


Key Maternity Care Stakeholders’ Views on Midwives’ Professional Autonomy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Recruitment
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Variation between Midwives
“So I think …., that to summarise there is a huge heterogeneity [in primary care midwives], and that there is a need for quality of care. I don’t mean that not everyone is doing their best to give quality but that, indeed, sometimes that goes in different directions”.(FG 3_Health Professional 2)
“I think that self-employed midwives who actually do so [performing homebirths] are insufficiently trained and experienced. I think, … that a midwife would act better if she had worked, an extra year for example, 1 or 2 years in a obstetric unit with at least 100 births a year, I say something. Because I think that you are then so much better skilled to make appropriate judgments at home”.(FG 1_Health Professional 1)
“We also question education. This is why recently at [two universities in the Brussels Capital Region] a further training in advanced midwifery practice was established. We know that midwifery education prepare midwives to work in the hospital under supervision, … and that they are not always prepared to work autonomous …”.(FG2_Consumer 1)
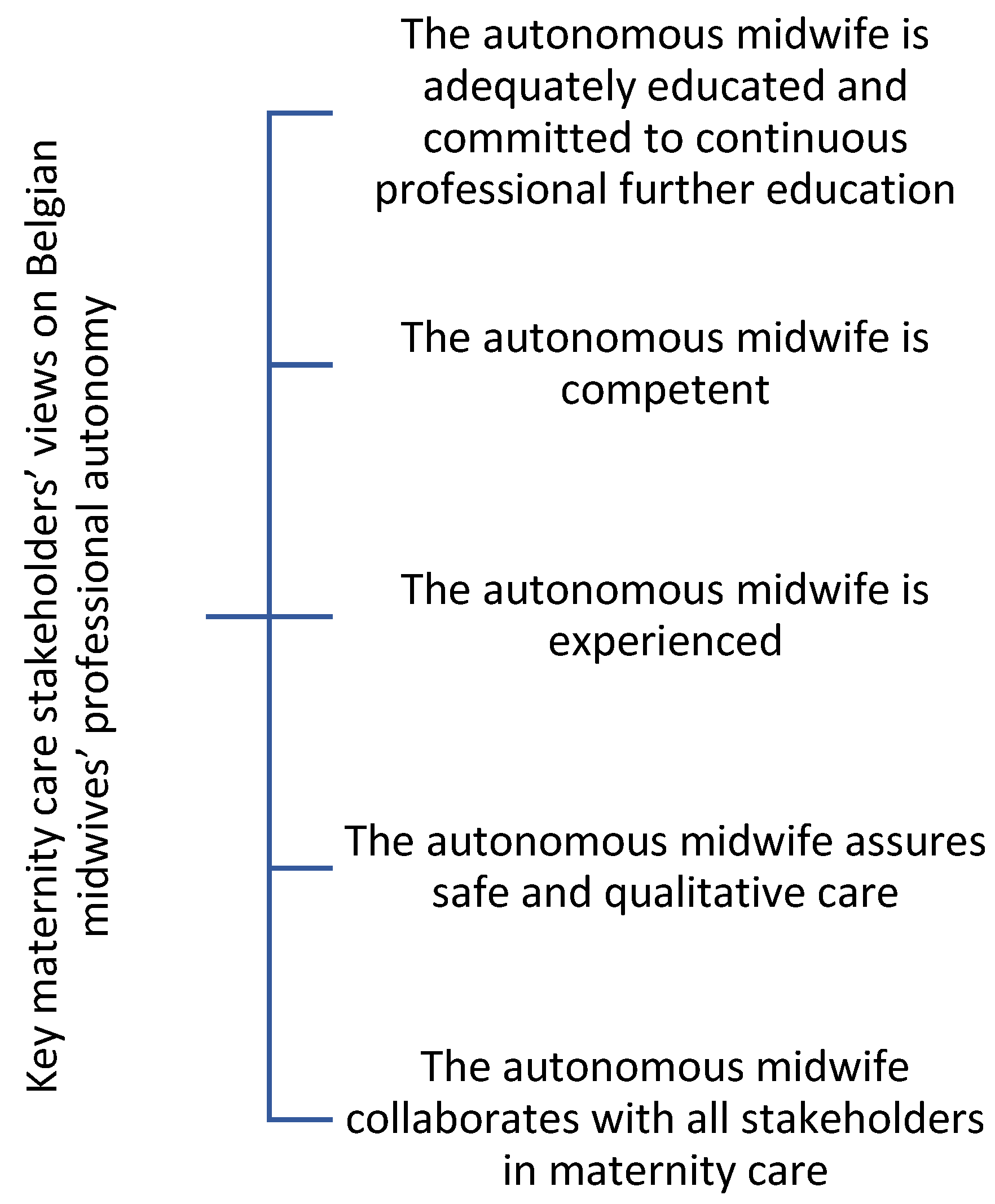
3.2. The Autonomous Midwife Is Competent
“She [the midwife] has completed the necessary education so that she can call in the required help when needed. This need to be in her basic training irrespective if she works at home, at a birth centre or in a hospital. She needs to be competent to identify when and where to refer”.(FG2_Consumer 2)
“I think, for example, giving advice on potty training, is that still a task of an independent midwife? To what extent, … because you can stretch it to … 25 years, to what extent does midwives’ competence reach? I believe that the professional profile and legislation should be guiding in this”.(FG2_Health Professional 2)
“When I may speak for the users, I think the expectations are that they [midwives] are competent, that they are capable, that they can detect if there are problems, if there are pathologies… then refer to other professionals when this is the case”.(FG1_Consumer 5)
“So, the needs of the patients are unknown to us,… and it is our role as professionals to talk about their options, to help them make informed choices … And I think it is our duty as health professionals to inform them correctly”.(FG3_Hospital management 13)
3.3. The Autonomous Midwife Is Experienced
“In your definition [definition of midwifery autonomy in Belgium] there is a word that drew my attention, and that is ‘mastery’. And there I support [a stakeholder from hospital management,] to achieve mastery you must work with different professionals. To be autonomous it is the mastery, the anticipation and the continuity of care”.(FG3_Health Professional 4)
“I think you need a minimum experience in performing births in a hospital to know em, … when it suddenly unexpectedly goes wrong. Because if you don’t have real work experience in the hospital, I think you’re missing some competences … So a minimal experience, … really working as a midwife and in the hospital, I find that indispensable as a paediatrician”.(FG2_Health Professional 2)
3.4. The Autonomous Midwife Assures Safe and Qualitative Care
“For me, autonomy of midwives in Belgium should be limited to a physiological pregnancy, … but always in a medical setting,… So, autonomy of midwives is certainly possible, it is done in many hospitals where midwives can consult autonomously, but in collaboration with a doctor who can always give their opinion. Like in the labour room, midwives are equipped for it to be, perfectly possible that the midwife performs normal births, I am the first defender of that, but always in a medical setting”.(FG2_Policy advisor 1)
“What secures birth is the human and not the machines, it’s not the hospital that secures birth. It is the caregivers who are well equipped, well trained and work together. Autonomy is about collaboration, but with respect to the expertise and knowledge of each one. And so it’s not because you are a doctor that you are a good doctor, …, it’s not because you are a midwife that you are poorly trained, that you have no experience and that you don’t know your limits”.(FG2_Consumer 1)
“A pregnancy is a period when a kind of checklist needs to be used to anticipate and to make clear agreements between your network, between paediatricians, with obstetricians …. So now, I think that is a very important issue because we are actually talking about, a care path and about agreements and about em limits”.(FG3_Health Professional 3)
“And what I find difficult is that they [independent midwives] are a group is that often goes quite the alternative tour and yes, … I have seen few children who have not been sent to the osteopath, recommended to take supplements—that cost a lot of money—but which isn’t much of proven value”.(FG2_Health Professional 2)
3.5. The Autonomous Midwife Collaborates with All Stakeholders in Maternity Care
“Autonomy, that sounds like ‘I work on my own, and this is my field of expertise and you must stay away’, … and if we would collaborate and respect each other’s competences …, with that we would move forward”.(FG3_Policy Advisor 1)
“Nowadays obstetricians are absolutely willing to respect physiology as much as possible. But we know that many independent midwives do not trust, … So I regret that, I think it really, really [accentuated] is time that obstetricians and independent midwives come back together, because I think we do not really have so many differences in vision at the end, … together we can make good progress”.(FG1_Health Professional 1)
“… to act in a confraternal way and, … we must restrain debate, … As obstetricians we have to stop saying ‘yes, but the midwife knows nothing’ and the midwife has to stop saying ‘yes, but the obstetricians are always exaggerating’. When we have that mutual reserve, it is obvious that we will move on much better”.(FG3_Health Professional 4)
“I can testify that it [respectful collaboration] goes very well with the paediatricians, obstetricians, … All the health professionals surrounding the midwife, where everyone has a place and respects each other in what they do. When it brings value to the patient, it is good for the patient and the continuity of care and most important …, I think, for each one of us”.(FG3_Hospital Management 1)
4. Discussion
4.1. Competence
4.2. Education
4.3. Collaboration
4.4. Respect
4.5. Strengths and Limitations
4.5.1. Strengths
4.5.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Healy, S.; Humphreys, E.; Kennedy, C. A qualitative exploration of how midwives’ and obstetricians’ perception of risk affects care practices for low-risk women and normal birth. Women Birth 2017, 30, 367–375. [Google Scholar] [CrossRef]
- Prosen, M. A systematic integrative literature review of the factors influencing the professionalization of midwifery in the last decade (2009–2019). Midwifery 2022, 106, 103246. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.; Luyben, A.; O’Connell, R.; Gillen, P.; Escuriet, R.; Fleming, V. Failure or progress?: The current state of the professionalisation of midwifery in Europe. Eur. J. Midwifery 2019, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mead, M.; Bogaerts, A.; Reyns, M. Midwives’ perception of the intrapartum risk of healthy nulliparae in spontaneous labour, in The Flanders, Belgium. Midwifery 2007, 23, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Fleming, V. Autonomous or automatons? An exploration through history of the concept of autonomy in midwifery in Scotland and New Zealand. Nurs. Ethics 1998, 5, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Baird, K. Exploring autonomy in education: Preparing student midwives. Br. J. Midwifery 2007, 15, 400–405. [Google Scholar] [CrossRef]
- Vermeulen, J.; Luyben, A.; Buyl, R.; Debonnet, S.; Castiaux, G.; Niset, A.; Muyldermans, J.; Fleming, V.; Fobelets, M. The state of professionalisation of midwifery in Belgium: A discussion paper. Women Birth 2020, 7–13. [Google Scholar] [CrossRef]
- PlanKad Vroedvrouwen 2019. Cel Planning van Het Aanbod van de Gezondheidszorgberoepen, Dienst Gezondheidszorgberoepen en Beroepsuitoefening, Directoraat-generaal Gezondheidszorg, FOD Volksgezondheid, Veiligheid van de Voedselketen en Leefmilieu. Available online: https://overlegorganen.gezondheid.belgie.be/sites/default/files/documents/vroedvrouwen_op_de_arbeidsmarkt_2019.pdf (accessed on 7 September 2022).
- Benahmed, N.; Devos, C.; San Miguel, L.; Vinck, I.; Van Kelst, L.; Lauwerier, E.; Verschueren, M.; Obyn, C.; Paulus, D.; Christiaens, W. Caring for Mothers and Newborns after Uncomplicated Delivery: Towards Integrated Postnatal Care; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2014. Available online: https://kce.fgov.be/sites/default/files/2021-11/KCE_232Cs_Postnatal_care_Synthesis_3.pdf (accessed on 7 September 2022).
- Van de Voorde, C.; Van den Heede, K.; Beguin, C.; Bouckaert, N.; Camberlin, C.; de Bekker, P.; Defourny, N.; De Schutter, H.; Devos, C.; Gerkens, S.; et al. Required Hospital Capacity in 2025 and Criteria for Rationalisation of Complex Cancer Surgery, Radiotherapy and Maternity Services; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2017. Available online: https://kce.fgov.be/sites/default/files/2021-11/Download%20the%20report%20in%20English%20(550%20p.).pdf (accessed on 7 September 2022).
- Vandeputte, L.; Van Den Bergh, E.; Rothmann, I.; Pink, K.; Tency, I.; Reyns, M.; D’haenens, F.; Muyldermans, J. Jaarrapport Vroedvrouwgeleide Zorg Tijdens de Arbeid en Bevalling in Cijfers: 2021 [Annual Report on Midwifery-Led Care in Labour and Childbirth: 2021]; Vlaamse Beroepsorganisatie van Vroedvrouwen [Flemish Professional Association of Midwives]: Antwerp, Belgium, 2023. [Google Scholar]
- Statbel. Statbel: België in Cijfers [Statbel: Belgium in Figures]. Available online: https://statbel.fgov.be/nl/themas/bevolking/structuur-van-de-bevolking (accessed on 7 September 2022).
- Devos, C.; Cordon, A.; Lefèvre, M.; Obyn, C.; Renard, F.; Bouckaert, N.; Gerkens, S.; Maertens de Noordhout, C.; Devleesschauwer, B.; Haelterman, M.; et al. Performance of the Belgian health System—Report 2019. Health Services Research (HSR); Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2019.
- Goemaes, R.; Fomenko, E.; Laubach, M.; De Coen, K.; Roelens, K.; Bogaerts, A. Perinatale Gezondheid in Vlaanderen—Jaar 2021. [Perinatal Health in Flanders—Year 2021]; Studiecentrum voor Perinatale Epidemiologie: Brussel, Belgium, 2022. [Google Scholar]
- Leroy, C.; Van Leeuw, V. Santé Périnatale en Wallonie—Année 2021. [Perinatal Health in Walloon—Year 2021]; Centre d’Épidémiologie Périnatale: Brussel, Belgium, 2022. [Google Scholar]
- Van Leeuw, V.; Leroy, C. Santé Périnatale en Région Bruxelloise—Année 2021. [Perinatal Health in Brussels Capital Region—Year 2021]; Centre d’Épidémiologie Périnatale: Brussel, Belgium, 2022. [Google Scholar]
- Van Kelst, L.; Spitz, B.; Sermeus, W.; Thomson, A. A hermeneutic phenomenological study of Belgian midwives’ views on ideal and actual maternity care. Midwifery 2013, 29, e9–e17. [Google Scholar] [CrossRef]
- Christiaens, W.; Nieuwenhuijze, M.; de Vries, R. Trends in the medicalisation of childbirth in Flanders and the Netherlands. Midwifery 2013, 29, e1–e8. [Google Scholar] [CrossRef]
- Belgian Federal Public Service Public Health, Food Chain Safety and Environment. Key Data in Health Care—Healthcare Professionals. Available online: https://www.health.belgium.be/sites/default/files/uploads/fields/fpshealth_theme_file/healthcare_profesionals.pdf (accessed on 7 September 2022).
- Clemons, J.H.; Gilkison, A.; Mharapara, T.L.; Dixon, L.; McAra-Couper, J. Midwifery Job Autonomy in New Zealand: I do it all the time. Women Birth J. Aust. Coll. Midwives 2021, 34, 30–37. [Google Scholar] [CrossRef]
- Yoshida, Y.; Sandall, J. Occupational burnout and work factors in community and hospital midwives: A survey analysis. Midwifery 2013, 29, 921–926. [Google Scholar] [CrossRef]
- European Parliament and the Council of the European Union. Directive 2013/55/EU of the European Parliament and of the Council of 20th November 2013 (English); 28.12.2013, L354/132-L354/169; Official Journal of the European Union: Brussels, Belgium, 2013. [Google Scholar]
- Vermeulen, J.; Luyben, A.; Jokinen, M.; Matintupa, E.; O’Connell, R.; Bick, D. Establishing a Europe-wide foundation for high quality midwifery education: The role of the European Midwives Association (EMA). Midwifery 2018, 64, 128–131. [Google Scholar] [CrossRef]
- Van Kelst, L.; Spitz, B.; Sermeus, W.; Thomson, A. Student midwives’ views on maternity care just before their graduation. J. Adv. Nurs. 2013, 69, 600–609. [Google Scholar] [CrossRef]
- Goemaes, R.; Beeckman, D.; Verhaeghe, S.; Van Hecke, A. Sustaining the quality of midwifery practice in Belgium: Challenges and opportunities for advanced midwife practitioners. Midwifery 2020, 89, 102792. [Google Scholar] [CrossRef]
- Vermeulen, J.; Buyl, R.; Luyben, A.; Fleming, V.; Fobelets, M. Defining midwifery autonomy in Belgium: Consensus of a modified Delphi study. J. Adv. Nurs. 2022, 78, 2849–2860. [Google Scholar] [CrossRef]
- Perdok, H.; Jans, S.; Verhoeven, C.; Henneman, L.; Wiegers, T.; Mol, B.W.; Schellevis, F.; de Jonge, A. Opinions of maternity care professionals and other stakeholders about integration of maternity care: A qualitative study in the Netherlands. BMC Pregnancy Childbirth 2016, 16, 188. [Google Scholar] [CrossRef]
- Feo, R.; Conroy, T.; Jangland, E.; Muntlin Athlin, Å.; Brovall, M.; Parr, J.; Blomberg, K.; Kitson, A. Towards a standardised definition for fundamental care: A modified Delphi study. J Clin. Nurs. 2018, 27, 2285–2299. [Google Scholar] [CrossRef]
- Devane, D.; Begley, C.M.; Clarke, M.; Horey, D.; Oboyle, C. Evaluating maternity care: A core set of outcome measures. Birth 2007, 34, 164–172. [Google Scholar] [CrossRef]
- Lefèvre, M.; Bouckaert, N.; Camberlin, C.; Devriese, S.; Pincé, H.; de Meester, C.; Fricheteau, B.; Van de Voorde, C. Organisation of Maternity Services in Belgium; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2019. Available online: https://kce.fgov.be/sites/default/files/2021-11/KCE_323_Maternity_services_Belgium_Report.pdf (accessed on 7 September 2022).
- Krueger, R. Focus Groups: A Practical Guide for Applied Research; Sage Publications: London, UK, 2014. [Google Scholar]
- Forrestal, S.; D’Angelo, A.; Vogel, L. Considerations for and lessons learned from online, synchronous focus groups. Surv. Pract. 2015, 8, 8–15. [Google Scholar] [CrossRef]
- Wong, L.P. Focus group discussion: A tool for health and medical research. Singap. Med. J. 2008, 49, 256–260. [Google Scholar]
- Roller, M.R.; Lavrakas, P.J. Applied Qualitative Research Design: A Total Quality Framework Approach; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care J. 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Renfrew, M.J.; Cheyne, H.; Burnett, A.; Crozier, K.; Downe, S.; Heazell, A.; Hundley, V.; Hunter, B.; King, K.; Marshall, J.E.; et al. Responding to the Ockenden Review: Safe care for all needs evidence-based system change-and strengthened midwifery. Midwifery 2022, 112, 103391. [Google Scholar] [CrossRef] [PubMed]
- Lanssens, D.; Goemaes, R.; Vrielinck, C.; Tency, I. Knowledge, attitudes and use of evidence-based practice among midwives in Belgium: A cross-sectional survey. Eur. J. Midwifery 2022, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Newnham, E.; Kirkham, M. Beyond autonomy: Care ethics for midwifery and the humanization of birth. Nurs. Ethics 2019, 26, 2147–2157. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, L.; Reed, R.; Broadbent, M.; Hastie, C. “I didn’t feel like I could trust her and that felt really risky”: A phenomenographic exploration of how Australian Midwives describe intrapartum risk. Midwifery 2022, 118, 103582. [Google Scholar] [CrossRef]
- Catling-Paull, C.; Coddington, R.L.; Foureur, M.J.; Homer, C.S. Publicly funded homebirth in Australia: A review of maternal and neonatal outcomes over 6 years. Med. J. Aust. 2013, 198, 616–620. [Google Scholar] [CrossRef]
- Advies van de Federale Raad Voor de Vroedvrouwen Betreffende Vroedvrouwen Die Onder Hun Eigen Verantwoordelijkheid Bevallingen Uitvoeren. [Advice of the Federal Council for Midwives Concerning Midwives Who Perform Births under Their Own Responsibility]. Available online: https://overlegorganen.gezondheid.belgie.be/sites/default/files/documents/federale_raad_voor_de_vroedvrouwen/19105129.pdf (accessed on 7 September 2022).
- Gecommentarieerde Code van Medische Deontologie [Commented Code of Medical Deontology]. Orde Der Artsen. [Order of Doctors]; Larcier: Brussels, Belgium, 2019.
- Greenhalgh, T.; Howick, J.; Maskrey, N. Evidence based medicine: A movement in crisis? BMJ 2014, 348, g3725. [Google Scholar] [CrossRef]
- Bleijenbergh, R.; Mestdagh, E.; Kuipers, Y.J. Midwifery Practice and Education in Antwerp: Forecasting Its Future with Scenario Planning. J. Contin. Educ. Nurs. 2022, 53, 21–29. [Google Scholar] [CrossRef]
- Buring, S.M.; Bhushan, A.; Broeseker, A.; Conway, S.; Duncan-Hewitt, W.; Hansen, L.; Westberg, S. Interprofessional education: Definitions, student competencies, and guidelines for implementation. Am. J. Pharm. Educ. 2009, 73, 59. [Google Scholar] [CrossRef]
- Darlow, B.; Coleman, K.; McKinlay, E.; Donovan, S.; Beckingsale, L.; Gray, B.; Neser, H.; Perry, M.; Stanley, J.; Pullon, S. The positive impact of interprofessional education: A controlled trial to evaluate a programme for health professional students. BMC Med. Educ. 2015, 15, 98. [Google Scholar] [CrossRef]
- Vermeulen, J.; Vivilaki, V.G. A value-based philosophy debate on academic midwifery education in Europe. Eur. J. Midwifery 2021, 5, 55. [Google Scholar] [CrossRef]
- van Minde, M.R.C.; van Veen-Belle, D.W.; Ernst-Smelt, H.E.; Rosman, A.N.; Raat, H.; Steegers, E.A.P.; de Kroon, M.L.A. Handover of care and of information by community midwives, maternity care assistants and Preventive Child Healthcare professionals, a qualitative study. Midwifery 2019, 78, 25–31. [Google Scholar] [CrossRef]
- Perdok, H.; Cronie, D.; van der Speld, C.; van Dillen, J.; de Jonge, A.; Rijnders, M.; de Graaf, I.; Schellevis, F.; Verhoeven, C. Experienced job autonomy among maternity care professionals in The Netherlands. Midwifery 2017, 54, 67–72. [Google Scholar] [CrossRef]
- Mattison, C.; Bourret, K.; Hebert, E.; Leshabari, S.; Kabeya, A.; Achiga, P.; Robinson, J.; Darling, E. Health systems factors impacting the integration of midwifery: An evidence-informed framework on strengthening midwifery associations. BMJ Glob. Health 2021, 6, e004850. [Google Scholar] [CrossRef]
- van Minde, M. Building Bridges between Perinatal & Preventive Child Healthcare; Erasmus Universiteit Rotterdam: Rotterdam, The Netherlands, 2022. [Google Scholar]
- Dahlen, H.G.; Drandic, D.; Shah, N.; Cadee, F.; Malata, A. Supporting midwifery is the answer to the wicked problems in maternity care. Lancet Glob. Health 2022, 10, e951–e952. [Google Scholar] [CrossRef]
- Sutton, E.A.; Ananthram, H.; Montgomery, N.; Matthews, R. Be as you wish to seem: Tragedy, triumphalism, and toxicity in maternity services. Lancet Glob. Health 2022, 10, e1237. [Google Scholar] [CrossRef]
- Shareef, N.; Scholten, N.; Nieuwenhuijze, M.; Stramrood, C.; de Vries, M.; van Dillen, J. The role of birth plans for shared decision-making around birth choices of pregnant women in maternity care: A scoping review. Women Birth J. Aust. Coll. Midwives 2022. [Google Scholar] [CrossRef]
- Welffens, K.; Derisbourg, S.; Costa, E.; Englert, Y.; Pintiaux, A.; Warnimont, M.; Kirkpatrick, C.; Buekens, P.; Daelemans, C. The “Cocoon”, first alongside midwifery-led unit within a Belgian hospital: Comparison of the maternal and neonatal outcomes with the standard obstetric unit over 2 years. Birth 2020, 47, 115–122. [Google Scholar] [CrossRef]
- Benahmed, N.; Hendrickx, E.; Adriaenssens, J.; Stordeur, S. Planning van Gezondheidszorgpersoneel en Gegevens over Vroedvrouwen [Planning of Health Care Staff and Data on Midwives]; Belgian Health Care Knowledge Centre (KCE): Brussels, Belgium, 2016. Available online: https://kce.fgov.be/nl/publicaties/alle-rapporten/planning-van-gezondheidszorgpersoneel-en-gegevens-over-vroedvrouwen (accessed on 7 September 2022).
- Kuipers, Y.; Degraeve, J.; Bosmans, V.; Thaels, E.; Mestdagh, E. Midwifery-led care: A single mixed-methods synthesis. Int. J. Healthc. Manag. 2022, 16, 35–50. [Google Scholar] [CrossRef]
- Corbie-Smith, G.; Wynn, M.; Richmond, A.; Rennie, S.; Green, M.; Hoover, S.M.; Watson-Hopper, S.; Nisbeth, K.S. Stakeholder-driven, consensus development methods to design an ethical framework and guidelines for engaged research. PLoS ONE 2018, 13, e0199451. [Google Scholar] [CrossRef]


{kind=link}
| Health Professionals | Policy Advisors | Hospital Management | Consumers |
|---|---|---|---|
| Flemish Association for Obstetrics and Gynaecology | Planification commission | Council of University Hospitals Belgium | Flemish patient platform |
| Professional association of Belgian obstetricians and gynaecologists | Federal Knowledge Centre for Healthcare KCE | Board of nursing managers NVKVV Network Nursing | Representatives of patients in the Federal Knowledge Centre for Healthcare KCE |
| Royal College of Gynaecologists Obstetricians of French Language of Belgium RVB | Study centre for perinatal epidemiology, Flanders | Flemish Association for Nursing executives | Women’s Council FERM |
| Belgian Group of French-speaking Paediatricians | Perinatal Epidemiology Center, Brussels and Walloon | Flemish Hospital network | Health Services Users League |
| Flemish Society for Paediatrics | Federal Council of Midwives | Belgian Association of Nurses and National Federation of Nurses of Belgium: Board of Directors of Nursing Departments | Platform for a respected birth |
| Belgian Society for Paediatrics | National Institute for Health and Disability Insurance | Federal Council of Hospitals | Together for respectful birth |
| Professional association of General Practitioners in Flanders and Brussels | Federal Public Service Health, Food Chain Safety and Environment | The world according to women | |
| Belgian Group of General Practitioners | Federal Public Service Social Security | Dutch-speaking women’s Council | |
| College of physicians for the mother and the newborn | Zorgnet ICURO, umbrella organisation of the Flemish general hospitals, initiatives in mental healthcare and social profit facilities in geriatric care | Council of French-speaking women of Belgium | |
| Belgian Society for Neonatology | Flemish health ambassador | Feminine Life | |
| Child and Family Services | Flemish association for parents of incubator babies | ||
| the Office of Birth and Childhood ONE | |||
| Federation of Francophone Medical Centres and Health Collectives | |||
| Scientific Society of General Medicine |
| Engagement Question |
| How do you perceive Belgian midwives’ autonomy in everyday practice? |
| Exploring questions |
| What are your expectations of midwives working as autonomous practitioners? |
| To what extent do you think that midwives should act autonomously? |
| What would you think are factors/stakeholders that influence midwives’ autonomy? |
| Probes (in order to minimise misunderstandings) |
| Can you please tell more about this? |
| Please, help us understand what you exactly mean by that? |
| Can you give us an example of that? |
| Exit questions |
| Is there anything additional you would like to say about midwifery autonomy? |
| Of all things discussed today, what do you think is the most important? |
| Health Professionals n = 12 | Policy Advisors n = 3 | Hospital Management n = 4 | Consumers n = 8 | ||
|---|---|---|---|---|---|
| Gender (female, male) | Female | 9 | 2 | 3 | 8 |
| Male | 3 | 1 | 1 | 0 | |
| Age (years) | 20–30 | 0 | 0 | 0 | 1 |
| 31–40 | 1 | 0 | 1 | 4 | |
| 41–50 | 3 | 2 | 0 | 0 | |
| 51–60 | 6 | 1 | 1 | 1 | |
| >60 | 2 | 0 | 2 | 2 | |
| Native language (Dutch, French) | Dutch | 7 | 2 | 2 | 4 |
| French | 5 | 1 | 2 | 4 | |
| Education level (highest completed education) | No education/Primary education only | 0 | 0 | 0 | 0 |
| Secondary education | 0 | 0 | 0 | 0 | |
| Tertiary education | 12 | 3 | 4 | 8 | |
| Professional experience (years) | <5 | 0 | 0 | 0 | 3 |
| 5–10 | 0 | 0 | 0 | 2 | |
| 11–20 | 3 | 1 | 1 | 2 | |
| 21–30 | 7 | 1 | 1 | 1 | |
| >30 | 2 | 1 | 2 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vermeulen, J.; Buyl, R.; Luyben, A.; Fleming, V.; Fobelets, M. Key Maternity Care Stakeholders’ Views on Midwives’ Professional Autonomy. Healthcare 2023, 11, 1231. https://doi.org/10.3390/healthcare11091231
Vermeulen J, Buyl R, Luyben A, Fleming V, Fobelets M. Key Maternity Care Stakeholders’ Views on Midwives’ Professional Autonomy. Healthcare. 2023; 11(9):1231. https://doi.org/10.3390/healthcare11091231
Chicago/Turabian StyleVermeulen, Joeri, Ronald Buyl, Ans Luyben, Valerie Fleming, and Maaike Fobelets. 2023. "Key Maternity Care Stakeholders’ Views on Midwives’ Professional Autonomy" Healthcare 11, no. 9: 1231. https://doi.org/10.3390/healthcare11091231
APA StyleVermeulen, J., Buyl, R., Luyben, A., Fleming, V., & Fobelets, M. (2023). Key Maternity Care Stakeholders’ Views on Midwives’ Professional Autonomy. Healthcare, 11(9), 1231. https://doi.org/10.3390/healthcare11091231