
Effectiveness of Respiratory Rehabilitation in COVID-19’s Post-Acute Phase: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Research
2.2. Eligibility Criteria
- -
- P (population): patients diagnosed with COVID-19 in the post-acute phase and clinically stable were included. Instead, severe COVID-19 cases or acute-phase cases with clinical instability were excluded.
- -
- I (intervention): respiratory physiotherapy in its different means were included, either delivered in conventional form (in person) or through telemedicine. Other forms of rehabilitation were excluded.
- -
- C (comparison): patients who only receive standard assistance/cure or receive no cure.
- -
- O (outcome): improvement of respiratory function and physical performance, reduction in dyspnea and fatigue and improvement of autonomy and quality of life in patients affected by COVID-19. The Table 1 shows the PICO strategy used.
- -
- Publication date (year) of the articles: we have included in the revision those articles that had been published in multimedia databases in the time range spanning from the 1 January 2020 to the 27 September 2022.
- -
- Language of publication of the articles: all studies that were not redacted in either Italian or English were excluded.
- -
- Type of study: in the present review, we included randomized controlled trials, cohort studies, declarations of consent and practical guidelines on pulmonary rehabilitation for SARS-CoV-2.
2.3. Selection of the Studies
2.4. Data Collection Process
2.5. Evaluation of Methodologic Quality
3. Results
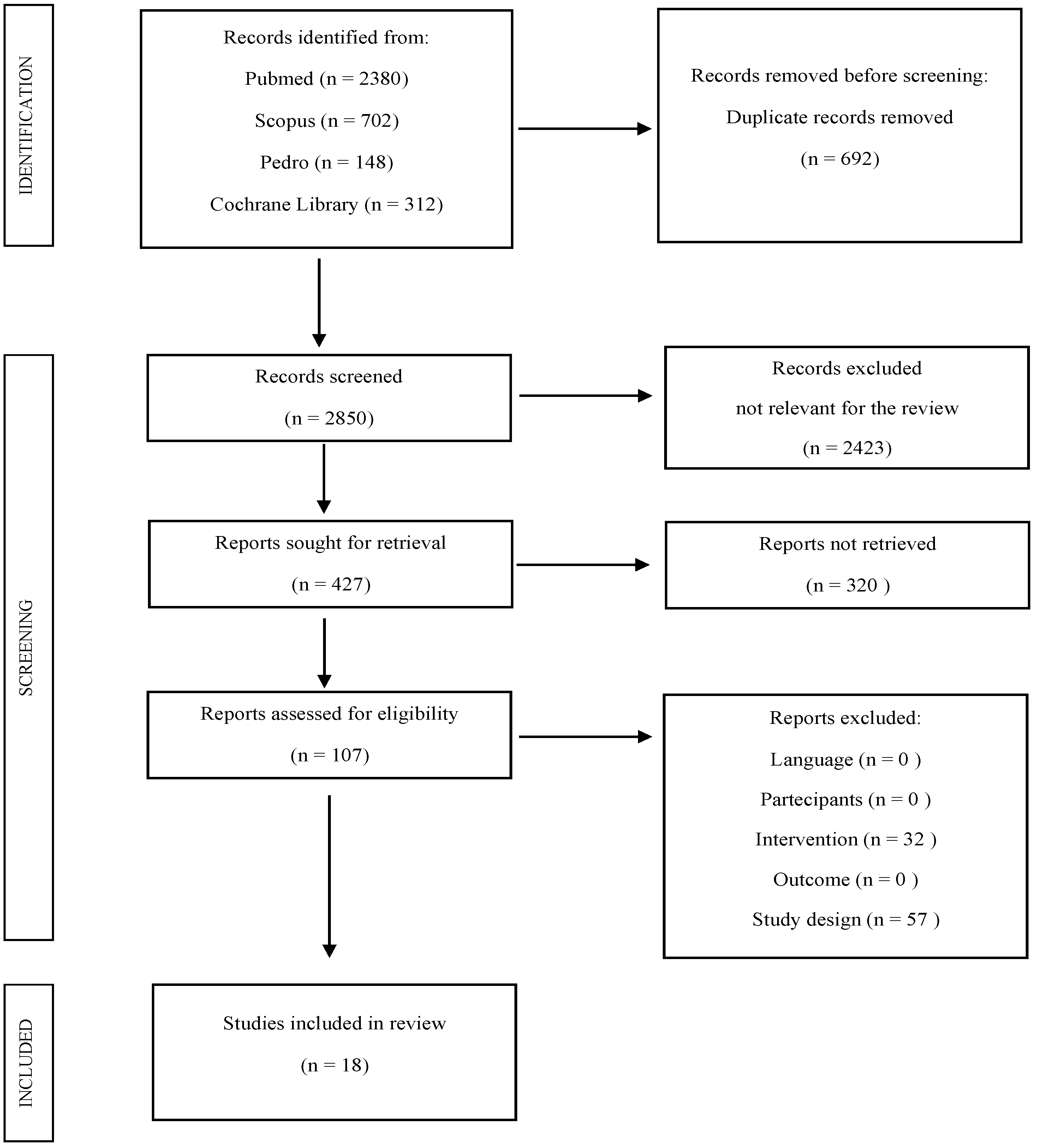
3.1. Selection of Studies
3.2. Evaluation of the Methodologic Quality
3.3. Features of Studies
3.4. Population
3.5. Intervention
3.6. Comparison
3.7. Outcome
3.8. Summary of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Medline: Scopus and Cochrane Library | (Pulmonary rehabilitation OR post-acute) AND COVID-19. |
| Pedro | (Pulmonary rehabilitation OR post-acute) AND COVID-19; Pulmonary rehabilitation AND COVID, COVID-19 AND Rehabilitation, COVID-19 AND Physiotherapy, SARS-CoV-2 AND Rehabilitation, SARS-CoV-2 AND Physiotherapy, COVID-19, SARS-CoV-2. |
References
- OMS Dashboard Updated to 2/12/2022. Available online: https://covid19.who.int/ (accessed on 2 December 2022).
- National Institutes of Health. COVID-19 Treatment Guidelines. Management of Persons with COVID-19. Bethesda, MD NIH. 2020. Available online: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf (accessed on 20 November 2022).
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am. J. Respir. Crit. Care. Med. 1994, 149, 818–824. [Google Scholar] [CrossRef]
- Zhu, J.; Ji, P.; Pang, J.; Zhong, Z.; Li, H.; He, C.; Zhang, J.; Zhao, C. Clinical characteristics of 3062 COVID-19 patients: A meta-analysis. J. Med. Virol. 2020, 92, 1902–1914. [Google Scholar] [CrossRef] [Green Version]
- Spagnolo, P.; Balestro, E.; Aliberti, S.; Cocconcelli, E.; Biondini, D.; Della Casa, G.; Sverzellati, N.; Maher, T.M. Pulmonary fibrosis secondary to COVID-19: A call to arms? Respir. Med Hand. 2020, 8, 750–752. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S. Sindrome post-acuta da COVID-19. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics. The Prevalence of Long COVID Symptoms and COVID-19 Complications. 2020. Available online: https://www.ons.gov.uk/news/statementsandletters/theprevalenceoflongcovidsymptomsandcovid19complications (accessed on 10 November 2022).
- COVID-19 Rapid Guideline: Managing the Longterm Effects of COVID-19 9—NICE, RCGP, and SIGN. 1.20 Published on 3 November 2022. Available online: https://www.nice.org.uk/guidance/ng188/resources/covid19-rapid-guideline-managing-the-longterm-effects-of-covid19-pdf-51035515742 (accessed on 10 November 2022).
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Cattadori, G.; Di Marco, S.; Baravelli, M.; Picozzi, A.; Ambrosio, G. Training exercise in post-COVID-19 patients: The need for a multifactorial protocol for a multifactorial pathophysiology. J. Clin. Med. 2022, 11, 2228. [Google Scholar] [CrossRef]
- Peng, X.L.; Cheng, J.S.; Gong, H.L.; Yuan, M.D.; Zhao, X.H.; Li, Z.; Wei, D.X. Advances in the design and development of SARS-CoV-2 vaccines. Mil. Med. Res. 2021, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D.C. Exercise Is Medicine for Immune Function: Implication for COVID-19. Curr. Sports Med. Rep. 2021, 20, 395–401. [Google Scholar] [CrossRef]
- NICE. Rehabilitation After Critical Illness in Adults. 2009. Available online: https://www.nice.org.uk/guidance/cg83/resources/rehabilitation-after-critical-illness-in-adults-pdf-975687209413 (accessed on 10 November 2022).
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Zhao, H.M.; Xie, Y.X.; Wang, C.; Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Recommendations for respiratory rehabilitation in adults with coronavirus disease 2019. Chin. Med. J. (Engl.) 2020, 133, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S. The Stanford Hall consensus statement for post-COVID-19 rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Capin, J.J.; Jolley, S.E.; Morrow, M.; Connors, M.; Hare, K.; MaWhinney, S.; Nordon-Craft, A.; Rauzi, M.; Flynn, S.; Stevens-Lapsley, J.E.; et al. Safety, feasibility and initial efficacy of an app-facilitated telerehabilitation (AFTER) programme for COVID-19 survivors: A pilot randomised study. BMJ Open 2022, 12, e061285. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xia, W.; Zhan, C.; Liu, S.; Yin, Z.; Wang, J.; Chong, Y.; Zheng, C.; Fang, X.; Cheng, W.; et al. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): A randomised controlled trial. Thorax 2022, 77, 697–706. [Google Scholar] [CrossRef]
- Pehlivan, E.; Palalı, İ.; Atan, S.G.; Turan, D.; Çınarka, H.; Çetinkaya, E. The effectiveness of POST-DISCHARGE telerehabilitation practices in COVID-19 patients: Tele-COVID study-randomized controlled trial. Ann. Thorac. Med. 2022, 17, 110–117. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Al Chikhanie, Y.; Veale, D.; Schoeffler, M.; Pépin, J.L.; Verges, S.; Hérengt, F. Effectiveness of pulmonary rehabilitation in COVID-19 respiratory failure patients post-ICU. Respir. Physiol. Neurobiol. 2021, 287, 103639. [Google Scholar] [CrossRef]
- Büsching, G.; Zhang, Z.; Schmid, J.P.; Sigrist, T.; Khatami, R. Effectiveness of Pulmonary Rehabilitation in Severe and Critically Ill COVID-19 Patients: A Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 8956. [Google Scholar] [CrossRef]
- Curci, C.; Negrini, F.; Ferrillo, M.; Bergonzi, R.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; DEFranceschi, S.; Guarnieri, R.; Moro, P.; et al. Functional outcome after inpatient rehabilitation in postintensive care unit COVID-19 patients: Findings and clinical implications from a real-practice retrospective study. Eur. J. Phys. Rehabil. Med. 2021, 57, 443–450. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Chaplin, E.; Gardiner, N.; Singh, S.J. Early experiences of rehabilitation for individuals post-COVID to improve fatigue, breathlessness exercise capacity and cognition—A cohort study. Chron. Respir. Dis. 2021, 18, 14799731211015691. [Google Scholar] [CrossRef]
- Dun, Y.; Liu, C.; Ripley-Gonzalez, J.W.; Liu, P.; Zhou, N.; Gong, X.; You, B.; Du, Y.; Liu, J.; Li, B.; et al. Six-month outcomes and effect of pulmonary rehabilitation among patients hospitalized with COVID-19: A retrospective cohort study. Ann. Med. 2021, 53, 2099–2109. [Google Scholar] [CrossRef]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of pulmonary rehabilitation in COVID-19: A prospective observational cohort study. ERJ Open Res. 2021, 7, 00108–02021. [Google Scholar] [CrossRef]
- Hameed, F.; Palatulan, E.; Jaywant, A.; Said, R.; Lau, C.; Sood, V.; Layton, A.; Gellhorn, A. Outcomes of a COVID-19 recovery program for patients hospitalized with SARS-CoV-2 infection in New York City: A prospective cohort study. PM R 2021, 13, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.C.; Limbach, M.; Schuler, M.; Merkl, S.; Schwarzl, G.; Jakab, K.; Nowak, D.; Schultz, K. Effectiveness of a Three-Week Inpatient Pulmonary Rehabilitation Program for Patients after COVID-19: A Prospective Observational Study. Int. J. Environ Res. Public Health 2021, 18, 9001. [Google Scholar] [CrossRef]
- Hermann, M.; Pekacka-Egli, A.M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation After COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Puchner, B.; Sahanic, S.; Kirchmair, R.; Pizzini, A.; Sonnweber, B.; Wöll, E.; Mühlbacher, A.; Garimorth, K.; Dareb, B.; Ehling, R.; et al. Beneficial effects of multi-disciplinary rehabilitation in postacute COVID-19: An observational cohort study. Eur. J. Phys. Rehabil. Med. 2021, 57, 189–198. [Google Scholar] [CrossRef]
- Spielmanns, M.; Pekacka-Egli, A.M.; Schoendorf, S.; Windisch, W.; Hermann, M. Effects of a Comprehensive Pulmonary Rehabilitation in Severe Post-COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2695. [Google Scholar] [CrossRef]
- Zampogna, E.; Paneroni, M.; Belli, S.; Aliani, M.; Gandolfo, A.; Visca, D.; Bellanti, M.T.; Ambrosino, N.; Vitacca, M. Pulmonary Rehabilitation in Patients Recovering from COVID-19. Respiration 2021, 100, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Vitacca, M.; Carone, M.; Clini, E.M.; Paneroni, M.; Lazzeri, M.; Lanza, A.; Privitera, E.; Pasqua, F.; Gigliotti, F.; Castellana, G.; et al. Joint Statement on the Role of Respiratory Rehabilitation in the COVID-19 Crisis: The Italian Position Paper. Respiration 2020, 99, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Vitacca, M.; Lazzeri, M.; Guffanti, E.; Frigerio, P.; D’Abrosca, F.; Gianola, S.; Carone, M.; Paneroni, M.; Ceriana, P.; Pasqua, F.; et al. Italian suggestions for pulmonary rehabilitation in COVID-19 patients recovering from acute respiratory failure: Results of a Delphi process. Monaldi. Arch. Chest. Dis. 2020, 90, 385–393. [Google Scholar] [CrossRef]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Tonia, T.; Wilson, K.C.; Troosters, T. COVID-19: Interim Guidance on Rehabilitation in the Hospital and Post-Hospital Phase from a European Respiratory Society and American Thoracic Society-coordinated International Task Force. Eur. Respir. J. 2020, 56, 2002197. [Google Scholar] [CrossRef] [PubMed]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Navarro-Cruz, R.; Alfaro-Acha, A.; Ara, I.; García-García, F.J.; Alegre, L.M.; Guadalupe-Grau, A. Effects of concurrent exercise training on muscle dysfunction and systemic oxidative stress in older people with COPD. Scand. J. Med. Sci. Sports 2019, 29, 1591–1603. [Google Scholar] [CrossRef] [PubMed]
- Official Recommendations of the American Thoracic Society and European Respiratory Society: Implementation, Use, and Dissemination of Respiratory Rehabilitation. Available online: https://www.ers-education.org/lrMedia/2015/pdf/393777.pdf (accessed on 20 October 2022).

| P (population) | Patients diagnosed with COVID-19 in the post-acute phase and clinically stable. Severe COVID-19 cases or acute-phase cases with clinical instability were excluded. |
| I (intervention) | Physiotherapeutic respiratory intervention in its different means, either delivered in conventional form (in person) or through telemedicine. |
| C (comparison) | Patients who only receive standard assistance/cure or receive no cure whatsoever. |
| O (outcome) | Improvement of the respiratory function and physical performance, reduction in dyspnea and fatigue and improvement of autonomy and quality of life in patients affected by COVID-19. |
| Autor | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Capin 2022 [18] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Li 2021 [19] | Y | Y | Y | Y | N | N | Y | Y | N | Y | Y | 6 |
| Liu 2020 [21] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Pehlivan 2022 [20] | Y | Y | Y | Y | N | N | N | N | N | Y | Y | 6 |
| Autor | Quality of Selected Cohort | Cohort Comparability | Results Obtained | Score |
|---|---|---|---|---|
| Al Chikhanie 2021 [22] | ♦♦♦♦ | ♦ | ♦ | 6/9 |
| Daynes 2021 [25] | ♦♦♦ | ♦♦ | 5/9 | |
| Dun 2021[26] | ♦♦♦♦ | ♦ | ♦♦ | 7/9 |
| Gloeckl 2021 [27] | ♦♦♦ | ♦ | ♦♦ | 6/9 |
| Hameed 2021 [28] | ♦♦♦♦ | ♦ | ♦♦ | 7/9 |
| Hayden 2021 [29] | ♦♦♦ | ♦ | ♦ | 5/9 |
| Hermann 2020 [30] | ♦♦♦ | ♦ | ♦ | 5/9 |
| Puchner 2021 [31] | ♦♦♦ | ♦ | 4/9 | |
| Spielmanns 2021 [32] | ♦♦♦ | ♦ | ♦ | 5/9 |
| Autor | Selection | Comparability | Exposure | Score |
|---|---|---|---|---|
| Busching 2021 [23] | ♦♦♦ | ♦ | ♦♦ | 6/9 |
| Curci 2021 [24] | ♦♦ | ♦ | 3/9 | |
| Zampogna 2021 [33] | ♦♦ | ♦ | 3/9 |
| Author Year Title | Study Design | Rehabilitation Protocol | Intervention Frequency | Participants | Outcome Measures | Evaluation Time | Results |
|---|---|---|---|---|---|---|---|
| Al Chikhanie et al., 2021 [22] | Cohort study | EG and CG: breathing exercises, muscle strengthening, balance and walking when possible, cycling and gymnastics according to current ATS/ERS recommendations | EG: 27.6 ± 14.2 days CG: 29.9 ± 17.3 days | EG: (n.21) -Mean age: 70.9 ± 10.6 -Gender: 14M/7F CG: (n.21) -Mean age: 69.1 ± 9.4 -Gender: 13M/8F | Primary: FEV1; CVF: PImax; PEmax; 6MWT; Tinetti Scale; Borg test; Muscle strength; St George Questionnaire: Quality of Life (QoL); Pichot’s questionnaire; HADS; PCLS Secondary: N/A | At baseline and at the end of the PR program. 6MWT, also performed weekly during PR. | Extensive and rapid recovery of exercise capacity among COVID-19 patients rehabilitated after admission to intensive care, as well as extensive improvements in muscle strength, balance and psychosocial status. Significant improvement in 6MWT, greater in COVID-19 patients (+205 ± 121 m) compared to non-COVID-19 patients (+93 ± 66 m). |
| Busching et al., 2021 [23] | Retrospective observational study | EG and GC: cardiopulmonary training (cycling, guided walking), strength exercise (free weight, resistance bands), breathing exercises (deep breathing, sputum evacuation), relaxation techniques (progressive muscle relaxation), if indicated psychological, nutritional, speech therapy and occupational therapy. | A minimum of 540 min of patient education and therapy in individual and group settings. | EG: (n.51) -Mean age: 65.8 ± 11.7 -Gender: 38M/13F CG: (n.51) -Mean age: 69.8 ± 9.6, -Gender: 23M/28F | Primary: 6 MWT; FIM: Functional Independence Measure; CRQ: chronic respiratory questionnaire Secondary: N/A | At baseline and at the end of the PR program | Both groups achieved significant improvements in 6MWT, CRQ and FIM. At discharge, COVID-19 patients performed better in 6MWT and FIM, but similar CRQ scores compared to the control group. Regression analysis of the 2 subgroups: COVID-19 intensive care versus non-ICU subgroup: no significant difference in 6MWT at discharge. The outcome of physical functioning in the PR program is similar among critical and severe COVID-19 patients. |
| Capin et al., 2022 [18] | RCT | EG: breathing and compensation techniques, high-intensity strength training, aerobic and cardiovascular exercises, balance exercises, functional activities, stretching and lifestyle coaching and motivational interviewing. The Health in Motion application used to facilitate self-directed intervention outside of supervised sessions. CG: exercise education with educational handout and weekly check-in phone calls. | 12 individual and supervised telerehabilitation sessions provided: 3 times a week in the first week, 2 times a week in weeks 2–4 once a week in weeks 5–6 and 1 single “recall” visit session during week 9 or 10. | EG: (n.29) CG: (n.15) -Mean age: 52 aa -Gender: 23M/21F | Primary: Feasibility through safety and adherence (percentage of sessions attended). Secondary: TUG; MRC; ABC; PROMIS-SF; PHQ8; MoCA | At baseline, 6 weeks after baseline and 12 weeks after baseline (week 12). | The informed multi-component and biobehavioral telerehabilitation program for COVID-19 survivors is safe and feasible. Participants in both groups functionally improved from baseline to 6 weeks and 12 weeks after intervention. |
| Curci et al., 2021 [24] | Retrospective observational study | EG: Initially: posture changes, passive mobilization, postural drainage, chest clapping and vibration, breathing control exercises and chest-abdomen coordination. Muscle strengthening exercises of the upper and lower limbs, trunk and gluteal muscles. Breathing exercises with the pep bottle, forced inhalation/exhalation and use of the incentive spirometer. Balance and coordination exercises and train yourself to walk for progressive distances. CG: N/A | 30 min/set, 2 times a day for the duration of hospitalization. (LOS average in the COVID-19 Rehabilitation Unit was 31.97 ± 9.06 days). | EG: (n.41) -Mean age 72.15 ± 11.07 aa -Gender: 25M/16F CG: N/A | Primary: BI Secondary: MRC; 6-MWT; RPE; Type of respiratory support required; Results of arterial blood gas analysis; Serum levels of laboratory markers. | At hospitalization (T0) and at the end of the PR program (T1). | Statistically significant improvement in the Barthel Index (BI) (84.87 ± 15.56 vs. 43.37 ± 26.00), 6-MWT (303.37 ± 112.18 vs. 240.0 ± 81.31 m) and Borg RPE scale (12.23 ± 2.51 vs. 16.03 ± 2.28). Finally, an improvement also in CT scans in 74.4% of cases |
| Daynes et al., 2021 [25] | Cohort study | EG: Aerobic exercises based on walking/treadmill, upper and lower limb strength training. Educational sessions with handouts included: dyspnea, cough, fatigue, fear and anxiety, memory and concentration, managing daily activities and returning to work. CG: N/A | 2 sessions per week for 6 weeks. | EG: (n.32) -Mean age: 58 aa -Gender: 52%M/48%F CG: N/A | Primary: Incremental running and resistance test (ISWT/ESWT); CAT; FACIT; HADS; EQ5D; MoCA. Secondary: N/A | At baseline and at the end of the PR program | PR produced average improvement within the group of 112 m in the Incremental Shuttle Walking Test (ISWT) and 544 s in the Endurance Shuttle Walking Test (ESWT). The FACIT improved by 5 points, the EQ5D improved by 8 points and the MoCA by 2 points. The CAT score improved by 3 points, while for Anxiety and depression: minimal improvement, equal to 1 point. |
| Dun et al., 2021 [26] | Retrospective cohort studies | EG: inspiratory muscle training; 30 sets of ruffled lip breathing techniques and active breathing cycle (ACBT); a series of 30 repetitions of maximum voluntary diaphragmatic contractions in the supine position, placing an average weight (1–3 kg) on the anterior abdominal wall to resist diaphragmatic descent; two high-intensity interval workouts of 4 min via bike or treadmill interspersed with 4 min low-intensity intervals. CG: patients that did not perform any PR during the 6 m of convalescence. | 3 sessions per week for 12 weeks. | EG (n.27) -Mean age: 54 ± 16 -Gender: 9M/18FCG (n.71) -Mean age: 44 ± 13 -Gender: 36M/35F | Primary: 6-MWT Secondary: -Changes in SARS-CoV-2 specific IgG and IgM immunoglobulins, T lymphocytes and blood chemistry | Baseline, 2 weeks and 6 months. | Patients in the PR group acquired a greater increase in the distance traveled in 6-MWT compared to the control. There were no significant differences between PR and control groups in IgG and IgM specific for SARS-CoV-2, CD3+ T cells, CD8+ cells, CD8+ T cells, CD4+/CD8+ ratio, and all biomarkers. |
| Gloeckl et al., 2021 [27] | Prospective and observational cohort study | EG1 (COVID-19 mild/moderate) and EG2 (COVID-19 severe/critical): Pulmonary rehabilitation program for COVID-19 patients includes resistance training, strength training, patient education sessions, respiratory physiotherapy, daily life training activities and relaxation techniques. CG: N/A | 3 weeks | EG1 (COVID-19 mild/moderate) (n.24) -Mean age: 52 -Gender: 4M/20F EG2 (COVID-19-severe/critical) (n.26) -Mean age: 66 -Gender: 18M/8F CG: N/A | Primary: 6MWT. Secondary: -Complete effort test (only in the subgroup of patients with severe/critical COVID-19); Shuttle walking test (ESWT); Maximum isometric knee extension force (MicroFET 2 dynamometer) and grip force (Jamar manual dynamometer) evaluated by dynamometry; Test sit-to-stand; FVC; FEV 1), TLC; DLCO; MRC; SF-36; GAD-7; PHQ-9 | At baseline and at the end of the PR program | Measures of FVC or FEV1 lung function improved significantly in the range of 7.7–15.7% in both groups. Quality of life improved significantly only in patients with severe/critical COVID-19 in the SF-36 mental sum score (38.5 to 52.9 points; p < 0.001). |
| Hameed et al., 2021 [28] | Prospective cohort study | EG1 (MTM): virtual physical therapy via a telemedicine platform. EG2 (HPT): Home Physical Therapy EG3 (IE): independent exercise program CG: No therapy. | 1–2 times a week with sessions of 30–60 min. | EG1 (VPT) (n.44) -Mean age: 60 -Gender: 53%M/57%F EG2 (HPT) (n.25) -Mean age: 57 -Gender: 86%M/24%F EG3 (IE) (n.17) -Mean age: 59 -Gender: 65%M/35%F CG (n.20) -Mean age: 58 -Gender: 55%M/55%F | Primary: Change in lower limb strength; sit-to-stand test; 2MWT. Secondary: N/A | At baseline and 2-week follow-up. | At follow-up, 65% of patients in the VPT group and 88% of patients in the HPT group achieved clinically significant difference for improvement in sit-to-stand scores, compared with 50% and 17% of those in the IE group and the non-exercise group (p = 0.056). The clinically significant difference for step test improvement was met by 74% of patients in the VPT group and 50% of patients in the HPT, IE and non-exercise groups (p = 0.12). |
| Hayden et al., 2021 [29] | Prospective observational study | EG1 (Severe Acute COVID-19); EG2 (Severe COVID-19); EG3 (Mild COVID-19): the program has been adapted to individual needs. Physical training with resistance and strength training, vibratory training for the whole body and inspiratory muscle training. Respiratory physiotherapy with individual training on breathing, seminar on coughing techniques and mucolytic inhalation therapies. General physiotherapy with mobility and gait training. Psychosocial support, nutritional counselling and occupational therapy. CG: N/A | 3 weeks Average duration of PR treatment: 26.3 ± 5.9 days | EG1 (Severe Acute) (n.55) -Mean age: 57.9 ± 10.8 -Gender: 34M/21F EG2 (Severe) (n.32) -Mean age: 54.0 ± 9.9 -Gender: 21M/11F EG3 (Mild) (n.21) -Mean age: 52.1 ± 6.8 -Gender: 4M/17F CG: N/A | Primary: NRS; MRC Secondary:Cardinal symptom: list of symptoms associated with COVID-19; 6MWT, FEV1, vital capacity (CV), residual volume (VR), total lung capacity (TLC), total specific airway resistance (sRtot), maximum inspiratory pressure (PImax) and capillary carbon monoxide alveolus diffusion (TLCO) Blood gas analysis, Laboratory blood test, NRS, BFI, EQ-5D-5L, PHQ-9, GAD-7, GROC, Estimation of the overall effectiveness of rehabilitation from the point of view of the patient: 11-point Likert scale | At baseline and at the end of the PR program. | PR was effective after acute COVID-19 in all three groups analyzed. 6MWT improved with large effect sizes in all groups, with major changes in subgroups 1 and 2. Groups 1 and 2 showed statistically significant improvements with moderate to high effect sizes in VC%, TLC%, FEV1%, TLCO_SB% and PImax. Significant decrease in fatigue was observed in groups 1 and 2, with large effect sizes. Anxiety values decreased, with moderate to high effect sizes. All groups showed significant improvement with high effect sizes in QoL. |
| Hermann et al., 2020 [30] | Cohort study | EG1 (ventilated), EG2 (unventilated): individualized training including aerobic exercise and strength training. Respiratory physiotherapy consisted of teaching breath control (breathing of ruffled lips, mobilization of secretions and diaphragmatic breathing), energy-saving techniques and controlled cough exercises. Twice a week (1 h each), all patients participated in educational sessions. CG: N/A | 2–4 weeks with 25–30 therapy sessions, which took place on 5–6 days a week. | EG1 (ventilated) (n. 12) -Mean age: 64.3 -Gender: 9M/12F EG2 (not ventilated) (n. 16) -Mean age: 67.4 -Gender: 5M/16F CG: N/A | Primary: 6-MWT, CRQ, FIM, CIRS, HADS -Patients’ feelings about their actual well-being: Sensitive thermometer (FT) -Lung function, blood gas analysis and oxygen therapy Secondary: N/A | At baseline and at the end of the PR program. | Significant improvements were observed in 6-MWT (+130 m) and FT (+40 points) for the total cohort with no significant differences in intergroup comparison, between ventilated and unventilated patients. Pulmonary function tests showed persistent obstructed ventilation only in a few cases, however, still a part of the patients had limited ventilation and reduced diffusion capacity with the following results: mean FEV1 56%, mean FEV1% FVC 81%, mean TLC 62%, DLCO 56%. |
| Li et al., 2021 [19] | RCT | EG: via a smartphone application called RehabApp: breathing control and chest expansion, aerobic exercise and LMS exercises specified in a three-level exercise plan with difficulty and intensity programmed to increase over time. CG: Brief Educational Instructions | 3–4 sessions per week for 6 weeks. | EG (TERECO) (n. 59) -Mean age: 49.17 -Gender: 26M/34F CG (n.61) -Mean age: 52.03 -Gender: 27M/32F | Primary: 6MWT Secondary: -Squat time in seconds to evaluate the muscle strength of the lower limbs; -Lung function: spirometry, SF-12, mMRC | At baseline, at 6 weeks (post-treatment) and at 28 weeks (follow-up). | The 6MWT in the TERECO group improved by 80.2 m in the after-treatment period, while in the control group there was a small improvement of 17.1 m. Lower limb muscle strength (SML) improved to a greater extent in the TERECO group, treatment effects were 20.12 sec post-treatment and 22.23 sec at follow-up. Lung function parameters improved in both groups, except for maximal voluntary ventilation (MVV) which improved post-treatment most in the TERECO group. The increase in the physical component of SF-12 was greater in the TERECO group with treatment effects estimated at 3.79 post-treatment and 2.69 following. |
| Liu et al., 2021 [21] | RCT | EG: training of respiratory muscles; exercise for cough; diaphragmatic training; stretching exercise; and exercise at home (ruffled lip breathing and cough training: 30 sets per day). Exercises for upper limb in flexion, horizontal extension, abduction and external rotation. CG: no treatment | 2 sessions per week for 6 weeks. | EG (n. 36) -Mean age: 69.4 -Gender: 24M/12F CG (n.36) -Mean age: 68.9 -Gender: 25M/11F | Primary: Respiratory function: forced expiratory volume in 1st second forced expiratory volume(FEV1); Forced vital capacity (CVF); capillary alveolus diffusion of carbon monoxide DLCO (%) Secondary:6MWT, FIM, SF-36, SDS, SAS | At baseline and at the end of the PR program. | In the intervention group, significant differences were found in FEV1(L), FVC(L), FEV1/FVC%, DLCO% and 6MWT. SF-36 scores, in 8 dimensions, were statistically significant within the intervention group and between the two groups. SAS and SDS scores in the intervention group decreased after the intervention, but only anxiety had a significant outcome within and between the two groups. |
| Pehlivan et al., 2022 [20] | RCT | EG (TeleGr): patient education, rhythm running/autonomous walking in the corridor, breathing exercises, active cycle of breathing techniques, range of motion exercises and standing squats. The exercises were performed 10 times per session. The number of repetitions has been adjusted according to the fatigue rate. CG: exercise brochures with the same content (patient education, breathing exercises, movement exercises, self-walking and squats) | 3 days a week for 6 weeks. | EG (TeleGr): (n.34) -Mean age: 50.76 -Gender: 14M/3F CG: (n.34) -Mean age: 43.24 -Gender: 6M/11F | Primary: MRC; VAS, TUG, Short Battery for Physical Performance (SPPB) includes three tasks: a standing balance test (side-by-side, semi-tandem and tandem), a usual gait speed of 4 m and sitting and getting up 5v from a chairSt. George’s breathing questionnaire, BDI Secondary: N/A | At baseline and at the end of the PR program. | Significant improvement in EG (TelerGr) in terms of mMRC (p = 0.035), 30STS (p = 0.005), 5 sitting to standing time, which is one of the subtests of SPPB (p = 0.039) and SGRQ scores. A significant improvement was observed only in the pain score in the CG (p = 0.039). Statistically significant difference between groups in SGRQ (p = 0.035) and total (p = 0.042) scores. In addition, a more symptomatic improvement was found in TeleGr. |
| Puchner et al., 2021 [31] | Observational cohort study | EG: Respiratory therapy; Training of respiratory muscles; Mobilization and perception of breath; Endurance and strength training; Speech therapy intervention and swallowing evaluation; Occupational therapy, psychological therapy. CG: N/A | 25–50 min sessions for 3 weeks. | EG (n.23) -Mean age: 57 ± 10 -Gender: 16M/7F CG: N/A | Primary:Respiratory function by spirometry: forced vital capacity (FVC), forced vital capacity in one second (FEV1), FEV1/FVC, total lung capacity (TLC), residual volume (RL) and diffusion capacity for carbon monoxide (DLCO) and blood gas analysis pH, pO2 and pCO2, MIP, 6MWT, BI | At baseline and at the end of the PR program. | Significant improvement in lung function: increased forced vital capacity (FVC), forced expiratory volume in one second (FEV1), total lung capacity (TLC) and carbon monoxide diffusion capacity (DLCO). The state of physical performance has improved: average increase of 176 m in 6MWT and significant improvement in the Barthel Index (BI). Lung function is still impaired in 57% of all patients, and 83% of all study participants still had DLCO reduction at the end of the rehabilitation program. |
| Spielmanns et al., 2021 [32] | Prospective observational study | EG and CG: resistance training (cycling and treadmill), 3-level gymnastics, 3-level indoor and outdoor walking and strength training; Respiratory physiotherapy: breathing with wrinkled lips, mobilization of secretions and diaphragmatic breathing), energy-saving techniques and controlled cough exercises; Twice a week (1 h each): educational sessions (self-management, coping skills, self-medication, infection and exacerbation management, dyspnea, oxygen use and nutritional interventions). | 25–30 therapy sessions in 5–6 weekdays for 3 weeks. | EG (n.99) -Mean age: 67.72 -Gender: 57M/42F CG: (n.419) -Mean age: 69.28 -Gender: 206M/213F | Primary: 6MWT, Pulmonary function test: spirometry and plethysmography and blood gas analysis,CRQ, FIM, HADS, CIRS -Wellness: Sensitive thermometer (FT) Secondary: N/A | At baseline and at the end of the PR program. | Improvements in 6-MWT in pre-post comparison averaged 180 (±101) meters for EG and 102 (±89) meters for CG (p < 0.001). FT showed a significant improvement for post-COVID-19 patients (PG) of 21 (±14) points and for patients with other lung disease (LG) of 17 (±16) points (p < 0.039), while FIM increased significantly by 11 (±10) points in post-COVID-19 patients (PG) and 7 (±8) points in patients with other lung disease (LG) (p < 0.001). |
| Vitacca et al., 2020 [34] | Practical guideline | / | / | / | / | / | / |
| Vitacca et al., 2020 [35] | Declaration of consent | / | / | / | / | / | / |
| Zampogna et al., 2021 [33] | Multicenter retrospective observational study | EG: Level A: SPPB < 6 with a 1:1 physiotherapist/patient ratio with mobilization, active exercises and free walking, peripheral limb muscles, shoulders and upper limb activity. Level B: SPPB ≥ 6 with a 1:4–5 physiotherapist/patient ratio with gymnastics, strengthening, balance exercise, rhythmic walking, and thoracic physiotherapy with bronchial hygiene techniques and lung expansion procedures. CG: N/A | From a minimum of 1 session a day of 20 min up to 2–3 sessions of 30 min a day. | EG (n.140) -Mean age: 71.0 -Gender: 95M/45F CG: N/A | Primary: -Exercise tolerance: 6 Minutes Walking Test (6MWT); -Function of the lower limbs: Short Physical Performance Battery (SPPB); -Motor performance: the Barthel Index (BI). Secondary: N/A | At baseline and at the end of the PR program | Improvements in lower limb function in SPPB and motor performance in BI with scores ranging from 55 to 95. 81 patients after rehabilitation treatment were able to complete the 6 MWT with an average distance of 285 m. The percentage of patients who at the time of admission were unable to stand, get up from a chair and walk after rehabilitation is significantly reduced. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamburlani, M.; Cuscito, R.; Servadio, A.; Galeoto, G. Effectiveness of Respiratory Rehabilitation in COVID-19’s Post-Acute Phase: A Systematic Review. Healthcare 2023, 11, 1071. https://doi.org/10.3390/healthcare11081071
Tamburlani M, Cuscito R, Servadio A, Galeoto G. Effectiveness of Respiratory Rehabilitation in COVID-19’s Post-Acute Phase: A Systematic Review. Healthcare. 2023; 11(8):1071. https://doi.org/10.3390/healthcare11081071
Chicago/Turabian StyleTamburlani, Matteo, Rossana Cuscito, Annamaria Servadio, and Giovanni Galeoto. 2023. "Effectiveness of Respiratory Rehabilitation in COVID-19’s Post-Acute Phase: A Systematic Review" Healthcare 11, no. 8: 1071. https://doi.org/10.3390/healthcare11081071
APA StyleTamburlani, M., Cuscito, R., Servadio, A., & Galeoto, G. (2023). Effectiveness of Respiratory Rehabilitation in COVID-19’s Post-Acute Phase: A Systematic Review. Healthcare, 11(8), 1071. https://doi.org/10.3390/healthcare11081071