlled group (n = 3) | 86 | 1.11 [−0.68, 2.90] | 0.22 | 92 | <0.00001 |
| Pre/posttest group (n = 1) | 5 | 4.98 [1.91, 8.04] | 0.001 | - | - | |
| Total (n = 4) | 91 | 1.76 [−0.06, 3.57] | 0.06 | 91 | <0.00001 | |
| Cognitive functioning | Controlled group (n = 3) | 123 | 1.58 [0.62, 2.54] | 0.001 | 81 | <0.00001 |
| Pre/posttest group (n = 4) | 66 | 3.47 [−1.02, 7.97] | 0.13 | 98 | 0.006 | |
| Total (n = 7) | 189 | 2.50 [0.77, 4.23] | 0.005 | 96 | <0.00001 | |
| Self-regard | Controlled group (n = 2) | 92 | 2.83 [−0.90, 6.56] | 0.14 | 96 | <0.00001 |
| Pre/posttest group (n = 3) | 123 | 0.39 [0.14, 0.65] | 0.002 | 0 | 0.83 | |
| Total (n = 5) | 215 | 1.40 [−0.06, 2.86] | 0.06 | 95 | <0.00001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, L.; Alizadeh, F.; Cui, W. Effectiveness of Drama-Based Intervention in Improving Mental Health and Well-Being: A Systematic Review and Meta-Analysis during the COVID-19 Pandemic and Post-Pandemic Period. Healthcare 2023, 11, 839. https://doi.org/10.3390/healthcare11060839
Jiang L, Alizadeh F, Cui W. Effectiveness of Drama-Based Intervention in Improving Mental Health and Well-Being: A Systematic Review and Meta-Analysis during the COVID-19 Pandemic and Post-Pandemic Period. Healthcare. 2023; 11(6):839. https://doi.org/10.3390/healthcare11060839
Chicago/Turabian StyleJiang, Lulu, Farideh Alizadeh, and Wenjing Cui. 2023. "Effectiveness of Drama-Based Intervention in Improving Mental Health and Well-Being: A Systematic Review and Meta-Analysis during the COVID-19 Pandemic and Post-Pandemic Period" Healthcare 11, no. 6: 839. https://doi.org/10.3390/healthcare11060839