
Associations between Physical Activity Frequency in Leisure Time and Subjective Cognitive Limitations in Middle-Aged Spanish Adults: A Cross-Sectional Study
 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Age and Cognitive Function
1.2. Cognitive Function and Risk Factors
1.3. Physical Activity and Cognitive Function
2. Materials and Methods
2.1. Study Design
2.2. Instruments (Spanish National Health Survey and European Health Survey in Spain)
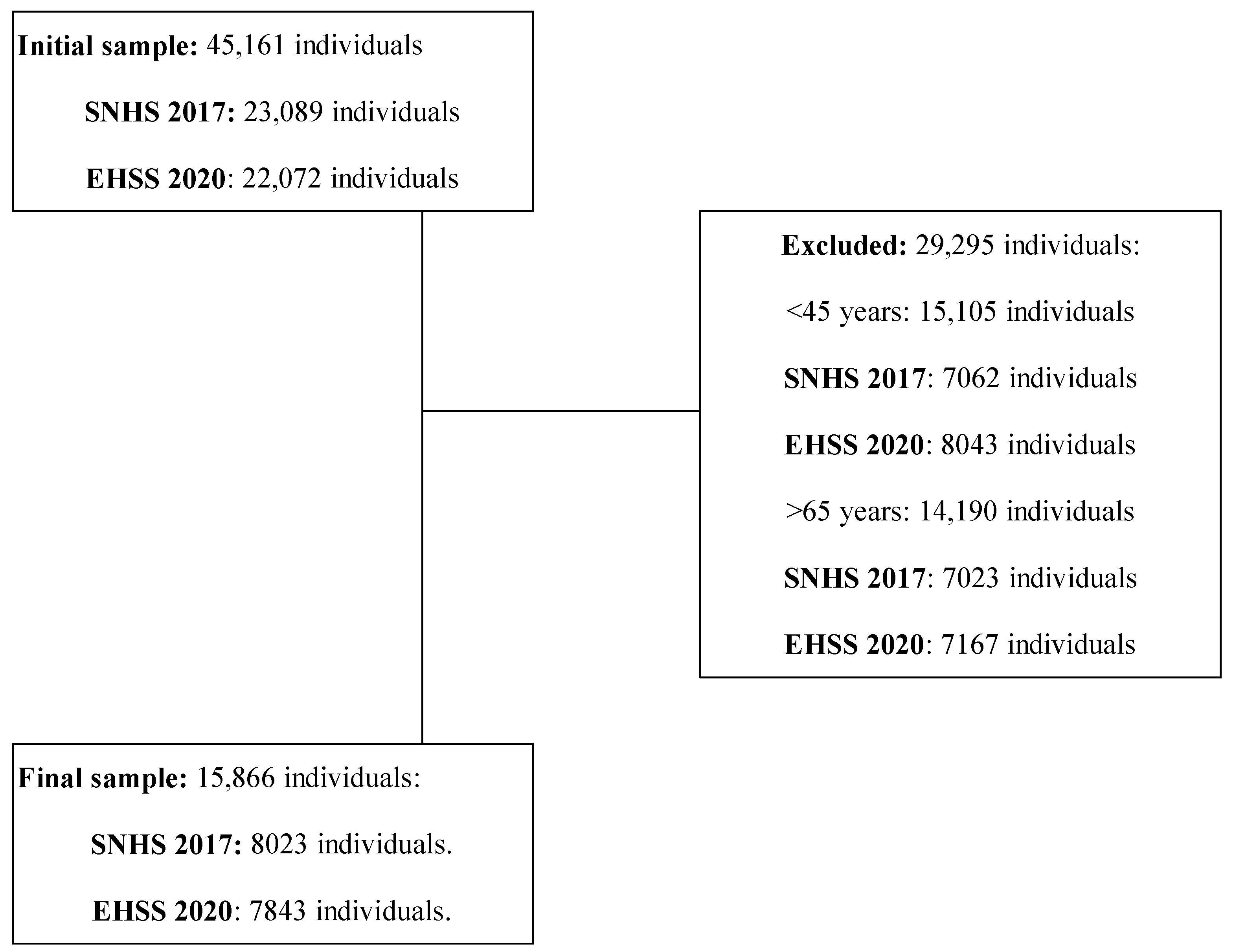
2.3. Sample
2.4. Variables Extracted from the Surveys
2.4.1. Outcome Variables
- Subjective Cognitive Limitation Levels (SCLLs) were extracted from responses to the Q.38a variable: Do you have difficulty to remember or to concentrate? With 4 possible answers, as follows:
- (1)
- No, no difficulty (“None”).
- (2)
- Yes, some difficulty (“Some”).
- (3)
- Yes, many difficulties (“A lot”).
- (4)
- I can’t do it at all (“Absolutely”).
- Subjective Cognitive Limitations (SCLs): This dichotomous variable was created from the responses to the SCLL variable. The results were grouped into 2 categories:
- (1)
- No: Participants who answered “No, no difficulty”.
- (2)
- Yes: Participants who answered “Yes, some difficulty”, or “Yes, many difficulties or can’t do it at all”.
2.4.2. Independent, Predictor and Covariate Variables
- Age: In years. This continuous variable was drawn from the variable “AGEa” of both surveys.
- Sex: This was drawn from the variable “SEXOa” from both surveys with two possible responses (Men or Women).
- Body Mass Index (BMI) Group: This was drawn from the variable “BMIa” from both surveys. Participants were grouped according to their BMI (Weight in kg/Height2 in metres). The following 4 groups were established:
- (1)
- Underweight (BMI < 18.5).
- (2)
- Normal (BMI ≥ 18.5 and <25).
- (3)
- Overweight (BMI ≥ 25 and <30).
- (4)
- Obesity (BMI ≥ 30).
- Civil Status: This was drawn from the answers given by participants to item Q.4b: What is your legal marital status? There were 5 possible answers:
- (1)
- Single.
- (2)
- Married.
- (3)
- Widowed.
- (4)
- Legally Separated.
- (5)
- Divorced.
- Study Level: This was extracted from the variables “NIVEST” (SNHS 2017) and “STUDY” (EHSS 2020). These variables reflected the highest level of study attained by the participants. For this research, participants were grouped into 5 groups:
- (1)
- Primary studies (participants with completed or incomplete primary education).
- (2)
- Secondary studies (participants with compulsory secondary education with or without a diploma).
- (3)
- Baccalaureate (participants with baccalaureate studies).
- (4)
- Vocational training (participants with vocational education and training at intermediate or higher level or equivalent).
- (5)
- University (participants with university education).
- Social Class: This was extracted from the variable “CLASE_PR” from both surveys. Both surveys grouped participants into six social classes (I, II, III, IV, V, and VI) according to their occupations as indicated. Table S2 shows a more comprehensive description of this classification.
- Physical Activity Frequency (PAF): This was taken from item Q.112 of both surveys. The question was as follows: Which of these possibilities best describes the frequency with which you do some physical activity in your free time? There were 4 possible answers. For this study, the groups were named as follows:
- (1)
- Never: Participants who answered “I do not exercise”.
- (2)
- Occasional: Participants who answered “I do occasional physical activity or sport”.
- (3)
- Frequently: Participants who responded “I do physical activity several times a month”.
- (4)
- Very frequently: Participants who responded “I do physical or sport training several times a week”.
2.5. Statistical Analysis
3. Results
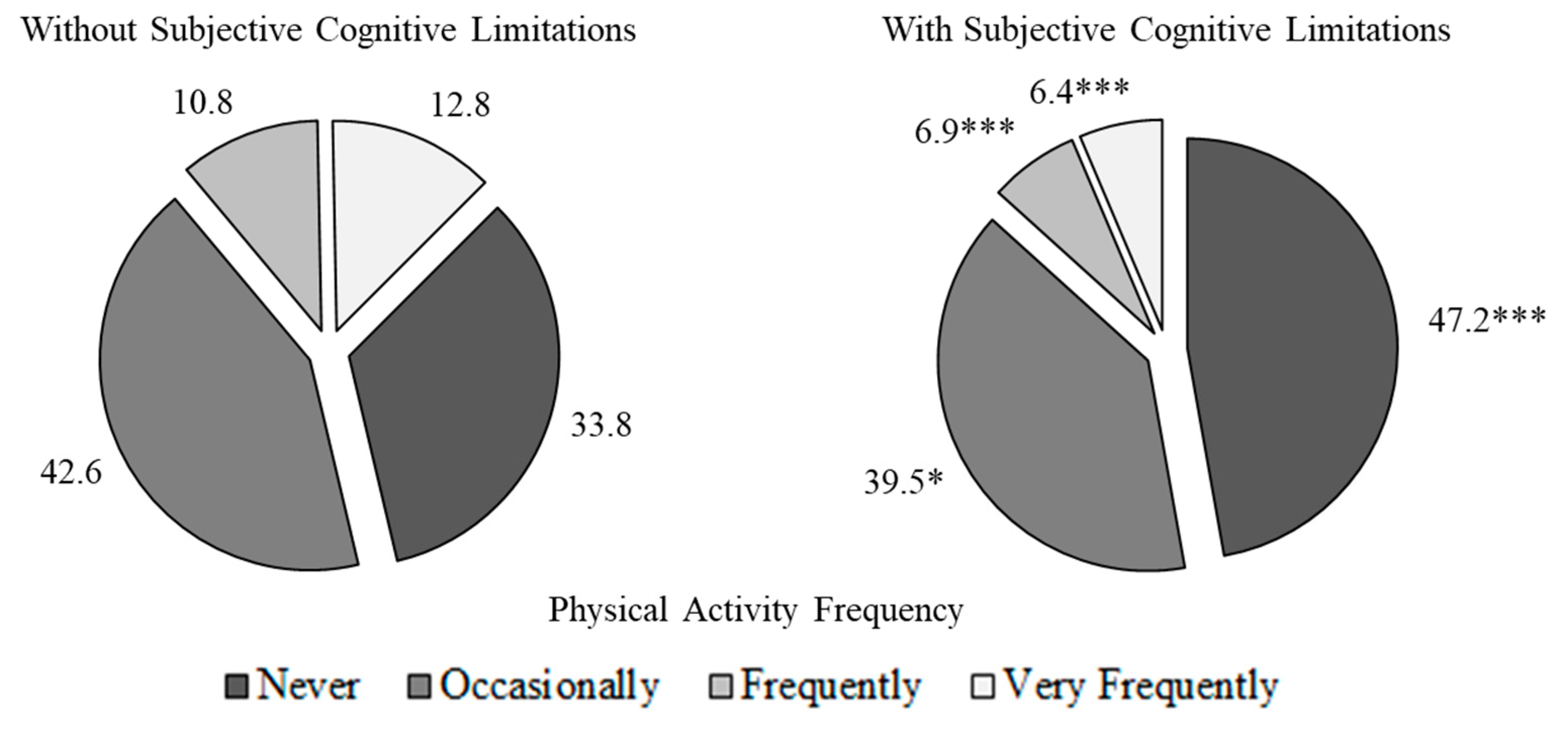
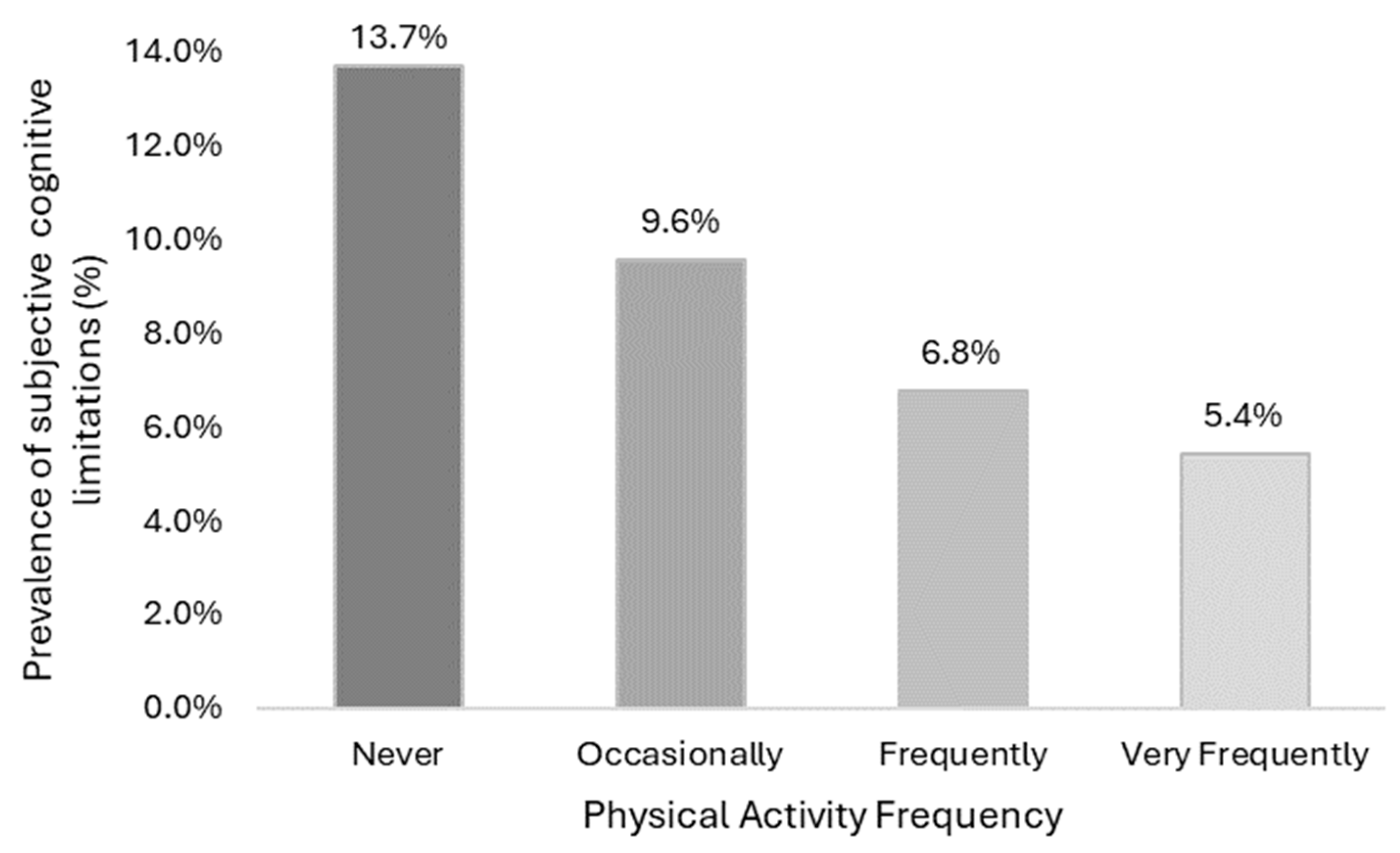
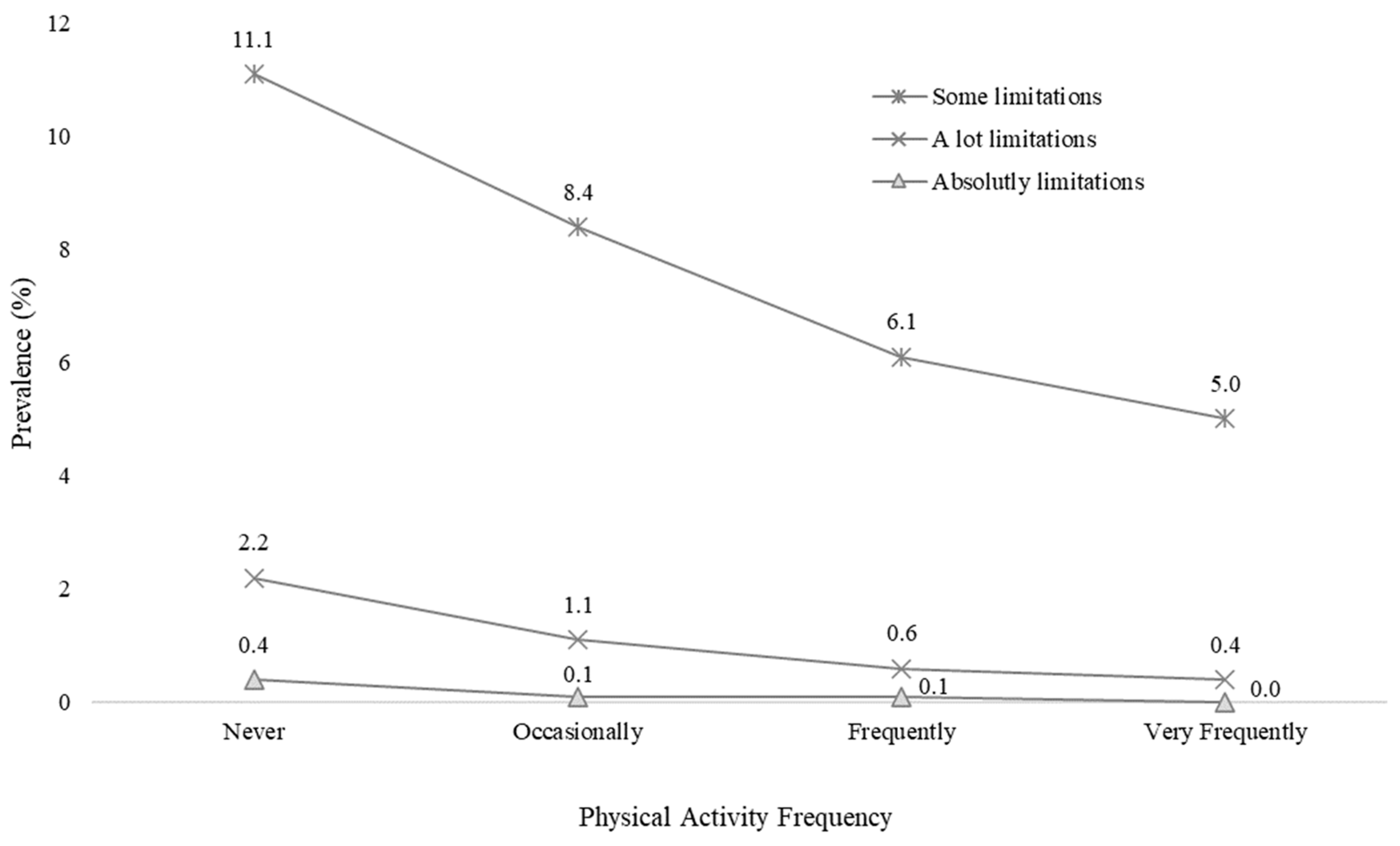
3.1. Physical Activity Frequency and Subjective Cognitive Limitations
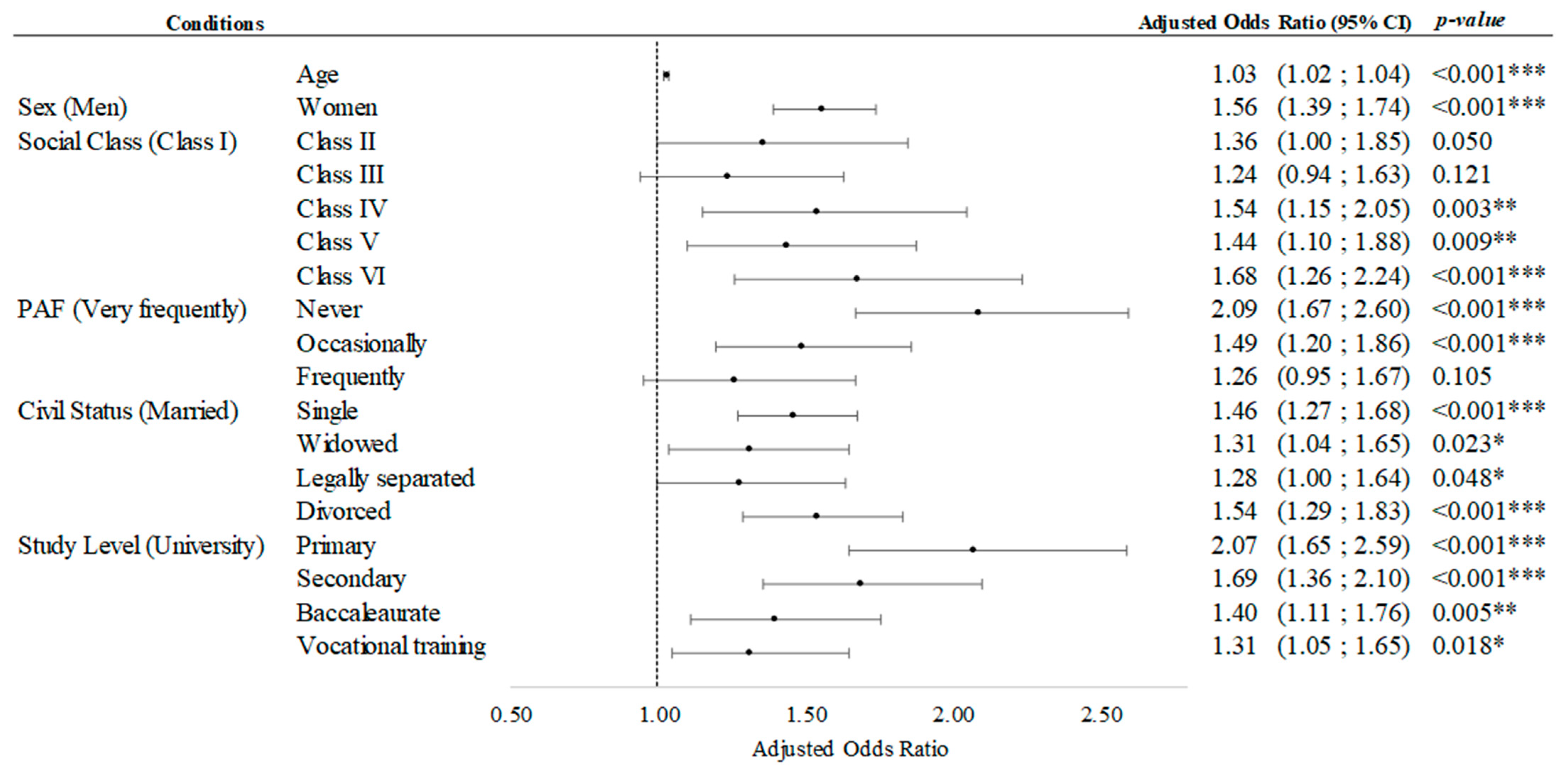
3.2. Multiple Binary Logistic Regression
4. Discussion
4.1. Subjective Cognitive Limitations and Physical Activity in Leisure Time
Logistic Regression Analysis
4.2. Limitations and Future Lines of Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eurostat Half of EU’s Population Older than 44.4 Years in 2022. Eurostat, 22 February 2023.
- Møgelmose, S.; Neels, K.; Beutels, P.; Hens, N. Exploring the impact of population ageing on the spread of emerging respiratory infections and the associated burden of mortality. BMC Infect. Dis. 2023, 23, 767. [Google Scholar] [CrossRef]
- Dexter, M.; Ossmy, O. The effects of typical ageing on cognitive control: Recent advances and future directions. Front. Aging Neurosci. 2023, 15, 1231410. [Google Scholar] [CrossRef]
- Maldonado, T.; Orr, J.M.; Goen, J.R.M.; Bernard, J.A. Age Differences in the Subcomponents of Executive Functioning. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, e31–e55. [Google Scholar] [CrossRef] [PubMed]
- Korotkevich, Y.; Trewartha, K.M.; Penhune, V.B.; Li, K.Z.H. Effects of age and cognitive load on response reprogramming. Exp. Brain Res. 2015, 233, 937–946. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, D.; Hou, W.; Li, H. Cognitive Decline Associated with Aging. Adv. Exp. Med. Biol. 2023, 1419, 25–46. [Google Scholar] [CrossRef] [PubMed]
- Models of Visuospatial and Verbal Memory Across the Adult Life Span (PDF)—Pamela K. Smith. Available online: https://www.pamelaksmith.com/publications/models-of-visuospatial-and-verbal-memory-across-the-adult-life-span-pdf (accessed on 4 March 2024).
- Su, J.; Xiao, X. Factors leading to the trajectory of cognitive decline in middle-aged and older adults using group-based trajectory modeling: A cohort study. Medicine 2022, 101, E31817. [Google Scholar] [CrossRef]
- Roh, M.; Dan, H.; Kim, O. Influencing Factors of Subjective Cognitive Impairment in Middle-Aged and Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 11488. [Google Scholar] [CrossRef] [PubMed]
- Subjective Cognitive Decline—A Public Health Issue. 2019. Available online: https://www.cdc.gov/aging/data/subjective-cognitive-decline-brief.html (accessed on 13 March 2024).
- D’Aurizio, G.; Festucci, F.; Di Pompeo, I.; Tempesta, D.; Curcio, G. Effects of Physical Activity on Cognitive Functioning: The Role of Cognitive Reserve and Active Aging. Brain Sci. 2023, 13, 1581. [Google Scholar] [CrossRef]
- Cosco, T.D.; Howse, K.; Brayne, C. Healthy ageing, resilience and wellbeing. Epidemiol. Psychiatr. Sci. 2017, 26, 579–583. [Google Scholar] [CrossRef]
- Kartschmit, N.; Mikolajczyk, R.; Schubert, T.; Lacruz, M.E. Measuring Cognitive Reserve (CR)—A systematic review of measurement properties of CR questionnaires for the adult population. PLoS ONE 2019, 14, e0219851. [Google Scholar] [CrossRef]
- Chêne, G.; Beiser, A.; Au, R.; Preis, S.R.; Wolf, P.A.; Dufouil, C.; Seshadri, S. Gender and incidence of dementia in the Framingham Heart Study from mid-adult life. Alzheimer’s Dement. 2015, 11, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Harris, K.; Lipnicki, D.M.; Castro-Costa, E.; Lima-Costa, M.F.; Diniz, B.S.; Xiao, S.; Lipton, R.B.; Katz, M.J.; Wang, C.; et al. Sex differences in dementia risk and risk factors: Individual-participant data analysis using 21 cohorts across six continents from the COSMIC consortium. Alzheimer’s Dement. 2023, 19, 3365–3378. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.P.; Smith, D.M.; Mukherjee, S.; Zhang, Y.; Hou, W.; Link, B.G.; Richards, M. Education and Cognitive Decline: An Integrative Analysis of Global Longitudinal Studies of Cognitive Aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, E151–E160. [Google Scholar] [CrossRef] [PubMed]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 2015, 29, 649. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Smith, S.C.; Neuburger, J.; Chrysanthaki, T.; Hendriks, A.A.J.; Black, N. Sociodemographic Characteristics, Cognitive Function, and Health-related Quality of Life of Patients Referred to Memory Assessment Services in England. Alzheimer Dis. Assoc. Disord. 2017, 31, 159–167. [Google Scholar] [CrossRef]
- Lee, Y.; Back, J.H.; Kim, J.; Byeon, H. Multiple socioeconomic risks and cognitive impairment in older adults. Dement. Geriatr. Cogn. Disord. 2010, 29, 523–529. [Google Scholar] [CrossRef]
- Muhammad, T.; Srivastava, S.; Sekher, T.V. Association of self-perceived income sufficiency with cognitive impairment among older adults: A population-based study in India. BMC Psychiatry 2021, 21, 256. [Google Scholar] [CrossRef]
- Yeh, S.C.J.; Liu, Y.Y. Influence of social support on cognitive function in the elderly. BMC Health Serv. Res. 2003, 3, 9. [Google Scholar] [CrossRef]
- Shi, L.; Tao, L.; Chen, N.; Liang, H. Relationship between socioeconomic status and cognitive ability among Chinese older adults: The moderating role of social support. Int. J. Equity Health 2023, 22, 70. [Google Scholar] [CrossRef]
- Karunathilaka, N.; Rathnayake, S. Screening for mild cognitive impairment in people with obesity: A systematic review. BMC Endocr. Disord. 2021, 21, 230. [Google Scholar] [CrossRef]
- Fan, R.; Zhao, L.; Ding, B.; Xiao, R.; Ma, W. The association of blood non-esterified fatty acid, saturated fatty acids, and polyunsaturated fatty acids levels with mild cognitive impairment in Chinese population aged 35–64 years: A cross-sectional study. Nutr. Neurosci. 2021, 24, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Feng, T.; Feng, Z.; Jiang, L.; Yu, Q.; Liu, K. Associations of health behaviors, food preferences, and obesity patterns with the incidence of mild cognitive impairment in the middle-aged and elderly population: An 18-year cohort study. J. Affect. Disord. 2020, 275, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Liu, Q.; Du, Y.; Zhu, Y.; Sun, C.; Lin, H.; Jin, M.; Ma, F.; Li, W.; Liu, H.; et al. Age- and Sex-Specific Prevalence and Modifiable Risk Factors of Mild Cognitive Impairment Among Older Adults in China: A Population-Based Observational Study. Front. Aging Neurosci. 2020, 12, 578742. [Google Scholar] [CrossRef] [PubMed]
- Pedditizi, E.; Peters, R.; Beckett, N. The risk of overweight/obesity in mid-life and late life for the development of dementia: A systematic review and meta-analysis of longitudinal studies. Age Ageing 2016, 45, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Chi, I.; Palinkas, L.A. Widowhood, leisure activity engagement, and cognitive function among older adults. Aging Ment. Health 2019, 23, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, K.; Rovio, S.; Helkala, E.L.; Vilska, A.R.; Winblad, B.; Soininen, H.; Nissinen, A.; Mohammed, A.H.; Kivipelto, M. Association between mid-life marital status and cognitive function in later life: Population based cohort study. BMJ 2009, 339, 99. [Google Scholar] [CrossRef] [PubMed]
- Jennings, E.A.; Farrell, M.T.; Liu, Y.; Montana, L. Associations between cognitive function and marital status in the United States, South Africa, Mexico, and China. SSM Popul. Health 2022, 20, 101288. [Google Scholar] [CrossRef] [PubMed]
- Sundström, A.; Westerlund, O.; Mousavi-Nasab, H.; Adolfsson, R.; Nilsson, L.G. The relationship between marital and parental status and the risk of dementia. Int. Psychogeriatr. 2014, 26, 749–757. [Google Scholar] [CrossRef]
- Bubu, O.M.; Brannick, M.; Mortimer, J.; Umasabor-Bubu, O.; Sebastião, Y.V.; Wen, Y.; Schwartz, S.; Borenstein, A.R.; Wu, Y.; Morgan, D.; et al. Sleep, Cognitive impairment, and Alzheimer’s disease: A Systematic Review and Meta-Analysis. Sleep 2017, 40, zsw032. [Google Scholar] [CrossRef]
- Wang, Q.; Xu, S.; Liu, F.; Liu, Y.; Chen, K.; Huang, L.; Xu, F.; Liu, Y. Causal relationship between sleep traits and cognitive impairment: A Mendelian randomization study. J. Evid. Based Med. 2023, 16, 485–494. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Keadle, S.K.; Conroy, D.E.; Buman, M.P.; Dunstan, D.W.; Matthews, C.E. Targeting Reductions in Sitting Time to Increase Physical Activity and Improve Health. Med. Sci. Sports Exerc. 2017, 49, 1572. [Google Scholar] [CrossRef]
- Wu, J.; Fu, Y.; Chen, D.; Zhang, H.; Xue, E.; Shao, J.; Tang, L.; Zhao, B.; Lai, C.; Ye, Z. Sedentary behavior patterns and the risk of non-communicable diseases and all-cause mortality: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2023, 146, 104563. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.Y.; Qian, G.P.; Wang, F.; Zhang, M.Y.; Da, Y.J.; Liang, J.H. Association between sedentary behavior and risk of cognitive decline or mild cognitive impairment among the elderly: A systematic review and meta-analysis. Front. Neurosci. 2023, 17, 1221990. [Google Scholar] [CrossRef] [PubMed]
- Le Roux, E.; De Jong, N.P.; Blanc, S.; Simon, C.; Bessesen, D.H.; Bergouignan, A. Physiology of physical inactivity, sedentary behaviors and non-exercise activity: Insights from space bedrest model. J. Physiol. 2022, 600, 1037. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical Activity, Cognition, and Brain Outcomes: A Review of the 2018 Physical Activity Guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Barha, C.K.; Best, J.R. Physical activity for brain health in older adults. Appl. Physiol. Nutr. Metab. 2018, 43, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Spartano, N.L.; Demissie, S.; Himali, J.J.; Dukes, K.A.; Murabito, J.M.; Vasan, R.S.; Beiser, A.S.; Seshadri, S. Accelerometer-determined physical activity and cognitive function in middle-aged and older adults from two generations of the Framingham Heart Study. Alzheimer’s Dement. 2019, 5, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Banducci, S.E.; Weinstein, A.M.; Macdonald, A.W.; Ferrell, R.E.; Halder, I.; Flory, J.D.; Manuck, S.B. The brain-derived neurotrophic factor Val66Met polymorphism moderates an effect of physical activity on working memory performance. Psychol. Sci. 2013, 24, 1770–1779. [Google Scholar] [CrossRef]
- Winneke, A.; Godde, B.; Reuter, E.-M.; Vieluf, S.; Voelcker-Rehage, C. The Association between Physical Activity and Attentional Control in Younger and Older Middle-Aged Adults. GeroPsych J. Gerontopsychol. Geriatr. Psychiatry 2012, 25, 207–221. [Google Scholar] [CrossRef]
- Miyawaki, C.E.; Bouldin, E.D.; Kumar, G.S.; McGuire, L.C. Associations between physical activity and cognitive functioningamong middle-aged and older adults. J. Nutr. Health Aging 2017, 21, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Vásquez, E.; Strizich, G.; Isasi, C.R.; Echeverria, S.E.; Sotres-Alvarez, D.; Evenson, K.R.; Gellman, M.D.; Palta, P.; Qi, Q.; Lamar, M.; et al. Is there a relationship between accelerometer-assessed physical activity and sedentary behavior and cognitive function in US Hispanic/Latino adults? The Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Prev. Med. 2017, 103, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Ciria, L.F.; Román-Caballero, R.; Vadillo, M.A.; Holgado, D.; Luque-Casado, A.; Perakakis, P.; Sanabria, D. An Umbrella Review of Randomized Control Trials on the Effects of Physical Exercise on Cognition. Nat. Hum. Behav. 2023, 6, 928–941. [Google Scholar] [CrossRef]
- Yu, D.J.; Yu, A.P.; Bernal, J.D.K.; Fong, D.Y.; Chan, D.K.C.; Cheng, C.P.; Siu, P.M. Effects of exercise intensity and frequency on improving cognitive performance in middle-aged and older adults with mild cognitive impairment: A pilot randomized controlled trial on the minimum physical activity recommendation from WHO. Front. Physiol. 2022, 13, 1021428. [Google Scholar] [CrossRef]
- Encuesta Nacional de Salud 2017. EESE 2017. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/ENSE17_Metodologia.pdf (accessed on 15 May 2024).
- Encuesta Europea de Salud en España 2020. EESE 2020. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/EncuestaEuropea/EncuestaEuropea2020/Metodologia_EESE_2020.pdf (accessed on 15 May 2024).
- Dwumoh, D.; Essuman, E.E.; Afagbedzi, S.K. Determinant of factors associated with child health outcomes and service utilization in Ghana: Multiple indicator cluster survey conducted in 2011. Arch. Public Health 2014, 72, 42. [Google Scholar] [CrossRef]
- Xu, L.; Jiang, C.Q.; Lam, T.H.; Zhang, W.S.; Thomas, G.N.; Cheng, K.K. Dose-Response Relation between Physical Activity and Cognitive Function: Guangzhou Biobank Cohort Study. Ann. Epidemiol. 2011, 21, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Klimova, B.; Dostalova, R. The Impact of Physical Activities on Cognitive Performance among Healthy Older Individuals. Brain Sci. 2020, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, C.; Rattray, B.; Pryor, D.; Northey, J.M.; Cherbuin, N. Physical activity and cognitive function in middle-aged adults: A cross-sectional analysis of the PATH through life study. Front. Psychol. 2023, 14, 1022868. [Google Scholar] [CrossRef]
- Zerr, C.L.; Berg, J.J.; Nelson, S.M.; Fishell, A.K.; Savalia, N.K.; McDermott, K.B. Learning Efficiency: Identifying Individual Differences in Learning Rate and Retention in Healthy Adults. Psychol. Sci. 2018, 29, 1436–1450. [Google Scholar] [CrossRef]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P.R. Subjective versus Objective Measure of Physical Activity: A Systematic Review and Meta-Analysis of the Convergent Validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public Health 2021, 18, 3413. [Google Scholar] [CrossRef]
- Iso-Markku, P.; Aaltonen, S.; Kujala, U.M.; Halme, H.-L.; Phipps, D.; Knittle, K.; Vuoksimaa, E.; Waller, K. Physical Activity and Cognitive Decline Among Older Adults: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2024, 7, e2354285. [Google Scholar] [CrossRef]
- Taylor, C.A.; Bouldin, E.D.; McGuire, L.C. Subjective Cognitive Decline Among Adults Aged ≥45 Years—United States, 2015–2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 753–757. [Google Scholar] [CrossRef]
- Lin, L.-H.; Wang, S.-B.; Xu, W.-Q.; Hu, Q.; Zhang, P.; Ke, Y.-F.; Huang, J.-H.; Ding, K.-R.; Li, X.-L.; Hou, C.-L.; et al. Subjective cognitive decline symptoms and its association with socio-demographic characteristics and common chronic diseases in the southern Chinese older adults. BMC Public Health 2022, 22, 127. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, Y.; Burgard, S.A.; Needham, B.L. Marital status and cognitive impairment in the United States: Evidence from the National Health and Aging Trends Study. Ann. Epidemiol. 2019, 38, 28–34.e2. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total = 15,866 | Men = 7765 | Women = 8101 | X2 | df | p | V | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | IQR | Median | IQR | Median | IQR | |||||
| Age (Years) | 55 | (10) | 54 | (10) | 55 | (10) | n.a. | n.a. | 0.166 | n.a. |
| Civil Status | n | % | n | % | N | % | X2 | df | p * | V |
| Single | 2883 | 18.2 | 1628 | 21.0 | 1255 | 15.6 *** | 349.3 | 4 | <0.001 | 0.15 |
| Married | 10,074 | 63.7 | 5035 | 65.0 | 5039 | 62.5 ** | ||||
| Widowed | 692 | 4.4 | 127 | 1.6 | 565 | 7.0 *** | ||||
| Legally separated | 678 | 4.3 | 306 | 4.0 | 372 | 4.6 * | ||||
| Divorced | 1484 | 9.4 | 648 | 8.4 | 836 | 10.4 *** | ||||
| Study Level | ||||||||||
| Primary | 3149 | 19.8 | 1538 | 19.8 | 1611 | 19.9 | 50.7 | 4 | <0.001 | 0.06 |
| Secondary | 4396 | 27.7 | 2288 | 29.5 | 2108 | 26.0 *** | ||||
| Baccalaureate | 2175 | 13.7 | 1073 | 13.8 | 1102 | 13.6 | ||||
| Vocational training | 2768 | 17.4 | 1379 | 17.8 | 1389 | 17.1 | ||||
| University | 3378 | 21.3 | 1487 | 19.2 | 1891 | 23.3 *** | ||||
| Social Class | ||||||||||
| I | 1788 | 11.5 | 855 | 11.1 | 933 | 11.9 | 136.2 | 5 | <0.001 | 0.09 |
| II | 1259 | 8.1 | 590 | 7.7 | 669 | 8.5 | ||||
| III | 3155 | 20.3 | 1436 | 18.7 | 1719 | 21.9 *** | ||||
| IV | 2070 | 13.3 | 1213 | 15.8 | 857 | 10.9 *** | ||||
| V | 5056 | 32.5 | 2616 | 34.1 | 2440 | 31.0 *** | ||||
| VI | 2206 | 14.2 | 959 | 12.5 | 1247 | 15.9 *** | ||||
| BMI Group | ||||||||||
| Underweight | 191 | 1.2 | 33 | 0.4 | 158 | 2.0 *** | 812.0 | 3 | <0.001 | 0.23 |
| Normal | 5925 | 38.6 | 2145 | 28.3 | 3780 | 48.6 *** | ||||
| Overweight | 6389 | 41.6 | 3817 | 50.3 | 2572 | 33.1 *** | ||||
| Obesity | 2862 | 18.6 | 1597 | 21.0 | 1265 | 16.3 *** | ||||
| PAF | ||||||||||
| Never | 5579 | 35.2 | 2740 | 35.3 | 2839 | 35.1 | 50.2 | 3 | <0.001 | 0.06 |
| Occasionally | 6696 | 42.2 | 3102 | 40.0 | 3594 | 44.4 ** | ||||
| Frequently | 1655 | 10.4 | 905 | 11.7 | 750 | 9.3 *** | ||||
| Very frequently | 1922 | 12.1 | 1010 | 13.0 | 912 | 11.3 ** | ||||
| Subjective Cognitive Limitations Level | ||||||||||
| No | 14,246 | 89.8 | 7115 | 91.6 | 7131 | 88.0 *** | 63.0 | 3 | <0.001 | 0.06 |
| Yes, something | 1382 | 8.7 | 537 | 6.9 | 845 | 10.4 *** | ||||
| Yes, a lot | 211 | 1.3 | 98 | 1.3 | 113 | 1.4 | ||||
| Yes, absolutely | 27 | 0.2 | 15 | 0.2 | 12 | 0.1 | ||||
| Subjective Cognitive Limitations | X2 | df | p | Φ | ||||||
| No | 14,246 | 89.8 | 7115 | 91.6 | 7131 | 88.0 * | 56.1 | 1 | <0.001 | 0.06 |
| Yes | 1620 | 10.2 | 650 | 8.4 | 970 | 12.0 *** | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, Á.; Salas-Gómez, D.; Franco-García, J.M.; Adsuar, J.C.; Parraca, J.A.; Collado-Mateo, D. Associations between Physical Activity Frequency in Leisure Time and Subjective Cognitive Limitations in Middle-Aged Spanish Adults: A Cross-Sectional Study. Healthcare 2024, 12, 1056. https://doi.org/10.3390/healthcare12111056
Denche-Zamorano Á, Salas-Gómez D, Franco-García JM, Adsuar JC, Parraca JA, Collado-Mateo D. Associations between Physical Activity Frequency in Leisure Time and Subjective Cognitive Limitations in Middle-Aged Spanish Adults: A Cross-Sectional Study. Healthcare. 2024; 12(11):1056. https://doi.org/10.3390/healthcare12111056
Chicago/Turabian StyleDenche-Zamorano, Ángel, Diana Salas-Gómez, Juan Manuel Franco-García, José Carmelo Adsuar, José A. Parraca, and Daniel Collado-Mateo. 2024. "Associations between Physical Activity Frequency in Leisure Time and Subjective Cognitive Limitations in Middle-Aged Spanish Adults: A Cross-Sectional Study" Healthcare 12, no. 11: 1056. https://doi.org/10.3390/healthcare12111056