
Change Trajectory of Symptom Distress, Coping Strategies, and Spiritual Wellbeing in Colorectal Cancer Patients Undergoing Chemotherapy


Abstract
1. Introduction
2. Methods
2.1. Study Design and Subjects
2.2. Study Process
2.3. Study Tools
2.3.1. M. D. Anderson Symptom Inventory-Taiwan Form (MDASI-T)
2.3.2. Jalowiec Coping Scale (JCS)
2.4. Data Analysis
3. Results
3.1. Relationship between Patient Demographics, Medical Characteristics, and Spiritual Wellbeing
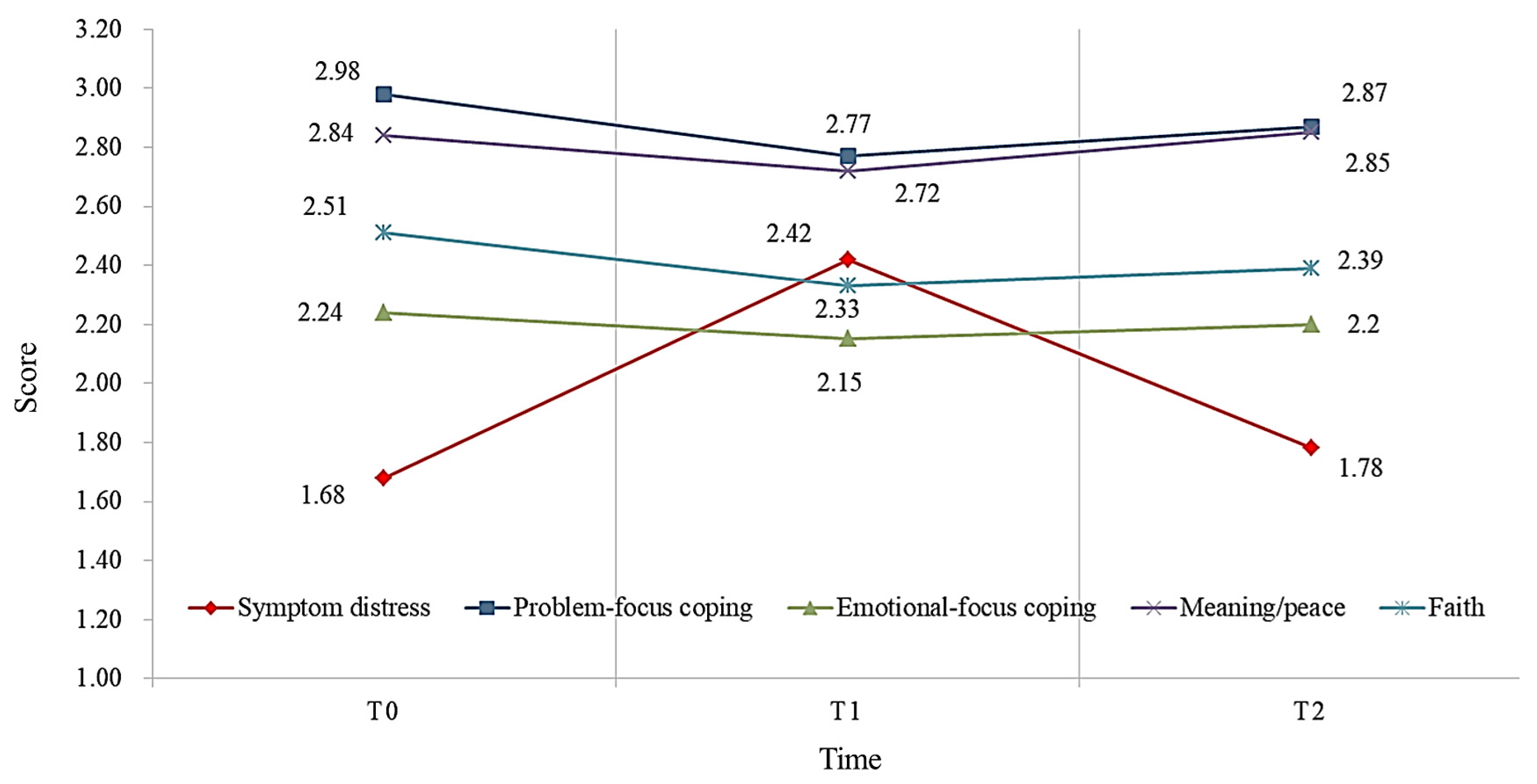
3.2. Scores and Trends of Symptom Distress, Coping Strategies and Spiritual Wellbeing
3.3. Correlation between Symptom Distress, Coping Strategies, and Spiritual Wellbeing
3.4. Predictors of Spiritual Wellbeing
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- World Health Organization. New Cancer Report Offers Hope for Patients and Communities. Available online: https://www.who.int/news/item/28-06-2002-new-cancer-report-offers-hope-for-patients-and-communities (accessed on 2 April 2022).
- Ministry of Health and Welfare. Historical Statistics: 109 Death Statistics. Available online: https://dep.mohw.gov.tw/dos/lp-5069-113.html (accessed on 2 April 2022).
- Ferrell, B.; Chung, V.; Koczywas, M.; Borneman, T.; Irish, T.L.; Ruel, N.H.; Azad, N.S.; Rhonda, S.; Cooper, R.S.; Smith, T.J. Spirituality in cancer patients on phase 1 clinical trials. Psycho-Oncology 2022, 29, 1077–1083. [Google Scholar] [CrossRef]
- Puchalski, C.M. Spirituality in the cancer trajectory. Ann. Oncol. 2012, 23, iii49–iii55. [Google Scholar] [CrossRef] [PubMed]
- Hungelmann, J.; Kenkel-Rossi, E.; Klassen, L.; Stollenwerk, R.M. Spiritual well-being in older adults: Harmonious interconnectedness. J. Relig. Health 1985, 24, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Hungelmann, J.; Kenkel-Rossi, E.; Klassen, L.; Stollenwerk, R. Focus on spiritual well-being: Harmonious interconnectedness of mind-body-spirit—Use of the JAREL spiritual well-being scale: Assessment of spiritual well-being is essential to the health of individuals. Geriatr. Nurs. 1996, 17, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Nejat, N.; Whitehead, L.; Crowe, M. The use of spirituality and religiosity in coping with colorectal cancer. Contemp. Nurse 2017, 53, 48–59. [Google Scholar] [CrossRef]
- Paredes, A.C.; Pereira, M.G. Spirituality, distress and posttraumatic growth in breast cancer patients. J. Relig. Health 2018, 57, 1606–1617. [Google Scholar] [CrossRef]
- Puchalski, C.M.; Sbrana, A.; Ferrell, B.; Jafari, N.; King, S.; Balboni, T.; Miccinesi, G.; Vandenhoeck, A.; Silbermann, M.; Balducci, L.; et al. Interprofessional spiritual care in oncology: A literature review. ESMO Open 2019, 4, e000465. [Google Scholar] [CrossRef]
- Rabow, M.W.; Knish, S.J. Spiritual well-being among outpatients with cancer receiving concurrent oncologic and palliative care. Support. Care Cancer 2015, 23, 919–923. [Google Scholar] [CrossRef]
- Miles, A.; McClements, P.L.; Steele, R.J.C.; Redeker, C.; Sevdalis, N.; Wardle, J. Perceived diagnostic delay and cancer-related distress: A cross-sectional study of patients with colorectal cancer. Psycho-Oncology 2017, 26, 29–36. [Google Scholar] [CrossRef]
- Stanton, A.L.; Wiley, J.F.; Krull, J.L.; Crespi, C.M.; Weihs, K.L. Cancer-related coping processes as predictors of depressive symptoms, trajectories, and episodes. J. Consult. Clin. Psychol. 2018, 86, 820–830. [Google Scholar] [CrossRef]
- Foster, C.; Haviland, J.; Winter, J.; Grimmett, C.; Seymour, K.C.; Batehup, L.; Calman, L.; Corner, J.; Din, A.; Fenlon, D.; et al. Pre-surgery depression and confidence to manage problems predict recovery trajectories of health and wellbeing in the first two Years following colorectal cancer: Results from the CREW cohort study. PLoS ONE 2016, 11, e0155434. [Google Scholar] [CrossRef] [PubMed]
- Bovero, A.; Tosi, C.; Botto, R.; Opezzo, M.; Giono-Calvetto, F.; Torta, R. The Spirituality in End-of-Life Cancer Patients, in Relation to Anxiety, Depression, Coping Strategies and the Daily Spiritual Experiences: A Cross-Sectional Study. J. Relig. Health 2019, 58, 2144–2160. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Abelson, J.S.; Chait, A.; Shen, M.J.; Charlson, M.; Dickerman, A.; Yeo, H. Coping strategies among colorectal cancer patients undergoing surgery and the role of the surgeon in mitigating distress: A qualitative study. Surgery 2019, 165, 461–468. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S.; Gruen, R.J.; DeLongis, A. Appraisal, coping, health status, and psychological symptoms. J. Pers. Soc. Psychol. 1986, 50, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. The relationship between coping and emotion:Implications for theory and research. Soc. Sci. Med. 1988, 26, 309–317. [Google Scholar] [CrossRef]
- Peterman, A.H.; Fitchett, G.; Brady, M.J.; Hernandez, L.; Cella, D. Measuring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy—Spiritual well-being scale (FACIT-Sp). Ann. Behav. Med. 2002, 24, 49–58. [Google Scholar] [CrossRef]
- Lin, C.C.; Chang, A.P.; Cleeland, C.S.; Mendoza, T.R.; Wang, X.S. Taiwanese version of the M. D. Anderson symptom inventory: Symptom assessment in cancer patients. J. Pain Symptom Manag. 2007, 33, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.H.; Wei, C.W.; Tung, H.H.; Tung, T.H.; Liang, S.Y. Symptom severity and interference assessment in geriatric survivors of urinary bladder cancer. Aging Med. Healthc. 2019, 10, 72–79. [Google Scholar] [CrossRef]
- Wu, S.F.; Ching, C.Y.; Lee, H.Y.; Tung, H.Y.; Juan, C.W.; Chao, T.B. Symptom distress, depression, and quality of life in colorectal cancer patients at different disease stages. Hu Li Za Zhi 2015, 62, 68–80. [Google Scholar]
- Jalowiec, A. Construct Validation of the Jalowiec Coping Scale. Ph.D. Dissertation, University of Illinois, Chicago, IL, USA, 1985. [Google Scholar]
- Jalowiec, A. Confirmatory factor analysis of the Jalowiec Coping Scale. In Measurement of Nursing Outcomes; Measuring Client Outcomes; Waltz, C.E., Strickland, O.L., Eds.; Springer: New York, NY, USA, 1988; pp. 287–305. [Google Scholar]
- Chiou, C.P. An Exploratory Study of the Hemodialysis Patient’s Stress Perception, Psychosocial Adjustment and Related Factors. Master’s Thesis, National Defense Medical Center, Taipei, Taiwan, 1987. [Google Scholar]
- Yeh, Y.-C. Symptom distress, stress, and quality of life in the first year of gynecological cancers: A longitudinal study of women in Taiwan. Eur. J. Oncol. Nurs. 2021, 53, 101984. [Google Scholar] [CrossRef]
- Qaderi, S.M.; van der Heijden, J.A.G.; Verhoeven, R.H.A.; de Wilt, J.H.W.; Custers, J.A.E.; PLCRC study group. Trajectories of health-related quality of life and psychological distress in patients with colorectal cancer: A population-based study. Eur. J. Cancer. 2021, 158, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Sari, D.K.; Dewi, R.; Daulay, W. Association between family support, coping strategies and anxiety in cancer patients undergoing chemotherapy at general hospital in Medan, North Sumatera, Indonesia. Asian Pac. J. Cancer Prev. 2019, 20, 3015–3019. [Google Scholar] [CrossRef] [PubMed]
- Lashbrook, M.P.; Valery, P.C.; Knott, V.; Kirshbaum, M.N.; Bernardes, C.M. Coping strategies used by breast, prostate, and colorectal cancer survivors: A literature review. Cancer Nurs. 2018, 41, E23–E39. [Google Scholar] [CrossRef]
- Kyzar, K.B.; Turnbull, A.P.; Summers, J.A.; Gómez, V.A. The relationship of family support to family outcomes: A synthesis of key findings from research on severe disability. Res. Pract. Pers. Sev. Disabil. 2012, 37, 31–44. [Google Scholar] [CrossRef]
- Davidson, J.E.; Aslakson, R.A.; Long, A.C.; Puntillo, K.A.; Kross, E.K.; Hart, J.; Cox, C.E.; Wunsch, H.; Wickline, M.A.; Nunnally, M.E.; et al. Guidelines for family-centered care in the neonatal, pediatric, and adult ICU. Crit. Care Med. 2017, 45, 103–128. [Google Scholar] [CrossRef]
- Ulfah, Q.; Wulandari, Y.; Supatmi, S. Relationship of Family Support with Quality of Life among Breast Cancer Patients in Surabaya. In Proceedings of the 1st International Conference of Nursing and Public Health Virtually, Chicago, IL, USA, 6–7 October 2021. [Google Scholar]
- Pardede, J.A.; Simamora, M.; Simanjuntak, G.V. Family support and self-esteem of patient with breast cancer. EAS J. Nurs. Midwifery 2020, 2, 173–177. [Google Scholar]
- Ciria-Suarez, L.; Calderon, C.; Fernández Montes, A.; Antoñanzas, M.; Hernández, R.; Rogado, J.; Pacheo-Barcia, V.; Ansensio-Martínez, E.; Palacín-Lois, M.; Jimenez-Fonseca, P. Optimism and social support as contributing factors to spirituality in Cancer patients. Support. Care Cancer 2021, 29, 3367–3373. [Google Scholar] [CrossRef]
- Kamijo, Y.; Miyamura, T. Spirituality and associated factors among cancer patients undergoing chemotherapy. Jpn. J. Nurs. Sci. 2020, 17, e12276. [Google Scholar] [CrossRef] [PubMed]
- Zare, A.; Bahia, N.J.; Eidy, F.; Adib, N.; Sedighe, F. The relationship between spiritual well-being, mental health, and quality of life in cancer patients receiving chemotherapy. J. Fam. Med. Prim. Care 2019, 8, 1701–1705. [Google Scholar]
- Newberry, A.G.; Choi, C.W.; Donovan, H.S.; Schulz, R.; Bender, C.; Given, B.; Sherwood, P. Exploring spirituality in family caregivers of patients with primary malignant brain tumors across the disease trajectory. Oncol. Nurs. Forum 2013, 40, E119–E125. [Google Scholar] [CrossRef] [PubMed]
- Bailly, N.; Martinent, G.; Ferrand, C.; Agli, O.; Giraudeau, C.; Gana, K.; Roussiau, N. Spirituality, social support, and flexibility among older adults: A five-year longitudinal study. Int. Psychogeriatr. 2018, 30, 1745–1752. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | n (%) | Spiritual Wellbeing | t/F | p-Value | |
|---|---|---|---|---|---|
| M ± SD | |||||
| Sex | 0.18 | 0.98 | |||
| Male | 55 | 56.7 | 32.84 ± 7.30 | ||
| Female | 42 | 43.3 | 32.81 ± 7.07 | ||
| Age (years) | 0.86 | 0.42 | |||
| ≤55 | 29 | 29.9 | 33.76 ± 6.49 | ||
| 55-65 | 29 | 29.9 | 33.45 ± 7.14 | ||
| ≧66 | 39 | 40.2 | 31.67 ± 7.67 | ||
| Marital status | 0.40 | 0.68 | |||
| Unmarried/divorced/widowed | 31 | 32.0 | 33.26 ± 6.63 | ||
| Married | 66 | 68.0 | 32.62 ± 7.44 | ||
| Education level | 2.59 | 0.08 | |||
| Junior high school and below | 33 | 34.0 | 30.88 ± 7.04 | ||
| Senior high school and vocational school | 37 | 38.1 | 32.95 ± 7.43 | ||
| University and above | 27 | 27.8 | 35.04 ± 6.48 | ||
| Religion | −0.32 | .74 | |||
| No | 15 | 15.5 | 32.27 ± 6.53 | ||
| Yes | 82 | 84.5 | 32.93 ± 7.30 | ||
| Family monthly income (USD) | 0.03 | 0.96 | |||
| ≤3500 | 71 | 73.2 | 32.72 ± 7.31 | ||
| 3501–7100 | 19 | 19.6 | 33.00 ± 5.94 | ||
| ≧7101 | July | 7.2 | 33.43 ± 9.53 | ||
| Family support | −2.89 | 0.005 | |||
| Fair | 27 | 27.8 | 29.56 ± 6.69 | ||
| Good | 70 | 72.2 | 34.09 ± 6.68 | ||
| Employment | −1.38 | 0.16 | |||
| No | 75 | 77.3 | 32.28 ± 7.31 | ||
| Yes | 22 | 22.7 | 34.68 ± 6.42 | ||
| History of chronic disease | −1.62 | 0.10 | |||
| No | 53 | 54.6 | 31.75 ± 6.25 | ||
| Yes | 44 | 45.4 | 34.11 ± 8.01 | ||
| Smoking | −0.17 | 0.86 | |||
| No | 71 | 73.2 | 32.75 ± 7.26 | ||
| Yes | 26 | 26.8 | 33.04 ± 7.02 | ||
| Alcohol consumption | −1.08 | 0.28 | |||
| No | 80 | 82.5 | 32.46 ± 7.29 | ||
| Yes | 17 | 17.5 | 34.53 ± 6.44 | ||
| Cancer stage | 0.16 | 0.85 | |||
| II | 32 | 33.0 | 33.41 ± 7.03 | ||
| III | 44 | 45.4 | 32.61 ± 7.43 | ||
| IV | 21 | 21.6 | 32.38 ± 7.06 | ||
| Type of chemotherapy | 1.17 | 0.31 | |||
| Oxalip | 56 | 57.7 | 33.34 ± 6.96 | ||
| Campto | 37 | 38.1 | 31.65 ± 7.65 | ||
| Oral | 4 | 4.1 | 36.50 ± 3.31 | ||
| Variables | T0 | T1 | T2 | F | p-Value | LSD |
|---|---|---|---|---|---|---|
| M ± SD | M ± SD | M ± SD | ||||
| Symptom distress | 1.68 ± 1.11 | 2.42 ± 1.79 | 1.78 ± 1.41 | 16.28 | <0.001 | T1 > T0 |
| Severity | 2.00 ± 1.31 | 3.32 ± 1.56 | 2.52 ± 1.93 | 23.36 | <0.001 | T1 > T2 > T0 |
| Interference | 1.36 ± 1.12 | 1.53 ± 1.02 | 1.04 ± 0.98 | 9.14 | <0.001 | T0, T1 > T2 |
| Coping strategies | 2.51 ± 0.47 | 2.38 ± 0.37 | 2.44 ± 0.42 | 4.82 | 0.012 | T0 > T1 |
| Problem-focus | 2.98 ± 0.69 | 2.77 ± 0.60 | 2.87 ± 0.68 | 5.40 | 0.008 | T0 > T1 |
| Emotional-focus | 2.24 ± 0.46 | 2.15 ± 0.35 | 2.20 ± 0.37 | 2.16 | 0.126 | |
| Spiritual wellbeing | 32.82 ± 7.16 | 31.08 ± 6.31 | 32.44 ± 6.04 | 4.31 | 0.017 | T0, T2 > T1 |
| Meaning/peace | 22.76 ± 4.18 | 21.75 ± 3.74 | 22.86 ± 3.32 | 5.77 | 0.005 | T0, T2 > T1 |
| Faith | 10.06 ± 4.07 | 9.33 ± 3.47 | 9.59 ± 3.53 | 1.78 | 0.171 |
| Variables | Symptom Distress | Coping Strategies | ||
|---|---|---|---|---|
| Problem | Emotional | |||
| Symptom distress | 1 | |||
| Coping strategies | Problem | 0.127 | 1 | |
| Emotional | −0.289 | 0.072 | 1 | |
| Spiritual wellbeing | Meaning/peace | −0.075 | 0.504 ** | −0.098 |
| Faith Total scale | 0.141 0.036 | 0.566 ** 0.439 ** | −0.030 −0.160 | |
| Variables | T0 | T1 | T2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| B | t | p-Value | B | t | p-Value | B | t | p-Value | |
| Family support Fair (ref) vs. good | 0.39 | 2.74 | 0.007 ** | 0.13 | 1.33 | 0.184 | 0.20 | 1.77 | 0.079 |
| Symptom distress | −0.20 | −0.33 | 0.742 | −0.18 | −1.74 | 0.048 * | −0.07 | −0.26 | 0.797 |
| Problem coping | 0.47 | 4.87 | 0.001 ** | 0.26 | 2.23 | 0.028 * | 0.11 | 1.26 | 0.209 |
| Emotion coping | −0.17 | −1.91 | 0.060 | −0.11 | −0.97 | 0.330 | 0.02 | 0.25 | 0.799 |
| R2 | 0.52 | 0.30 | 0.25 | ||||||
| F | 8.60 | 2.23 | 1.64 | ||||||
| p-value | 0.001 ** | 0.045 * | 0.169 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, C.-W.; Liang, S.-Y.; Chin, C.-H.; Lin, H.-C.; Rosenberg, J. Change Trajectory of Symptom Distress, Coping Strategies, and Spiritual Wellbeing in Colorectal Cancer Patients Undergoing Chemotherapy. Healthcare 2023, 11, 857. https://doi.org/10.3390/healthcare11060857
Wei C-W, Liang S-Y, Chin C-H, Lin H-C, Rosenberg J. Change Trajectory of Symptom Distress, Coping Strategies, and Spiritual Wellbeing in Colorectal Cancer Patients Undergoing Chemotherapy. Healthcare. 2023; 11(6):857. https://doi.org/10.3390/healthcare11060857
Chicago/Turabian StyleWei, Ching-Wen, Shu-Yuan Liang, Chia-Hui Chin, Hua-Ching Lin, and John Rosenberg. 2023. "Change Trajectory of Symptom Distress, Coping Strategies, and Spiritual Wellbeing in Colorectal Cancer Patients Undergoing Chemotherapy" Healthcare 11, no. 6: 857. https://doi.org/10.3390/healthcare11060857
APA StyleWei, C.-W., Liang, S.-Y., Chin, C.-H., Lin, H.-C., & Rosenberg, J. (2023). Change Trajectory of Symptom Distress, Coping Strategies, and Spiritual Wellbeing in Colorectal Cancer Patients Undergoing Chemotherapy. Healthcare, 11(6), 857. https://doi.org/10.3390/healthcare11060857