
Assessing the Reliability and Validity of the Spanish Version of the Actual Scope of Nursing Practice Scale

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Phase 1. Traslation and Cultural Adaptation of the Instrument
2.2. Phase 2. Analysis of the Psychometric Characteristics of the Instrument
2.2.1. Participants
2.2.2. Data Collection
2.2.3. Data Analysis
2.2.4. Validity
2.2.5. Ethical Issues/Statement
3. Results
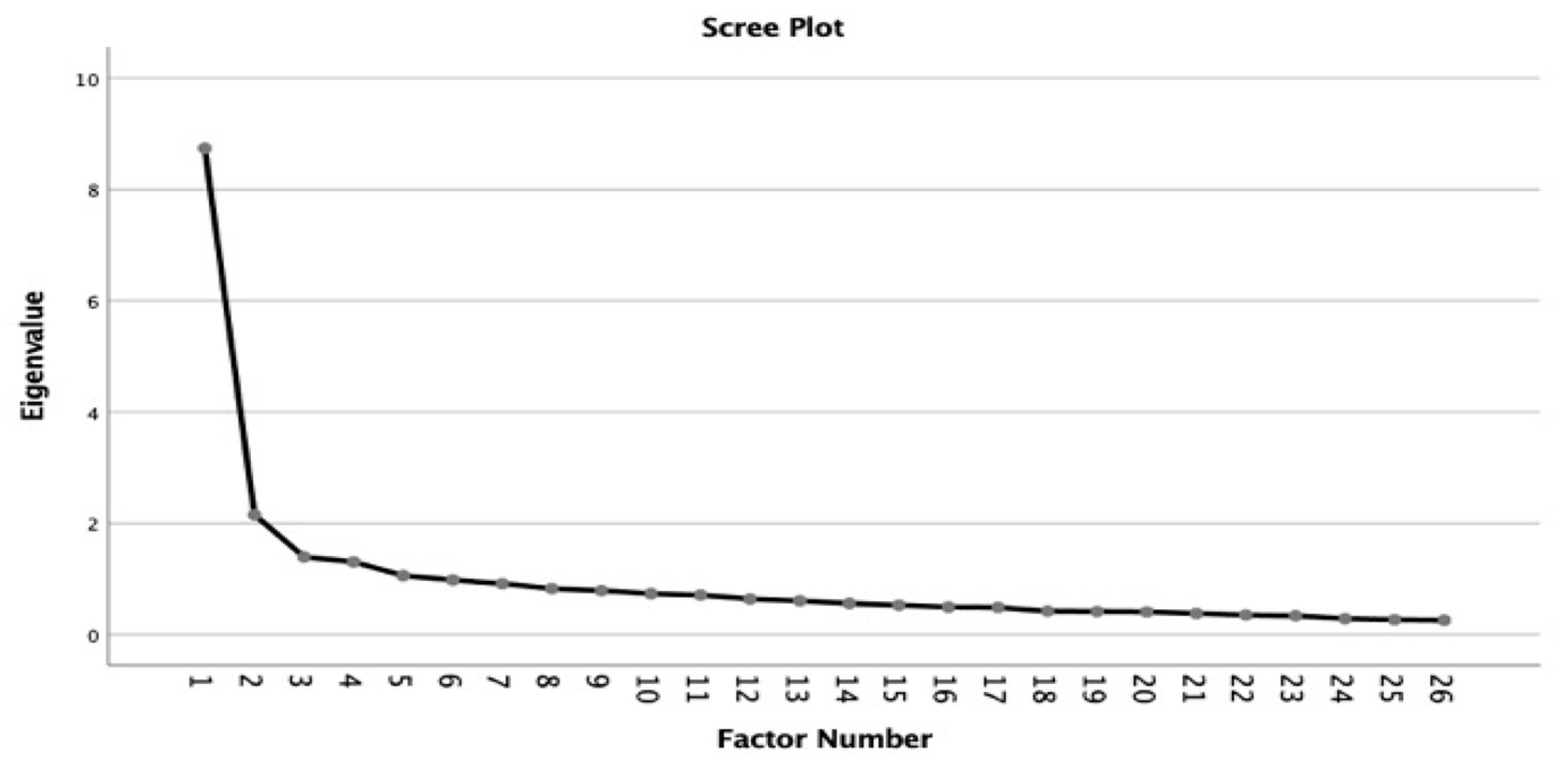
3.1. Exploratory Factor Analysis
3.2. Confirmatory Factor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Instrucciones: Indique para cada enunciado la respuesta que mejor corresponda a su práctica diaria en su puesto de trabajo. Seleccione la frecuencia con la que realiza estas actividades: . 1. Nunca . 2. Muy raramente . 3. A veces . 4. Frecuentemente . 5. Casi a diario . 6. Siempre | ||||||
| Ítems | 1 | 2 | 3 | 4 | 5 | 6 |
| Participo en el desarrollo de la práctica enfermera. (ej. Revisión de protocolos de cuidados, proyectos diversos…) | ||||||
| Mantengo al día mis conocimientos. (lectura de artículos científicos, etc.) | ||||||
| Utilizo estrategias didácticas que se adaptan a cada paciente y a sus familiares según el nivel de autonomía del paciente. | ||||||
| Ejerzo de mentora o formadora del personal de reciente incorporación. | ||||||
| Notifico las situaciones clínicas en las que considero que existen deficiencias respecto a la calidad y a la seguridad de los cuidados. | ||||||
| Participo en reuniones y actividades del equipo interdisciplinar | ||||||
| Participo en la orientación y la formación de estudiantes de enfermería o del personal de reciente incorporación | ||||||
| Participo en la creación, la aplicación y la actualización de distintos planes y protocolos de atención a los pacientes (por ejemplo: Planes de cuidados estandarizados, informes de enfermería al alta, etc.) | ||||||
| Cuando se realiza la modificación de una práctica, comparto con el equipo de enfermería la evidencia derivada de los estudios de investigación. | ||||||
| Participo en el desarrollo y realización de actividades formativas del equipo de cuidados en función de mi capacidad. | ||||||
| Para asegurar la continuidad de los cuidados, coordino las intervenciones del equipo interprofesional en el hospital (médicos, fisioterapeutas, etc.) | ||||||
| Comunico a los miembros del equipo toda la información que podría afectar a la coordinación de la atención. | ||||||
| Verifico que el paciente y sus familiares han comprendido las indicaciones que se les han facilitado. | ||||||
| Mejoro mi práctica basándome en nuevos conocimientos derivados de las “buenas prácticas” e investigaciones en enfermería y otras ciencias de la salud. | ||||||
| Participo en la identificación de las necesidades de formación continua de mi unidad. | ||||||
| Actualizo con regularidad, por escrito, la información sobre el estado del paciente y los cuidados que se le proporcionan (el plan de cuidados, las anotaciones de las enfermeras, etc.). | ||||||
| Compruebo la calidad de la información facilitada al paciente en la unidad. | ||||||
| Transmito toda la información relevante a los profesionales sanitarios de otras instituciones para asegurarme de la continuidad de los cuidados. | ||||||
| Evalúo el estado físico y mental del paciente teniendo en cuenta los aspectos biopsicosociales. | ||||||
| Participo en la actualización de las prácticas para mejorar la calidad y la seguridad de los cuidados. | ||||||
References
- Gazar, H.E.; Zoromba, M.A. Nursing Human Resource Practices and Hospitals’ Performance Excellence: The Mediating Role of Nurses’ Performance. Acta Biomed. 2021, 92, e2021022. [Google Scholar] [CrossRef]
- White, K.; Macfarlane, H.; Hoffmann, B.; Sirvas-Brown, H.; Hines, K.; Rolley, J.X.; Graham, S. Consensus Statement of Standards for Interventional Cardiovascular Nursing Practice. Heart Lung. Circ. 2017, 27, 535–551. [Google Scholar] [CrossRef]
- Camelo, S. Legal politics of human resources: National Health System, legal bases, and implications for nursing. R. Enferm. UERJ 2009, 17, 589–594. [Google Scholar]
- Michel, O.; Garcia Manjon, A.J.; Pasquier, J.; Ortoleva Bucher, C. How do nurses spend their time? A time and motion analysis of nursing activities in an internal medicine unit. J. Adv. Nurs. 2021, 77, 4459–4470. [Google Scholar] [CrossRef] [PubMed]
- D’Amour, D.; Dubois, C.A.; Déry, J.; Clarke, S.; Tchouaket, É.; Blais, R.; Rivard, M. Measuring Actual Scope of Nursing Practice. J. Nurs. Adm. 2012, 42, 248–255. [Google Scholar] [CrossRef]
- Aljohani, K.A.; Alamri, M.S.; Al-Dossary, R.; Albaqawi, H.; Hosis, K.A.; Aljohani, M.S.; Almadani, N.; Alrasheadi, B.; Falatah, R.; Almazan, J.; et al. Scope of Nursing Practice as Perceived by Nurses Working in Saudi Arabia. Int. J. Environ. Res. Public. Health 2022, 19, 4220. [Google Scholar] [CrossRef] [PubMed]
- Highfield, M.E.F.; Collier, A.; Collins, M.; Crowley, R.M. Partnering to Promote Evidence-Based Implications for Nursing Professional Development Specialists. J. Nurses Prof. Dev. 2016, 32, 130–136. [Google Scholar] [CrossRef]
- Brunt, B.A.; Morris, M.M. Nursing Professional Development. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- White, K.A.; Davis, D.; Maughan, E.D. Development and validation of an instrument to measure scope of practice in school nurses. J. Adv. Nurs. 2021, 77, 3226–3237. [Google Scholar] [CrossRef]
- Ganz, F.D.; Toren, O.; Fadlon, Y. Factors Associated with Full Implementation of Scope of Practice. J. Nurs. Scholarsh. 2016, 48, 285–293. [Google Scholar] [CrossRef]
- Birks, M.; Smithson, J.; Lindsay, D.; Davis, J. How registered nurses determine their scope of practice: A cross-sectional study. Contemp. Nurse 2018, 54, 578–591. [Google Scholar] [CrossRef]
- Younan, L.; Clinton, M.; Fares, S.; Samaha, H. The translation and cultural adaptation validity of the Actual Scope of Practice Questionnaire. East. Mediterr. Health J. 2019, 25, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Clinton, M.; Younan, L. The first Arabic version of the Actual Scope of Nursing Practice Scale: Psychometric evaluation. J. Nurs. Manag. 2018, 26, 1059–1065. [Google Scholar] [CrossRef]
- Dery, J. The Actual Extent of the Practice of Nurses in Pediatrics: Its Determinants and Influence on Job. Satisfaction Thesis, University of Montreal, Montréal, QC, Canada, 2013. Available online: https://www.proquest.com/dissertations-theses/actual-extent-practice-nurses-pediatrics/docview/1692288327/se-2 (accessed on 15 December 2021). (Original Work Published in Spanish).
- Mason, T.C. Cross-cultural instrument translation: Assessment, translation, and statistical applications. Am. Ann. Deaf. 2005, 150, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Brislin, R.W. Back-Translation for Cross-Cultural Research. J. Cross Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Sperber, A.D. Translation and Validation of Study Instruments for Cross-Cultural Research. Gastroenterology 2004, 126, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Lloret-Segura, S.; Ferreres-Traver, A.; Tomás-Marco, A.H.I. Exploratory Item Factor Analysis: A practical guide revised and updated. An. De Psicol. 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research, 2nd ed.; The Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Liu, Y.; Millsap, R.E.; West, S.G.; Tein, J.-Y.; Tanaka, R.; Grimm, K.J. Testing measurement invariance in longitudinal data with ordered-categorical measures. Psychol. Methods 2017, 22, 486–506. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory, 2nd ed.; McGraw-Hill: Nueva York, NY, USA, 1978. [Google Scholar]
- Ebel, R.L.; Frisbie, D.A. Essentials of Educational Measurement, 5th ed.; Prentice-Hall: Englewood Cliffs, NJ, USA, 1991. [Google Scholar]
- Campos, M.S.; Oliveira, B.A.; Perroca, M.G. Workload of nurses: Observational study of indirect care activities/interventions. Rev. Bras. Enferm. 2018, 71, 297–305. [Google Scholar] [CrossRef]
- Van den Oetelaar, W.F.J.M.; Van Stel, H.F.; Van Rhenen, W.; Stellato, R.K.; Grolman, W. Mapping nurses’ activities in surgical hospital wards: A time study. PLoS ONE 2018, 13, e0191807. [Google Scholar] [CrossRef]
- Butcher, H.K.; Bullechek, G.M.; Dochterman, J.M.; Wagner, C. Nursing Intervention Classification (NIC), 7th ed.; Mosby: St. Louis, MI, USA, 2018. [Google Scholar]
- Dallaire, C.; Dallaire, M. Nursing knowledge in nursing functions. In Nursing Knowledge at the Heart of the Discipline and the Profession; Editor, Gaetan Morin: Quebec, Canada, 2008; pp. 265–312, (Original Work Published in Spanish). [Google Scholar]
- O’Rourke, M.W. Rebuilding a professional practice model. The return of role-based practice accountability. Nurs. Adm. Quart. 2003, 27, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Scott, P.; Harvey, C.; Felzmann, H.; Suhonen, R.; Habermann, M.; Halvorsen, K.; Christiansen, K.; Toffoli, L.; Papastavrou, E. Resource allocation and rationing in nursing care: A discussion paper. Nurs. Ethics 2018, 26, 1528–1539. [Google Scholar] [CrossRef] [PubMed]
- Suhonen, R.; Stolt, M.; Habermann, M.; Hjaltadottir, I.; Vryonides, S.; Tonnessen, S.; Halvorsen, K.; Harvey, C.; Toffoli, L.; Scott, P.A. Ethical elements in priority setting in nursing care: A scoping review. Int. J. Nurs. Stud. 2018, 88, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Plochg, T.; Arah, O.A.; Botje, D.; Thompson, C.A.; Klazinga, N.S.; Wagner, C.; Mannion, R.; Lombarts, K.; DUQuE Project Consortium. Measuring clinical management by physicians and nurses in European hospitals: Development and validation of two scales. Int. J. Qual. Health Care 2014, 26, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Maughan, E.D.; Bergren, M.D. Future of Nursing 2030: The Future Is Bright for School Nursing. NASN Sch. Nurs. 2021, 36, 248–251. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Descriptive Information | Statistic for Normality | Proportion for Each Level of Response | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Std. Dev | Median | Skew | Kurtosis | Lilliefors (KS) | p Value | Normality | 1 | 2 | 3 | 4 | 5 | 6 | |
| item_1 | 4.29 | 1.134 | 4 | −0.073 | −0.832 | 0.174 | <0.001 | NO | 0.3 | 0.3 | 3.5 | 24.2 | 28.1 | 26.8 |
| item_2 | 4.33 | 1.275 | 4 | −0.203 | −1.003 | 0.165 | <0.001 | NO | 0.3 | 0.3 | 7.7 | 21 | 24.5 | 22.6 |
| item_3 | 3.3 | 1.187 | 3 | 0.408 | −0.236 | 0.2 | <0.001 | NO | 3.5 | 3.5 | 23.2 | 33.2 | 25.2 | 9.4 |
| item_4 | 3.9 | 1.006 | 4 | 0.209 | −0.056 | 0.23 | <0.001 | NO | 0.3 | 0.3 | 6.5 | 27.1 | 43.2 | 15.2 |
| item_5 | 4.33 | 1.074 | 4 | −0.11 | −0.413 | 0.213 | <0.001 | NO | 0.3 | 0.3 | 3.9 | 16.1 | 39 | 23.9 |
| item_6 | 3.9 | 1.182 | 4 | −0.124 | −0.294 | 0.169 | <0.001 | NO | 2.6 | 2.6 | 8.1 | 25.8 | 33.5 | 20.3 |
| item_7 | 3.96 | 1.175 | 4 | 0.106 | −0.37 | 0.202 | <0.001 | NO | 1.6 | 1.6 | 6.5 | 28.4 | 35.2 | 14.8 |
| item_8 | 3.55 | 1.383 | 4 | 0.044 | −0.718 | 0.153 | <0.001 | NO | 6.8 | 6.8 | 18.1 | 22.6 | 28.7 | 13.5 |
| item_9 | 3.91 | 1.23 | 4 | −0.205 | −0.266 | 0.181 | <0.001 | NO | 3.5 | 3.5 | 8.4 | 22.9 | 34.8 | 19.4 |
| item_10 | 4.21 | 1.157 | 4 | −0.126 | −0.648 | 0.175 | <0.001 | NO | 0.3 | 0.3 | 7.1 | 19.4 | 33.5 | 23.9 |
| item_11 | 3.28 | 1.35 | 3 | 0.346 | −0.579 | 0.174 | <0.001 | NO | 7.1 | 7.1 | 24.8 | 27.1 | 22.6 | 10.3 |
| item_12 | 4.02 | 1.415 | 4 | −0.378 | −0.631 | 0.171 | <0.001 | NO | 5.5 | 5.5 | 11 | 15.8 | 28.4 | 22.3 |
| item_13 | 3.34 | 1.438 | 3 | 0.271 | −0.704 | 0.156 | <0.001 | NO | 9 | 9 | 24.2 | 20.3 | 28.4 | 6.8 |
| item_14 | 3.38 | 1.392 | 3 | 0.157 | −0.731 | 0.152 | <0.001 | NO | 8.7 | 8.7 | 20.3 | 25.5 | 23.9 | 13.2 |
| item_15 | 3.42 | 1.596 | 3 | 0.077 | −1.103 | 0.138 | <0.001 | NO | 14.2 | 14.2 | 18.4 | 20.3 | 18.4 | 16.1 |
| item_16 | 4.54 | 1.311 | 5 | −0.644 | −0.22 | 0.174 | <0.001 | NO | 2.6 | 2.6 | 4.5 | 13.5 | 25.8 | 22.9 |
| item_17 | 5.12 | 0.962 | 5 | −0.784 | −0.09 | 0.279 | <0.001 | NO | 0 | 0 | 1.3 | 2.9 | 24.5 | 25.5 |
| item_18 | 4.34 | 1.153 | 4 | −0.084 | −0.678 | 0.211 | <0.001 | NO | 0.3 | 0.3 | 4.8 | 17.4 | 37.1 | 19 |
| item_19 | 4.07 | 1.168 | 4 | 0.064 | −0.528 | 0.201 | <0.001 | NO | 1 | 1 | 6.1 | 25.5 | 35.2 | 17.1 |
| item_20 | 3.52 | 1.331 | 3 | 0.112 | −0.494 | 0.165 | <0.001 | NO | 6.8 | 6.8 | 14.5 | 30 | 27.1 | 11.9 |
| item_21 | 5.01 | 1.149 | 5 | −1.056 | 0.47 | 0.264 | <0.001 | NO | 0.3 | 0.3 | 4.5 | 4.8 | 20.6 | 23.9 |
| item_22 | 4.42 | 1.214 | 4 | −0.375 | −0.551 | 0.173 | <0.001 | NO | 1 | 1 | 5.2 | 16.8 | 28.1 | 25.8 |
| item_23 | 3.31 | 1.313 | 3 | 0.244 | −0.632 | 0.155 | <0.001 | NO | 6.5 | 6.5 | 24.5 | 25.2 | 25.5 | 11.9 |
| item_24 | 4.35 | 1.382 | 4 | −0.445 | −0.638 | 0.162 | <0.001 | NO | 2.6 | 2.6 | 9 | 13.5 | 28.7 | 18.4 |
| item_25 | 5 | 1.049 | 5 | −0.745 | −0.206 | 0.259 | <0.001 | NO | 0 | 0 | 2.3 | 5.2 | 25.8 | 23.9 |
| item_26 | 4.03 | 1.351 | 4 | −0.17 | −0.791 | 0.142 | <0.001 | NO | 2.6 | 2.6 | 11.9 | 20.3 | 27.7 | 19.7 |
| EFA | CFA | ||||||
|---|---|---|---|---|---|---|---|
| Factor Loading | 95% CI | ||||||
| Kiss Item | 1 | 2 | λ | LL | UL | SE | p Value |
| item_1R | 0.262 | 0.195 | |||||
| item_2R | 0.137 | 0.184 | |||||
| item_3 | −0.045 | 0.539 | 1.116 | 0.855 | 1.376 | 0.133 | <0.001 |
| item_4 | 0.049 | 0.419 | 0.661 | 0.475 | 0.847 | 0.095 | <0.001 |
| item_5 | 0.495 | 0.158 | 0.751 | 0.548 | 0.955 | 0.104 | <0.001 |
| item_6 | −0.189 | 0.716 | 1.065 | 0.795 | 1.334 | 0.138 | <0.001 |
| item_7 | −0.060 | 0.575 | 0.745 | 0.519 | 0.970 | 0.115 | <0.001 |
| item_8 | −0.126 | 0.669 | 1.165 | 0.828 | 1.501 | 0.172 | <0.001 |
| item_9 | −0.014 | 0.581 | 1.005 | 0.736 | 1.275 | 0.138 | <0.001 |
| item_10R | 0.377 | 0.355 | <0.001 | ||||
| item_11 | 0.044 | 0.460 | 1.153 | 0.824 | 1.482 | 0.168 | <0.001 |
| item_12R | 0.331 | 0.349 | |||||
| item_13 | 0.168 | 0.512 | 1.057 | 0.770 | 1.345 | 0.146 | <0.001 |
| item_14 | −0.035 | 0.626 | 0.968 | 0.637 | 1.298 | 0.169 | <0.001 |
| item_15 | 0.531 | 0.103 | 1.162 | 0.788 | 1.537 | 0.191 | <0.001 |
| item_16 | 0.673 | 0.041 | 0.846 | 0.587 | 1.105 | 0.132 | <0.001 |
| item_17 | 0.810 | −0.129 | 0.629 | 0.484 | 0.774 | 0.074 | <0.001 |
| item_18 | 0.521 | 0.279 | 0.694 | 0.509 | 0.879 | 0.094 | <0.001 |
| item_19R | 0.325 | 0.362 | |||||
| item_20 | −0.143 | 0.651 | 1.322 | 0.971 | 1.672 | 0.179 | <0.001 |
| item_21 | 0.667 | −0.263 | 0.990 | 0.772 | 1.208 | 0.111 | <0.001 |
| item_22 | 0.764 | 0.027 | 0.824 | 0.622 | 1.026 | 0.103 | <0.001 |
| item_23R | 0.280 | 0.209 | |||||
| item_24 | 0.630 | −0.051 | 1.010 | 0.701 | 1.318 | 0.157 | <0.001 |
| item_25 | 0.706 | −0.112 | 0.648 | 0.472 | 0.824 | 0.090 | <0.001 |
| item_26 | 0.444 | 0.320 | 1.227 | 0.939 | 1.516 | 0.147 | <0.001 |
| Adjustment Indices | Good Fit | 6 Factors | 1 Factor | 2 Factors | |
|---|---|---|---|---|---|
| Reason For Fit | χ2/gL | <2 | 1.6 | ||
| Root Mean Square Error of Approximation | RMSEA | <0.08 | 0.09 | 0.11 | 0.02 |
| Standarized Root Mean Square Residual | SRMR | <0.08 | 0.11 | 0.12 | 0.07 |
| Goodness-of-Fit Index | GFI | >0.90 | 0.80 | 0.75 | 0.96 |
| Comparative Fit Index | CFI | >0.90 | 0.94 | 0.92 | 0.99 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saralegui-Gainza, A.; Soto-Ruiz, N.; Escalada-Hernández, P.; García-Vivar, C.; Rivera, D.; Martín-Rodríguez, L.S. Assessing the Reliability and Validity of the Spanish Version of the Actual Scope of Nursing Practice Scale. Healthcare 2023, 11, 1170. https://doi.org/10.3390/healthcare11081170
Saralegui-Gainza A, Soto-Ruiz N, Escalada-Hernández P, García-Vivar C, Rivera D, Martín-Rodríguez LS. Assessing the Reliability and Validity of the Spanish Version of the Actual Scope of Nursing Practice Scale. Healthcare. 2023; 11(8):1170. https://doi.org/10.3390/healthcare11081170
Chicago/Turabian StyleSaralegui-Gainza, Amaia, Nelia Soto-Ruiz, Paula Escalada-Hernández, Cristina García-Vivar, Diego Rivera, and Leticia San Martín-Rodríguez. 2023. "Assessing the Reliability and Validity of the Spanish Version of the Actual Scope of Nursing Practice Scale" Healthcare 11, no. 8: 1170. https://doi.org/10.3390/healthcare11081170